
Abstract
Background and objectives
Behavioral and psychological symptoms of dementia are highly prevalent, stressful, and challenging to manage. Caregivers’ approaches for handling these behaviors have implications for both care partners’ well-being. Yet the specific strategies that caregivers use in their daily management of behavioral and psychological symptoms of dementia are relatively unknown. This study used in-depth focus group data to examine family caregivers’ strategies for managing behavioral and psychological symptoms of dementia.
Design
As part of a larger study (NINR R01NR014200), four focus groups were conducted with a total of 26 family caregivers of older adults with dementia. Caregivers were asked to describe the strategies they use to manage behavioral and psychological symptoms of dementia. Data from audio-recorded sessions were transcribed, coded to identify relevant concepts, and reduced to determine major categories.
Results
Caregivers managed behavioral and psychological symptoms of dementia through (1) modifying interactions within the care dyad (e.g., simplifying communication); (2) modifying the care environment (e.g., using written prompts); (3) activity engagement; (4) humor; (5) self-care; and (6) social support.
Conclusion
Family caregivers manage behavioral and psychological symptoms of dementia using strategies to minimize stress and address the needs of both care partners. Caregivers’ own accounts of these approaches reveal a window into their everyday management of difficult behaviors. The present findings generate key information for routine clinical care and targeted interventions to promote caregiver well-being.
Keywords
Introduction
Behavioral and psychological symptoms of dementia (BPSD) pose significant challenges for the well-being of persons living with dementia (PLWDs) and their family caregivers. BPSD such as psychomotor agitation, sleep disturbances, and delusions have been associated with elevated caregiver burden and depression, along with excess morbidity, nursing home placement, and earlier mortality among PLWDs (Kales, Gitlin, & Lyketsos, 2015). Caregivers vary in how they manage and cope with BPSD (Kales et al., 2015). Nevertheless, little is known about the specific strategies that caregivers use in their everyday management of these behaviors. Gaining greater knowledge of these strategies would inform the design of targeted interventions to sustain both care partners’ optimal health and functioning. This study used in-depth focus group data to examine family caregivers’ perspectives on the strategies they use to manage BPSD.
Although BPSD arise from underlying neurodegeneration, their presence and severity are often influenced by interacting characteristics of the PLWD (e.g., fatigue, physical illness), the caregiver (e.g., ineffective communication), and the environment (e.g., lack of routine or activity; Kales et al., 2015; Sink, Covinsky, Barnes, Newcomer, & Yaffe, 2006). Consequently, theoretical frameworks have been developed to guide caregivers in the use of psychological, social, and environmental strategies to manage these behaviors. The progressively lowered stress threshold (PLST) model proposes that dementia gradually diminishes the PLWD’s capacity to cope with stressors that are internal (e.g., pain, impaired communication skills) and external (e.g., noise overload, interpersonal conflict) as a result of declines in their cognitive, affective, and functional abilities (Hall & Buckwalter, 1987; Smith, Gerdner, Hall, & Buckwalter, 2004). In turn, BPSD may occur when the PLWD encounters stressors that exceed his or her coping threshold. Consistent with this perspective, research has found that caregivers manage BPSD in part by adapting the social or physical environment in ways that minimize the PLWD’s exposure to stressors (Moore, Ozanne, Ames, & Dow, 2013). Similarly, other studies show that caregivers with nonconfrontational approaches to BPSD that are sensitive to the PLWD’s level of functioning (e.g., not challenging his or her understanding of events or situations) report more effective management of these symptoms and less decline in feelings of competence than those who use corrective or punitive tactics which could amplify stress within the care dyad (Colling, 2004; de Vugt et al., 2004; Harvath, 1994).
Complementing the PLST model, the need-driven dementia comprised behavior (NDB) model holds that BPSD are partly attributed to unmet physical, psychological, and social needs (Algase et al., 1996; Colling & Buettner, 2002). Dementia-related cognitive and social difficulties increasingly lead PLWDs to express their needs through various behaviors. In accord with this model, previous research demonstrates that caregivers recognize these needs and commonly manage BPSD through engaging the PLWD in enjoyable activities (e.g., exercise, socializing) or ameliorating physiological discomfort (e.g., cold, hunger; Harvath, 1994; Huis in het Veld et al., 2016; Moore et al., 2013).
