
Abstract
The number of older Moroccan migrants reaching the age of high risk for dementia is increasing in Belgium. Yet no study has been performed to explore how Moroccan families facing dementia experience and manage the condition. The study employed a qualitative design using semi-structured interviews with 12 informal and 13 formal caregivers to answer this research question. Findings indicate that the experience of dementia includes several invisible realities that challenge the informal and formal caregivers: (1) the invisibility of dementia as a condition; (2) the invisible subtleties of the informal care execution; (3) the invisibility and inaccessibility of care services as explanation for these family’s non-use of available services; and (4) the overlooking of culture, migration and religion as invisible influencers of the overall dementia experience. A better understanding of these hidden realities of migrant older people with dementia and their caregivers could lead to interventions to provide effective and tailored person-centred care that is sensitive to the individual’s life experiences, culture and religious background.
Keywords
Introduction
In 2016, the Flemish governmental research centre estimated that in Flanders, the Dutch-speaking region of Belgium, 6% of all persons aged 65 and older had a migration background (Lodewijcks, 2017). The number is much higher in those cities and regions that hosted the majority of migrants who came to Belgium during 1960s and 1970s (Lodewijcks, 2014, 2017). Moreover, the share of older persons of diverse ethnic background will grow in the future (Lodewijcks, 2014). Ethnic minorities of Moroccan origin constitute the largest group of non-European migrants in Flanders (Ouali, 2004): 10% of the ethnic minority older people in Flanders are of Moroccan background. This percentage is higher in cities and regions with strong migration history, such as Antwerp, Brussels and Limburg. For example, in 2010, 28% of older persons in Brussels who were of migration background had Moroccan roots (Lodewijcks, 2014).
These Moroccan older people migrated to Belgium during the 1960s and 1970s under the guest worker program to work in mining and other industries (Reniers, 1999; Van Mol & de Valk, 2016). The host country initially expected that these migrants would work for a temporary period and then return to their home country; reality proved different, however. The migrants, sometimes counter to their own original aspirations, ended up staying, having developed emotional attachment (Buffel, 2015) to their host country, in particular by having children and grandchildren there and having realized the value of a high-quality health care system (Albert, Ferring, & Lang, 2016). This migration history has been a key negative influence on the current socio-economic position of these older people. A low literacy has been confirmed by the quantitative data of Lodewijcks (2014): 70% of seniors of Moroccan origin aged 70 or older had never had any type of formal schooling. The adverse socio-economic status of older immigrants is something that European labour migrants appear to share in old age (Liversage & Jakobsen, 2016).
Older Moroccan migrants with dementia
In 2016, the Flanders government estimated that 122,000 persons in the region had dementia. This prevalence of dementia is projected to increase by 25% by 2030 (Vandeurzen, 2016). Given the difficulty of diagnosing dementia in ethnic minority seniors, it remains a challenge to accurately estimate the prevalence of dementia amongst such groups (Nielsen, Vogel, Phung, Gade, & Waldemar, 2010). Recent research by Parlevliet et al. (2016) using culturally sensitive diagnostic tools shows a higher prevalence of dementia among non-European older people in the Netherlands. The prevalence of dementia among older people of Moroccan background in the Netherlands was four times higher than among native-born older people. Segers et al. (2013) detected an increase from 6% to 16% of newly referred non-European patients from 2005 until the first half of 2012 in their memory clinic in Brussels. Dementia centres in 15 European countries have reported similar increases (Nielsen et al., 2011).
Although clinical manifestations of dementia may be similar across different countries, migration and cultural background can influence the experience of the condition (Johl, Patterson, & Pearson, 2015). This is suggested by research performed in countries with longer migration histories, such as the United States (Cooper, Tandy, Balamurali, & Livingston, 2010; Livney et al., 2011). The results of previous studies are valuable, though difficult to apply to the Belgian context. This is also the case for studies about older migrants with Moroccan background in neighbouring countries. As documented by Ouali (2003) the migration patterns, profiles of Moroccans differ between European countries. Also, the migration policy of the different European hosting countries differs, having a different impact on these migrants. An example is the policy of family reunification: Belgium stimulated family reunification of its Moroccan labour migrants from the start of the labour migration in the 1960s, whereas neighbouring countries like France and the Netherlands only started this policy after the migration stop in 1973. Recent insights (Ferrer, Grenier, Brotman, & Koehn, 2017; Torres, 2015) also recommend an intersectional approach in studies dealing with the intersection of migration and ageing, taking into account the macro contextual influence on the individual life courses. As migration history, ethnicities and migration policies are markedly different in each national context; thus, we must be cautious in trying to establish general conclusions (Constant, García-Muñoz, Neuman, & Neuman, 2018; Kuo, 2014; Sodowsky & Plake, 1992).
