
Abstract
Background
Health care professionals have poor recognition of cognitive impairment among older patients and often have difficulties in providing care for people with dementia in acute hospitals. There are also reported high levels of stigma and negative staff attitudes towards people with dementia.
Methodology
A one-time survey of staff working on acute medical and orthopaedic wards of five District Health Boards in New Zealand using the ‘Approaches to Dementia Questionnaire’; a 19-item Questionnaire that aims to capture two attitudinal domains (Hope and Person-Centredness), towards people with dementia. A total of 563 questionnaires were distributed. Data were analysed using R.
Results
Three hundred and four (53.99%) respondents completed the survey. Ninety-four of the respondents (31.1%) were aged 51 years or older, and nearly all (88.4%) were women. One hundred and sixty-four of the respondents (53.9%) were registered nurses, 10 were student nurses (3.3%), 24 (7.9%) were healthcare assistants, 70 (23.0%) were allied health professionals, 27 (8.9%) were doctors and 9 (3%) were pharmacists. The mean total score of 72.7 reflected positive attitudes overall on the part of the respondents. Allied health professionals, student nurses and pharmacists had high scores on both scales whilst healthcare assistants scored lowest on both scales.
Conclusion
Overall, the Approaches to Dementia Questionnaire is a useful measure, but it can be difficult to differentiate between genuine attitudinal differences and confounding influences such as level of knowledge and education amongst such a diverse group of participants. Differences between staff may be considered as a reflection of the high level of direct care that is expected of some staff and not of others. Further, the Approaches to Dementia Questionnaire may not be the most appropriate measure to accurately understand attitudes to dementia care in acute environments; and that it more usefully reveals knowledge about dementia rather than attitudes related to real-time practice.
Keywords
Introduction
In 2017 it was estimated that there were 50 million people living with dementia worldwide; this number is expected to double approximately every 20 years to 131.5 million in 2050 (Alzheimer’s Disease International, 2019). Fifty-eight per cent of all people with dementia lived in countries with low or middle incomes in 2010. It is anticipated that this will rise to 71% in 2050 (Prince, Prina, & Guerchet, 2013). In New Zealand in 2011 48,182 people, or 1.1% of the total population had dementia; it is estimated that by 2050 this number will be 147,359, accounting for 2.6% of the population (Alzheimers New Zealand, 2012; Alzheimer’s New Zealand Incorporated, 2008; Alzheimer’s Research Trust, 2010). Future health policy and service delivery will need to reflect the needs of the generation of baby boomers reaching an age where they are susceptible to neurodegenerative disorders (Choi & Twamley, 2013), and other needs identified through advanced disease surveillance, increased longevity, and increased numbers of people living with a comorbid life-limiting illness which may predispose to higher prevalence of dementia (Choi & Twamley, 2013; Whitmer, Gunderson, Quesenberry, Zhou, & Yaffe, 2007), especially when being cared for in the acute hospital setting (Mukadam & Sampson, 2011).
Background
In a systematic review of literature on prevalence, association and outcomes of dementia in older general hospital inpatients, Mukadam and Sampson (2011) found prevalence estimates of between 12.9% and 63%. UK studies have estimated that people with dementia occupy up to one quarter of acute hospital beds at any one time (Alzheimer’s Society UK, 2009; Royal College of Psychiatrists, 2013). Of 598 older patients admitted to acute hospitals in Ireland 25% overall had dementia (Timmons et al., 2015). Travers, Byrne, Pachana, Klein, and Gray (2013) reported a dementia prevalence of 21% across 493 older admissions to medical, surgical and orthopaedic wards in four Queensland teaching hospitals; this rate increased to 47.4% in patients aged 90 years or older. In Japan 15–20% of acute care inpatients have dementia (Fukuda, Shimizu, & Seto, 2015).
Length of stay in hospital is a significant issue and people with dementia tend to use greater resources during their stay (Alzheimer’s Society UK, 2009; King, Jones, & Brand, 2006; Lyketsos, Sheppard, & Rabins, 2000). Longer stay in hospital increases the effect of dementia symptoms on physical health and prescription of antipsychotics, and they are more likely to be discharged to a care home (Alzheimer’s Society UK, 2009). In a Finnish study people with Alzheimer’s disease had 16 more hospital days/person per year (Taipalea et al., 2015) and Dementia Action Alliance, UK (2018) found the average length of stay for people with dementia was 13.25 compared to 10.85 days for people without dementia. However, increased length of stay for people with dementia per year is largely attributed to higher admission rates (Motzek et al., 2018). There are no New Zealand prevalence figures on people with dementia in acute hospitals at any one time.
There is a growing body of evidence that shows that health care professionals have poor recognition of cognitive impairment among older patients (Borbasi, Jones, Lockwood, & Emden, 2006; Lyketsos et al., 2000; Torisson, Minthon, Stavenow, & Londos, 2012); and lack skills in communicating with people with dementia (Allwood et al., 2017; Bamford, Hughes, & Robinson, 2007; Turner, Eccles, Elvish, Simpson, & Keady, 2017). Staff who work in acute hospitals have reported difficulties in providing care for people with dementia predominantly in relation to uncertainty and lack of screening and unclear diagnosis (Pinkert et al., 2018), lack of confidence (Tropea, Brand, LoGiudice, Liew, & Roberts, 2017; Turner et al., 2017) and lack of knowledge and skills (Dewing & Dijk, 2014; Eriksson & Saveman, 2002; Surr & Gates, 2017; Turner et al., 2017). Turner et al.’s (2017) review showed that, in the acute hospital setting, the constraints of the environment and wider organisational context meant staff frequently interpreted responses to the environment by people with dementia as disruptive, much in the manner reported by Dupuis, Wiersma, and Loiselle (2012) in research in the long-term care context, where behaviour was filtered through the lens of pathology, or pathologised. This response is also reflected in the reported high levels of stigma and negative staff attitudes towards people with dementia in acute hospital, identified in the Digby, Lee, and Williams’ (2017) study.
