
Abstract
Background
Caring for a family member with dementia puts caregivers at risk for depressive symptoms. Yet, interventions with promising effects on caregiver depressive symptoms are not well documented.
Aims
This review aimed to examine the quality and effectiveness of interventions to reduce depressive symptoms reported by caregivers of people with dementia.
Design
A systematic review and meta-analysis of nonpharmacological intervention trials was conducted.
Methods
The electronic databases searched included MEDLINE, CINAHL, and PsycINFO to find randomized controlled trials published between 2007 and 2017. A total of 31 randomized controlled trials were included in the meta-analysis.
Results
Cognitive-behavioral therapy (838 participants) showed a large, significant effect (standardized mean difference = −0.905; 95% CI = (−1.622, −0.187); p = 0.013) and mindfulness interventions (186 participants) showed moderate, significant effects (standardized mean difference = −0.578; 95% CI = (−0.881, −0.275); p < 0.001) on decreasing caregiver depressive symptoms, while psychoeducational interventions demonstrated small but significant effects (standardized mean difference = −0.244; 95% CI = (−0.395, −0.092); p = 0.002). Emotional support, cognitive rehabilitation, and multicomponent interventions showed less than small or nonsignificant effects related to depressive symptoms among caregivers.
Conclusion
Cognitive-behavioral therapy interventions, which focus on diminishing negative thoughts and increasing positive activities, can effectively decrease depressive symptoms for caregivers of individuals with dementia. Future research is recommended to assess the long-term effectiveness of cognitive-behavioral therapy in this population.
Introduction
Dementia, including Alzheimer’s disease, is the sixth leading cause of the death in the U.S. and one of the top 10 causes of death worldwide regardless of race, sex, or age (Alzheimer’s Association, 2018). About 46.5 million people are living with dementia worldwide and the number is predicted to double approximately every 20 years, exceeding 74.7 million by 2030 and 131.5 million by 2050 (The Global Voice on Dementia, n.d.). Caregivers, usually family and friends, provide unpaid care to home-dwelling older adults with dementia. Caregivers meet essential and necessary needs of their care recipients, including helping with activities of daily living (e.g., bathing, eating, and moving), administering medications and treatments, and coordinating with physicians for the person’s care (Lwi, Ford, Casey, Miller, & Levenson, 2017). Family and friend caregivers will continue to become an even more critical resource given the rapidly increasing rate of dementia and the rising costs associated with dementia care (Vernooij‐Dassen, Draskovic, McCleery, & Downs, 2011).
Caregivers and depressive symptoms
Caregivers of people with dementia are particularly vulnerable to developing depressive symptoms. According to a recent systematic review that investigated the impact of caregiving, rates of depression are higher among those who provide care for people with dementia than among caregivers of people with other chronic illnesses (Schoenmakers, Buntinx, & Delepeleire, 2010). In addition, reported prevalence of depression among caregivers of people with dementia ranges from 30 to 80% (Schoenmakers et al., 2010). Furthermore, when caregiving became more demanding (increased weekly hours of caregiving), caregivers were six times more likely to experience depressive symptoms than noncaregivers (Cannuscio et al., 2002).
Interventions for caregivers of people with dementia have included cognitive-behavioral therapy (CBT), psychoeducational programs, emotional support, cognitive rehabilitation therapy, and multicomponent interventions (Waller, Dilworth, Mansfield, & Sanson-Fisher, 2017). However, it remains unclear which type or types of interventions are most effective in reducing caregivers’ depressive symptoms. Most published systematic reviews incorporating meta-analyses typically report the effectiveness of interventions based on mode of delivery, such as group-, individual-, or technology-based, rather than the content or approach of the intervention (Boots, Vugt, Knippenberg, Kempen, & Verhey, 2014; Olazarán et al., 2010; Thompson et al., 2007; Waller et al., 2017). Although two meta-analyses have reported effectiveness based on content (Pinquart & Sörensen, 2006; Sörensen, Pinquart, & Duberstein, 2002), those studies were conducted more than 10 years ago and, therefore, do not reflect the findings of more recent interventions. Also, these two reports included randomized as well as nonrandomized trials, affecting the generalizability of the findings (Pinquart & Sörensen, 2006; Sörensen et al., 2002).
Objectives
Over the past 10 years, a number of experimental studies for caregivers of people with dementia have been conducted worldwide, demonstrating some favorable outcomes for caregivers (Waller et al., 2017). Among experimental studies, randomized controlled trials (RCTs) are considered the “gold standard” for examining the effectiveness of interventions and provide a stronger basis for translating research results into clinical practice (Spieth et al., 2016). For that reason, to find high quality, evidence-based interventions for depressive symptoms experienced by caregivers of people with dementia, the current study synthesized the most recent 10 years of RCT data.
The aims of this systematic review incorporating meta-analyses are (1) to compare the effectiveness of different types of RCT interventions targeting depressive symptoms among caregivers of people with dementia and (2) to describe the nature and quality of current studies using methodological quality appraisal.
