
Abstract
Dementia has been identified as one of the major challenges in the 21st Century. The detrimental effects of dementia can jeopardise personhood, thus person-centred interventions including reminiscence and arts practice have been recommended as tools to promote social inclusion and improve the quality of life. This study aimed to evaluate the effectiveness of group reminiscence arts sessions for people living with dementia in care homes (residential and nursing homes) using a comparative and time series design to collect data on quality of life. The intervention was conducted in six care homes in London over a period of 24 weeks and compared with six care homes not receiving the intervention (control). Dementia Care Mapping was used as the primary data collection instrument to measure positive behaviours and rate quality of life before, during and after group reminiscence arts sessions. The evaluation team observed the sessions at three-weekly intervals. Statistical modelling found that positive behaviours and quality of life of care home residents participating in group reminiscence arts sessions increased over the 24-week period. Well-being increased sharply during each session and plateaued at 50 minutes with a sustained positive effect after the sessions. On a longer timescale, well-being and quality of life increased slowly and steadily from one session to the next. The findings were statistically significant (p < 0.001). The study concludes that group reminiscence arts sessions can have a positive and sustained impact on the quality of life of people with dementia. However, the evidence on the sustainability of the effect over time remains unknown. More research is needed to assess in much greater depth the association between quality of life and group reminiscence arts sessions.
Introduction and background
Critical dementia researchers have demonstrated that models of research that focus solely on brain function tend to isolate individuals from the wider social environment (Dumit, 2004; Whitehouse & George, 2008). Person-centred care for people with dementia was conceived in the 1980s and challenged the dominant medical model of the condition to a more psycho-social approach (Kitwood, 1997). Person-centred care offers an alternative to care that was primarily task-centred, and recognises the social and personal implications of the condition. According to Brooker (2003, p. 217), person-centred care aims to:
“value people with dementia and those who care for them; treat people as individuals; look at the world from the perspective of the person with dementia; create a positive social environment in which the person living with dementia can experience relative well-being”.
This paper presents findings from a study to evaluate group reminiscence arts (RA) sessions in care home settings in London, England. The primary purpose of the evaluation was to assess the impact of the intervention on the overall quality of life (QoL) of people with dementia. This paper starts with a brief review of the literature, provides an overview of the methods, presents the findings and concludes that engagement in group RA sessions proved beneficial for the psychological well-being of people with dementia living in care homes.
Recent developments in dementia care
There have been significant developments in dementia care and advancing the knowledge base about it. Two such developments will be reviewed here, i.e., person-centred and psycho-social approaches to care, and research developments in measuring the QoL of people with dementia living in care homes.
Dementia, reminiscence and arts practice
People with dementia are at risk of having their personhood compromised (Johnston & Narayanasamy, 2016; Kitwood, 1997). Psycho-social interventions such as life story work, reminiscence therapy and music therapy have been advocated to address the social consequences of dementia to maintain individuals’ QoL (National Institute for Clinical Evidence, 2006; O’Shea et al., 2014) and to bring a shift from the medicalised approach to dementia care (Dempsey et al., 2014). This supports the view of Thorgrimsen et al. (2002) who suggested that a diagnosis of dementia focuses on the illness and the symptoms associated with it, whereas an intervention such as reminiscence activities or therapy emphasises social relationships, coping strategies and stress reduction. Reminiscence therapy has also been promoted as an intervention that can relieve depressive symptoms, improve cognitive functioning and improve QoL (Innes & Surr, 2001; O’Shea et al., 2014; Smit, Willemse, de Lange, & Pot, 2015).
Evaluations and reviews of the effectiveness of reminiscence activities present mixed results. Woods, Spector, Jones, Orrel, and Davies (2005, updated in 2018) in a Cochrane review of reminiscence therapy for dementia found that the effects are inconsistent and show differences between care homes and community settings. For example, they found that reminiscence activities had some positive effect on the QoL of residents’ with dementia in care homes, whilst in community settings the benefits were associated with cognition and mood. They also suggested that the inconclusiveness of the evidence was due to methodological issues such as sample size, lack of randomisation and lack of clear protocols. However, Woods, O’Philbi, Farrell, Spector, and Orrel (2018) concluded that there is a growing body of evidence based on large-scale randomised control trials (RCT) with studies using clearly defined interventions and protocols. For example, Azcurra (2012) used a RCT design to overcome the methodological issues and found that people with dementia who participated in reminiscence groups showed significant improvements in their QoL and that the effect was sustained over time. O’Shea et al. (2014) in a randomised controlled trial of a reminiscence group for people with dementia and their family carers found that the use of reminiscence had a positive effect on participants’ QoL, but noted that the effect was short lived. However, there is agreement that people with dementia who participated in reminiscence activities reported that they enjoyed the groups and that it benefited their QoL (O’Shea et al., 2014). These authors conclude that perhaps interventions for people with dementia should be evaluated in relation to immediate effects rather than examining long-term benefits. This is pertinent given the degenerative nature of the condition.