The primary methods used to manage behaviours, perceived by staff as disruptive, has become antipsychotic medications and to some extent psychosocial interventions. Even though prescribing antipsychotic medications is no longer considered a first-line treatment these continue to be used to manage dementia care in hospital environments, nationally and internationally (Kirkham et al., 2017; McIlroy, Thomas, & Coleman, 2014; White et al., 2017). The prescription of antipsychotic medications, however, have not been applied or monitored in a systematic way (Borbasi et al., 2006; White et al., 2017). People with dementia are considered overly demanding of nursing time (Borbasi et al., 2006; Eriksson & Saveman, 2002; Fukuda et al., 2015), with higher perceived strain in caring for older patients with cognitive impairment (Fukuda et al., 2015; Nilsson, Lindkvist, Rasmussen, & Edvardsson, 2012), and threatening to other patients (Eriksson & Saveman, 2002; Fukuda et al., 2015). Risk management approaches are frequently used where the emphasis is on safety rather than well-being and dignity (Digby et al., 2017; Moyle, Olorenshaw, Wallis, & Borbasi, 2008). The hospital’s physical environment and organisational culture, deficits in the knowledge and skills of staff and students, and negative staff attitudes have led to staff struggling to provide care for people with dementia (Merritt, Baillie, & Cox, 2012; Turner et al., 2017).
Study aims and objectives
The research presented in this article was part of a larger three phase mixed method study conducted at five District Health Boards (DHBs) in New Zealand. The rationale for this study was based on a comprehensive report from the United Kingdom (UK) demonstrating that people with dementia receive poor care in acute units (Alzheimer's Society UK, 2009; Health Service Commissioner for England, 2011). Little is known of the experiences of this patient group in acute units in New Zealand. The objective of Phase 1 was to review the recorded experiences from the clinical records of people over the age of 65 admitted to acute medical and orthopaedic wards; the objective of Phase 2 was to investigate the experiences of staff caring for people with dementia across these wards. This involved the administration of the ‘Approaches to Dementia Questionnaire’ (ADQ) and focus group and individual interviews with staff (doctors, nurses, healthcare assistants (HCA), physio therapists, occupational therapists and speech and language therapists) who provided care on the wards identified (reported elsewhere). In Phase 3 family members of people with dementia were interviewed (de Vries, Drury-Ruddlesden & Gaul, 2016). Ethical approval was gained from Central Ethics Committee, New Zealand (MEC/12/EXP/003).
In this paper we report on the results of the administration of the ADQ section of the study. Our aim was to better understand the approaches taken by staff toward people with dementia in the acute environment; this information was then used to augment the qualitative data collected in Focus Group interviews with as many staff as possible who had completed the ADQ.
The Approaches to Dementia Questionnaire
The model of person-centred care (Kitwood, 1997) is considered the cornerstone of caring for older people, including people with dementia (Brooker, 2004; Dewing, 2008); the ADQ (Lintern, 2001) is a commonly used measure for estimating person-centred care approaches and therefore selected as the preferred tool for this study. It is a 19-item questionnaire that aims to capture two attitudinal domains (Hope and Person-Centredness), towards people with dementia (Lintern, 2001). Test–retest reliability for the ADQ was: Total = 0.76; Hope = 0.70; Person-Centeredness = 0.69; as shown by Lintern (2001). A five-point Likert scale, ranging from ‘Strongly Disagree’ to ‘Strongly Agree’, is used to rate the extent to which respondents agree with 19 statements about dementia providing a total score and two sub-scores for ‘Person-Centredness’ and ‘Hope’. The Person-Centred dimension denotes the way in which people with dementia are recognised and responded to as unique individuals, whilst the Hope dimension aims to reveal a sense of optimism/pessimism towards the abilities and the future of people with dementia. Possible scores for the ADQ Total scale range from 19 to 95; possible scores for the ADQ Hope subscale range from 8 to 40 and possible scores for the ADQ Person-Centred Scale range from 11 to 55 (Lintern, 2001).
The ADQ has been the scale of choice in a number of studies undertaken, predominantly in long-term care facilities (Kada, Nygaard, Mukesh, & Geitung, 2009; Lintern, Woods, & Phair, 2000; MacDonald & Woods, 2005; Moyle, Murfield, Griffiths, & Venturato, 2011; Spector & Orrell, 2006; Winzelberg, Williams, Preisser, Zimmerman, & Sloane, 2005; Zimmerman et al., 2005), the environment in which the scale had been designed for use (Lintern, 2001). In Northern Ireland, Barry, Parsons, Passmore, and Hughes (2013) undertook a study where 530 community pharmacists were asked to complete the ADQ focusing on the management of pain in people with dementia. They concluded that community pharmacists have positive attitudes towards this patient population. Travers, Beattie, Martin-Khan, and Fielding (2013) administered the ADQ to 524 registered nurses and allied health professionals (AHP) working in Queensland in community services; residential care, acute care and sub-acute outpatient and emergency services (but not hospital wards). The team confirmed their hypothesis of positive relationships between education, training, self-confidence and positive attitudes towards people with dementia.
ADQ administration in acute hospital environments include a descriptive study of 100 Korean registered nurses working in acute care settings in two hospitals in southern Korea, seeking to identify and describe Korean nurses’ attitudes towards older people with dementia (Kang, Moyle, & Venturato, 2011). The researchers used a number of measures, including the ADQ. They found moderately positive attitudes towards older people with dementia in the acute care setting and concluded that the environment, work routine and technology may influence the likelihood of negative attitude towards people with dementia and that nurses in medical units had more positive attitudes toward people with dementia than did those in surgical units.
The ADQ was used by Surr, Smith, Crossland, and Robins (2016) as part of a repeated measures design evaluation of a specialist training programme for acute hospital staff regarding improving attitudes, satisfaction and feelings of caring efficacy, in provision of care to people with dementia in an NHS Trust in the North of England in the UK. Forty acute hospital staff, 90% of whom were nurses working in clinical roles, participated in the study. A significant positive effect was found on the ADQ between baseline and after completion of Foundation-level training. It was also used by Banks et al. (2014) as a pre and post measure of an education intervention for staff working in acute settings in their evaluation of The Scottish Dementia Champions programme. Similar to Surr et al. (2016) they identified a significant shift towards more positive attitudes to dementia, particularly associated with person-centred approaches.
Method
The ADQ (Lintern, 2001) was used to undertake a one-time survey of staff (nurses, doctors, (HCA), occupational therapists, physio therapists, speech and language therapists and pharmacists) working on acute medical and orthopaedic wards of five DHBs in New Zealand; two in the South Island and three in the North Island. Ethical approval was granted by the Multi-Region Ethics Committee of New Zealand (MEC/12/EXP/003). Directors of Nursing at each site were the champions of the research in terms of gaining permission and steering the research request through the appropriate channels within the acute hospital systems. The lead researchers liaised with the Director of Nursing at each site to identify clinical research links (administrative, nursing medical and AHP. Once approval had been achieved, site link nurses were identified. Link nurses liaised with researchers and facilitated distribution and collection of flyers, letters, consent forms and survey instrument to the multidisciplinary teams of staff working on the medical and orthopaedic wards (in three DHB sites orthopaedic patients were on surgical wards) and who were directly involved in the care of persons with dementia.