Older migrants with dementia are a relatively new phenomenon, and this is reflected in the limited research on the topic for Belgium (Nielsen et al., 2011; Segers et al., 2013).
Barriers to help-seeking for dementia in ethnic minority groups
Dementia has a great impact on older people and their caregivers (Snyder et al., 2014). Janevic and Connell (2001) stress the importance of accounting for cultural factors when dealing with dementia. Detecting these group-specific elements is essential for developing suitable care and support both for the older people and for their informal caregivers. According to Mukadam, Cooper, and Livingston (2013), ethnic minority groups in Western countries such as the United Kingdom and the United States face three barriers in seeking help when confronted with dementia. The first concerns how dementia is perceived. As compared to the majority population, ethnic minorities appear to perceive dementia as a normal consequence of aging. They do not recognize it as an illness, and they attribute associated behavioural changes, such as forgetfulness, to normal aging-related behaviour (Mukadam, Cooper, & Livingston, 2011; Mukadam, Cooper, Basit, & Livingston, 2011; Van Wezel et al., 2016).
The second barrier concerns society- and community-related factors. Care for relatives is perceived as an engagement that family members will execute until it becomes unmanageable or otherwise unfeasible. This attitude towards care, in combination with less frequent use of care services and with pressures to conform to cultural expectations related to caring for family members can lead to an especially heavy care burden (Moriarty, Sharif, & Robinson, 2014; Van Wezel et al., 2016). Cultural aspects appear to play a major role in defining how family care should be executed. For example, ethnic minorities expect more from women and adult children as caregivers (Moriarty, 2015). This is confirmed by Van Wezel’s study (2016), which examined non-European migrants in the Netherlands. Family care is seen as a task imposed by culture and religion and one ascribed primarily to women.
The third barrier refers to the health care system and the experience with health care professionals. European health care systems present structural barriers towards ethnic minorities, leading to inequity in accessing this care. These barriers result from national policies of lesser entitlement to health for ethnic minorities in combination with the ‘one size fits all’ approaches practiced by health care facilities (Ingleby, Chiarenza, Devillé, & Kotsioni, 2012). These structural barriers are enforced by personal and cultural barriers, thereby leading to underuse of dementia care by ethnic minorities (Mukadam et al., 2013). The perceived pressure to care for one’s parents, the sense of stigma felt when using the services, together with the experienced or perceived lack of culturally suitable care for older people, reinforce the wariness and hesitation to make use of these services (Denier & Gastmans, 2013; La Fontaine, Ahuja, Bradbury, Phillips, & Oyebode, 2007; Mukadam et al., 2013; Nielsen et al., 2011). These studies underscore the need for individually tailored dementia services through which ethnic minority older people and their relatives can receive support that is both effective and positive.
The information described above suggests that older Moroccan migrants, the largest subgroup within the ethnic minority older population of Belgium, are growing older and have an expected high risk for dementia (Lodewijcks, 2017; Parlevliet et al., 2016). To our knowledge, there is no data available on how their caregivers experience dementia or how these experiences affect the Moroccan population in Belgium. This study aims therefore to answer the following research questions: (1) How do (informal and formal) caregivers experience the dementia and care of a Moroccan migrant elder? (2) How do culture and religion influence this dementia experience?
Methods
Design
A qualitative study with semi-structured interviews was held to collect in-depth information about the experiences of informal and formal caregivers of older persons of Moroccan origin with dementia (Gibson, Timlin, Curran, & Wattis, 2004).
Participants
Participants among Moroccan informal caregivers’ (IC) demographics (age, gender, socio-economic profile) and relationship to person with dementia (PD) and his/her diagnosis: AD (Alzheimer’s disease) FTD (frontotemporal dementia).

Note. Region refers to where the caregiver lives.