Creative practice and the participatory arts with and for people living with different forms of dementia can play a role in improving well-being (Zeilig, Killick, & Fox, 2014). There is significant evidence that participating in the arts and creative practice has positive benefits for people with dementia. For example, the potential for the arts to deliver health and social care outcomes, often emphasising its cost effectiveness, have been documented (Buttrick, Parkinson, Wallis, Trentham, & Riseborough, 2013; Cohen et al., 2006; Hanna & Perlstein, 2008; Noice, Noice, & Kramer, 2013; Ramsey, 2013). Others have demonstrated the positive effects of the arts on the mood and feelings of social isolation of people living with dementia (Eekelaar, Camic, & Springham, 2012; Guzmá, GarcÍa, Hughes, James, & Rochester, 2013; McLean, 2011; Smith, Waller, Colvin, Naylor, & Hayes, 2012).
Measuring quality of life
Another development in building the evidence base on the most effective ways to provide support and care for people with dementia and those around them is developing research tools that capture the perspectives of people with dementia. Warner, Milne, and Peet (2010) in a review of the various measures to assess the QoL of people with dementia suggested that when data is collected directly from those affected by the condition, it can provide the ‘best’ evidence and gives an insight into their worldview. QoL is widely regarded as a social project, associated with relationality and mutual responsibility (Williamson, 2010). In this study, we have defined QoL in the terms advocated by the World Health Organisation (WHO, 1997), which includes the context in which people live, their relationships with others and their relationship with the environment.
In dementia studies, QoL can be measured using three different approaches: self-rating, proxy rating and observational methods (Fossey, Lee, & Ballard, 2002). As Algar, Woods, and Windle (2016) pointed out, observational methods can provide robust evidence for the effects of creative participation on the QoL of people with dementia who are unable to self-rate their levels of well-being due to mental capacity issues. Dementia Care Mapping (DCM) is one such observational tool (Bradford Dementia Group, 2005). DCM was originally developed as a clinical tool to improve care and inform service development, but is increasingly being used as a research tool. Sloane et al. (2007) suggested that DCM is suited to small-scale within-subjects or group intervention studies. DCM has been used to examine QoL (Ballard et al., 2001; Sloane et al., 2007) and is viewed as a reliable research tool as recommended by Fossey et al. (2002) who found that it has internal consistency and is a useful tool for intervention studies for people with dementia in residential settings (see also Cooke & Chaudhury, 2012). Sloane et al. (2007) suggested that DCM might be a closer assessment of QoL than other tools as it is rated from the perspective of the person with dementia (Algar et al., 2016).
Concerns have been raised about using DCM as a research tool to observe QoL. Methodological issues have been related to psychometric properties, sampling bias, inadequate sample sizes and short evaluation periods (Bartlett & O’Connor, 2010; Beavis, Simpson, & Graham, 2002; Fossey et al., 2002; Sloane et al., 2007). It has also been noted that there is potential to over-estimate well-being by recording the highest level of well-being (Cooke & Chaudhury, 2012). DCM captures micro changes (Lai, Chi, & Kayser-Jones, 2004) and therefore may not capture long-term effects of an intervention such as reminiscence and arts and that a more global scale such as the Social Engagement Scale (Azcurra, 2012) that measures status over time may be more appropriate. Despite these methodological issues, DCM is considered a tool that has internal consistency, acceptable face validity and captures a diversity of activity (Brooker & Surr, 2005; Cooke & Chaudhury, 2012; Fossey et al., 2002). It has been suggested that more work is needed to establish test–retest reliability of DCM (Cooke & Chaudhury, 2012).
In summary, it has been argued here that psycho-social approaches to dementia care can prove beneficial for QoL and that research methods that use observational methods can provide robust evidence on how to improve QoL for people living with dementia.
Methods
The aim of the evaluation was to assess what difference, if any, do group reminiscence arts sessions make to the QoL of people with dementia living in care homes? The study’s aim was achieved through a comparative and time series design, which gathered evidence from residents with dementia living in care homes in London, England.
The intervention
The intervention was titled Reminiscence, Arts and Dementia: Impact on Quality of Life (RADIQL). RADIQL was pioneered by Age Exchange Theatre Trust (AETT), a Charity in London, to test an innovative person-centred form of care. The intervention was aimed at promoting communication and well-being through the use of creative art forms and memory methods to connect people with dementia to their present, their social space, and others around them. The intervention comprised a range of activities that were adapted to suit individual and group needs and mainly included activities such as throwing a ball or pulling a string as ice-breaker activities. Other activities included singing, playing/touching musical instruments, painting, craft making, food, gardening, dancing and looking at photographs. Each session had a reminiscence element to it and was tailored to the likes/dislikes, needs, abilities and interests of individuals in the groups. The intervention was aimed at increasing engagement, stimulation and social interaction.
Reminiscence arts recognise and value embodied and sensory memories as well as verbal or narrative recall (Dempsey et al., 2014). The arts activities extend reminiscence practices, which often relied on verbal discussion, by involving all the senses and enabled participants to communicate non-verbally through mark making and movement. This multi-sensory approach involved practice that was responsive to the needs of participants in the study, particularly those with advanced dementia.