Administration of the ADQ
Respondents were identified by the link nurse using the weekly staffing roster. All participants regularly undertook care of people with dementia in an acute medical or surgical/orthopaedic unit. Each respondent completed the questionnaire in private, placed it in a sealed envelope and posted it into sealed collection boxes located in each of the clinical areas.
The study population was 563 multidisciplinary staff who regularly participated in care of patients with dementia (identified by the link nurse using the weekly staffing roster. Of the 563 surveys distributed, initially there were 299 respondents (53.11%), however, this rose to (56.66%) after a verbal reminder delivered through the staff meetings network (n = 319), which is considered a good response in questionnaire survey research (Carley-Baxter et al., 2009). Of these, 15 had missing data and were removed from the data set, resulting in a final data set of 304 care provider respondents (53.99%). A front page of socio-demographic terms was attached to the ADQ covering: role, gender, age, ethnicity, hours worked per week, years of work experience and specialised training in dementia care facilitated description of socio-demographic characteristics of the respondents. However, as the survey was otherwise non-identifiable, this limited our ability to discern how non-responders differed from responders.
Data analysis
The ADQ data were analysed using R, version 3.4.4 (R Core Team, 2018). 1 Cronbach’s coefficient alpha was used to measure internal consistency of the ADQ scores on Hope and Person-Centred sub-score attitude scales. Descriptive and inferential statistics are provided followed by linear models for the Hope and Person-Centred scores.
Summary statistics are presented for test scores with confidence intervals where appropriate. The Shapiro–Wilk test for normality of the score data was used to ascertain whether parametric or non-parametric tests were required for further analysis. Cronbach’s alpha is reported for the Hope and Person-Centred results to provide an indicator of internal consistency of the cohort responses.
The impact on test scores of factors including ethnicity were initially examined (using the Kruskal–Wallace test as the preferred test of difference of central tendency) these provided an initial illustration of where those factors, including ethnicity, influenced the resulting score. Correlations between test score and continuous variables are reported using Pearson’s r as an initial view of the impact of variables including age.
Linear models were then developed to provide a guide to the overall relative impact of factors and continuous variables on the resulting score; these are presented both for Hope, Person-Centred and total scores. These models show the relative importance of the various influences on the scores and provide an indication (using the R2 measure) of how much of the total score variance can be accounted for by demographic and other factors. These models also provide an approximate comparison to the results of Kada et al. (2009). Diagnostics used on the models included tests of normality of the residuals and reports of variance inflation factors to show the extent to which parameter variances have been adversely impacted by collinearity.
Results
Demographic data
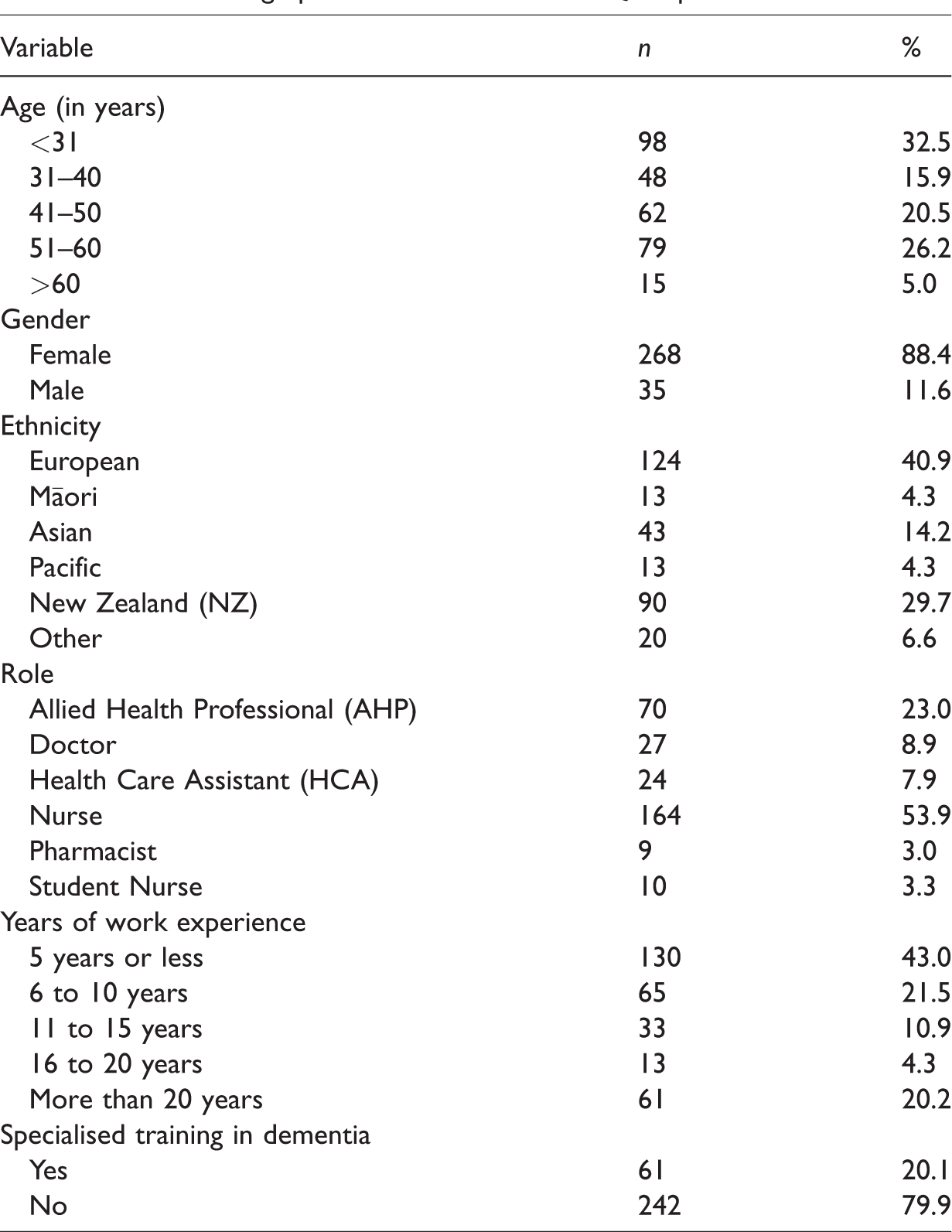
Three hundred and four (53.99%) respondents completed the survey. Ninety-four of the respondents (31.1%) were aged 51 years or older, and nearly all (88.4%) were women. The majority of respondents identified ethnically as European, 124 (40.9%) or New Zealand, 90 (29.7%). Thirteen (4.3%) identified as Māori and the same number as Pacific; 43 (14.2%) as Asian and the remaining 20 (6.6%) as other. One hundred and sixty-four of the respondents (53.9%) were registered nurses, 10 were student nurses (3.3%), 24 (7.9%) were HCAs, 70 (23.0%) were AHPs, 27 (8.9%) were doctors and 9 (3%) were pharmacists. Only 61 (20.1%) of respondents had specialist training in dementia care and 195 (64.6%) had 10 or fewer years of working experience (Table 1).