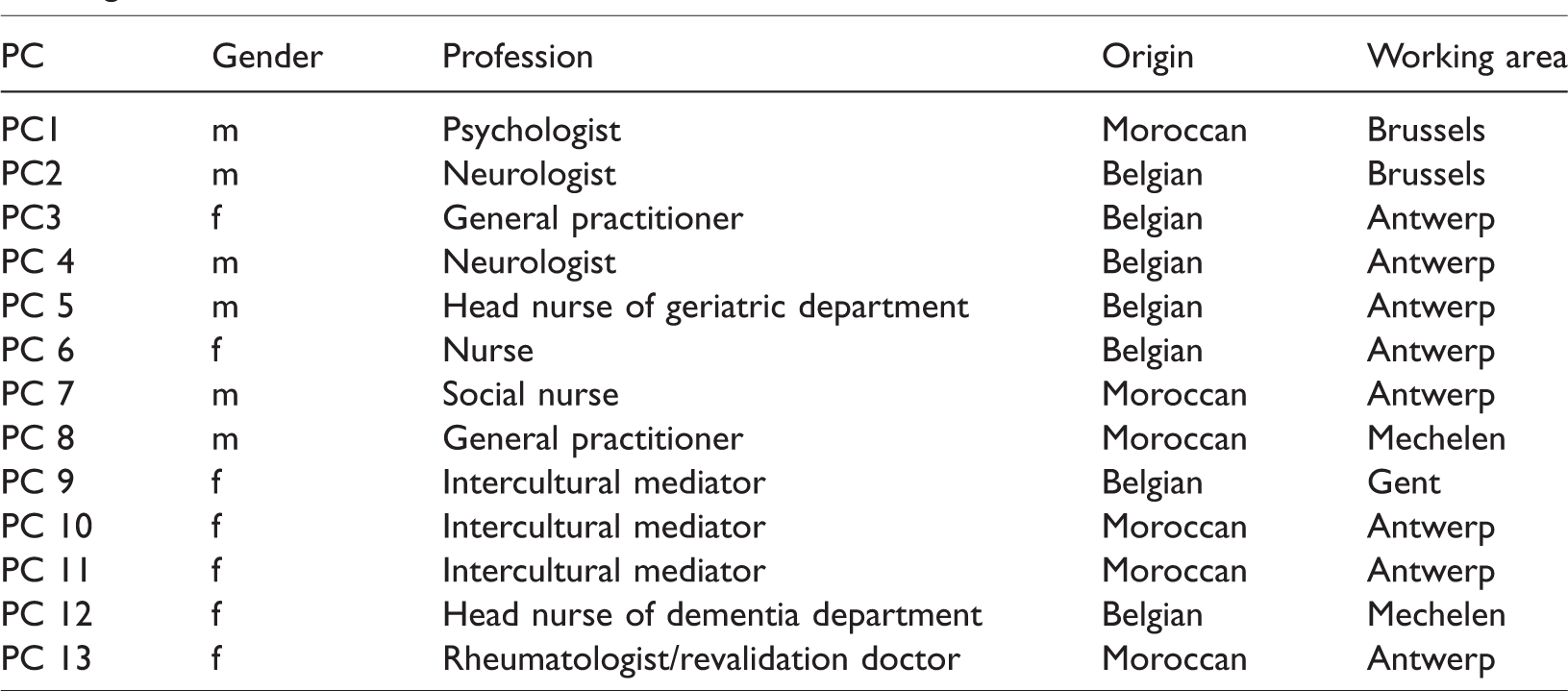
The participation criterion for professional caregivers was: being a care professional with experience in caring for Moroccan seniors with dementia. To include different perspectives, these professional caregivers were active in different care disciplines, ranging from general practitioners to nurses, to intercultural mediators (see Table 2). This corresponds with the multidisciplinary approach to dementia. The search area was chosen based on typical migrant settlement patterns in Belgium. Regions that attracted large numbers of people of Moroccan origin include Antwerp, Brussels and Mechelen (Lodewijcks, 2014).
Participants among professional caregivers’ (PC) demographics (gender, origin), profession and working area.