Methods
Search strategy and eligibility criteria
This systematic review incorporating meta-analysis is exempt from IRB approval as in this study investigators collected and synthesized data from former RCTs that the clinical trial researchers obtained the ethics approvals and participants already agreed on the informed consent. Trials were searched using major health care research databases including MEDLINE (Ovid), CINAHL, and PsycINFO. Four key terms “Dementia” or “Alzheimer’s disease” AND “Caregiver*” AND “depression” AND “intervention” were combined using a Boolean technique to intensify the search of the relevant literature. The search was limited to literature published from 2007 to 2017 and written in English. The initial search yielded 289 citations from MEDLINE, 373 from CINAHL, and 339 from PsycINFO. Using Refworks®, duplicate citations (n = 537) were removed, resulting in a total of 464 citations.
The titles and abstracts of the 464 citations were screened using the following inclusion criteria: (i) participants were unpaid caregivers such as a spouse, child, other family member, or friend; (ii) care recipients were diagnosed with dementia, Alzheimer’s disease, or mild cognitive impairment; (iii) the care recipient and caregiver resided in a community setting; (iv) depressive symptoms were measured as an outcome; (v) the study used a RCT design; and (vi) the findings were published in a journal article. Studies were excluded if (i) they were review articles, concept analyses, case reports, or expert opinion articles; (ii) were poster or paper presentations; (iii) the sample size was fewer than 10; and (iv) the report did not identify the type of intervention or did not provide enough information to identify which type of intervention was conducted (e.g. only described as psychosocial intervention).
After applying the inclusion and exclusion criteria, 41 studies remained for full-text screening. Authors were contacted for additional information if the studies did not report sufficient statistical data (means, standard deviations, or p- or t-values) to measure effect size. Because 10 studies did not provide additional information, these were excluded. A final sample of 31 studies remained. The search strategy is depicted in Figure 1 using a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart (Moher et., 2015).

PRISMA flow chart of search studies. RCT: randomized controlled trial.
Major study details were extracted from each article. These included characteristics of the caregiver participants (country, age, gender) and study methods (sample size, intervention content, intervention period, duration of one session, facilitators, types of control group, outcome measures of depressive symptoms).
Assessment of methodological quality
Applying the risk of bias tool from the Cochrane Effective Practice and Organization of Care (EPOC, 2017) group, we assessed the methodological quality of included studies. The risk of bias tool evaluates nine criteria: random sequence generation, allocation concealment, similarity of baseline outcome measurement and baseline characteristics, incomplete outcome data, allocation blinding, contamination, selective reporting, and other bias.
The Cochrane EPOC risk of bias tool guides reviewers in how to make a judgment for a low, unclear, or high risk of bias. First, if a random method in the sequence generation process is reported (e.g. computerized random number generator), the study is rated as having a low risk of bias in random sequence generation. If there is an evident report of bias in random sequence generation (e.g. randomization based on admission date), the study is rated as having a high risk of bias. If the study did not mention a specific criterion, it was evaluated as “unclear.” Additional information for making judgments for each criterion is explained in the suggested risk of bias criteria (EPOC, 2017).
Types of interventions
We categorized all interventions into five types based on descriptions by Pinquart and Sörensen (2006): (a) CBT, (b) psychoeducational intervention, (c) emotional support intervention, (d) cognitive rehabilitation for care recipients, and (e) multicomponent interventions. CBT focuses on identifying and modifying maladaptive thoughts, developing a new behavioral pattern, and increasing pleasant leisure activities. Psychoeducational interventions provide information regarding dementia and caregiving-related issues and practice applying new knowledge to individual caregiving situations. Emotional support interventions provide the opportunity to express personal feelings and to reduce social isolation. Cognitive rehabilitation for care recipients was designed to improve or maintain the competence of the care recipients using strategies designed to strengthen cognition because their severity of cognitive decline is highly correlated with depression among their caregivers (Pinquart & Sörensen, 2006). Lastly, multicomponent interventions combine more than one type of interventions such as education, skill building, social support, and/or cognitive strategies (Belle et al., 2006).
In addition, we added a mindfulness-based intervention category given its frequent appearance in the literature. Mindfulness interventions involve a particular type of attention such as increased awareness of the present moment, mind and body movement, and openness and curiosity (Whitebird et al., 2013).
Measures of depressive symptoms
According to the Diagnostic and Statistical Manual of Mental Disorders, depression can be diagnosed when a person has more than two depressive symptoms such as loss of interest, sleep disturbance, or suicidal ideation that exists longer than two weeks (Spector & Tampi, 2005). In this study, we use the term depressive symptoms instead of depression because the vast majority of caregivers self-reported their level of depressive symptoms, rather than having a diagnostic clinical interview for depressive disorders by a health care professional. When a study measured levels of depressive symptoms using self-report scales, such as the Center for Epidemiologic Studies-Depression Scale, the Geriatric Depression Scale, Beck Depression Inventory, Hospital Anxiety and Depression Scale-Depression Score, Montgomery and Asberg Depression Rating Scale, or Cornell Scale for Depression in Dementia as a study outcome, these data were included in the meta-analysis.
