
Abstract
Arts programming for people living with dementia and their caregivers has gained popularity as a way to provide opportunities for social interaction, expression, and continual learning. The goal of the present study, referred to as Retaining Identity: Creativity & Caregiving is to: (1) describe the process of designing and implementing a structured art experience for people living with memory loss and their co-residing caregiver; and (2) to summarize feedback provided by caregivers at the conclusion of the program. Retaining Identity is an eight-week program offered by professional artists who instructed dementia caregivers in four visual art activities, which they then taught to their care recipient. The program was designed for individuals with no art experience and the art projects were carefully developed to be engaging for both people living with dementia and their caregivers. The evaluation process included a qualitative survey completed by the caregivers to measure the impact of the program on the caregiver/care recipient relationship. The main themes that emerged from the survey were: caregiver growth, caregiver awareness, and creative discovery. The participants’ artwork supports that art making has the potential to encourage an equitable exchange and outcome for people with memory loss and their caregivers. Although the survey is limited in scope, the results support the use of the arts to positively impact caregivers and their relationship with their care recipient.
Keywords
Introduction
As the prevalence of dementia continues to rise, there is an increased need to develop programs to support people living with memory loss and their families. The 2017 Alzheimer’s Disease Facts and Figures Report estimated that 5.4 million Americans age 65 and older have Alzheimer’s disease; and the number was projected to reach 7.1 million by 2025 (Alzheimer’s Association, 2017). Furthermore, caregivers provide over 18 billion hours of care to family members with Alzheimer’s (Alzheimer’s Association, 2017). With the increasing prevalence and numbers affected, innovative programs to increase quality of life of people living with dementia and their caregivers are greatly needed.
Art has the unique potential to increase awareness of the self and of the outside world. As such, it provides rich terrain as a therapeutic context for people living with dementia. In his research on creativity and aging, Cohen (2006) describes how imagination and engagement trigger positive feelings for people living with dementia. Music, theater, dance, writing, and visual art are becoming widely accepted components of dementia care that rely on creativity to initiate discoveries, invite dialogue, engage in meaningful activities, and “bring something beautiful into existence” (Killick & Craig, 2012, p. 20; Rosenberg, 2009). Art programming often brings out an emotional side to building connections between persons living with dementia and their care partners (Bastings, 2006; Zeilig, Killick, & Fox, 2014).
Anne Basting’s TimeSlips™, The Metropolitan Museum of Art’s Meet Me at MoMA, and the Frye Art Museum’s here:now are examples of creative programs for people living with memory loss that use visual imagery to prompt imaginative responses (Burnside, Knecht, Hopley, & Logsdon, 2017; Fritsch et al., 2009; Rosenberg, 2009). TimeSlips™ is a group storytelling program focused on creative expression for residents in long-term care facilities. Fritsch et al. (2009) report that program participants were more engaged in interactions than residents in the control facilities. The Metropolitan Museum of Modern Art’s Meet Me at MoMA program provides a guided discussion of the museum’s art collection for people with early to moderate dementia and their care partners (Rosenberg, 2009). For people living with dementia, the program increased engagement and alertness; caregivers reported a sense of joy in being able to participate in a shared experience with their family member (Rosenberg, Parsa, Humble, & McGee, 2009). Another program that integrates a museum discussion and art-making experience is the Frye Art Museum’s here:now (Burnside et al., 2017). Designed for people living with dementia and their care partners, participants engage in an art activity related to a theme discussed earlier in the museum (Burnside et al., 2017). Through participant interviews, the researchers found that the here:now program contributed to increased socialization and provided opportunities for personal expression and creative exploration (Burnside et al., 2017).
Despite the potential and recent popularity of these programs, research in the field of art and dementia is limited. Many challenges arise in establishing interdisciplinary collaborations that pair artists and researchers to design and test interventions (Loken, Sauer, & Li, 2016). For example, Goulding (2013) notes that art programs are typically short term, small scale, and involve small numbers of participants with a high turnover (p. 134). And, according to the National Endowment of the Arts, a common deficiency in arts and health research is that programs are not well defined or documented and therefore cannot be easily replicated (Kent & Li, 2013, p. 2). Beard (2011) also noted the lack of detailed descriptions of art activities as one of the gaps in the research and the need for programming for people with dementia that live at home.