Group RA sessions normally lasted between one to two hours. Two creative reminiscence arts practitioners (RAPs) trained in different disciplines (e.g. reminiscence, dance and creative arts) were assigned to each of the intervention groups. RAPs co-facilitated a range of activities with people with dementia, according to their personal/group interests and needs, thus enabling participants with complex and diverse abilities to engage imaginatively in their environment in different ways. In addition, it was expected that two care home staff would be involved to support the needs of the residents in the group. Six intervention sites received the group RA sessions every week for 24 weeks.
Sampling
Care homes
Around 100 care homes (residential homes and nursing homes) were identified by AETT through a desktop search of care homes in two London Boroughs. Thirty care homes that conformed to the parameters of the research (i.e. provision of dementia services in a care home setting) were invited to participate. Of these, 15 care homes were suitable having residents with dementia. The final selection of 12 care homes was determined by availability of care homes during the study period, speed of recruitment and agreement to be part of the study. Seven care homes were from XXX and five from XX. Nine care homes were private and three were National Health Service (NHS) run. Three of the 12 care homes were run by faith-based organisations.
Six care homes were assigned to receive the RADIQL intervention, and six were designated as control sites. Randomising the selection was not possible due to uncertainties around availability within the required time frame. Instead, we ensured that all the care homes met the requirements for inclusion, i.e., that they were providing care and support for people with dementia and that there were sufficient numbers of people with dementia to be included in the study. Care homes in the control group received group RA sessions following the completion of this study; these groups were not evaluated. Care staff or activities coordinators working in the care home identified residents with a diagnosis of dementia. In instances where a resident did not have a clear diagnosis of dementia, an ICD-10 screening tool for dementia (WHO, 1992) was completed by a lead nursing or care staff member. One of the researchers then approached potential participants to introduce the project, outline what it would entail and asked whether they would like to be involved in the research. If the person had mental capacity, in accordance with the Mental Capacity Act, Her Majesty's Government (HMG, 2005), then the study was explained to them by the researcher, they were given a participant information sheet and asked to sign a written consent form. However, if the person did not have mental capacity to understand the research and the implications this had for them, their next of kin was asked to act as their consultee. If the consultee confirmed that to the best of their knowledge, before the person had dementia they would have agreed to take part in the study, and it was in their ‘best interest’, then they gave their written assent for the person with dementia to be involved in the study. In the absence of a next of kin, the care home manager acted as the residents’ consultee.
Groups
Each of the 12 care homes, whether in the intervention or control arm of the study, aimed to include six to eight participants. The size of the group was dependent on the number of residents and the stage of their dementia. If the majority of people with dementia were in the later stages of dementia then the group size was ideally six; however if participants were in the early stages of dementia then the group could include eight participants. These numbers were guidelines set out by AETT, and made for practical reasons, so that care staff and RAPs were able to safely and effectively support all participants in the group.
Data collection procedures
Demographics
Demographic information was gathered for each of the 12 care homes and people with dementia at a screening visit, which occurred just before baseline. Demographic details were used to describe the sample and to ensure that the two arms of the study did not differ significantly from each other. Demographic details included: age, gender, ethnicity and dementia type.
Outcome measures
DCM (Bradford Dementia Group, 2005) was the primary data collection tool. There is a range of tools to measure QoL, but DCM was chosen as an observational tool/proxy for QoL, because it is dementia specific, adopts a person centred approach and is focused on gaining an understanding of the subjective experience of the person with dementia. We used the DCM tool pre, during and post the intervention.
DCM (see Sloane et al., 2007 for a more detailed explanation) involves continuous observation during which a trained observer (mapper) tracks five to eight individuals for a dedicated period. DCM assesses four domains: (a) behaviour, (b) mood/engagement, (c) personal distractions and (d) positive events. For this study, coding frames used were behaviour category codes (BCC) to assess positive behaviours, and mood and engagement (ME) values to assess QoL. The BCC domain consists of 24 categories of behaviours (e.g. eating, physical exercise). ME scores use a scale of numerical values ranging from −5 (severe ill-being) to +5 (positive well-being), with a score of 1 being a neutral state of ill/well-being.