It is important to enhance further understanding of caregivers’ views about how they manage BPSD for at least three reasons. First, the few studies on this topic have limitations including a focus on behavior-specific management (e.g., wandering, passivity; Colling, 2004; Dodds, 1994) and the consideration of general response orientations (e.g., being calm, patient, or positive) more than distinct strategies (e.g., using written prompts; de Vugt et al., 2004; Harvath, 1994; Huis in het Veld et al., 2016; Turner et al., 2015). As a consequence much remains unknown about particular approaches that caregivers use to manage a range of behaviors. Second, prior studies have primarily used individual interviews. Although this work has made key contributions, research examining an in-person focus group for Latino caregivers and an online caregiver focus group suggest that interviewing caregivers about managing BPSD among their peers generates candid and nuanced information may extend beyond what is shared during one-on-one interviews (Huis in het Veld et al., 2016; Turner et al., 2015). Finally, even caregivers who report knowing how they should respond to BPSD, in theory, have trouble putting these skills into practice (Huis in het Veld et al., 2016). Caregiver reactions to BPSD in daily life may therefore not align with prior education or knowledge about dementia, underscoring the value of capturing their own accounts of everyday strategies to manage these behaviors.
The present study examined family caregivers’ perceptions of the strategies they use to manage their relative’s BPSD. We extend the literature by using data from face-to-face caregiver focus groups, which enable spontaneous responses and allow caregivers to build on one another’s thoughts and reflections in a supportive social context.
Methods
A total of 26 family caregivers participated in four focus groups that were part of an NIH-funded project (NINR R01NR014200) to develop a web-based caregiver tool for assessing and managing BPSD (Kales et al., 2017). This project was approved by the University of Michigan’s Internal Review Board (HUM00066639). Caregivers were recruited from a variety of settings including outpatient clinics and local senior resource centers by (1) responding to fliers; and (2) staff referrals. Participants were eligible if they were primary caregivers of a relative with dementia. Caregivers provided written informed consent and completed a brief survey on sociodemographics, caregiving characteristics, and technology use before the group meeting.
An experienced facilitator led each group. Three groups included 5 caregivers and one group had 11 caregivers. Using an outline developed by the research team, participants were asked about their: (1) perceived need for psychoeducation about BPSD; (2) language used to describe BPSD; (3) opinions about medication versus behavioral management; and (4) related communication and experiences with providers and family members. Specific to the present study, caregivers were asked to discuss the strategies or approaches they use to deal with their relative’s challenging behaviors. Sessions lasted for roughly 90 minutes, were audio-recorded, and were later transcribed and verified for accuracy. The facilitator instructed participants to be respectful of one another’s opinions and vulnerabilities. Caregivers were reminded that they had the option to withdraw at any time for any reason, including focus group discussions that made them feel uncomfortable. No concerns were voiced, and many caregivers commented that they found the focus groups to be interesting and informative. None of the caregivers described unethical approaches for managing BPSD.
Content analysis was used to determine categories of caregivers’ strategies for managing BPSD. Six study team members (CAP, LMS, BS, MT, BB, and HCK) coded transcript data from four focus groups in succession during one in-person meeting. An all-inclusive data table technique in Microsoft Excel was used to code and analyze the data contained in separate spreadsheets for each focus group with seven row headings: transcript number, outline section, question asked, participant response, notes, code, and category (Guest & MacQueen, 2008; Watkins, 2012, 2017). The team coding session was led by BS, who has had extensive training and experience using this technique. Rigorous and accelerated data reduction (RADaR) was used to efficiently produce results (Watkins, 2012, 2017). Open coding identified concepts associated with caregivers’ approaches for managing BPSD. The coded data were then reduced by the first author to determine major categories of caregivers’ management strategies. All co-authors separately provided feedback on the categories. Minor differences of opinion were discussed and resolved among the authors as a group.