Following successful program models such as Meet me at MoMA and here:now, our program, named Retaining Identity, is a hands-on art-making program for people living with dementia and their care partners. It is unique in that it was designed to offer training to dementia caregivers to engage in art activities at home with their care recipient. In this way, we expect that the art activities would be incorporated into the daily experience of families living with dementia, hence the benefits of the program can be sustained.
Drawing from the theoretical framework referred to as the University of Minnesota Center for Spirituality and Healing Wellbeing Model, Retaining Identity is designed to encompass positive practices in three areas: purpose, relationships, and environment (Kreitzer, 2012). The Wellbeing Model emphasizes the value of finding purpose in life and daily activities (2012). Retaining Identity is based on integrating art activities into the lives of caregivers to provide opportunities for enjoyment, relaxation, and personal expression. Aiming to improve quality of the relationship between the caregiver and care recipient, Retaining Identity uses art as an opportunity for dyads to learn together in order to strengthen their relationship. Furthermore, the Wellbeing Model emphasizes the importance of a person’s environment in reducing stress (2012). The Retaining Identity team created a welcoming and inviting space for participants to explore their creativity and offered genuine praise during the art making and guided discussion.
The purpose of the present pilot study, referred to as Retaining Identity is to: (1) describe the process of designing and implementing a structured art experience for people living with memory loss and their co-residing caregivers; and (2) to summarize feedback provided by caregivers at the conclusion of the program.
Program description
Program overview
Retaining Identity is a 90-minute art-making session and art-related discussion that meets once a week for eight weeks for individuals with memory loss and their co-residing caregiver. The first four sessions were dedicated to caregivers learning a new art activity each week. In the second four sessions, caregivers guided their care recipient through the same four art activities. The art-making sessions were designed for small groups (6–12 people) and required three project staff members to run smoothly. All art materials and supplies were included as part of the program (e.g., paint, paper, ink, and brushes) and participants were able to keep all their artwork. Program completers, participants who completed more than half of the program, received an instruction booklet of the art activities to replicate the projects at home and a $35 gift card ($70 per dyad).
The 90-minute sessions were divided into: a project overview (10–15 minutes), art-making (60–75 minutes), and a guided discussion (10–15 minutes). The project overview involved introducing the art project, discussing materials and techniques that the project explores, and demonstrating the steps. The implementation team (a subgroup of the research team) led the project overview for the caregivers during the first half of the program. The caregivers then introduced the project to their care recipient during the second half of the program. During the art-making period, the implementation team provided the participants with materials, supplies, aprons, and gloves. Throughout the art-making, the implementation team made sure everyone had what they needed, pinned up all the artwork for display, and cleaned up. The sessions ended with a guided discussion about the completed art using a set of open-ended questions. Standing next to the completed artwork, the implementation team would lead the participants in the discussion by reading the question out loud (See online Appendix A for the list of discussion questions).
Weeks 1–4
The implementation team introduced four art activities to the caregivers: (1) monoprint, (2) shibori, (3) additive/subtractive acrylic painting with found objects, and (4) contour drawing with ink and watercolor (See online Appendix B for descriptions of each activity). During these sessions, the caregivers learned how to use a variety of art materials, explored their creativity, developed a basic understanding of art and design principles, and learned to use verbal and gestural cues to facilitate an art activity for persons with memory loss. The implementation team facilitated the art activities in the same manner as they would for people with memory loss to encourage the caregivers to integrate the same approaches when working with their care recipient. The implementation team also asked the caregivers to refrain from moving around the space too much to avoid unnecessary distractions when engaging with their care recipient. The implementation team was responsible for all clean up throughout the sessions to enable the caregivers to focus on the art experience. On-site respite care was available for care recipients. Provided by the research team, respite care consisted of games, puzzles, conversations, and gentle stretching.