Meta-analysis
A standardized mean difference (SMD) and 95% confidence intervals were calculated based on means, standard deviations, p- or t-values, and group sample size (Borenstein, Hedges, Higgins, & Rothstein, 2011). A random effects model was selected to account for different sources of variation among studies besides sampling differences (Deeks, Higgins, & Altman, 2008). Cohen’s d was used for interpreting the magnitude of effect sizes: 0.2–0.49 = small effect, 0.5–0.79 = moderate effect, and ≥0.8 = large effect (Cohen, 1988). Q and I2 statistics were calculated to assess the heterogeneity of the studies. A Q statistic with a p-value ≤ 0.05 was taken as an indication of heterogeneity, and I2 statistics of 0, 25, 50, and 75% were considered as no, low, moderate, or high heterogeneity (Higgins & Green, 2011).
Orwin’s fail-safe N analysis and funnel plot analysis were used to test publication bias. Orwin’s fail-safe N analysis indicates the number of studies required to nullify the results of a meta-analysis (Deeks et al., 2008). Funnel plot analysis shows publication bias if the inverted funnel shape is asymmetrical (Deeks et al., 2008). Statistical analyses were conducted using Comprehensive Meta-Analysis software version 3.0 (Borenstein, Hedges, Higgins, & Rothstein, 2014).
Results
Characteristics of trials, participants, and interventions
The combined sample from the 31 RCTs was 4039 participants, with individual study samples ranging from 16 to 487. The majority of the studies were conducted in the United States (n = 14), followed by the United Kingdom (n = 5), Hong Kong (n = 3), Denmark (n = 2), Italy (n = 2), Spain (n = 2), France (n = 1), the Netherlands (n = 1), and one study conducted in three European countries (Denmark, Poland, and Spain). The mean age of caregivers across studies was 62.2 years (range: 50.5–71.1; SD = 5.2), and most caregivers were women (78.2%, range: 62.5%–100%). Detailed information regarding each study intervention is reported in Table 1.
Summary of intervention studies on caregivers’ depressive symptoms.

CBT: cognitive-behavioral therapy; CES-D: Center for Epidemiologic Studies Depression Scale; NR: not reported.
Intervention effect sizes on caregiver depressive symptoms
Effect sizes according to intervention types are presented in forest plots in Figures 2 to 7.

The effects of CBT on improving depressive symptoms of caregivers of people with dementia.
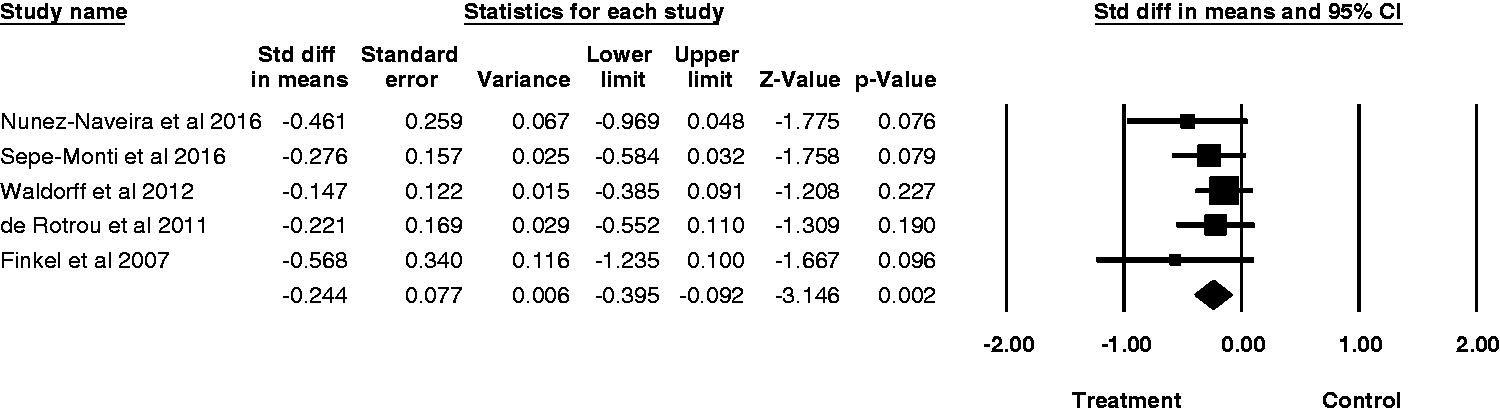
The effects of psychoeducation on improving depressive symptoms of caregivers of people with dementia.