Results
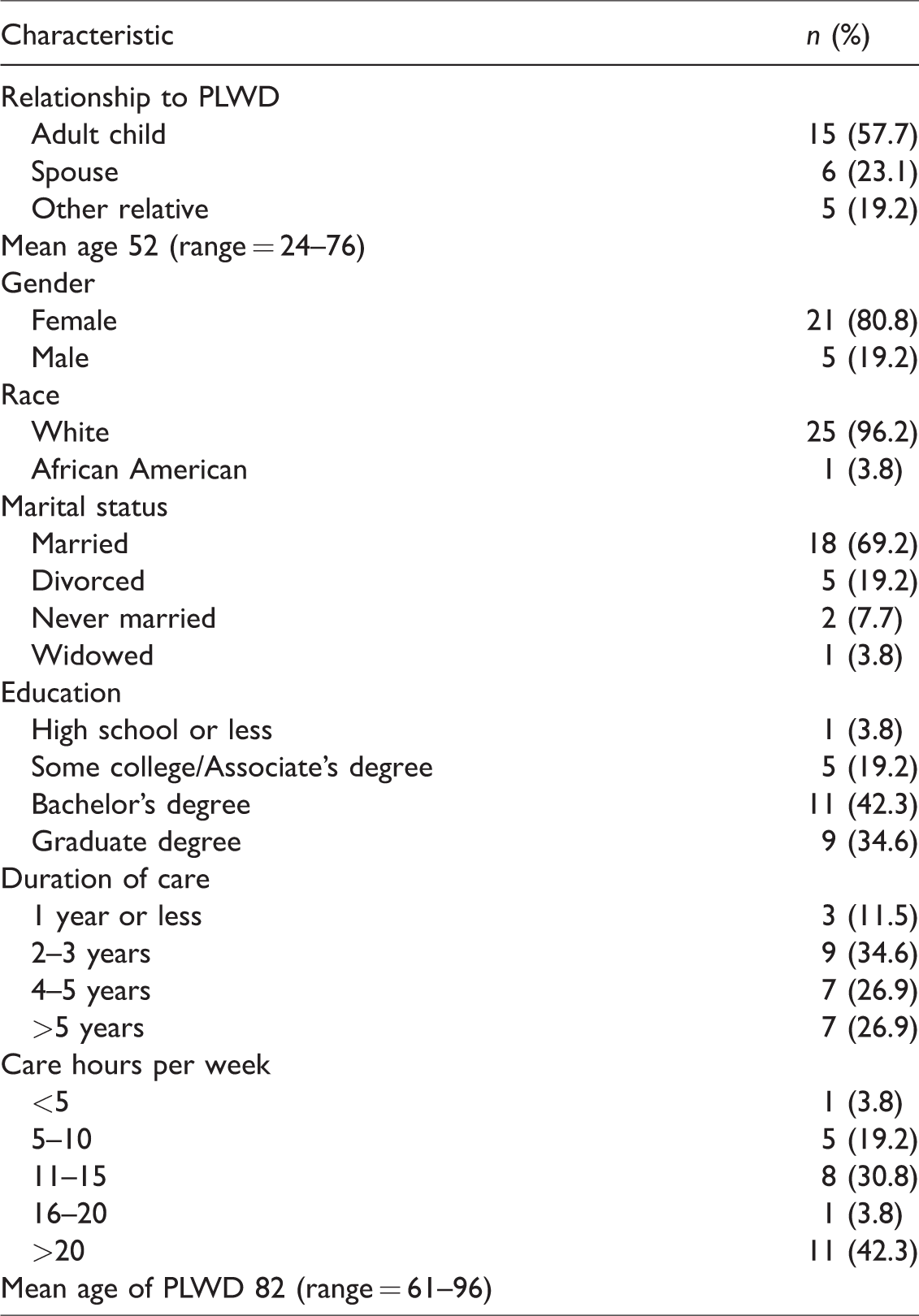
Table 1 shows background characteristics for the 26 family caregivers. The majority of caregivers cared for a parent, provided care for at least 2 years, and gave over 10 hours of care per week. Most were women, married, and White, with a college degree or higher.
Background characteristics for family caregivers of persons living with dementia (PLWDs) (N = 26).