Socio-demographic characteristics of ADQ respondents.
Predictors of Hope, Person-Centred and Total scores. a
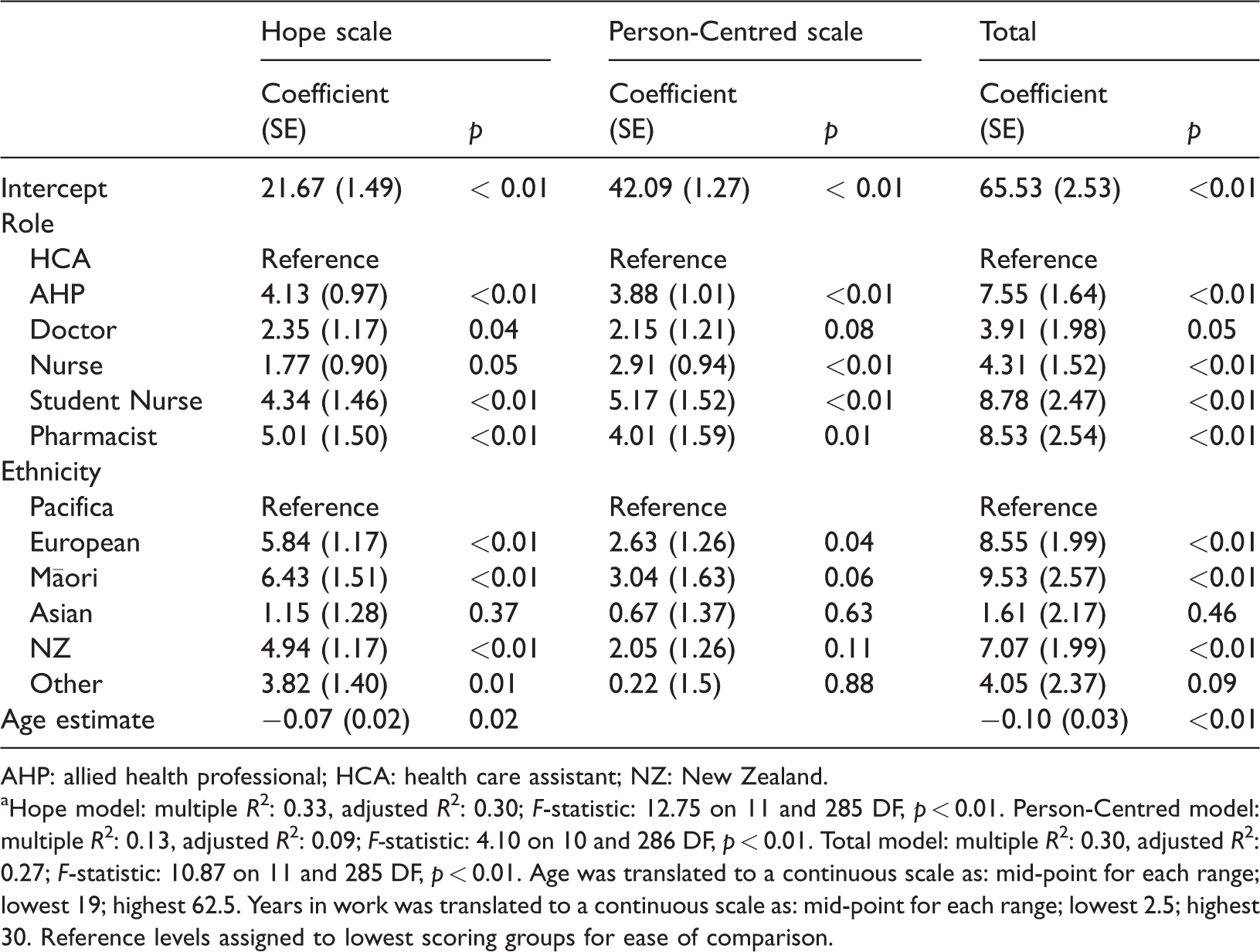
AHP: allied health professional; HCA: health care assistant; NZ: New Zealand.
aHope model: multiple R2: 0.33, adjusted R2: 0.30; F-statistic: 12.75 on 11 and 285 DF, p < 0.01. Person-Centred model: multiple R2: 0.13, adjusted R2: 0.09; F-statistic: 4.10 on 10 and 286 DF, p < 0.01. Total model: multiple R2: 0.30, adjusted R2: 0.27; F-statistic: 10.87 on 11 and 285 DF, p < 0.01. Age was translated to a continuous scale as: mid-point for each range; lowest 19; highest 62.5. Years in work was translated to a continuous scale as: mid-point for each range; lowest 2.5; highest 30. Reference levels assigned to lowest scoring groups for ease of comparison.
Statistical analysis
Summary
The mean total score of 72.7 (95% confidence interval for the mean of 71.9 to 73.6) may be considered as reflecting positive attitudes overall on the part of the respondents. Internal consistency, as measured by Cronbach’s α was 0.70 for the Hope scale and 0.76 for the Person-Centred scale. The summary statistics for the Hope domain were a mean score of 25.80 (SD 4.37; range 12 to 36; 95% CI of 25.30 to 26.29); and for the Person-Centred score, the mean was 46.95 (SD 4.19; range 37 to 55; 95% CI of 46.48 to 47.42). Shapiro–Wilk normality tests on the distributions of the Hope and Person-Centred scales found a poor fit for a normal distribution (at p < 0.05) and hence non-parametric comparisons for between-group scores were preferred.
Median scores by ethnicity or the Hope scale were: European 27; Māori 28; Asian 22; Pacific 21; NZ 26; and Other 24.5. For the Person-Centred scale they were: European 48; Māori 48; Asian 45; Pacific 44; NZ 47 and Other 45. These scores are shown on the charts (Figures 1 and 2) with a normalised scale to facilitate comparisons between scales.