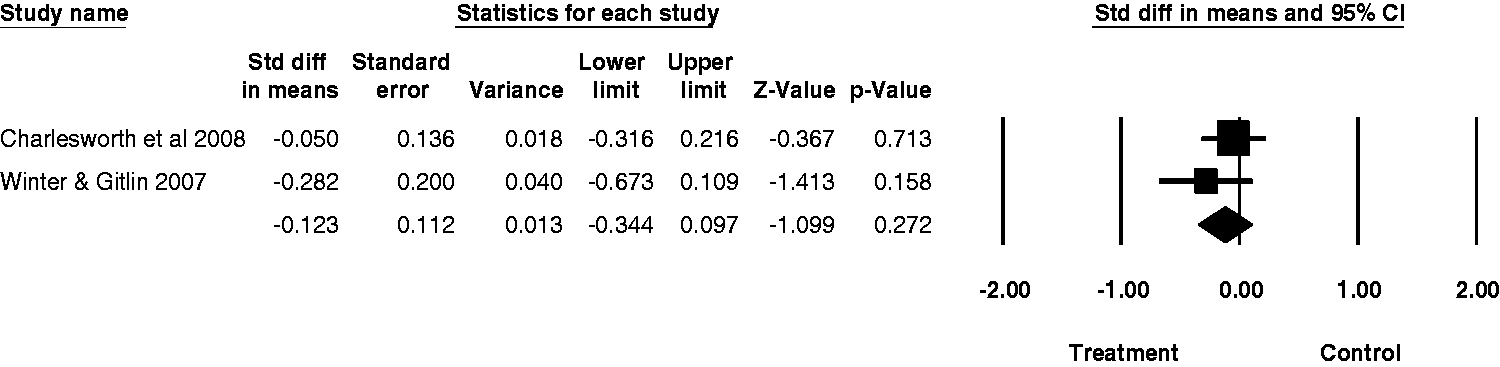
The effects of emotional support on improving depressive symptoms of caregivers of people with dementia.

The effects of cognitive rehabilitation for care recipients on improving depressive symptoms of caregivers of people with dementia.
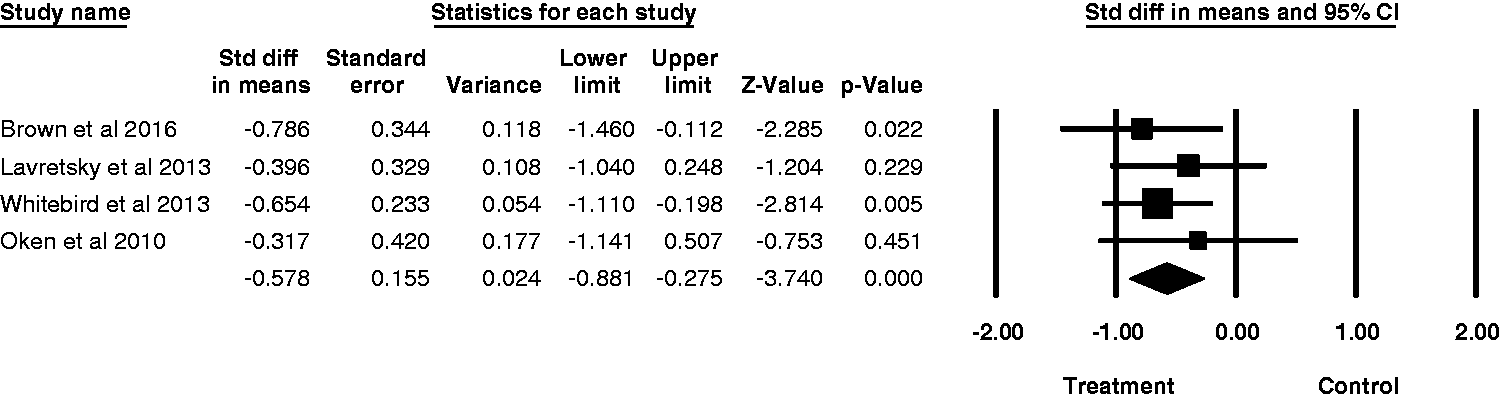
The effects of mindfulness intervention on improving depressive symptoms of caregivers of people with dementia.