Weeks 5–8
In the next four weeks, caregivers taught the same projects to their care recipient. During these sessions, the implementation team would introduce the project and remind the caregivers of the process. The caregivers then introduced the project steps to their care recipient using an instruction sheet for guidance. The implementation team observed the art-making and kept the participants’ workspace as clutter free as possible to avoid confusion or loss of focus. The implementation team also assisted the caregivers whenever they needed help in verbally delivering an instruction or to assist in making a quick adaptation to a project. The implementation team encouraged the caregivers to find what worked best for them and their partner. This flexibility resulted in some dyads working directly together on a project while others worked side-by-side. Similar to the first four weeks, the implementation team pinned all the completed artwork up for a guided discussion.
Program considerations
Several considerations informed the design of the program including the composition of the program staff, participant eligibility, the art projects, and logistics.
The implementation team was comprised of art instructors with expertise in both visual art and dementia care to design projects that took into consideration artistic merit as well as accessibility for people living with memory loss. Working within budget constraints, team members included: two professional artists with training in dementia care and two graduate students, one in social work and one in art. The team designed the projects, provided information and helpful tips for engaging people living with dementia in creative expression, and facilitated all the sessions to ensure the consistent delivery of the program. In addition to the implementation team, researchers and graduate students with expertise in dementia from public health and social work contributed to the pilot study.
The primary factor in the design was the selection of the four art activities. The research team discussed project ideas in terms of artistic merit, accessibility, enjoyment, and potential for discovery and experimentation. The four activities—monoprint (a printmaking project), shibori (a textile project), additive/subtractive acrylic painting with found objects, and contour drawing with ink and watercolor (a drawing technique used to capture the outline of objects)—were developed for the program based on the above criteria. The art activities were also selected for their ability to be completed by the participants within the 90-minute session. The 90-minute sessions enabled participants to have sufficient time to create while maintaining focus and interest.
Designed for co-residing caregivers and care recipients, eligibility criteria were established to ensure the participants could fully participate in the art program and potentially replicate the projects at home. Caregiver eligibility criteria included: living with and caring for a person with memory loss who is interested in the study, between the ages of 21 and 95, ability to hear and see sufficiently for group participation, ability to use upper body and arms, English speaking, does not have a memory diagnosis, and has own transportation. Eligibility criteria for the person with memory loss included: has a diagnosis of Mild Cognitive Impairment (MCI) or mild-moderate probable Alzheimer’s Disease, between the ages of 45 and 95, English speaking, ability to hear and see sufficiently for group participation, has use of hands and upper body, bathroom independent, and does not have psychiatric symptoms that may interfere with group participation.
The program was offered at a senior resource center on early weekday evenings and Saturdays. The research team selected this site based on its availability, floor plan, handicap accessibility, and free parking close to the building. The site is composed of one large room with a counter/sink area and several smaller rooms making the space ideal for the art sessions and on-site respite care. The eight-week sessions ran one at a time except for the last two sessions, which overlapped. Sessions were not offered during the winter months to avoid the cold weather and potential for unsafe driving conditions.
Recruitment
Because the art intervention needed to appeal to both the caregiver and care recipient, recruiting for the art program included multiple strategies. After obtaining institutional review board (IRB) approval, the research team recruited participants by contacting referrals provided by the Michigan Alzheimer’s Disease Center (MADC) and the University of Michigan website for recruiting participants for approved clinical trials. Flyers were posted at various sites, including outpatient hospitals, adult day care centers and senior centers, and online announcements were distributed through the Alzheimer’s Association. However, recruitment for 30 co-residing dyads was challenging. Even with offering sessions on various times/days and providing respite care, it took us three years to recruit 30 dyads. Recruitment challenges are addressed in the discussion section.
Phone screening
A phone screening by a trained research assistant was used to determine participant eligibility. A research team member reviewed the study requirements and then confirmed that the dyads met the study criteria. Consent forms were then mailed to eligible dyads prior to the first session and completed before they began the first session. Participants consented to having their artwork photographed, minus any identifiable information.