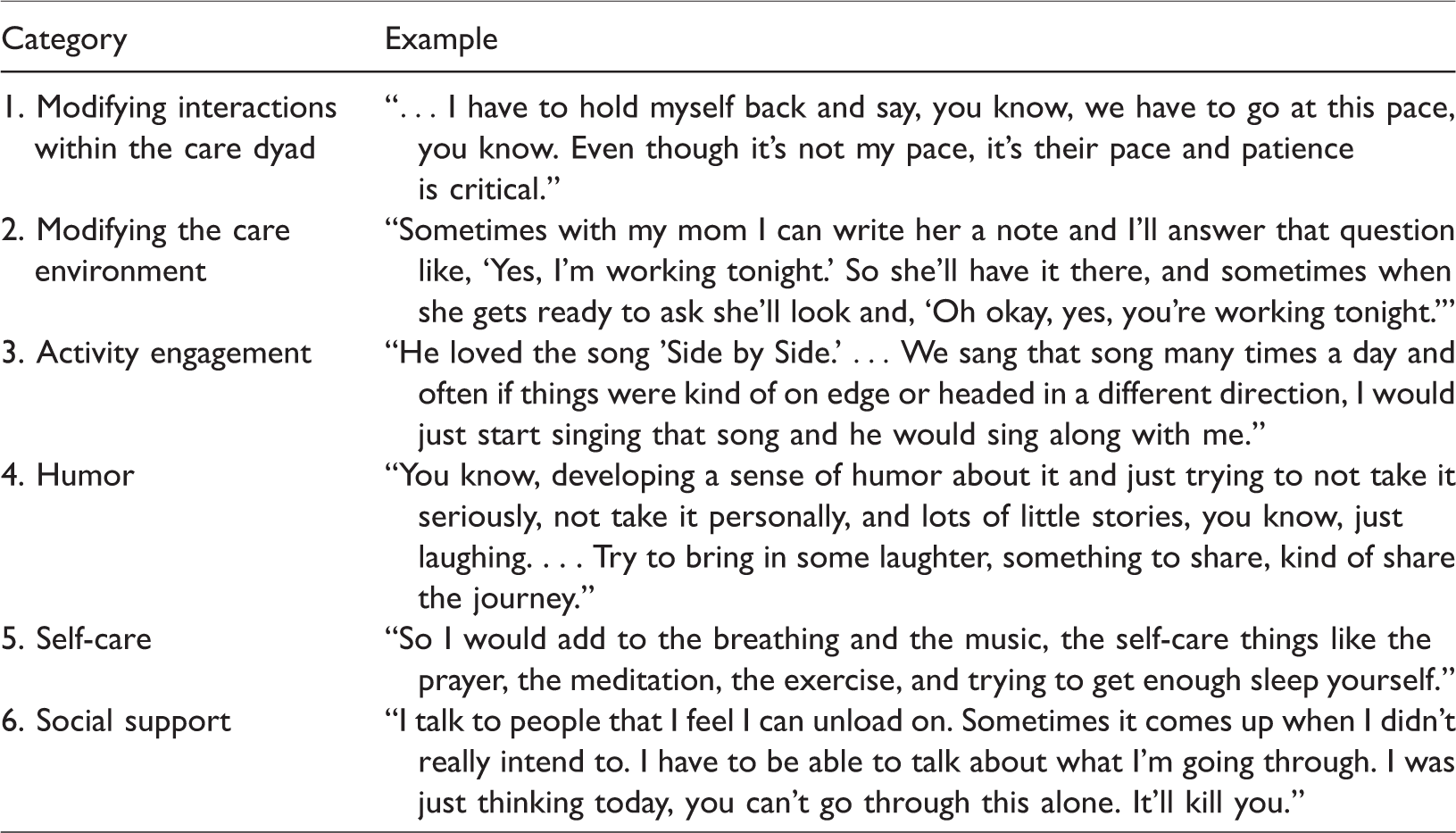
Six major categories were determined (Table 2). Caregivers managed BPSD through (1) modifying interactions within the care dyad; (2) modifying the care environment; (3) activity engagement; (4) humor; (5) self-care; and (6) social support.
Major categories of caregivers’ strategies for managing behavioral and psychological symptoms of dementia.