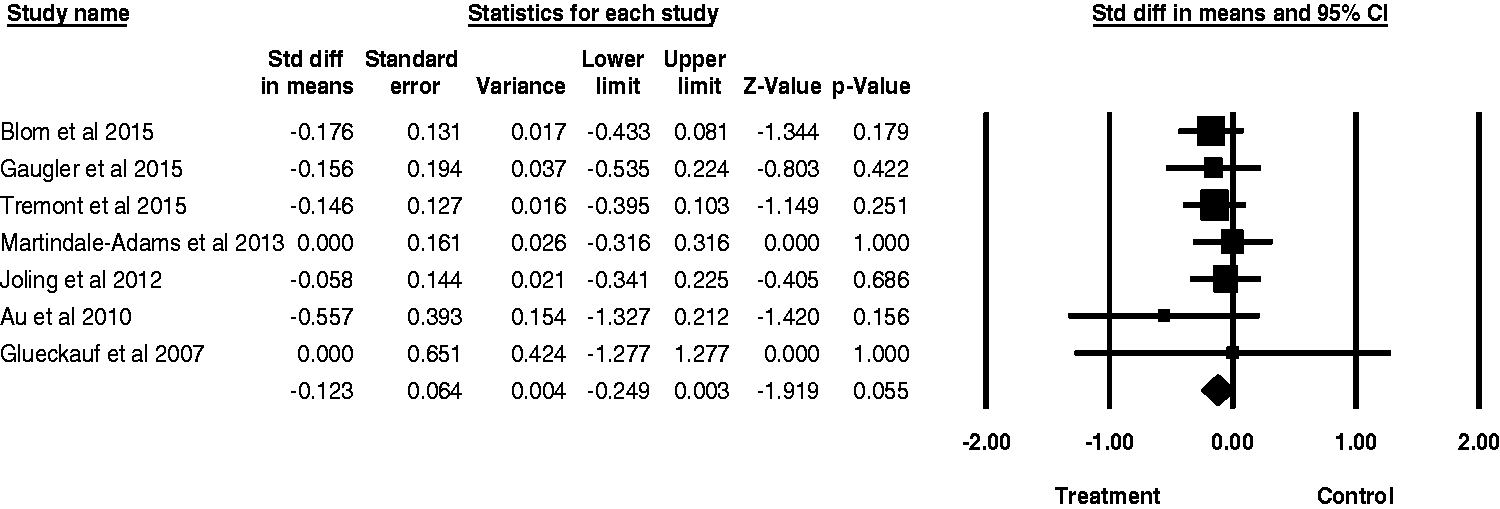
The effects of multicomponent intervention on improving depressive symptoms of caregivers of people with dementia.
CBT
Eight RCTs used CBT interventions. The average number of sessions was 10 (range: 6–14) and the average intervention period was 12 weeks (range: 6–20). Intervention facilitators were trained psychologists, clinicians, psychology graduate students, or senior citizens. Half of the studies were focused on behavioral activation that encouraged caregivers to develop and increase pleasant events. The remaining four studies targeted acknowledging unhelpful thoughts, changing thoughts, and positive reframing.
Meta-analysis of the eight CBT studies (838 participants) strongly suggested that CBT interventions have a large and statistically significant effect (SMD = −0.905; 95% CI = (−1.622, −0.187); p = 0.013) on reducing caregivers’ depressive symptoms. The Q statistic for the test of heterogeneity indicated statistical significance (Q = 133.98; p < 0.001) and the amount of heterogeneity was high (I2 = 94.78%), which indicates variation in the studies in terms of intervention design and study samples. To mitigate the effects of heterogeneity, we applied a random effects model and, to be consistent, used a random effects model when assessing the other interventions.
Psychoeducational intervention
Five RCTs applied a psychoeducational intervention. The average number of sessions was 11 (range: 6–14) and the average intervention period was 20 weeks (range: 6–48). Various health care workers including social workers, counselors, nurses, psychologists, and geriatricians facilitated the interventions. The content included disease progression of dementia, management of care recipients’ behavioral problems, problem-solving skills, and self-care for caregivers. Face-to-face delivery, telephone calls, a web-based course, and an application for mobile devices were used as modes of delivery.
Meta-analysis of these five studies (748 participants) indicated that psychoeducational interventions have a small but very significant effect (SMD = −0.244; 95% CI = (−0.395, −0.092); p = 0.002) on reducing caregivers’ depressive symptoms. The Q statistic for the test of heterogeneity indicated nonstatistical significance (Q = 2.30; p = 0.681) and the amount of heterogeneity was none (I2 = 0%).
Emotional support intervention
Two RCTs used emotional support interventions. One study used telephone calls and the other used face-to-face meetings. At least 24 sessions (daily or weekly contact) were delivered over a six-month period. Trained volunteers or social workers provided emotional support, which involved listening to and validating the caregivers’ emotions.
Meta-analysis of these two studies (339 participants) indicated that emotional support interventions do not demonstrate significant effects (SMD = −0.123; 95% CI = (−0.344, 0.097); p = 0.272) on reducing caregivers’ depressive symptoms. The Q statistic for the test of heterogeneity indicated nonsignificance (Q = 0.93; p = 0.336) and the amount of heterogeneity was none (I2 = 0%).
Cognitive rehabilitation for care recipients
Five RCTs used cognitive rehabilitation for the care recipients. An average of 29 sessions (range: 8–50 sessions) was provided and the average intervention period was 27 weeks (range: 8–48). The facilitators of the intervention were psychologists, occupational therapists, and trained family caregivers. Cognitive rehabilitation was comprised of diverse activities intended to stimulate memories and maintain attention, such as word games, art, and singing.
Meta-analysis of these five studies (933 participants) indicated that cognitive rehabilitation interventions do not demonstrate significant effects (SMD = −0.104; 95% CI = (−0.240, 0.031); p = 0.130) on reducing caregivers’ depressive symptoms. The Q statistic for the test of heterogeneity indicated nonsignificance (Q = 2.75; p = 0.600) and the amount of heterogeneity was none (I2 = 0%).
Mindfulness intervention
Four RCTs applied mindfulness interventions. Three studies delivered 7–8 weekly sessions and one study delivered a daily intervention for eight weeks. Three studies used clinical psychologists or trained instructors to facilitate the intervention while one study used a recorded CD-ROM. Three studies integrated meditative components into the core elements of the mindfulness intervention, such as attention to the present moment and nonjudgmental awareness, while the fourth did not.