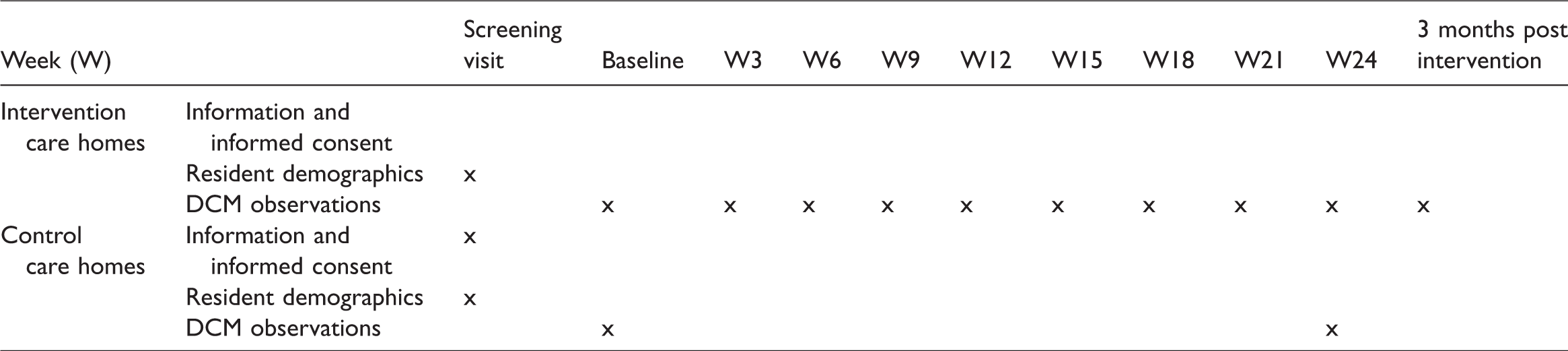
At baseline, participants in the intervention groups were observed for one hour during non-RA activity, and then observed every third week that the group RA session took place (e.g. weeks 3, 6, 9, 12, etc.). DCM was conducted for 30 minutes prior to the group RA session (in the lounge or dining area), during the group session (up to two hours) and 30 minutes after the group RA session. A three-month one hour post intervention DCM evaluation (similar to baseline DCM i.e. no RA activity) was also conducted to assess for any sustained effect from the intervention.
For the control care homes, DCM was used to observe one hour of non-RA activity at baseline and at 24-week follow-up (see Table 1 for an overview of the data collection process).
Overview of data collection process.
To reduce bias, two researchers (FK and LC) conducted an inter-rater reliability test for the DCM data. This was evaluated during a series of pilot mapping sessions where the two researchers observed the same individuals for a one-hour period calculating concordance by dividing the actual agreements score by the maximum possible score for the one-hour period. The concordance coefficient was at 90%, which was good given the suggestion that an appropriate concordance is 70% (Brooker & Surr, 2005).
Data analysis
Statistical modelling was used to look at how ME scores and BCCs changed over time, and how this differed between the control care homes and the intervention care homes. This took each individual’s severity of symptoms (in terms of ME scores and BCC’s) into account (a so-called ‘multilevel model’) at baseline and throughout and looked for average trends over time. BCCs were classified into two groups, positive (e.g. looking at photographs) and negative (e.g. withdrawn) or neutral behaviours (e.g. passively sitting), in accordance with the DCM manual (Bradford Dementia Group, 2005). All analyses were conducted using the Stata statistical package, version 12 (Acock, 2016).
Ethics
Involving people with dementia in research or evaluation raises a number of ethical concerns, and unique to this condition issues about mental capacity and the ability to provide informed consent. In line with guidance contained in the Mental Capacity Act (HMG, 2005), favourable ethical approvals were gained from the NRES Committee (London), the relevant local Research Governance Committees and the NHS Trusts in the region (REC reference: 13/LO/0903).
Results
Demographics of participants
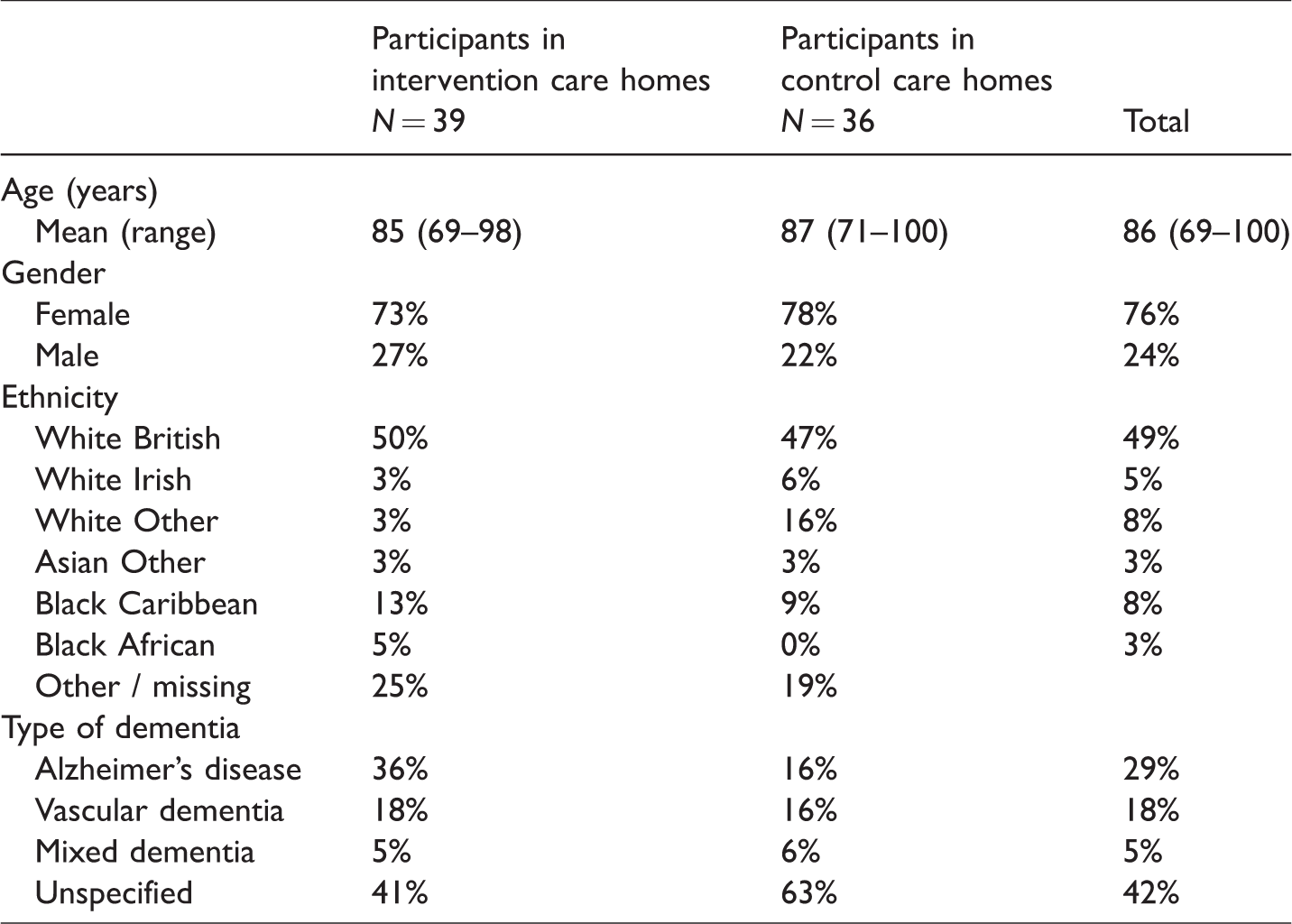