Study participants
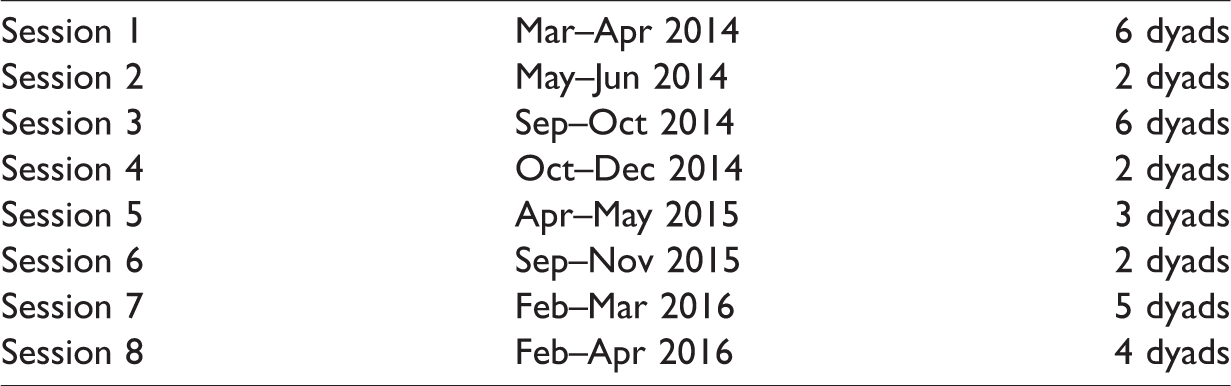
In total, 36 co-residing caregiver–care recipient dyads were recruited; 30 dyads completed the study. Completing the study involved the caregiver attending most if not all of the first four sessions, the caregiver/care recipient attending most if not all of the following four sessions, and the caregiver completing the survey. Most dyads missed 1–2 sessions during the eight-week program. Of the 30 caregivers, 66.7% were female, 26.7% were male, and 6.6% did not respond. Eighty-three percent of the caregivers were married and 17% were single. The caregivers’ age range was 6.7% between 31 and 40, 10% between 41 and 50, 20% between 51 and 60, 30% between 61 and 70, 20% between 71 and 80, 6.7% between 81 and 90, and 6.7% did not respond to this question. Of the 30 caregivers, 46.7% were serving as a caregiver for two years or less, 30% for three to five years, and 23.3% for 6 to 10 years. Eighty percent of the caregivers who participated were White, followed by 6.7% Black, 3.3% Multi-racial, 3.3% Asian, and 6.7% did not respond to this question. Due to recruitment challenges and participant drop out (6 dyads over the course of the intervention), the size of the groups for each session varied (See Table 1). The smallest group consisted of two dyads and the largest group consisted of six dyads.
Program timeline and group size.
Facilitation of the art making
For each project, the implementation team showed a sample of the project and then demonstrated the technique to illustrate a range of possibilities. The implementation team further encouraged experimentation by not restricting or correcting the art making. If a participant showed hesitation, the implementation team would gently encourage the participant by emphasizing that the project was an opportunity to have fun and try something new. The implementation team also allowed the participants to make as many or as few pieces as they wanted, which ranged from 3 to 5 pieces for the monoprint, shibori, and additive/subtractive projects.
Throughout the art making, the implementation team observed the care recipients’ interactions and level of memory impairment to offer guidance to caregivers. For instance, the additive/subtractive project introduced a variety of tools to add and remove paint from the paper. Caregivers of partners with more advanced dementia were taught to modify the activity by paring down the tool options and using hand gestures to demonstrate how a tool worked while still offering opportunities for choice and expression. Caregivers learning to modify activities and develop communication techniques through art making became an essential part of the program.
Using the same set of materials and techniques, the participants’ artwork resulted in a range of exploration. For the monoprint project, participants experimented with the consistency of the ink and layering to create multi-colored prints and various textures. For the shibori project, participants explored creating more complex patterns by combining folding, wrapping, and tying techniques prior to dyeing the fabric. For the acrylic painting project called additive/subtractive, participants invented ways to use combs, sticks, and other objects to add and subtract layers of paint and explored mixing colors. The contour drawing with ink and watercolor project was the last activity and most participants only completed one as it involved more steps. After being introduced to this life drawing technique, which focuses on slowly drawing the outline of the subject, the participants then explored creating variations in line and color with ink and watercolor paints. The implementation team observed that this project involved a more quiet focus than the other projects and that plants worked well as the subject for they allow a certain level of forgiveness when it comes to accuracy due to their organic nature (Figures 1–4).

Monoprint completed by Retaining Identity participant, 9” × 12”, print ink on paper, 2015.