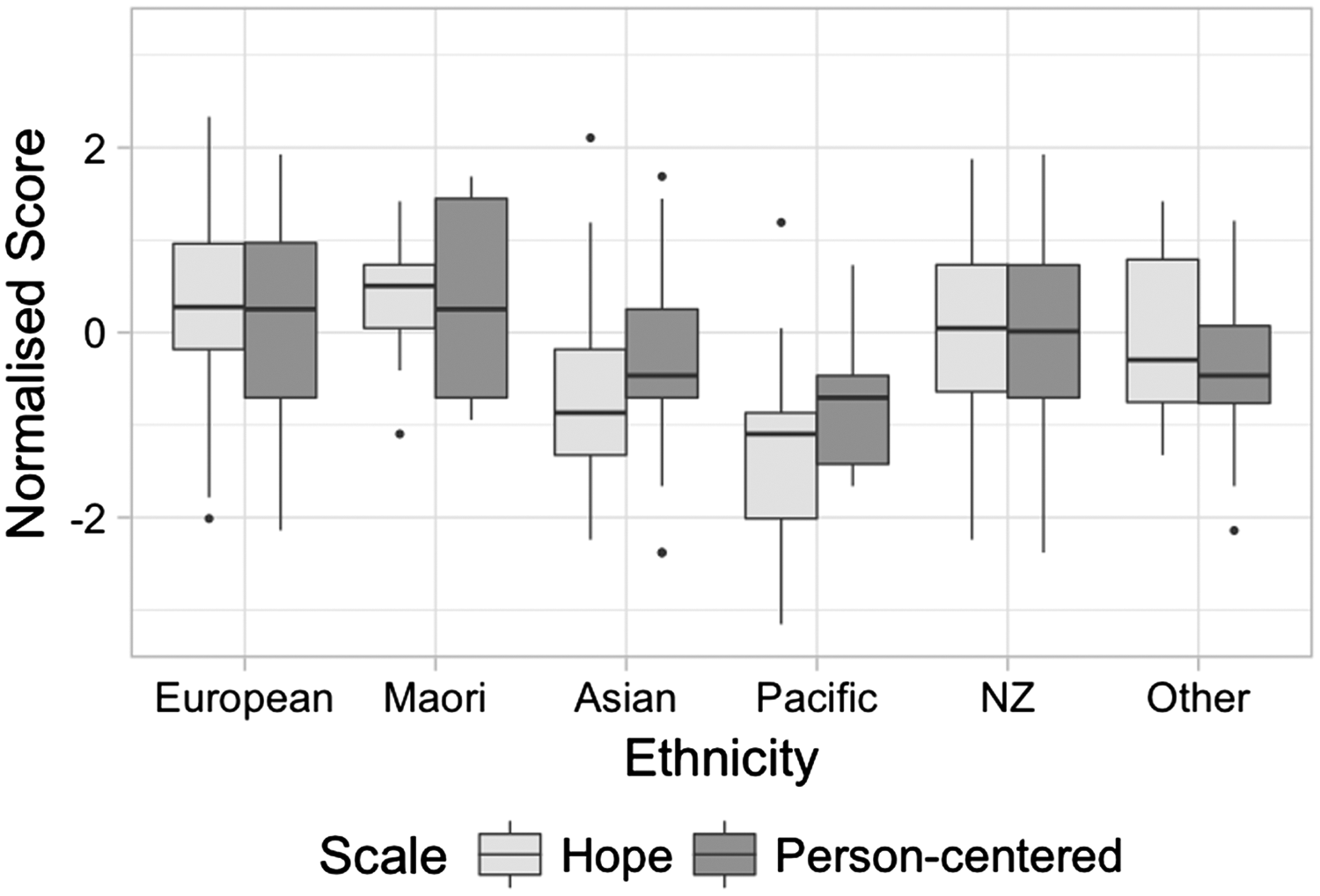
Person-Centred and Hope scale score (normalised) by ethnic group. Scores that are more than 1.5 times the interquartile range above the upper quartile or below the lower quartile are shown in the boxplots as outliers.
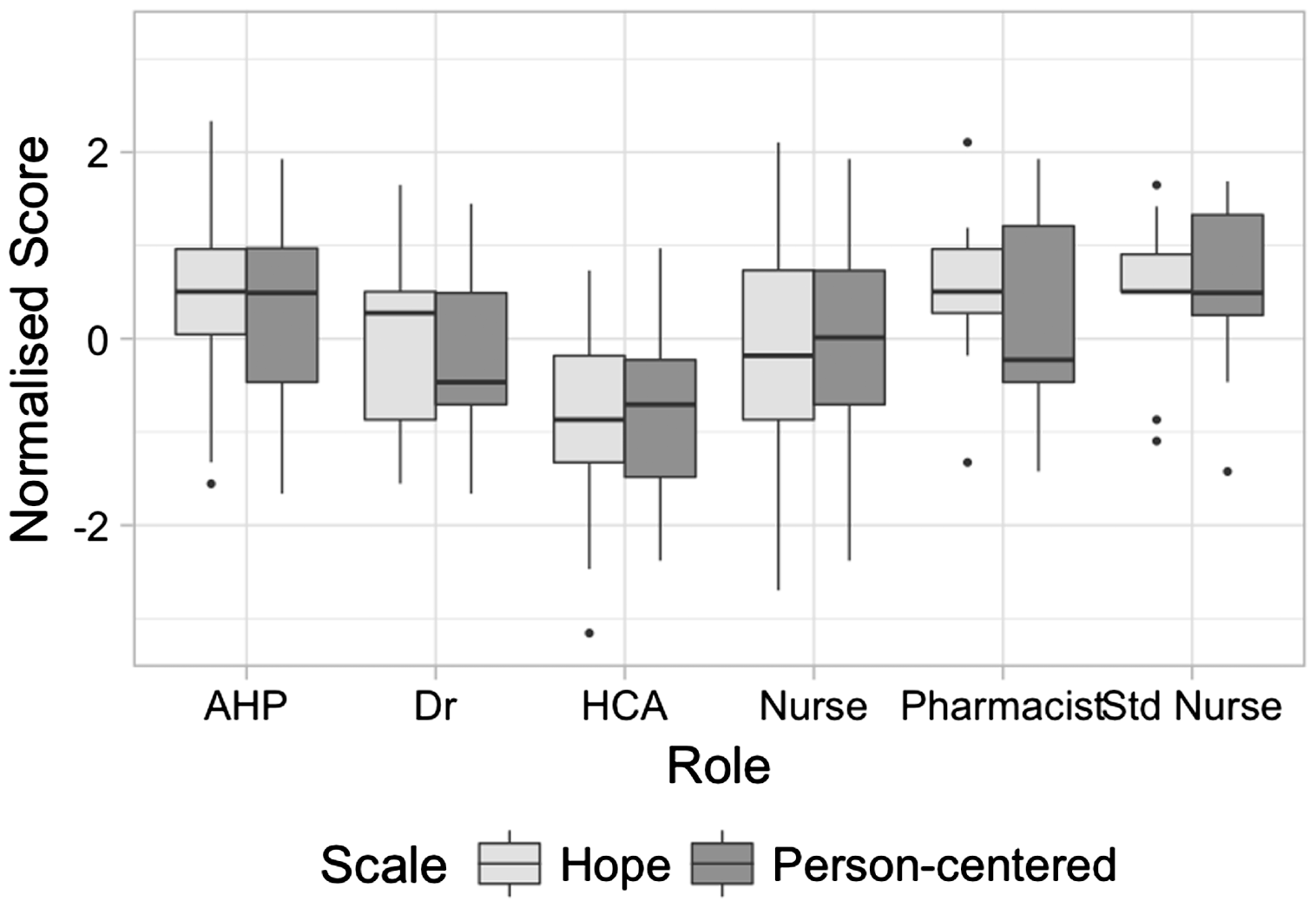
Person-Centred and Hope scale score (normalised) by role.