Seventy-five people with dementia participated in the study. The majority (76%) were female. Participants’ mean age was 86 years and ranged between 69 and 100 years. Although nearly half of the participants were White British (49%), there was some diversity in the group, as other ethnicities included white Irish (5%), white other (8%), Asian other (3%), black Caribbean (8%), and black African (3%). Most had English as their first language (73%); however other languages included (French, Gujarati, and Vietnamese). Concerning dementia diagnoses, nearly a third of participants had Alzheimer’s disease (29%), but 42% had an unspecified memory or cognitive problem (please note that all participants met the criteria for a diagnosis of dementia). Table 2 provides an overview of the demographics.
People with dementia demographics.
The number of participants in the groups at baseline ranged from five to eight with the mean number being seven. Attrition was observed over time as at week 24 group sizes ranged from four to eight with a mean group size of six. Reasons for attrition were: death (n = 3), moved to another care home (n = 1), and disengaged from the group RA session (n = 4).
Analysis of DCM mood/behaviour values and behaviour category codes
Measurements using DCM were recorded every five minutes, with a total of 6429 measurements. ME values were missing in 389 measurements but BCC were complete for all. At baseline there was evidence of ill-being, but during the course of the intervention there was an incremental increase in positive well-being scores.
The BCCs, dichotomised into high and low, provided us with a proportion of time in positive behaviour category codes for each participating resident. The Control groups showed more positive behaviours than the intervention groups and the difference was statistically significant. We know that other structured activities were taking place in those care homes. For example, these homes were participating in a dementia trial on person-centred practice that included activities such as reminiscence, painting, dancing which could explain the difference, particularly in view of Azcurra’s (2012) suggestion that when people with dementia are engaged in structured activity it is likely that their QoL will improve.
Regression models
Mood/engagement scores
The control arm of the study had significantly higher ME scores at baseline by a mean of 0.64 points (95% CI 0.28 to 1.00, p < 0.001). During each intervention, the ME scores of participants rose and levelled off according to the formula

Each activity (spaced three weeks apart) in the intervention group saw a steady increase in ME scores of 0.019 points on average (95% CI 0.014 to 0.024, p < 0.001). At 24 weeks, the control groups were not statistically significantly different to baseline, with an average change of −0.077 (95% CI −0.308 to 0.153, p = 0.51). At follow-up, the intervention groups were not significantly different to baseline (mean change 0.130, 95% CI −0.066 to 0.325, p = 0.19). The variation (random intercept) between participants was significant, with standard deviation 0.51, 95% CI 0.35 to 0.73. Figure 1 shows the model’s predicted values for ME scores over time.