Modifying interactions within the care dyad
Many caregivers adapted their interactions with the PLWD to accommodate his or her changing needs, such as moving at a slower pace: But the big thing that I learned was I had to slow down. I have to slow down in dealing with that person that’s afflicted, and what I found in staff at the assisted living and staff in a nursing home is the people that are the management probably loves them because they are fast. They get things done. That don’t work when you’re dealing with people with Alzheimer’s, it’s going to be a major setback. (Participant 2, Group 2) … I have to hold myself back and say, you know, we have to go at this pace, you know. Even though it’s not my pace, it’s their pace and patience is critical. (Participant 3, Group 2)
Some of these strategies accounted for the PLWD’s predementia characteristics: My dad was an engineer, and the caregivers all recognize the engineer type, really logical … . So I had to learn to recognize situations where he wanted to know why something was happening or what was going on, and often I couldn’t tell him. I tried the real reason and it just, it didn’t compute for his situation. So I try to find a way to fit it into some framework, just step by step by step, like a three- or four-step thing… . “Well you see there’s cars out there”, and that could be a redirection already at that point but if not, “and they have to park someplace and so they’ve developed this parking,” and he was very, and you know, then I get the “Oh it’s so wonderful that you know these things,” he would say. (Participant 2, Group 3)
Caregivers also simplified their communication with the PLWD: That’s how we ended up, we just went on a toddler level with my mom. Everything was simple, short like direction, short instruction. (Participant 5, Group 3)
Several caregivers learned to avoid challenging BPSD that are harmless: I’ve learned to just go with the flow with her, you know, and not challenge her. I have tried in the past to sit down and logically explain things like, you know, like, “No, there’s no one breaking into your house, you don’t have to hide your purse,” and this and that. It doesn’t really get me anywhere. So I’ve just learned to go with whatever she says because you know it works. Then she doesn’t get angry because you’re not challenging her, and it really doesn’t matter in the long run. (Participant 2, Group 4) She goes in and out of her purse. Who is she bothering, what is she hurting? Let her go in and out of her purse. (Participant 3, Group 4) She watches the golf channel because that is comforting to her. Then what’s humorous about it is she thinks that it’s my brother playing golf. So Jack Nicholson made a boo-boo and she says, “I told him to get new shoes.” She figures it’s my brother so I do not challenge her, that’s my brother. As long as it makes her happy, I’m at the point of what makes her happy. (Participant 5, Group 4)
Others remarked that they occasionally need to walk away or disengage from the PLWD: This is where I have to walk away sometimes. In the last two years, I have learned more about patience than I learned in the rest of my lifetime. (Participant 2, Group 1) Breathing, really, I mean besides sense of humor which I think is critical. Just take a breath, just before you scream or you do something that you’re going to regret I try to remember to breathe. Take a deep breath. (Participant 3, Group 2)
Confrontational strategies such as arguing were considered to be ineffective: What doesn’t work great is the whole force, raise your voice, get frustrated, just like a toddler. (Participant 4, Group 4)
Modifying the care environment
Caregivers used environmental strategies to prevent BPSD, such as a daily routine: I think another thing was just having a routine for my grandma. Because when things happened that weren’t in her normal routine that seemed to either make her way more anxious or way more aggressive, depending on where in her illness she was. So the more that we could do that, just stayed in a routine pattern, the smoother things seemed to go. (Participant 4, Group 3) She gets so much pleasure just that’s part of her routine. Reading that paper, she goes out to the mailbox, she gets it, she reads it. (Participant 2, Group 4)
Additionally, prompts or tools were used to proactively manage BPSD: Sometimes with my mom I can write her a note and I’ll answer that question like, “Yes, I’m working tonight.” So she’ll have it there, and sometimes when she gets ready to ask she’ll look and, “Oh okay, yes, you’re working tonight.” That so far has worked for me because she still reads and all of that, so that works so far. (Participant 3, Group 4) We put black tape over all the buttons that shouldn’t be used. Some red duct tape over one button and green over the other two buttons that you had to push and then a big card on top that said, “To turn it on, push green button one and then green button two. To turn it off, push the red button.” (Participant 2, Group 3) Like, you know, the wandering at nighttime, of course we were concerned about getting out of the house so we put on the extra locks on the inside that she couldn’t reach, you know… . Like the preemptive things like you would do with, you know, with thinking about again like going back to thinking about kids and childproofing your house. (Participant 5, Group 2)
One caregiver observed that these strategies help the PLWD retain a sense of control: What I’ve seen is, like, if I can get the food onto say a spoon say for him, he will pick it up and he will feed himself but really slow… . It’s struggling to think what can they do and how can you make it, what environment can you create so they can do something? So that they still have that sense of control that I’m able to do this. I think that’s just critical. (Participant 11, Group 3)