Meta-analysis of these four studies (186 participants) indicated that mindfulness interventions have a moderate, significant effect (SMD = −0.578; 95% CI = (−0.881, −0.275); p < 0.001) on reducing caregivers’ depressive symptoms. The Q statistic for the test of heterogeneity indicated nonstatistical significance (Q = 1.17; p = 0.761) and the amount of heterogeneity was none (I2 = 0%).
Multicomponent interventions
Seven RCTs used multicomponent interventions. An average of 11 sessions (range: 6–16) were provided and the average intervention period was 26 weeks (range: 12–48). Psychotherapists, trained therapists, counselors, psychologists, and trained family caregivers facilitated these interventions. Six studies used face-to-face delivery of the intervention and the last one used the internet as a venue for the intervention (Blom et al., 2015). The multicomponent interventions included a broad spectrum of content such as coping strategies, relaxation techniques, cognitive/behavioral skills, communication, psychosocial support, education on dementia, and caregiver well-being.
Meta-analysis of these seven studies (995 participants) indicated that the effects of multicomponent interventions were not significant (SMD = −0.123; 95% CI = (−0.249, 0.003); p = 0.055) in reducing caregivers’ depressive symptoms. The Q statistic from the test of heterogeneity indicated no statistical significance (Q = 2.27; p = 0.894) and the amount of heterogeneity was none (I2 = 0%).
Methodological quality appraisal
Methodological evaluation of each study is presented in Table 2. More than half of the trials examined (64.5%, 20 out of 31 studies) reported specific methods of random sequence generation, for example using a computer-generated algorithm, permuted-block randomization, or dynamic randomization. Allocation concealment was maintained by 35.5% of studies (11 out of 31 studies) using either centralized randomization methods, an on-site computer system, or by blinding an independent statistician. Almost half of the studies (48.4%, 15 out of 31 studies) showed baseline outcome measurements and characteristics were similar across groups by comparing the level of depressive symptoms of treatment and control groups at the baseline, by age and gender, or by controlling for any differences in predepressive levels. Outcomes were assessed blindly in 48.4% (15 out of 31 studies) of included trials. Incomplete outcome data were addressed adequately in most trials (87.1%, 27 out of 31 studies) by testing the difference between completers and noncompleters, stating detailed reasons for dropouts, or showing similar dropout rates of treatment and control groups. Approximately 61.3% of studies (19 out of 31 studies) protected against contamination by delivering the intervention at individual homes, by having random allocation stratified by center, or by delivering the intervention through telephone, Internet, or mobile device. All studies were free of selective outcome reporting bias by presenting all measurements listed in the “Methods” section and in the “Results” section.
Quality appraisal of included studies based on Cochrane effective practice and organization of care risk of bias tool.

Publication bias
To test for publication bias of the meta-analysis, a classic fail-safe N was examined. This meta-analysis combined data from 31 studies, with a z-value of −9.11 and the corresponding two-tailed p-value of <0.001. The fail-safe N was 639, meaning 639 “null” studies would be needed to exceed a two-tailed p-value of 0.05. Additionally, studies included in the meta-analysis were positioned at the top of the funnel plot, indicating high precision and large sample sizes (Figure 8). The mean effect size of this meta-analysis (Figure 8, open diamond) was very similar to the modified effect size (closed diamond) that incorporated published studies as well as possible unpublished studies. Therefore, the meta-analysis indicated no publication bias.