The box plots on the normalised Hope and Person-Centred scales by ethnicity (Figure 1) show the Māori ethnic group with the highest median score of 28 for the Hope scale; the median score for the Person-Centred scale, for Māori and European ethnicity are the highest of those groups, both at 48.
The Māori scores for the Hope scale also have the smallest interquartile range when compared to other ethnicities. Ethnicities recorded as Asian or Pacific have the lowest median scores for the Hope scale at 22 and 21 respectively; they also have lower scores, on the Person-Centred scale, than other ethnicities. It can also be seen that there is an association between the scores for each scale – ethnicities scoring high on one scale also tend to score high on another scale.
Median scores by role for the Hope scale were: AHP 28; doctor 27; HCA 22; nurse 25; student nurse 28; pharmacist 28. For the Person-Centred scale they were: AHP 49; doctor 45; HCA 44; nurse 47; student nurse 49; Pharmacist 46. These scores are shown on the charts with a normalised scale to facilitate between-group comparison to the Person-Centred scores.
The box plots (Figure 2) on the normalised Hope and Person-Centred scales by role show AHPs and student nurses having high scores on both scales with a median of 28 for both roles for the Hope scale and a median of 49 for both roles for the Person-Centred scale. The HCA participants scored lowest on both scales with median scores of 22 and 44 for Hope and Person-Centred measures, respectively. It should be emphasised that this sense of a ‘low’ score is relative and does not necessarily reflect a view lacking in hope or person-centredness on the part of the HCA participants.
Differences between roles and between ethnicities were analysed for both types of score using the Kruskal–Wallis test. Hence for the Hope scale scores a test was made for overall differences of (median) scores between roles; for the Hope scale scores a test was made for overall differences of scores between ethnicities and similarly for the Person-Centred scale scores. Each of the four tests gave p < 0.01 for between group differences.
The correlations between Hope scale and age, and Person-Centred scale scores and age were −0.19 and −0.12, respectively. Those between Hope scale and years of work, and Person-Centred scale and years of work were −0.09 and −0.07, respectively. On the Hope scale, median scores for males and females were 26 and 25, respectively; for Person-Centred scores they were 47 and 46, respectively. On the Hope scale those with specialised training in dementia had a median score of 27; those without had a median score of 26. On the Person-Centred scale both groups had a median score of 47. Each of these factors is included for consideration in the linear model presented below with the initial view of these influences being confirmed in the finally selected model where, from these variables, age alone is retained as a predictor and that only in the case of the Hope score.
Predictors for Hope and Person-Centred scores
Linear models for Hope and Person-Centred scores were derived by backward elimination – removing the less influential variables to produce a more parsimonious model. Values for R2, adjusted R2 and F-statistics are also summarised below (see Table 2).
Roles, for both models, showing the largest increases (over the reference levels) are AHPs, student nurses and pharmacists; with p < 0.05 in each of those cases. Ethnicity appears to have a less consistent impact when comparing the Hope and Person-Centred scores, with the Person-Centred score having smaller differences between ethnic groups and overall lower p values. The Hope score model also accounts for a higher proportion of the score variance, this being 0.30 and 0.09 (adjusted R2) for the Hope and Person-Centred models, respectively.
For the Hope score model, HCA and Pacifica were the lowest scoring groups for role and ethnicity, respectively; the highest scoring groups were pharmacist and Māori for role and ethnicity, respectively. The age parameter of the Hope scale model at −0.07, shows a decrease of 0.7 for every 10 years of age of the respondent.
For the Person-Centered model, HCA and Pacifica were the lowest scoring groups for role and ethnicity, respectively; the highest scoring groups were student nurse and Māori for role and ethnicity, respectively. The age parameter was eliminated from this model during the backward elimination process.
A linear model is also given for the total scores. For this model HCA and Pacifica were the lowest scoring groups for role and ethnicity, respectively; the highest scoring groups were student nurse and Māori for role and ethnicity, respectively. The age parameter of the Hope scale model at −0.1 shows a decrease of 1.0 unit for every 10 years of age of the respondent.
HCA scores compared to all other participants
An examination of scores for the HCA group, compared to all other participants, shows lower scores for both subscales for HCA participants. For the Hope subscale the HCA group median was 22 and that for the remaining combined roles was 26; for the Person-Centred subscale the HCA group median was 44 and that for the remaining combined roles was 47. (The difference in each case yielding a significant difference at p < 0.01 for the Wilcoxon rank-sum test.) Normalised scores for these groupings on both scales are shown in Figure 3.