Caregivers also described their use of distraction strategies in response to BPSD: I would say that one of the things that we used was the same thing that you might use if you raised children, which was that if there was something that was upsetting that person you could try to distract them or change the subject, change the venue, whatever. So if there’s something going on over here that’s causing, you know, your person to be upset or frustrated to find a way to, you know, introduce something new or to even change the visual, and that sometimes did work. (Participant 5, Group 2) Or the other thing is by distraction. Try to get them on to something else, you know. Like, once my mother was doing this kind of behavior [banging on the table]. And the thing is like, okay, just get her away from that environment, whatever it’s doing and then do something like, “Oh how about we go down to the room and you get some ice cream?” “Oh okay.” So you know, you just use distraction and try but it doesn’t always work. (Participant 5, Group 4)
Activity engagement
Caregivers encouraged the PLWD’s participation in activities to prevent or attenuate BPSD, such as those involving music: I’ve used music, too, with my wife. She has been in a choir for a long time, and I just very recently decided maybe it’s time that she stopped going because I don’t think anybody in the choir would ever tell her that she shouldn’t come. But I put on CDs of their concerts, and really she starts singing along. (Participant 1, Group 2) He loved the song “Side by Side.” … We sang that song many times a day and often if things were kind of on edge or headed in a different direction, I would just start singing that song and he would sing along with me. (Participant 2, Group 3) The other thing that works very effectively at least with my mom is song and dance. I think the music, you can just go back to the old songs. She knows all the old prayers, she can do the rosary, and she can recite every old song. So when you’re asking her to do something, if you just break out into a silly song she doesn’t realize then that she’s doing what you’re asking her to do. (Participant 4, Group 4)
Other caregivers found activities for the PLWD that were perceived to promote feelings of usefulness or reflect their predementia interests and identities: The same thing with stories, my mother had been a school teacher, and many times one room schools years ago… . So Dr. Seuss, the books. So if I take the books in with my granddaughter and I read books, because she taught reading she can connect with that. (Participant 5, Group 4) One of the suggestions from the support group I’m in at [De-identified location] was to find projects for them to do, busy work. One of them is they let them fold towels and then they throw them all out and then they let them fold them all over again. For men, sorting nuts and bolts. Any type of busy work, some people like to sweep the floor. Some people like to clear the tables. Allow them to continue to be useful. (Participant 8, Group 3) She was a great mom, you know, and that’s what she did. She washed the clothes and the whole dishwasher. I still think she feels like a successful person when she can do those things. So yeah, she’ll wash things over and over and over but in her mind she’s doing something constructive and it makes her happy, so his water bill goes up. (Participant 2, Group 4)
Humor
Several caregivers communicated the importance of maintaining a sense of humor: You know, developing a sense of humor about it and just trying to not take it seriously, not take it personally, and lots of little stories, you know, just laughing… . Try to bring in some laughter, something to share, kind of share the journey. (Participant 3, Group 1) One hell of a good sense of humor and it came from both me, my parents, my dad and then I could play off of it. Definitely humor, oh my gosh, humor and just a sense of keeping first and foremost. They’re human beings, I love them dearly, and I’m going to do the best I can for them with the way they are right now. (Participant 4, Group 2) Well humor. My dad was a joker … but I have to do that for my own sense of sanity. I taught kindergarten for 20 years, so I would try to remind myself that some of the things I would use with a four-year-old are actually very helpful in dealing with someone with dementia. (Participant 10, Group 3)
Self-care
Caregivers also relayed the necessity of self-care and taking time away from caregiving: So I would add to the breathing and the music, the self-care things like the prayer, the meditation, the exercise, and trying to get enough sleep yourself. All of those kind of on a day-to-day basis to kind of, you know, to be able to hit the ground running the next day, but then also to be able to just have that reminder to yourself that looking at your loved one knowing that this is the disease and not them… . (Participant 5, Group 2) Well exercise, that helps to clear your mind some because sometimes you really don’t have many other options. I mean I try to do things so I have breaks, but you don’t always get them. So you have to, you know, it really is a lot of taking each day one at a time and just trying to make do with what you’ve got, I think a lot of times to get away. (Participant 5, Group 1) …But just to get away, just to go to the store, just to not have that, go to the library. Anywhere that you can go when you get an opportunity you need to take it and to leave that situation for as many minutes or an hour, whatever you can get. It’s hugely important. It’s overwhelming. (Participant 4, Group 1) There are times when you need to get out yourself in order to cope with it. I don’t know what else to say. (Participant 5, Group 4)
Social support
One caregiver mentioned the role of family and paid helpers in managing BPSD: We’ve been able to split off, relatives have helped. I used to take up weekends with my mom. I’d go down Friday night after work and stay till Sunday night and come home. Then she had some extra paid help picked up during the week… . (Participant 1, Group 1)