Interview scheme
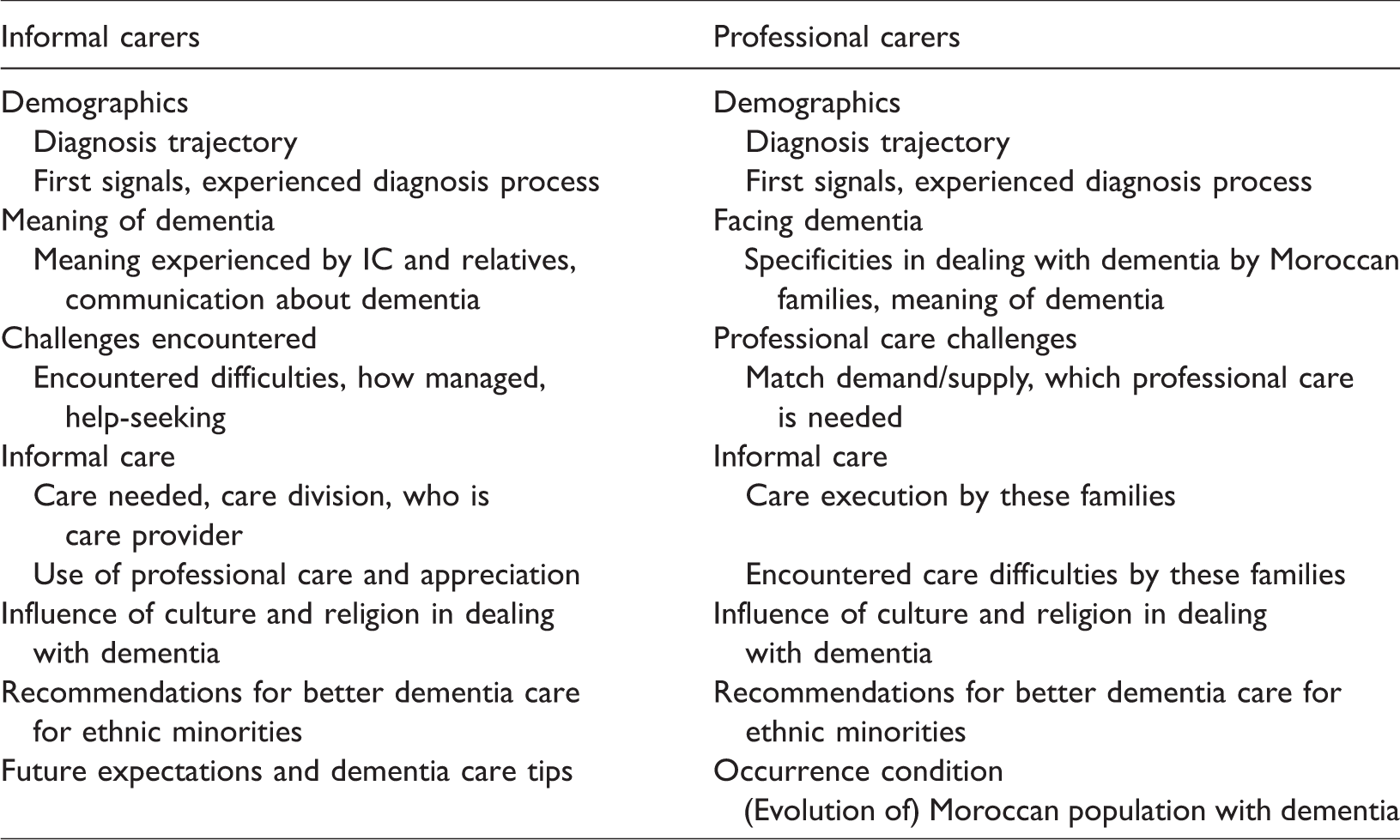
Twenty-two semi-structured interviews were the main data collection method in this qualitative study. One initial focus group was organized to determine relevant themes for further elaboration during the interviews (Gill, Stewart, Treasure, & Chadwick, 2008). Based on these themes two different interview schedules were composed, one for informal carers and one for professionals. Topics covered in both schedules are stated in Table 3.
Topics covered in interviews with informal and professional carers.
Data collection procedure
Recruitment of the participants proceeded in steps. Six key figures within the Moroccan community were involved (e.g. (social) care professionals, community leaders); they identified informal carers within their respective networks and introduced the researcher to them. Care professionals were also recruited in several steps. Several care professionals were already known by reputation as having diverse client population, in particular owing to their location in ethnically diverse neighbourhoods. Using the snowball method, additional professionals were contacted in the selected search area.
Data were collected in the period of November 2014 until March 2015. Each interview was conducted at a location chosen by the participant and took between 38 and 168 minutes. Dutch was the main data collection language, with some use of Arabic expressions by informal carers. One interview was held in French. The researcher is fluent in each of these languages.
Analysis
The interviews were recorded using Audacity recording software and then transcribed verbatim. The data analysis was conducted in an inductive way, with the data taken as a primary source for the conceptualization process (Charmaz, 2011). The analysis respected the steps needed for qualitative research, by first deconstructing the data by open, axial coding as an analytic process where the individual concepts and their properties are identified, followed by linking those concepts to categories with sub-categories (Dierickx de Casterleé et al., 2012). The next phase of reconstruction began with selective coding, where these categories are integrated and refined. These steps reflect the analytic process of qualitative research seen as de-conceptualization followed by reconceptualization (Cobb & Forbes, 2002).
Ethical aspects
All participants gave both written and verbal consent at the beginning of the individual interviews and focus group. An informed consent document was presented to the participants, detailing the broader objectives of the study, possibility to withdraw from the study at any time and information about data governance. To maintain confidentiality identifiable information was altered and participants were coded. The audio recordings were destroyed after the completion of the study. The study followed the guidelines of Human Sciences Ethical Committee of the VUB, respecting the European Framework for Research Ethics (http://ec.europa.eu/research/participants/data/ref/fp7/89888/ethics-for-researchers_en.pdf). Since the study only included competent human subjects and didn’t invade the participant’s privacy, no additional approval was needed by the committee (www.vub.ac.be/onderzoek/beleid/ethische-commissie).