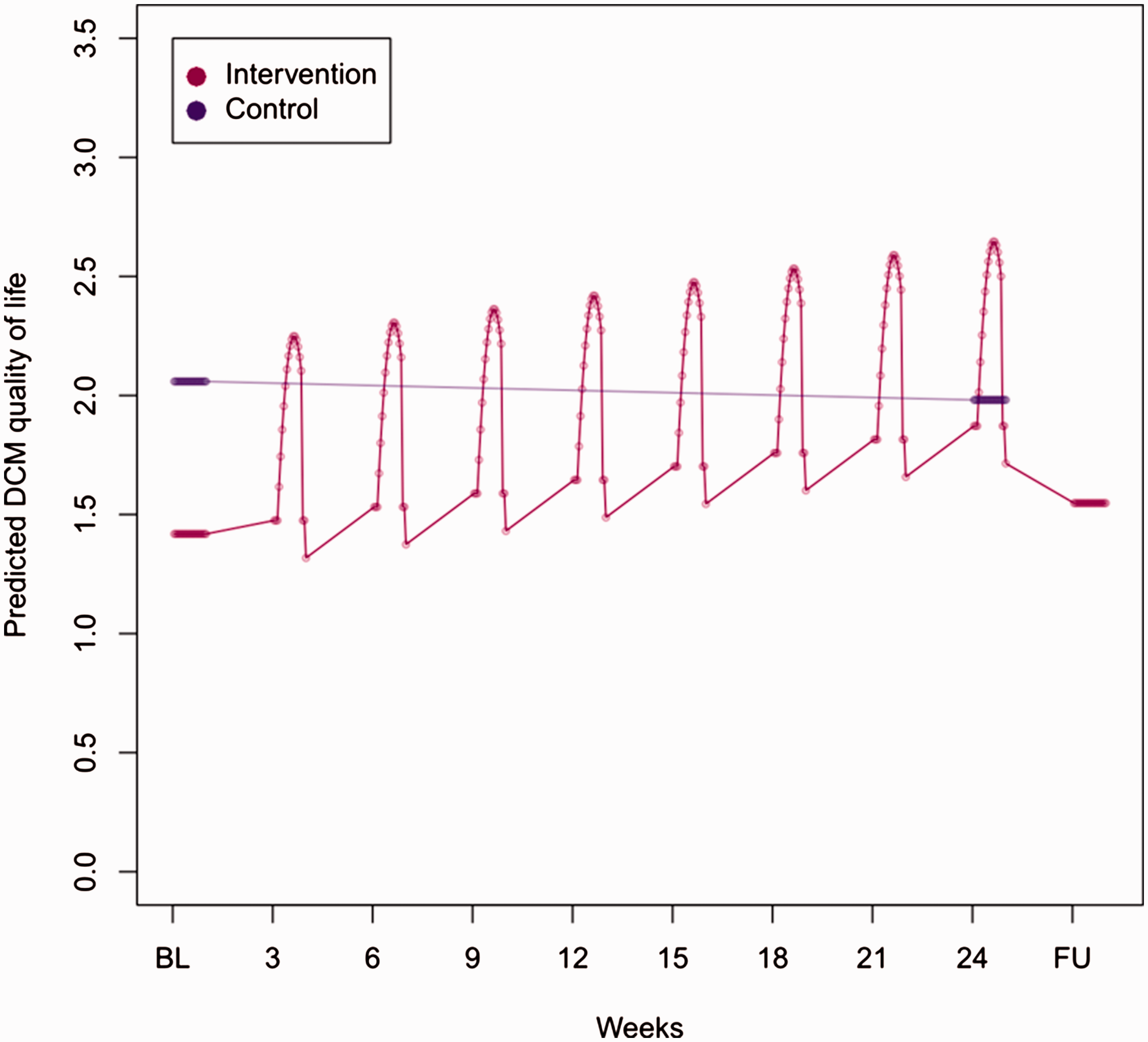
Predicted values of QoL over time.
Positive behaviour category codes
The multilevel logistic regression for positive behaviour category codes showed the same pattern of change over time as that for ME values, with one exception: the positive behaviour category codes after the group RA session had ended in the intervention care homes were significantly higher than prior to the session (OR 1.84, 95% CI 1.47 to 2.30, p < 0.001). The control care homes had significantly more positive behaviours at baseline (OR 2.32, 95% CI 1.27 to 4.25, p < 0.001). Behaviour increased and plateaued within each intervention period with odds ratio relative to the start given by
Both linear and quadratic coefficients are significant with p < 0.001. The increase over weeks was significant (OR 1.02, 95% CI 1.01 to 1.03, p = 0.001), but the difference between baseline and 24 weeks in the control group, and between baseline and follow-up in the intervention groups, was not (respectively, OR 0.88, 95% CI 0.52 to 1.49, p = 0.63 and OR 1.20, 95% CI 0.85 to 1.69, p = 0.29). The random intercept for inter-participant variability had standard deviation of 1.07 on the log-odds scale (95% CI 0.85 to 1.34). Figure 2 shows the model’s predicted values for positive behaviour over time.