Shibori textile completed by Retaining Identity participant, 14” × 16”, fabric, 2015.
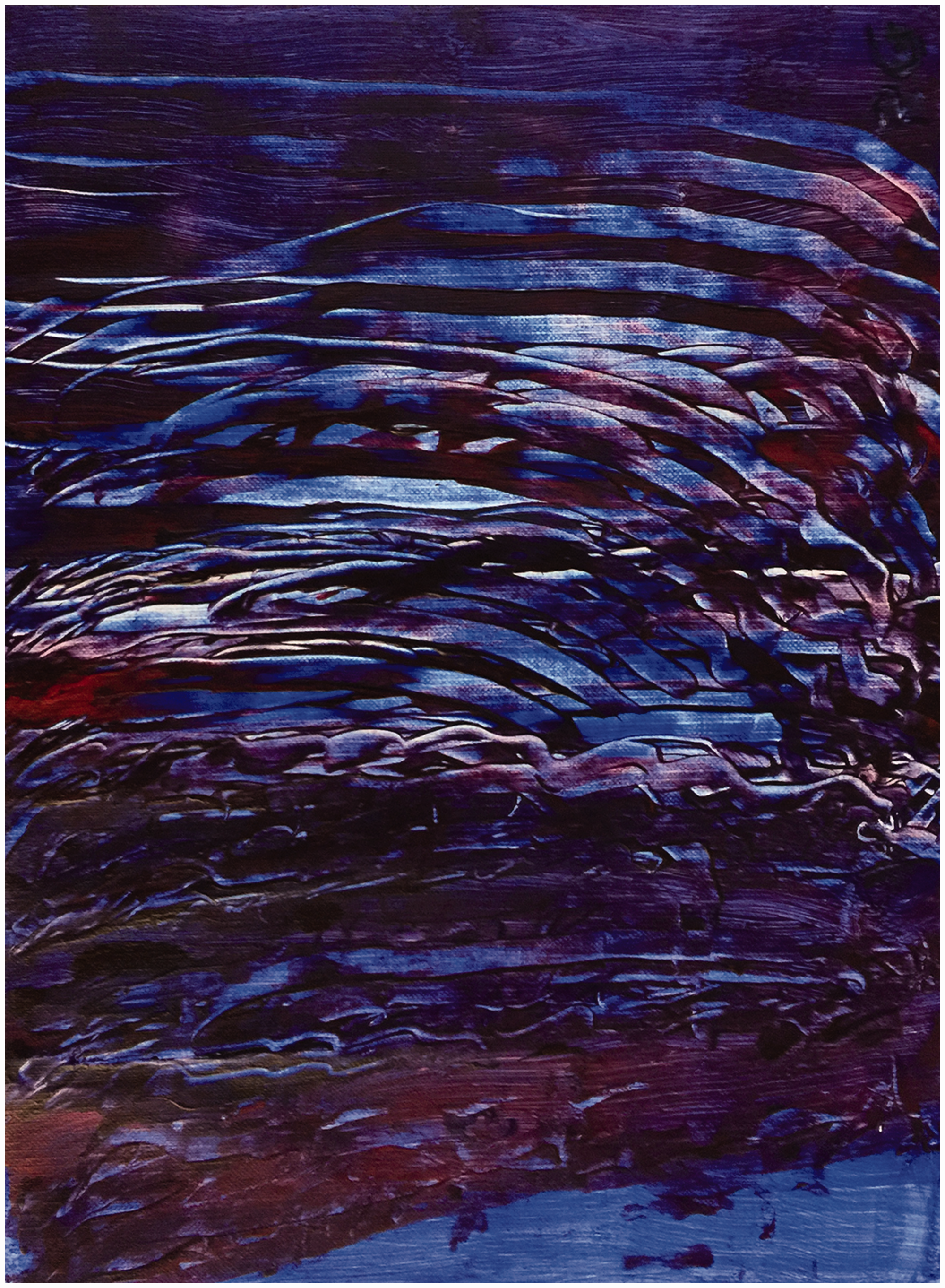
Additive/Subtractive painting completed by Retaining Identity participant, 9″ × 12″, acrylic paint on canvas paper, 2015.

Contour painting completed by Retaining Identity participant, 9″ × 12″, watercolor paint and ink on paper, 2015.