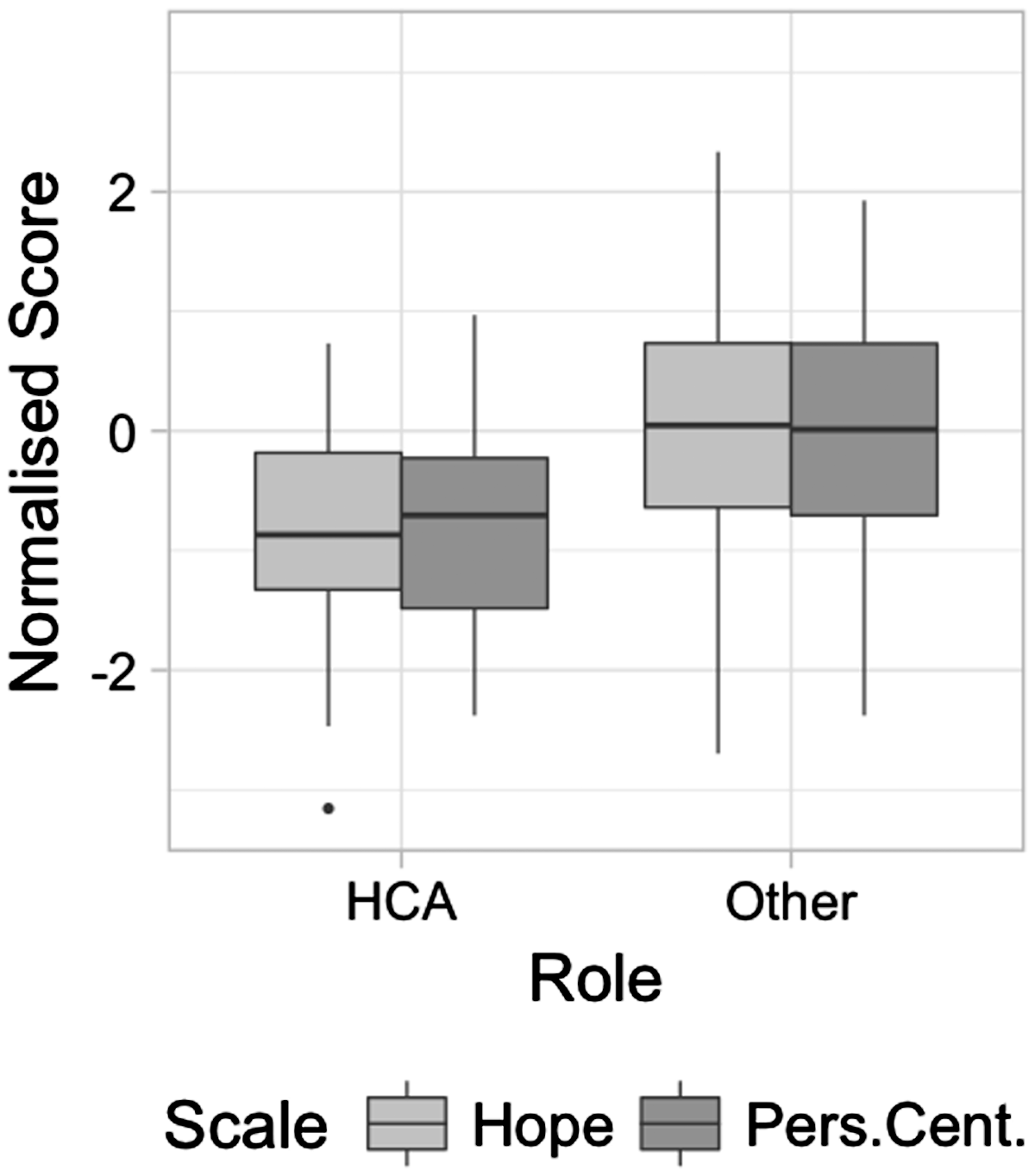
Hope and Person-Centred scores for HCA compared to all other participants.
Individual question analysis
A basic analysis of the percentage of respondents selecting ‘Agree’ or ‘Agree strongly’ to each of the questions in the Hope and Person-Centred survey was conducted. The highest percentages, of 98.7% (n = 300) and 98.4% (n = 299) respectively, were ‘People with dementia need to feel respected, just like anybody else’ and ‘It is important to respond to people with dementia with empathy and understanding’; both questions are part of the person-centred set and in each case the ‘Agree strongly’ response is at the high end (5) of the scale. The lowest number of ‘Agree’ or ‘Agree strongly’ responses were for the question, ‘It doesn't matter what you say to people with dementia because they forget it anyway’, with 3% (n = 9). The question ‘Once dementia develops in a person, it is inevitable that they will go downhill’ has responses with similar numbers when comparing those answering Agree or Strongly agree (n = 107), with those answering Disagree or Strongly disagree (n = 102), with a Chi-squared test failing to find a significant difference between the proportions (p = 0.73).
Discussion
The mean total score of 72.7 (95% CI 71.9 to 73.6) reflects positive attitudes overall and is comparable to the corresponding 70.3 reported by Kada et al. (2009) and Moyle et al. (2011). Our finding, that age of respondents – in the case of Hope scale – showed a decreased score with increasing age, was also in keeping with Kada et al. (2009) who found that person-centred attitude was lower among respondents who were over 50 years old. Kada et al. report on this at length, based on their findings, suggesting that attitudes towards old age become more negative as an individual grows older and that negative emotions increase with age where the subsequent burnout leads to less positive attitudes. They do, however, propose that more research needs to be undertaken to uphold this finding.
Due to the small number of studies using the ADQ in the acute hospital environment, plus the different ways in which the tool was applied and analysed, it is difficult to compare like-with-like from these studies. Comparable to the Kang et al. (2011) study – based in acute environments – gender and years of experience were not found to be predictors of Hope or Person-Centred scores in the cohort we studied. In our study, for both the Hope and Person-Centred cases, gender, years of work and specialised training in dementia were eliminated from the final model. We did not collect detail on the types of education undertaken, and Kang et al. (2011) did not include specialist education in dementia care as an item in their demographic data.
In regard to specialist training in dementia our findings are not in keeping with Kada et al. (2009) who found specialist training in dementia care increased overall scores in both Hope and Person-Centredness. They are more in keeping with MacDonald and Woods (2005) where they found that that increased person-centred attitudes were linked to better recognition of cognitive impairment independent of training and experience and that education and training was not statistically significant to improving hope and person-centredness.
However, Zimmerman et al. (2005) found that staff who perceived themselves to be better trained in dementia care were more likely to adopt person-centred care. They also found that hopeful or person-centred attitudes were more often adopted by staff with higher education and those working between one and two years versus longer periods of time, which is in keeping with our findings where the more highly educated AHPs and pharmacists reported higher levels of both hope and person-centredness.
Influence of the respondent professional role
Of note, in our findings, and which has not been studied in acute environments, was that individual professional role categories for both models show the largest increases over the reference levels for AHPs, student nurses and pharmacists with p < 0.01 level in each of those cases; whilst HCA participants scored lowest on both scales compared to all other participants.