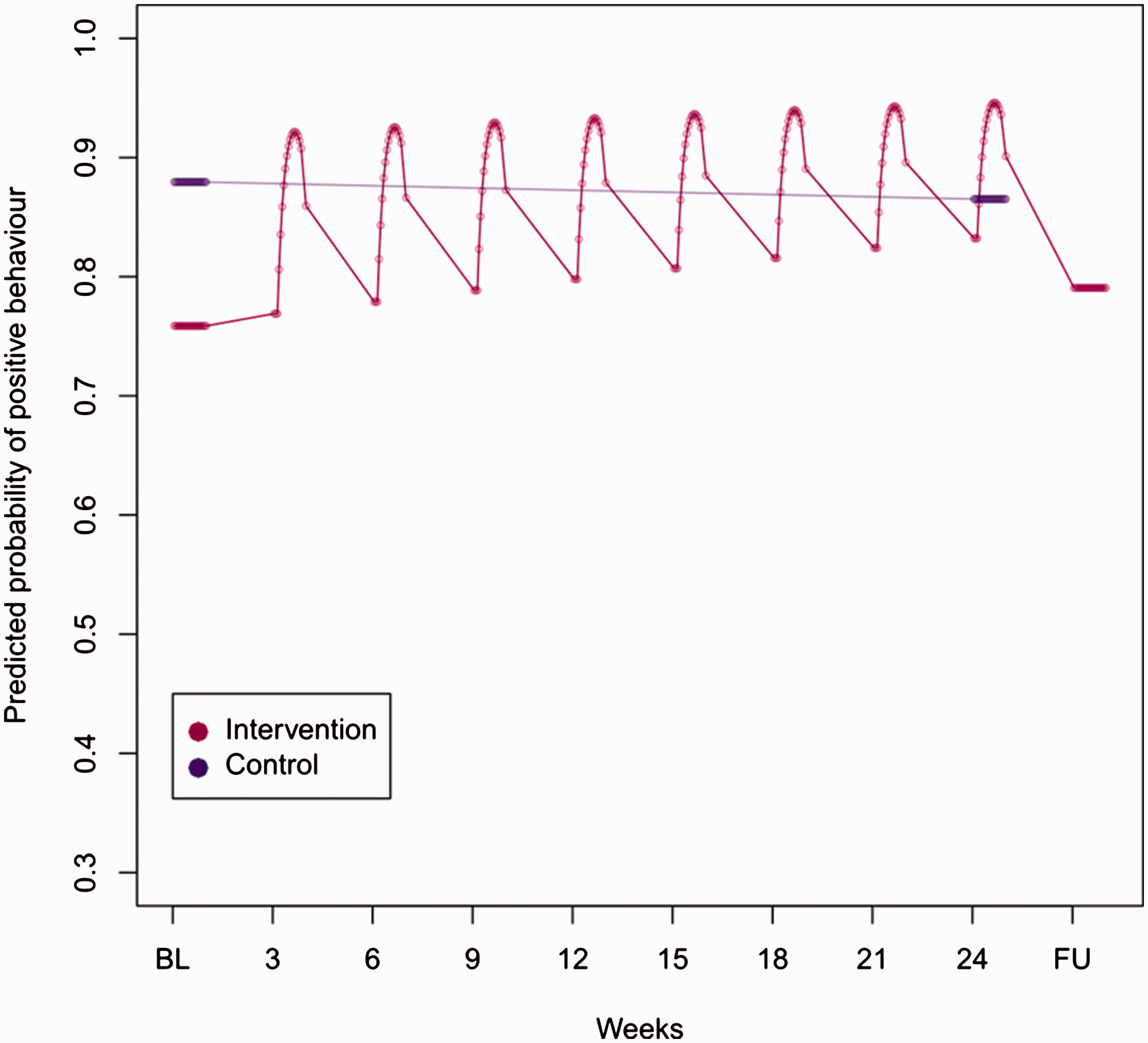
Predicted values for positive behaviour over time.
In summary, the analyses presented above show the following: Firstly, during the group RA sessions, positive behaviours and QoL of participants increased. Immediately after each evaluated session there was an observed sustained positive effect. This pattern was sustained over the whole study period and was found to be statistically significant. In addition, each group RA session, positive behaviours and QoL peaked at 50 minutes. This could be explained by the way sessions were planned. Most of the sessions were very energetic but wounded down towards the end with slower less demanding activities. Most sessions did not end abruptly but transitioned back into the daily life of the care home, for example, tea was served at the end of many sessions whilst some residents and the RAPs began to leave. However, this is only an explanation for those groups that were held for an hour (three of the six intervention groups). For the remaining three groups, the length of the groups was not previously determined, and could continue for two hours. Consequently, the results of the study suggest that the maximum benefit for participants may be at 50 minutes and therefore longer sessions would provide no further gains. However, this cannot be concluded from this study and further larger studies would be required to ascertain this. Secondly, positive behaviours and QoL of care home residents participating in group RA sessions increased as the 24 week projects progressed. It was observed at three weekly intervals that the participants’ QoL and behaviour was more positive than the previous session. This pattern was sustained over the period of the study and was statistically significant. However, it has to be noted that at three month follow-up after the 24-week intervention period, participants’ QoL and positive behaviours dropped, but not below the baseline.