Other caregivers emphasized the need for emotional support and understanding: There’s so few people that really understand Alzheimer's and it’s nice to sit down like this group, with a group of people that really do understand what you’re going through and can be helpful to you. (Participant 8, Group 3) I talk to people that I feel I can unload on. Sometimes it comes up when I didn’t really intend to. I have to be able to talk about what I'm going through. I was just thinking today, you can't go through this alone. It’ll kill you. (Participant 1, Group 2)
Caregivers also noted the significance of feeling validated by others’ experiences: Or even later on to discuss it can ease some of the sting of it. And to understand, you know, to have the feedback that it isn’t you, it isn’t her, it’s this issue. (Participant 4, Group 1) Knowing you are not in this by yourself and that when you, you know, here I am just retiring and I'm dealing with this every single day because I'm the only one that can and I'm angry because, you know, I raised my kids, I did my job, I did everything I'm supposed to do. And now this is supposed to be my time, and boom, I've got my parents. I'm really not real happy about that, and there was a guy that sat at one of our support groups and he just looked at me and he goes, “You know, I'm really mad about this,” he was speaking to the whole group and I thought I'm not crazy, I'm not the only one, I don’t have to feel guilty that I feel this way… . (Participant 4, Group 2)
Lastly, caregivers discussed the need to combat feelings of isolation: … I think that there’s such isolation for the caregiver because you often don’t have someone to talk to unless you have a large family. I tend to not have friends that, they don’t want to hear anything that you are doing this. You know, it’s like you see the glazing over pretty quickly and it is hard. I’ve always thought with support groups, you know, something that meets once a month doesn’t do much good. You almost need something that you can drop in or call in or something like that. (Participant 5, Group 1)
Discussion
The present study sheds light on the everyday strategies that family caregivers use to manage BPSD. In accord with the PLST and NDB models, caregivers modified interactions within the care dyad and the care environment to minimize stressors and address the PLWD’s unmet needs. Caregivers also expressed the value of humor, self-care, and social support in coping with the day-to-day challenges of difficult behaviors. The focus group approach used in this study expands the literature by interviewing caregivers among their peers, generating unique insights for interventions to mitigate caregiving stress.
Similar to other studies (e.g., Harvath, 1994; Huis in het Veld et al., 2016; Moore et al., 2013; Turner et al., 2015), caregivers adapted their interactions with the PLWD to fit his or her current functioning. Strategies included moving at a slower pace, simplifying communication, allowing BPSD to occur when they pose no harm, and refraining from challenging the PLWD’s beliefs. Such approaches may help to prevent distress for both care partners by avoiding unnecessary confrontation. As proposed by the PLST model, these strategies may also decrease BPSD through reductions in stressors that contribute to their occurrence (Hall & Buckwalter, 1987; Smith et al., 2004). Some caregivers indicated that they learned to modify how they interact with the PLWD over time as they realized their confrontational tactics (e.g., arguing) were unsuccessful. Indeed, caregivers who use punitive or confrontational strategies to manage BPSD report similarly negative reactions (e.g., resisting, becoming upset) from the PLWD (Song, Park, Park, Cheon, & Lee, 2016). This implies that education in the use of effective interaction strategies may be beneficial for caregivers early in the disease process.
Many caregivers discussed how they modified the care environment to manage BPSD. These modifications included maintaining a daily routine and using prompts to prevent problem behaviors. Such strategies are proactive and demonstrate caregivers’ recognition of BPSD as need-driven behavior. Caregivers also applied creativity and problem solving to maximize the PLWD’s strengths and capabilities, indicating their perceptions that he or she retains needs for autonomy and control. Environmental strategies that minimize potential triggers of BPSD can reduce their frequency (Kales et al., 2015). Consequently, these antecedent approaches may help to alleviate stress for PLWDs as well as their caregivers. By contrast, several caregivers observed that distraction strategies used in response to already occurring BPSD were not always effective. Taking the PLWD to get ice cream or engage in another pleasant activity when BPSD occur, for instance, could backfire by accidentally reinforcing these behaviors. Distraction strategies may also be limited to short-term reductions in BPSD or result in a constant need for redirection that is exhausting for caregivers (Moore et al., 2013; Song et al., 2016). Hence, caregivers could benefit from clinical guidance in the application of environmental modification strategies that are more or less likely to be successful.
In line with previous studies (de Vugt et al., 2004; Moore et al., 2013), a number of caregivers compared their management of BPSD to caring for children. Analogies to childcare may be useful in building on caregivers’ patience and empathy toward the PLWD. Furthermore, such comparisons could help caregivers draw from established skill sets (e.g., caregivers who are parents or have experience working with children) to more effectively manage BPSD. It is important to ensure, however, that caregivers with a nurturing orientation are not inclined to provide support over and above what the PLWD requires. Performing care tasks (e.g., dressing or eating) that the PLWD is still capable of completing independently, for example, may lead to excess disability (Verbugge & Jette, 1994).