Results
Invisibility of dementia as a condition
The results suggest that dementia was invisible to the respondents as an actual condition. This invisibility manifested itself during and after the diagnosis phase.
During the diagnosis phase, older adults, family members and professionals struggled with detecting and recognizing dementia. Family members often were the initiators of the diagnosis process, especially after witnessing alarming symptoms such as markedly ‘unfamiliar’ and/or dangerous behaviours. They started the process in search of explanation.
The second way the condition was diagnosed was via accidental contact with professional care during hospitalization for other matters. Care professionals confirmed this tendency for ‘accidental diagnosis’ through late contact with medical help. The first contact with Moroccan older people was often at a later stage of dementia when there were fewer possibilities for stabilizing the condition. Suggested reasons for this delay were lack of insight about dementia being a condition and the perception that ‘forgetting’ is normal age-related behaviour, as stated by an informal caregiver:
One day on his way back from the bank he gave all his money to anyone who looked needy. [Laughs] We thought this is maybe due to age…. Every time something else happened, until they [hospital staff] told us that he is ill.
Professionals appraised the combination of an absence of adequate assessment tools alongside the presence of a language barrier as the most challenging aspects in diagnosing these migrant older people. For these reasons, diagnostic tests such as the Mini-Mental State Examinations (MMSE) were not used, as mentioned by a General Practitioner: It stops there already … I have to invent half of the test. Which day are we today? Does every Moroccan illiterate housewife have to know that it is the 23rd of February? Does she have dementia because she cannot count backwards from 100?
Professional caregivers articulated the need for adequate culture-sensitive tests and language-bridging-tools such as assistance from a translator or intercultural mediator. Conversely, the intercultural mediators among the participants stated that a major problem was their not being consulted to perform an MMSE, despite their being trained to do so. The neurologists raised the issue of the resulting financial disadvantage for older Moroccan migrants when diagnostic tests are not used. The social security policy in Belgium indeed only refunds dementia medication in the early stage of dementia when the MMSE-scores are still high, and the effectiveness of the medication is the highest. Accordingly, the Moroccan seniors don’t benefit from this refund: A major problem of medication is that its reimbursement (through the healthcare system) depends on the MMSE score. These older seniors tend to score lower because of their low education, not because the dementia is in a severe stage, and [consequently they] don’t receive any refund. (A neurologist)
All participants mentioned that dementia is often labelled differently. These labels fall into two major categories: culturally known descriptions and biomedical labels. The first category reflects unfamiliarity with dementia (the older person is assumed to be forgetful, crazy, possessed, spoiled ‘fsoesh’, a confused head) while the second acknowledges dementia as a biomedical condition (Alzheimer, Zheimer, Dementia). The use of the first category partially reflects non-acceptance of the condition by denying its severity: None! She [mother with dementia] doesn’t use any words. It isn’t an illness for her, she doesn’t want to accept it. (Informal carer 11) Mother says, ‘I’m confused in my head (“trwent frasi”)’, you understand… then you will not say ‘Mama, you have dementia’. We didn’t even find any Arabic words for it. (Informal carer 6) They didn’t know Alzheimer, in Morocco neither. (Informal carer 10) I don’t use ‘dementia’ – they don’t use it, so I don’t! Some professionals persist in using biomedical terminology, but these older people don’t understand it and they seek confirmation. Sometimes you need to follow their words to approach the senior with sincerity. This is the first generation reaching that age. We [the Moroccan community], sadly, weren’t prepared for it. We also had to face a lot of challenges (education, employment issues, etc.)… we cannot anticipate everything.