Available during the first four weeks of the program, optional respite care proved to be an important factor in the program implementation. Respite care was well attended by the care recipients, which enabled caregivers to participate without needing to arrange for home care. Although not evaluated, several participants remarked that the quality of respite care contributed positively to the overall experience.
Program evaluation
Caregiver survey
Qualitative data were collected from the participating caregivers. After the last art session, caregivers were given a questionnaire with the request that it be mailed back to the research team within a two-week time frame. All 30 caregivers completed this process. The questionnaire included four open-ended questions: (1) Was there anything you learned as part of the program that can help you in the future as you face dementia?; (2) Over the course of the workshops, was there anything you learned about yourself?; (3) Over the course of the workshops, was there anything you learned about your partner?; and (4) Has this experience changed the way you interact with your partner? If so, how?
Data analysis
The two primary researchers and a research assistant conducted a thematic analysis of open-ended questions. The thematic analysis was conducted for each question using the Affinity Diagram or “K-J” method where individual comments were grouped according to similar themes and consensus was reached by the research team (Braun & Clarke, 2006; Scupin, 1997). For this process, the research team printed the comments on individual sheets of paper that were then grouped together. Once the comment cards were grouped, category names were added to identify the themes and a report was created to categorize each theme and the corresponding comments.
Research findings
Three main themes emerged from the qualitative data: caregiver growth, caregiver awareness, and creative discovery. Caregiver Growth refers to specific ways that caregivers can improve their communication. For example, one caregiver reported, “… I learn more when I listen than speak.” Other Comments such as “my patience has improved so we can interact more effectively” and “… I try to slow down the pace” also fall within this theme as caregivers realized the need to adjust their communication skills and behavior to better interact with their care recipient. Caregiver Awareness refers to comments in which the caregivers developed a deeper understanding and perspective of their partner’s cognitive ability which helped to improve their communication skills such as “That my loved one can do more than what I think he can” and “That she is very hesitant to beginning a project unless she can do things her way at her own pace.” Another caregiver remarked, “Spouse was able to come up with own creative ideas. Good to step back and let him continue on his idea.” Creative Discovery refers to comments in which caregivers discovered the benefits of creative endeavors for them and their care recipient. Comments within this theme include “Art is still fun”, “Art has no boundaries, no right or wrong way”, and “I learned that even though I do not have much artistic ability I had fun learning new techniques and look forward to doing these again with my husband.”
Responses referring to Caregiver Growth occurred across all four questions and made up 34% of the total comments. Caregiver Awareness and Creative Discovery both occurred in two questions and each made up 14% of the total comments. In all, these three themes account for 62% of the caregivers’ responses (See online Appendix C for individual question results). Caregiver Growth and Caregiver Awareness both refer to the development of caregiving skills and methods. In addition to creative discovery, participants identified the development of caregiving skills as a major impact of the experience. This suggests that the Retaining Identity program may assist caregivers in learning new skills and techniques that extend beyond the program into daily interactions with their care recipient.
One additional theme that emerged as a subcategory of Caregiver Growth that is worth noting is Patience. Patience is a recurring theme in Caregiver Growth throughout all four questions and made up 45% of the comments in Caregiver Growth to question 4: how the art intervention changed the way caregivers interacted with their family members? This finding supports explorations in art as a tool to increase caregiver patience further emphasizing the potential of the program to serve as a tool for caregivers in developing skills that may positively impact their relationship with their care recipient.
Other themes that emerged included: enjoyment, recognizing identity, and relationship building. Enjoyment refers to comments in which caregivers observed their care recipient’s enjoyment in the art projects such as “He really appreciated my going with him and was pleased to see me enjoying the artwork”. Recognizing Identity refers to comments in which caregivers recognized what makes their care recipient unique. One caregiver comment within this theme includes: “Renewed appreciation of his innate creative view and experience. Awareness of his inner confidence challenge peeking out at the world occasionally.” Relationship Building refers to comments in which caregivers indicated new ways to engage with their care recipient such as “Yes, art is needed as an activity that we could do to stay connected.”