Encouraging activity participation was mentioned as another approach to managing BPSD, aligning with prior work (Harvath, 1994; Huis in het Veld et al., 2016; Moore et al., 2013). Caregivers in this study used singing and dancing to engage the PLWD, along with activities that may promote his or her sense of usefulness or predementia identify. Activity-based strategies offer a host of potential advantages such as improving the PLWD’s mood, facilitating needed stimulation, and providing purposeful occupation, all of which may attenuate BPSD (Gitlin et al., 2008; Kolanowski, Fick, & Buettner, 2009; Teri & Logsdon, 1991). These approaches may also preserve core aspects of the PLWD’s personhood and help to sustain an emotional connection between care partners throughout the disease course.
Humor appeared to be a critical resource in managing BPSD for several caregivers, perhaps as a means to lighten the serious nature of dementia and reduce the tendency to feel hurt or offended by the PLWD’s upsetting behaviors (Dodds, 1994; Huis in het Veld et al., 2016). Having a sense of humor may also help caregivers keep a balanced perspective on dementia-related challenges and likely counteracts care-related stress. Additionally, humor may provide a way for caregivers to maintain positive elements of their predementia relationship with the PLWD (e.g., sharing a laugh).
Caregivers also stressed the centrality of self-care in their management of BPSD. Strategies such as participating in valued noncare activities, upholding healthy habits (e.g., getting adequate sleep and exercise), and taking a break from caregiving may restore caregivers’ emotional and physical capacity to handle the PLWD’s behavioral difficulties. Notably, research shows that caregivers have less exposure to care-related stressors, lower negative affect, and better cortisol regulation on days when the PLWD uses adult day services, suggesting that respite from caregiving offers a multitude of benefits (Leggett, Liu, Klein, & Zarit, 2016; Liu, Almeida, Rovine, & Zarit, 2016; Zarit, Kim, Femia, Almeida, & Klein, 2014). Similarly, whereas care-related activity restriction is linked to caregivers’ poorer mental and physical health, making time for social and leisure activities has been found to buffer caregiving stress (Chattillion et al., 2013; Mausbach et al., 2011; Schüz et al., 2015).
Lastly, caregivers emphasized the role of social support in managing BPSD. In particular, the caregivers in this study voiced their desire to meaningfully connect with peers who also care for a PLWD. This suggests that caregivers can serve as a crucial resource for one another by validating each other’s feelings, combating isolation, and sharing ideas for dealing with difficult behaviors. As one caregiver implied, support groups may be most useful in coping with BPSD when they involve frequent contact and facilitate opportunities for connecting outside the group to exchange ongoing emotional aid or practical assistance (e.g., stopping by to stay with the PLWD while the caregiver goes shopping).
This study has several limitations. First, caregivers were homogeneous in their sociodemographic characteristics and care situations, limiting generalizability. On average, the sample was highly educated and may use different strategies for managing BPSD than caregivers with lower education. Caregivers were also mostly women and adult children caring for a parent, consistent with current reports of dementia caregiving (Alzheimer’s Association, 2017). Future research should consider management strategies among more diverse types of caregivers. Second, the sample was self-selected and relatively small, which could introduce potential bias. Third, the retrospective appraisals assessed in this study may not represent the full spectrum of strategies that caregivers use in their real-time responses to BPSD. Fourth, among their peers, caregivers may have been more likely to highlight positive management strategies than more negative or punitive approaches. Nonetheless, the findings lay the groundwork for future research to delve more deeply into the everyday approaches that caregivers use to manage BPSD and their implications for both care partners.
In summary, the present study reveals that caregivers use a variety of strategies to avoid BPSD or lessen their impact. These approaches appear to be largely based on the perceived needs of each care partner, yet the findings suggest that routine clinical visits should include guidance in their implementation and evaluation. Elucidating understanding of how caregivers manage BPSD in their daily lives will inform the development of tailored interventions that more fully incorporate both care partners’ evolving needs and preferences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute of Nursing Research (R01NR014200). The funding organization had no role in any of the following: design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review, or approval of the manuscript. Courtney A. Polenick was supported by training grant T32 MH 073553–11 from the National Institute of Mental Health (Stephen J. Bartels, Principal Investigator). Additional support was provided by the University of Michigan Program for Positive Aging (Helen C. Kales, Director).