Invisibility of the involved parties and tasks in informal care
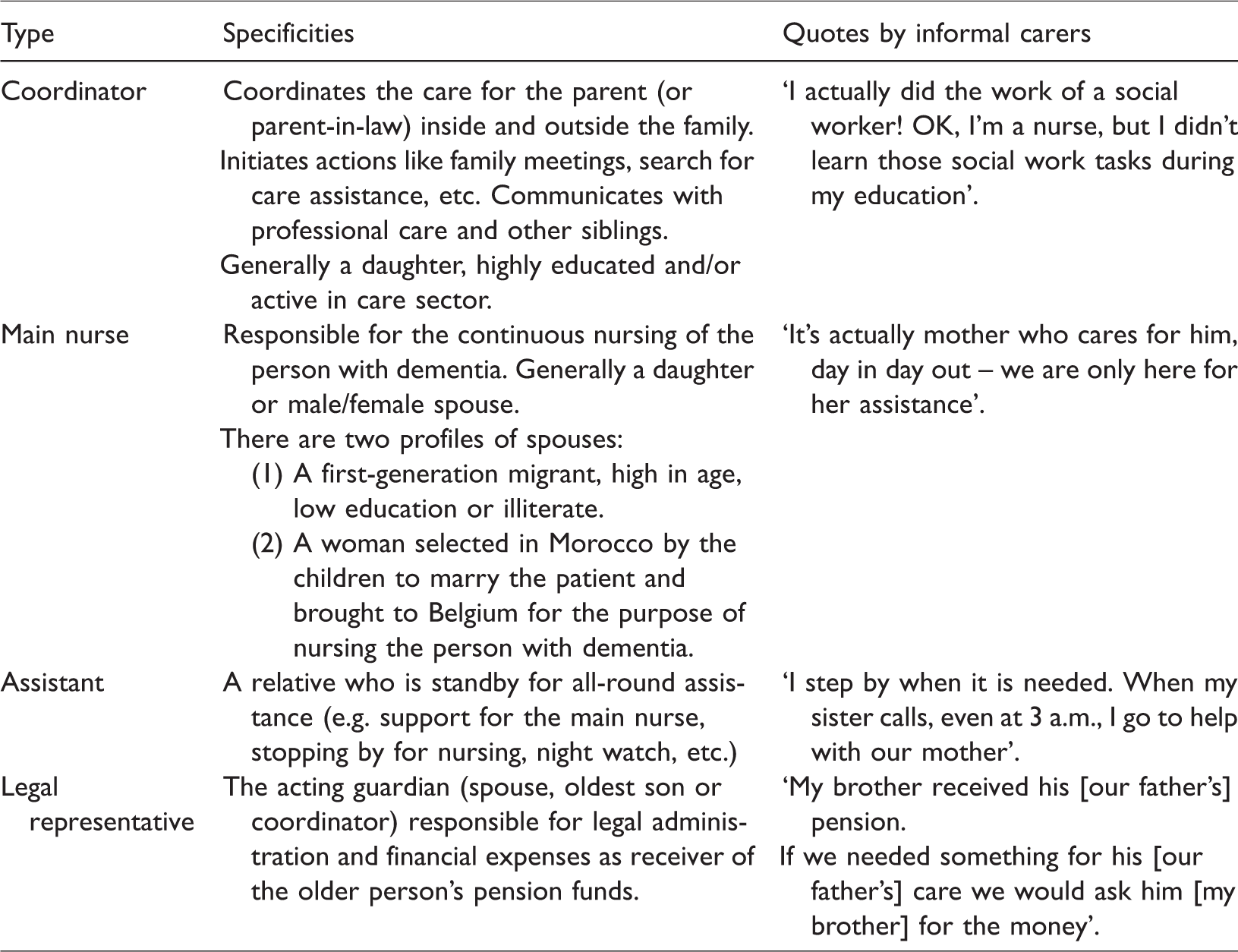
Findings suggest that professional caregivers saw only a glimpse of the meaning and the organization of informal care within these Moroccan families. They mentioned only females (e.g. wife, daughter or daughter-in-law) as informal caregivers in Moroccan families. Informal caregivers, however, displayed different views: they noted that both men and women were assuming informal caregiving tasks. Four roles of informal carers were derived from the analysis, nuancing the concept of ‘the’ informal caregiver: these roles are the coordinator, the assistant, the legal responsible and the main nurse (Table 4).
Types and descriptions of informal caregivers of Moroccan origin.
In most cases, these various types of informal caregivers contributed as a care network to provide informal care for the older person with dementia. They all shared a tremendous devotion in providing informal care. The professional participants found this attitude to be typical of Moroccan informal caregivers. Several professional caregivers voiced concern about this aspect, however, having seen problems such as self-abandonment and long-term (mental) health issues (e.g. depressions, exhaustion) emerge among informal caregivers as a result of their devotion.
Invisible and inaccessible dementia care services
Informal caregivers encountered several obstacles when they decided to seek professional help. The majority of the informal caregivers had been unaware of the extent of professional care for dementia that was available in Belgium. (Accidentally) encountering a professional caregiver who informed them about such care was decisive in their learning about potential options, as expressed by an informal carer: It was by chance. I was talking to my physiotherapist … he asked me if I knew about night care, and gave me the name of the organization…. I wouldn’t know about it if he hadn’t told me.