Discussion
This study aimed to investigate whether group RA sessions were effective for people with dementia in care homes. Findings from this evaluation show that participants benefited from group RA sessions, as QoL and positive behaviours rose incrementally over the course of the intervention. This is aligned with earlier studies that showed that higher levels of well-being are obtained and maintained during reminiscence sessions (Azcurra, 2012; Brooker & Duce, 2000; Lai et al., 2004; O’Shea et al., 2014). The findings show that participants’ QoL improved from the start of the session and peaked at 50 minutes and that there was an upward trajectory over time. At follow up there was a drop in well-being to near the baseline, but not below it. Even though this was not statistically significant, it is an important finding given that the focus is on a degenerative condition, when deterioration in QoL may be likely. We were surprised to find that the scores for the control group remained relatively stable during the life of the study and attribute this to the fact that there were ongoing structured activities taking place in the control groups and could be an explanation for this. The fact that the benefits of group RA sessions were not sustained beyond the intervention supports findings from previous studies (Lai et al., 2004; O’Shea et al., 2014). One explanation could be that structured activities such as group RA sessions did not continue beyond the intervention and participants returned to previous patterns of ‘care home life’. Another explanation could be that DCM captures micro changes at the time of observation and therefore may not be suited to capture long-term benefits of group RA sessions (Lai et al., 2004). We also measured changes at group level and it may have been better to measure changes at individual level (Scott & Clare, 2003) using more global measures of change. However, as mentioned previously, perhaps evaluations should focus on the immediate benefits of group RA sessions given the degenerative nature of the condition. Particularly, since it has been reported previously that participation in reminiscence activities was enjoyable and beneficial to participants (O’Shea et al., 2014). Overall, this evaluation supports, builds and strengthens the evidence base for reminiscence arts practice for people with dementia in care homes.
This study supports findings of previous research that demonstrated that regular engagement with reminiscence and arts activities is positively associated with higher levels of well-being and QoL for people with dementia (O’Shea et al., 2014). There is however, still a need to develop ways of capturing and exploring the views of people with dementia in care homes on the value of arts and reminiscence (Roe et al., 2016). We also need to find ways to overcome the methodological challenges to evaluate the effectiveness for reminiscence and arts for people with dementia as identified by Zeilig et al. (2014).
Limitations of the study
This was a small scale pilot study and the results, although significant should be viewed in light of this fact. There were no other non-reminiscence or arts structured activities in the intervention care homes, which meant that observations were limited to participants engaging in everyday activities such as watching television, chatting to a friend, etc. This means that conclusive statements about the impact of group RA sessions on QoL cannot be made. However, it can be confidently reported that engagement in reminiscence and arts activities impacted positively on the QoL of participants in the intervention groups.
Another limitation is the fact that we were not able to match the intervention groups with the control group and could only ensure that all participants had a diagnosis of dementia, so the groups were theoretically the same. We are therefore unable to say with confidence whether it is the RA groups that produced the positive effect or the fact that participants engaged in structured activities given that there were such activities in the control groups as well. We could also not control for other variables such as type of home that may have influence the outcome.
The way in which participants were identified for inclusion in the study may have introduced a level of bias in that staff may have been preferential in their selections. However, this was compensated for this during the consent seeking process and prospective participants who did not meet the inclusion criteria were excluded from the study. Another limitation of the study is that QoL was examined by using just one measure such as DCM, so the results should be treated with caution. Work of this nature could benefit by self reports, particularly from people with mild to moderate dementia. This also meant that it was not possible to evaluate to what extent the intervention enhanced the overall quality of care.
In addition, we were not able to assess whether the severity of dementia was a predictor for improved well-being given that over half of the intervention groups had a diagnosis of unspecified dementia. Given that the age range is small, we were unable to reach conclusions about the possible effect of age on QoL. Furthermore, given the small size of the groups, we were not able to assess for differences between the types of care homes, such as residential versus nursing, or faith-based versus non faith-based facilities.
Due to the flexible nature of the activities during the intervention, the differences in length of the sessions and the small number of participants in each group, we were not able to identify which elements of group RA sessions were beneficial to the QoL of people with dementia living in care homes. However, the irregularities in length of the sessions may not be a serious limitation given that our findings showed that benefits peaked at 50 minutes. There is also no clear evidence on the optimum time for mapping an intervention and further research is need to determine the length of time that accurately reflects an improvement in QoL (Cooke & Chaudhury, 2012).
Conclusion
This study found that RA group sessions had a beneficial effect on the QoL of people with dementia who live in care homes. It showed that positive mood and engagement with reminiscence art activities increased during the group sessions and that this increase was incremental over time. At three-month follow-up we found that the positive effects were not sustained, but we can conclude that RA group sessions had a positive effect on QoL for people with dementia in care homes during the life of the study. We recommend that service providers and policy makers promote and develop creative ways to increase engagement and social participation of people with dementia in care homes, given that this study supports other findings that suggest that engagement with structured activities is likely to improve QoL. Staff should be trained and supported to promote engagement and active participation during routine activities as well as during structured activities.
There is a need to assess in much greater depth the association between QoL and group RA sessions. This will provide a stronger evidence base on the effectiveness of group RA sessions. Moreover, to arrive at firmer conclusions from a quantitative study, there is a need to compare non-standard activities with iterative standardised activities; this is a challenge for work in this field of study. There is also a need to further explore to what extent group RA sessions can contribute to improvements in the overall quality of care for people with dementia. Further work is needed to explore other ways of measuring long-term effects of reminiscence and arts on QoL for people with dementia. DCM captures effects in the short-term, but if we are to improve the overall QoL for people with dementia, we need to find ways to sustain effects over time.
Footnotes
Acknowledgements
The authors thank Age Exchange Theatre Trust (in particular David Savill and belinda Sosinowicz) for facilitating the study and Professor Helen Nicholson and Dr Jayne Lloyd for support during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Guys and St Thomas Charity.