Results of the caregiver survey suggest that the social context provided by Retaining Identity was critical to its success. Caregivers in Retaining Identity commented that the other participants and the research team were a positive part of the experience. One participant commented: “All the instructors and helpers were very pleasant and upbeat that is very much needed, for both caregivers and family members.” The opportunity for social interaction and the importance of having friendly staff was also cited as key attributes to the impact of the Meet Me at MoMA program (Rosenberg et al, 2009).
Discussion and implications
Below the researchers share the lessons learned from implementing a structured art program for people living with memory loss and their co-residing caregivers, and offer suggestions to those who are considering developing similar programs. The main challenge in the implementation process was recruiting participants. It may be related to caregivers’ stressful lives and reluctance to make other commitments; people’s view of themselves as not being artistic; the study’s sample eligibility criteria; and a limited budget to advertise the study. The research team has identified possible ways to encourage greater participation. These include:
Expand the program to include caregivers and care recipients that do not co-reside: Even though the aim of the program is to focus on training the caregiver in order to replicate the activities at home, there is the potential for the activities to be integrated during time spent together. Build partnerships with local organizations and assisted living facilities: The site was a good fit for the program, but may have limited participation of people from surrounding areas due to transportation concerns. Partnering with other sites will potentially reach a wider, more diverse audience. One consideration is to partner with an assisted living facility and invite family caregivers to the site to work with their family member. Other possible partners to help identify and refer participants include local libraries, the YMCA, senior centers, and Area Agencies on Aging. Train artists to serve as program facilitators: Having an implementation team with expertise in art and dementia proved valuable in facilitating the program and designing projects that encouraged exploration. The shortcoming to this strategy—a team specialized in both art and dementia care—is the amount of time and energy it required from a small team to deliver the program; a larger team would have been able to offer more frequent programming. Moving forward, training artists to facilitate the program at various sites and developing a standard art kit for each project to implement at the sites will be considered. This direction will eventually extend the program beyond the research arm to embed the program into the community. Revise the program structure: Committing to an eight-week program was problematic for some participants and potential participants. From observing the sessions, a shorter program will suffice to provide caregivers with enough time to gain the experience and guidance they need to facilitate the art activities. Another option to consider is to allow participants to select two or three activities they would like to participate in. This would take some oversight to ensure the caregivers are attending enough sessions to facilitate the art projects. Noting the additional guidance caregivers needed if they were absent when the project was introduced in the first session, they might need to be excluded from that activity. Stress the opportunity to engage together: One possible recruitment factor may have been people’s reluctance to engage in art-making and potentially overlooking the fact that this is an opportunity to participate in an activity together. Several caregivers commented that they weren’t artists or that their partner does not enjoy art. Some potential participants may have also been reluctant to participate in arts programming due to assumptions around creativity and that only certain people are artistic (Killick & Craig, 2012). Integrating art activities for families early on as part of their care plan established by physicians or social workers could potentially assist in overcoming some of the hesitation to participate. Moving forward the researchers will better explain the intent of the program to focus on the process of engaging and providing dementia caregivers with guidance to facilitate activities that focus on their partner’s strengths (Bowlby Sifton, 2000).