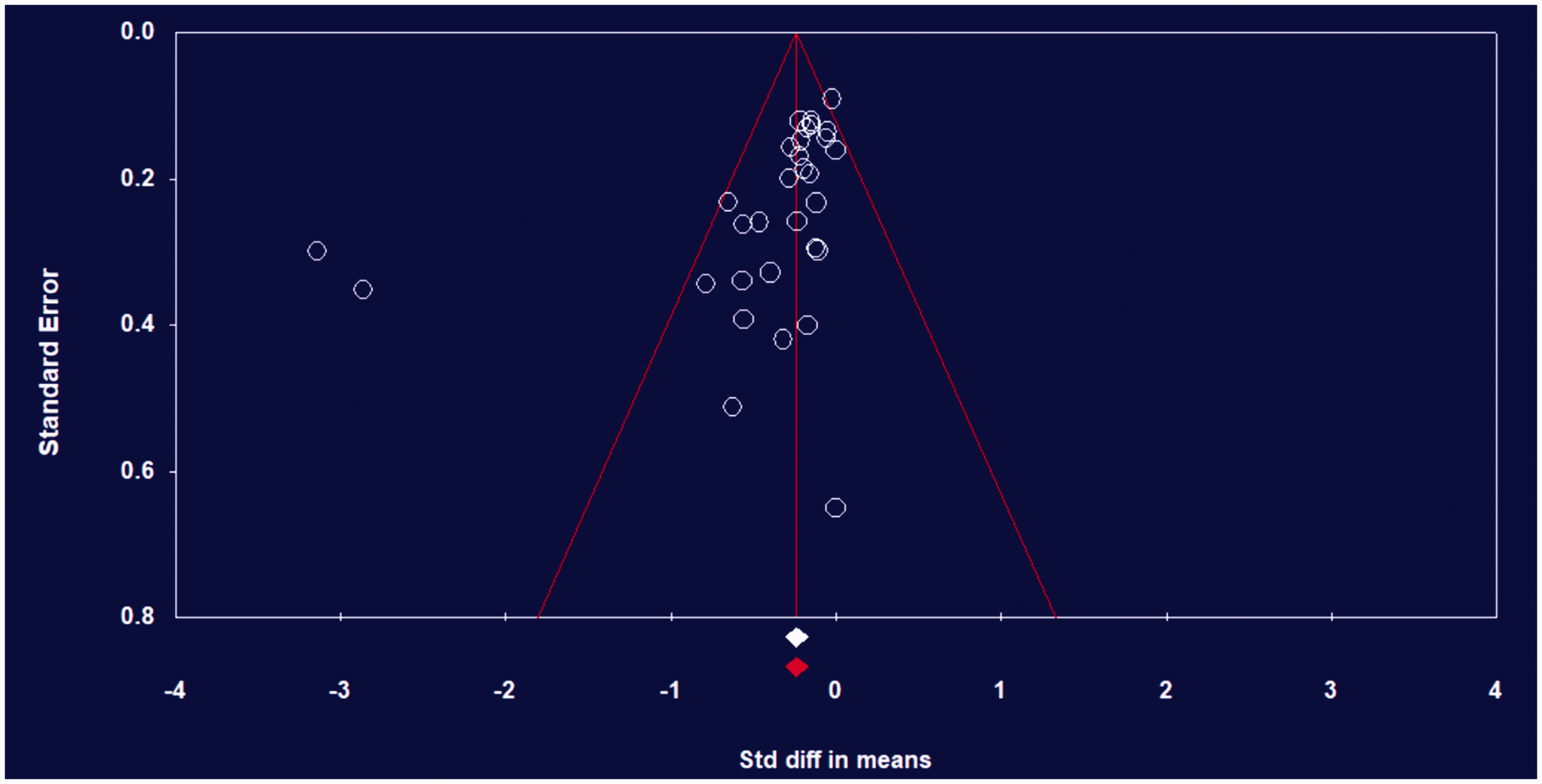
Funnel plot of standard error by standardized difference in means.
Discussion
This present systematic review and meta-analysis investigated 31 RCTs and examined the effectiveness of various types of interventions on depressive symptoms for caregivers of people with dementia. CBT interventions showed the largest and most significant effect on decreasing caregivers’ depressive symptoms. This result supports previous meta-analyses by Pinquart and Sörensen (2006) and Vernooij-Dassen et al. (2011). It is important to mention that three out of the eight RCTs that achieved a significant reduction in depressive symptoms uniformly implemented behavioral activation as a stand-alone intervention. Behavioral activation, which is a component of CBT, comprises a process of identifying leisure activities, scheduling activities, and reinforcing or modifying activities (Au et al., 2015; Moore et al., 2013; Steffen & Gant, 2016). As a result, behavioral activation can increase positive reinforcement, achieve task-oriented goals, and decrease avoidance and negative reinforcement, each of which can counteract depressive symptoms (Chartier & Provencher, 2013). Behavioral activation is easy to tailor to individual preferences and requires minimal time investment from a specialized therapist. For these reasons, the intervention can easily expand the accessibility and dissemination to a larger community (Au et al., 2015; Steffen & Gant, 2016).
Psychoeducational interventions showed a small but significant effect on caregivers’ depressive symptoms, which corresponds with previous meta-analyses (Jensen, Agbata, Canavan, & McCarthy, 2015; Pinquart & Sörensen, 2006). Psychoeducational interventions can be effective in reducing caregivers’ depressive symptoms through the attainment of caregiving skills, ways of self-adjustment, and facilitating a supportive network (Jensen et al., 2015). The effects of psychoeducational interventions on depressive symptoms can be enhanced by increased active participation of the caregivers, such as applying the learned knowledge and skills at home rather than merely providing information (Pinquart & Sörensen, 2006).
Emotional support interventions showed nonsignificant effects. Our results contradict those of Chien et al. (2011), who observed a moderate effect (0.40) of these support interventions. However, Chien et al. (2011) defined support groups more broadly than the present meta-analysis, such as those including educational psychology/training groups as support groups. Future research is needed to test the effectiveness of support interventions with a more consistent definition of the intervention.
Cognitive rehabilitation interventions for care recipients showed a nonsignificant effect. Our results have both similarity and dissimilarity with a previous meta-analysis by Leung, Orgeta, and Orrell (2017), which combined seven cognitive rehabilitation studies and showed a significant effect on caregivers’ depressive symptoms. The authors not only included stand-alone cognitive rehabilitation studies but also included a combination of cognitive rehabilitation and CBT interventions. The discrepancy in statistical significance of cognitive rehabilitation interventions between our results and the previous meta-analysis may be driven by the different classification criteria regarding interventions, although the extent of effect size from both studies was similar.