In attempting to explain our findings we considered some of the paradoxes within the data. Of interest was that the group, who are the main providers of dementia care and work closely and constantly with people with dementia, are HCAs. HCAs were found to have the lowest scores for Hope and Person-Centred scales, whilst AHPs, student nurses and pharmacists had the highest scores. A possible explanation for this is that HCAs become ‘burnt-out’ as a result of the pressures of caring for people with dementia in the acute environment (Banks et al., 2014; Digby et al., 2017; Eriksson & Saveman, 2002; Nolan, 2007) thus impacting on their attitudes towards this patient group; whereas AHPs and student nurses spend specifically designated and protected time with people with dementia – pharmacists rarely have extended direct contact with this patient group. It may also be explained by the nature of the clinical presentation of people with dementia in the acute environment in that they are also acutely ill and experiencing delirium (Ahmed, Leurent, & Sampson, 2014; Timmons et al., 2015) and consequently more difficult for HCAs to manage their care in ways that they would within care home facilities.
The above explanation may also illuminate the high scoring results of the questions, ‘People with dementia need to feel respected, just like anybody else’, and ‘It is important to respond to people with dementia with empathy and understanding’ (Person-Centred); whilst the ambivalent scoring for ‘Once dementia develops in a person, it is inevitable that they will go downhill’ (Hope). It may be the case that staff understand and aspire to be person-centred but may come to believe that there is little hope for people with dementia or experience a sense of ‘hopelessness’ as a result of the pressures within the acute environment in which they work (Banks et al., 2014; Bower, 2016; Fukuda et al., 2015). This aspect of the results warrants further investigation.
Influence of the respondent ethnicity
HCAs and Pacifica were the lowest scoring groups for role and ethnicity respectively with pharmacists and Māori the highest scoring groups, upheld in both the scores. The influence of ethnicity has not been examined in other studies so was of interest in this research. We found that Māori ethnicity scored higher on both the Hope and Person-Centred scales when compared to other ethnicities, whilst Asian and Pacifica ethnicities had the lowest median scores. An explanation for this may be that approaches taken to health care by Māori are influenced by cultural systems and frameworks that emphasise more holistic models of care (Mason Durie, 2017) and where older people, regardless of their health status are generally held in high esteem (Edwards, 2010); this is an area warranting further research.
A possible explanation for the low scores of Asian staff could be the nature of the questions used in the ADQ, which was designed for people who have English as a first language, and may not have been clearly understood by a group where English is their second language. Although there is an expectation that staff working in New Zealand hospitals attained a minimum IELTS score of 7.0, there always remains the possibility that questions posed, as they are in the ADQ, were misunderstood. Also cultural values in regard to people with dementia vary across cultures (Brooke, Cronin, Stiell, & Ojo, 2017). For example, in the context of the US study – set in care home facilities (Zimmerman et al., 2005) – it was shown that Black and other minority staff were less likely than Whites to report person-centred care.
Usefulness of ADQ as a measure in acute care
Consideration of whether the ADQ is the most appropriate tool to be used to understand attitudes to dementia care in acute environments is an important conclusion following this study. We believe that the ADQ may more appropriately be referred to as a scale that measures ‘knowledge’ about dementia rather than attitudes related to real-time practice. Banks et al. (2014) and Surr et al. (2016) posited that there was a significant positive effect using the ADQ, as a pre and post measure associated with dementia education and training programmes, for staff working in an acute hospital setting. However, in both studies, although not made explicit, it appears that the ADQ was administered immediately post the education intervention, therefore this more likely measures knowledge rather than changes in real-time care of people with dementia over time. That is, their results may not reflect actual changes in practice but reflect new knowledge acquisition. Measures that, for example, examine empathy (Digby, Williams, & Lee, 2016; Pulsford, Duxbury, & Carter, 2016) and compassion (Tadd et al., 2011), as personal qualities, may more accurately illustrate attitudes and responses toward people with dementia. This approach was suggested by Lintern (2001) herself, who proposed that attitude-based training may be a better approach to improving person-centred care for people with dementia.
Implications for practice
The implications for education and practice arising from this study suggest that attending to staff burnout, especially those who provide direct care for people with dementia, is an important consideration within support structures for staff in acute hospitals. Training and education programmes, in these environments, should be reviewed to reflect the need for attitude-based training, particularly taking into consideration that measures of empathy and/or compassion may better reflect staff attitudes towards people with dementia.
Strengths and limitations
The scale scores illustrate relative attitudes between the demographic groupings as shown; there is however some difficulty relating the scores to baseline measures or absolute location of person-centred or hope related positioning on any widely accepted reference points. These scores can possibly be influenced by a knowledge of what stance on attitudes is perceived as expected of the respondent rather than underlying practice, attitudes or dispositions. Clearly the results of this study can lead to certain conclusions when viewed from the standpoint of the analysis of ethnicity and another is apparent when looked at through role, leading to a tension between the two approaches. As the survey was non-identifiable our ability to discern differences between respondents and non-respondents was limited.
Conclusion
Overall, the cohort in this study demonstrated positive attitudes towards people with dementia. However, the differences between roles are a matter of interest and may be accounted for in a number of ways. If, as we suggest, the differences between HCAs and professionals in other roles can be considered as a reflection of the high level of direct care that is expected of HCAs for people with dementia, who are also acutely ill with likely delirium, and the possibility of burn-out in this group, then HCA support needs should be more carefully addressed within the acute hospital environments where they are undertaking an extremely demanding role.
Our results show that specialist training in dementia made no difference to respondent scores; this suggests that attention needs to be given to the type of education and training that all staff in acute hospitals receive within the context of that specific environment. If the ADQ is judged to be more of a measure of knowledge rather than attitudes or approaches then approaches to education and training should be on development of that attitude-based training rather than knowledge acquisition.
We were particularly interested in ethnicity; the only study that addressed this, albeit briefly, was that of Zimmerman et al., (2005). We could find no other studies that considered differences across ethnicities in provision of care for people with dementia using the ADQ. A possible explanation for lower score for Asian and Pacifica groups could relate to language difficulties and prevailing level of education in those groups. Overall, we believe that the ADQ is a useful measure, but it can be difficult to differentiate between genuine attitudinal differences and confounding influences such as level of knowledge and education amongst such a diverse group of participants. Further, the ADQ may not be the most appropriate measure to precisely understand attitudes to dementia care in acute environments. We suggest that the measure may more usefully reflect knowledge about dementia rather than attitudes related to real-time practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from Victoria University of Wellington, New Zealand.