Other program considerations that surfaced from the implementation include:
Balance the process and product: The artistic merit of the finished artwork was important to the overall participant experience. Many participants in the Retaining Identity program commented on the uniqueness and sophistication of the artwork, which enhanced the guided discussion by inspiring a range of positive comments and insights. Most importantly, the completed artwork was not identifiable as to whether it was created by the caregiver or care recipient. This makes a strong case for visual arts to be used as a dementia care activity that creates an equitable exchange and outcome for people with memory loss and their caregiver. The researchers also found that during the guided discussion participants were not concerned as to whether a caregiver or care recipient created the artwork. The art-making process was essential to the program and the positive response to the completed artwork may encourage participants to engage in the activities at home. Guide the caregivers: As noted earlier, the research team worked with caregivers to modify projects for their care recipient. Suggesting ways to tailor the projects were welcomed and encouraged by the caregivers. Continuing to implement this into future programs will be important to reduce the ‘disability gap’ that occurs when activities are not carefully adjusted to meet the needs of the care recipient (Bowlby Sifton, 2000). Guiding the caregivers in delivery of the projects is important to contribute to a positive interaction that may increase communication. For couples, Retaining Identity may create new opportunities for them to maintain their interactions and engage in reciprocal exchanges (Hellström, Nolan, & Lundh, 2007; Kaplan, Ade-Ridder, Hennon, Brubaker, & Brubaker, 1995). here:now researchers identified that hands-on art-making contributed to increased interactions by encouraging further discussion over participants’ completed artwork (Burnside et al., 2017). Expand the “retaining identity” theme: The program activities could further explore the theme to strengthen both the individual’s sense of identity and the couple’s sense of identity. For the caregiver, this could include integrating additional reflective opportunities, such as journaling. For the couple, additional opportunities, as one participant suggested, could be to provide a brief time for the caregiver and care recipient to respond to the questions as a couple prior to the group discussion. Meet Me at MoMA’s program evaluation found that the opportunity to participate in a program that both individuals in a married couple enjoyed strengthened their identity as a couple (Rosenberg et al., 2009). Integrating more opportunities for factors recognized as important to marriage, such as communication and sharing, into the program is worth considering (Kaplan et al., 1995). Integrate a comprehensive program assessment: The three main themes derived from the caregiver survey results– caregiver growth, caregiver awareness and creative discovery—align with previous findings that art activities are effective in providing dementia caregivers with new insights to better engage with their care recipient (Zeilig et al., 2014). Retaining Identity’s caregiver comments also supports the use of the arts to provide enriching and pleasurable activities for caregivers and their care recipient. The program provided caregivers with the chance to temporarily disconnect from the demands of daily life and focus on engaging in a fun activity with their care recipient (Zeilig et al., 2014). After the implementation challenges have been resolved, these initial findings support developing a more comprehensive evaluation to further assess the impact of hands-on art programming for caregivers and persons living with memory loss to maintain and build their relationship.
Retaining Identity’s multidisciplinary research team of art and dementia care experts in art, social work, and public health were able to balance the needs of the participants with the creation of aesthetically pleasing artwork. This multidisciplinary approach is starting to gain traction as seen by Dementia and the Imagination, a project underway in the UK led by experts in the arts, humanities, and social sciences to explore the use of art to improve quality of life for people with dementia and to promote dementia awareness within the community (Newman et al., 2016). Encouraging researchers to connect with artists at the local, national, and international level has the potential to develop new innovative programs and research initiatives.
Retaining Identity also relies on an interdisciplinary approach by having artists educated in dementia care facilitate the program. The artist’s knowledge and experience in dementia care were essential in providing best care practices and helpful tips to caregivers throughout the art sessions. Educational opportunities for artists to build their dementia care knowledge are growing. These include the University of Michigan School of Social Work’s Web-Based Certificate in Advanced Clinical Dementia Practice; Miami University Scripps Gerontology Center Opening Minds through Art training program; and the National Center for Creative Aging (NCCA) Creative Caregiving Initiative, a series of online art and dementia care modules. More educational programming geared towards artists to learn to facilitate programming for people living with memory loss and their caregivers would be beneficial to move the field forward.
To conclude, Retaining Identity relies on art as a means to provide meaningful activities for people living with dementia and their caregiver while also training caregivers in facilitating these activities at home. Teaching caregivers new skills and techniques to engage with their care recipients at home has the potential to positively impact people living with dementia and their care partner’s quality of life. Recognizing this potential, the recruitment and implementation challenges shared here will assist in strengthening future programming efforts and helping to disseminate the program in the community.
Supplemental Material
Supplemental material for Retaining identity: Creativity and caregiving
Supplemental material for Retaining identity: Creativity and caregiving by Anne Mondro, Cathleen M Connell, Lydia Li and Elaine Reed in Dementia
Footnotes
Acknowledgements
We wish to acknowledge Parisa Gharderi, Annie Hyrila, Brianna Broderick, Andee Jansen, and Mariana Voica for assisting with the program design and implementation. We would also like to thank Alexandra Steele and Victoria Adkins for their key role in collating and coding the surveys and Ashley Miller for assisting with the paper. Most importantly, we thank the program participants for creating art and sharing their experience.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to their research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a University of Michigan MCubed research grant and partially supported by the National Institute of Health/National Institute of Aging funded Michigan Alzheimer’s Disease Center [P30AG053760].
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.