Another obstacle related to how professional caregivers performed their care. Informal carers felt that a person-centred approach was often lacking. They experienced a lack of (cultural) sensitivity in combination with swift technical execution of care with little room for the humane aspects of such care. Despite the informal caregivers’ appreciation for the professionalism of these caregivers, these humane aspects were decisive in their opting whether or not to use professional care, either at home and residential. Due to the language barrier, Moroccan seniors were unable to formulate their needs to professional caregivers. This enhanced the informal caregiver’s anxiety to entrust the patient to professional caregivers who exhibited little cultural sensitivity. This anxiety was often based on experience with professional carers who did not respect religious rituals (such as prayer), halal dietary practices or gender matching.
Professional caregivers were generally unaware that the absence of culture- and religion-sensitive care was a primary reason that informal carers avoided using professional care. They often mentioned the informal carers’ culture as the main reason for this lack of professional care use. The apparent pressure on children to care for their parents was also mentioned by informal carers as an additional source of hesitation against seeking professional help. Children and other family members feared gossip and disapproval from the Moroccan community. Some informal caregivers even postponed professional aid, as described by a daughter: It took me six months to call the night care. Yes, what would people say…?
Invisibility of culture and religion as influencing factors
In addition to this more natural reflex on the part of the family to care for their elder with dementia, other positive aspects of the Moroccan culture that were described include collective support and concern. The aspects were mentioned mainly by professional caregivers with Belgian roots. Informal caregivers and professional caregivers with Moroccan origin introduced certain subtleties to this image of solidarity. The solidarity they experienced was limited to expressions of moral support and did not entail concrete actions.
Professional carers stressed the importance of culture as a motivator for providing informal care to the older people. According to most, informal care was a duty to be performed and not to be questioned. Informal caregivers themselves, however, presented a more complex reality about the meaning of informal care within their families. The initial religious- and culture-inspired values to provide informal care are commingled with more pragmatic reasons for doing so. The informal caregivers agreed that caring for older people as they had once cared for you is a natural cultural, religious and emotional norm.
Professional caregivers frequently mentioned that dementia remains a taboo, as formulated by this nurse: I don’t have the impression that you can talk about dementia with them, it’s taboo in their culture. I talk to everyone about it, my sisters do too. There are people from the Moroccan community who don’t. I find that unfortunate. The person with dementia didn’t choose it, neither did we.
Some respondents said that dementia is a condition that comes from God (Allah). Some informal caregivers considered the illness to be a way that their spouse or parent with dementia could erase all the bad deeds they had done in their life. This was experienced both as something positive and as something that helped in coping with the condition, as formulated by a son: Allah wanted it like this… that he has dementia; maybe my father did something in his life and by experiencing these illnesses he’s being forgiven by Allah. Our father, that’s the only thing that he had. He kept praying. He forgot everything except that. He found his peace of mind in it. Also with the Quran: when we put it on, he recited with the reciter.
Discussion
This study investigated how caregivers experienced dementia and care for first-generation seniors of Moroccan origin with dementia. We also explored the role of culture, migration and religion as influencing factors for these experiences.
Our results indicate an accumulation of invisibilities in the course of the dementia trajectory which lead to a specific experience of dementia by the Moroccan population. It begins with the invisibility of dementia as a condition, which leads to delay in initiating the diagnosis process and in applying accurate labels to the condition. The participants among the informal carers initiated the diagnosis process only after emergence of obvious dementia-related behavioural abnormalities. This confirms previous research which found that initial symptoms such as forgetfulness are considered normal age-related behaviours and not yet medically relevant enough to seek help for (Botsford, Clarke, & Gibb, 2011; Van Wezel et al., 2016). A lack of information about and understanding of dementia can also explain this delay (Johl et al., 2015). Our findings confirm the lack of culture-sensitive assessment tools, which research has shown leads to diagnostic evaluations of lesser quality (Nielsen et al., 2011). Informal caregivers find it challenging to communicate with their elders about their dementia diagnosis. The capability of the ill relative to bear and to understand such news is taken into consideration when deciding whether and to what extent to be open with them about the diagnosis (van Eechoud et al., 2015). Different ethnic minorities use different labels for dementia, based on their perceptions of the condition (Nielsen & Waldemar, 2015). Thus, informal caregivers employ a (culture-) specific combination of social and biomedical labels to communicate about the condition. It is typical, for these migrant seniors and their informal caregivers, that the term dementia is not used as a reference (Segers et al., 2013; Shanley et al., 2012). The accumulation of these underlying aspects renders dementia invisible and difficult to grasp, both for the person with dementia and for his or her carers, informal and professional.