Mindfulness interventions showed a moderate, significant effect, which is supported by previous studies (Kor, Chien, Liu, & Lai, 2017). Caregivers of people with dementia usually undergo stressful tasks and high degrees of uncertainties related to caregiving. Mindfulness may help caregivers accept their thoughts and feelings without judgment and be more relaxed within the stressful caregiving environment (Kor et al., 2017). However, mindfulness interventions should be used with caution. Mindfulness is a relatively new intervention for caregivers of people with dementia given that the earliest study included in this meta-analysis was conducted in 2010. Additionally, studies have involved comparatively small sample sizes, although this meta-analysis has a larger sample size than the previous one in Kor et al. (2017). Lastly, three RCTs out of four were preliminary or pilot RCTs conducted in the U.S. To confirm the effectiveness of mindfulness interventions, larger sample sizes and various geographical regions should be studied in future research.
Multicomponent interventions showed a no significant effect (p = 0.055) on caregivers’ depressive symptoms, which is supported by previous reports from Olazarán et al. (2010) and Pinquart and Sörensen (2006). The included multicomponent intervention studies discussed the possible reasons for the lack of effect on depressive symptoms such as not targeting individuals’ specific needs (Martindale-Adams et al., 2013) and studying samples having relatively low depressive symptoms (Glueckauf et al., 2007). The most frequently identified reason was the nonadherence and comparatively high dropout rates of participants in the treatment group (Blom et al., 2015; Gaugler et al., 2015; Joling et al., 2012). Multicomponent interventions usually have a long and time-intensive character given that these interventions involve different elements such as education, skills building, and emotional support (Blom et al., 2015). Caregivers may experience more stress or more family conflict by participating in lengthy and time-intensive interventions as these take time away from caregiving responsibilities and add another role of attending intervention sessions (Northouse, Katapodi, Song, Zhang, & Mood, 2010). Future research is needed, focusing on designing a method for caregivers to more easily implement different components of a multicomponent intervention.
In the current meta-analysis, the overall risk of bias decreased over time. In a previous meta-analysis, Thompson et al. (2007) investigated the effectiveness of social support interventions for caregivers of people with dementia and found that only 6.8% of included trials reported methods of randomization and concealment of allocation. However, in this meta-analysis, 64.5% of included studies reported specific methods of randomization and 33.5% reported allocation concealment. In addition, the previous meta-analysis by Thompson et al. (2007) found that 27.3% of included trials maintained blinding while the current study observed 48.4% of included studies assessed outcomes blindly.
Limitations
The limitations of the present study should be considered when interpreting the results. First, the CBT intervention studies had high heterogeneity. Contributors to high heterogeneity can be different geographical regions, a range of the number of intervention sessions, various intervention facilitators, diverse control groups, and different outcome measurements among the studies. Second, the long-term effects of the interventions were not examined. Because of the wide range of follow-up periods across studies, the meta-analysis examined only the immediate effects of interventions. Third, given that the majority of the caregiver participants were women, as in most caregiving research, this study results may not be generalizable to men. Fourth, complete information on intervention fidelity was not reported. Intervention content and delivery modes were examined in this study, but other essential intervention fidelity features such as training of providers, understanding of the intervention, and enactment of skills gained from the intervention were not evaluated because of inconsistent or rare reports from the studies.
Conclusion
As the roles of caregivers of individuals with dementia become ever more critical, maintaining the well-being of caregivers must be priority in public health. This systematic review and meta-analysis incorporating the most recent RCTs confirms that CBT interventions have the largest and most significant effect on reducing caregivers’ depressive symptoms. Increasing activities that caregivers enjoy, which is a part of CBT, can be effective in reducing depressive symptoms. Health care professionals should consider CBT or encourage leisure activities for caregivers of people with dementia. Future research investigating the long-term effectiveness and standardization of CBT procedures is warranted. Although mindfulness interventions showed a moderate effect on caregivers’ depressive symptoms, future large-scale studies are needed to verify these effects.
Improving nonpharmacological interventions to include CBT and mindfulness strategies may contribute to the health of older adults with dementia, their caregivers, and the overall health of the family. Particularly, improved caregiver mental health may play a positive role for allowing care recipients to reside in the community instead of being institutionalized in long-term care facilities. In return, health care costs related to dementia care as well as personal, financial, and organizational resources will be minimized.
Footnotes
Authors’ contributions
ML has contributed to study design, data analysis/interpretation, and writing the manuscript. JHR has contributed to data analysis/interpretation and writing the manuscript. MC has contributed to data analysis. JGA has been involved in conception of the study and critically revising the manuscript. KR has been involved in conception of the study and critically revising the manuscript. ICW has been involved in study conception, design, and revising manuscript substantially.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study supported by University of Virginia, School of Nursing, Lancaster Award.