A second invisible reality concerns the execution of informal care within Moroccan families in Belgium. Our results show a mixed image of the parties involved in performing informal care. Whereas the professional carers mentioned only females as informal carers, the informal carers themselves reported the involvement of a network of informal carers that included males and females. This involvement of a non-gender-specific informal care network is not in line with Van Wezel’s study (2016) of non-European migrants in the Netherlands. On the other hand, Jacobs, Van Tilburg, Groenewegen, & Van Groenou (2014) showed the invisibility of the sub-networks of caregivers and their importance in providing informal care. Moreover, several other cultures appear to have different definitions of ‘primary caregiver’ and to view care as belonging within a family system (Janevic & Connell, 2001). Our participants confirmed culture and religion (Johl et al., 2015) as motivators for caring for seniors with dementia, yet they also included emotional and practical reasons as equal motivators. Being a second-generation migrant (Lawrence, Murray, Samsi, & Banerjee, 2008) can explain the emergence of less traditional views of informal care held by a majority participants.
Our results suggest a third invisible factor underlying the non-use of professional dementia care. Dementia care options are inaccessible (Gillespie, Harrison, & Mullan, 2015) and unused (Moriarty, 2015) by informal carers for reasons that are not always evident to the professional carers. In line with the findings of De Graaff, Mistiaen, Devillé, and Francke (2012), we find that the lack of culture-sensitive and person-centred approach deters Moroccan informal caregivers from seeking professional care, even though doing so would likely relieve their burden. Language barriers, lack of awareness about dementia and stigma about the condition, as well as negative experiences with dementia services, contribute towards poor access to dementia care (Moriarty, 2015). These aspects, in addition to stereotyping and racism among professionals, result in delays in use of dementia services. These aspects can explain the third mutual invisibility of help and care options of informal and professional carers. Our findings emphasize that understanding these underlying elements is critically important for developing more effective culturally sensitive care (Cipriani & Borin, 2014; Johl et al., 2015; Mukadam, Cooper, & Livingston, 2011).
Finally, our findings confirm previous studies which found that migration (Jutlla, 2015) in addition to culture (Cipriani & Borin, 2014; Ivey et al., 2013) and religion (Regan, 2013) influence the experience of dementia both for the older people and for their informal carers. Migration from Morocco is a critically important life event that shapes the dementia experience and the execution of informal care (Jutlla, 2015). The ‘ethnic minority’ status of Moroccan older people and their offspring and their experiences of discrimination influence their reluctance to turn to professional care (Jutlla, 2015; Mukadam, Cooper, & Livingston, 2011). Being Belgian and of Moroccan background is a key cultural aspect influencing the experience of dementia and the execution of informal care (Regan, 2013). Regan (2013) argues that research should consider religion as a distinct part of culture to discover any overlooked aspects. The majority of our participants were not aware, however, of the interplay between migration, culture and religion as influencing factors of the dementia experience.
Results suggest several implications for practice. The invisibilities described by the informal and formal caregivers highlight the importance of further research to identify these invisible realities within our societies. Dementia should be made visible as a condition through investing in awareness and education programs for (potential) informal carers (Ivey et al., 2013) and by investing in culturally sensitive diagnostics for professional carers (Nielsen & Waldemar, 2015). It is also necessary to invest in actions to strengthen the relationship between informal and formal carers (Gillespie et al., 2015). This can be achieved by investing in the cultural competence of the dementia care services. There is also need for more culture-, religion- and migration-sensitive dementia care services that do not lose the individual approach to migrants with dementia (Gillespie et al., 2015; Regan, 2014). More suitable care option can further aid the informal carers in fulfilling their care role by reducing the risks that the carer will suffer adverse consequences from the care burden.
Study limitations and further research
Our findings should be considered in light of the following limitations. This study uses a relatively small sample with a concentration of informal caregivers from Antwerp, which makes generalizing the findings difficult (Moriarty et al., 2014). Also, these informal carers are mainly female, highly educated and second-generation migrants. Inclusion of males and first-generation carers from various socio-economic backgrounds is needed in future research (Johl et al., 2015). Inclusion of the immediate experience of persons from migration backgrounds who have dementia is also needed to present a fuller picture of the overall experience of dementia.
Conclusion
Our findings confirm the universality of the experience of dementia alongside specific social-contextual aspects. For older adults with migration background and their family carers, this experience is influenced by their migration history, culture and religion. We now see a first generation of informal and professional caregivers in Belgium who are confronting how to deal with this migrant group of seniors with dementia. The mutual invisibilities and mismatch of expectations appear to undermine the search process for appropriate dementia care for these older persons. In order to establish positive and effective migration-, culture- and religion-sensitive dementia care, it is necessary to integrate these different perspectives. This requires further research on practical actions in which the parties collaborate and a care policy that endorses this innovative approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.