
Abstract
Objectives
Within an implementation study, we investigated the effectiveness of a combined community-based day care programme for persons with dementia and their carers versus traditional psychogeriatric nursing home-based day care. The effects on needs, sense of competence, burden and quality of life of the family carers were studied.
Methods
A pretest–posttest control group design among family carers of people with dementia who joined community-based day care centres (n = 67) or nursing home-based day care centres (n = 64).
Results
After six months, family carers using community-based day care more often expressed an unmet need for support regarding psychological distress than carers utilising nursing home-based day care. No effect of community-based day care on sense of competence was found. However, carers with a low sense of competence at baseline using community-based compared to nursing home-based day care became less emotionally burdened by behaviour and mood problems of their relative.
Introduction
In 2017, in the Netherlands, about 300,000 family carers cared for about 270,000 people with dementia. Family carers play an important role in the care for community-dwelling people with dementia: on average they care for their relatives 20 h a week during five years (Dutch Alzheimer Association, 2017). As a result of this caregiving role, and in particular the experienced difficulties in dealing with neuropsychiatric symptoms of the person with dementia, negative side effects occur frequently: 70% of family carers feel burdened and almost 20% feel overburdened (Peeters, Werkman, & Francke, 2012). High levels of strain, anxiety and depression are reported by dementia carers across countries in the last decades (Brodaty, Green, & Koschera, 2003; Cooper et al., 2012; Pot, Deeg, & van Dyck, 2000; Schulz, O’Brien, Bookwala, & Fleissner, 1995). Studies on support needs of family carers report the need for respite and daytime activities for the person with dementia they care for (Van der Heide, van den Buuse, & Francke, 2018; Van der Roest et al., 2009). Day care centres offer respite care, and several studies found beneficial effects on behavioural and psychological problems, subjective wellbeing and life satisfaction of people with dementia (Gaugler et al., 2003; Mossello et al., 2008; Zank & Schacke, 2002; Zarit et al., 2011). Tretteteig, Vatne, & Rokstad (2016) describe in their review of the literature that family carers experience day care centres, depending on their quality, as a respite and to some extent as a support service improving their competence in caring for the person with dementia. Zarit, Stephens, Townsend, & Greene (1998) also found lower stress and depression in family carers of people with dementia attending a day care centre compared to family carers of people who did not attend a day care centre. Nevertheless, day care utilisation is low. Reasons for non-utilisation include difficulties with accepting the diagnosis of dementia, lack of knowledge about respite facilities (Donath, Winkler, Graessel, & Luttenberger, 2011; Montoro-Rodriguez, Kosloski, & Montgomery, 2003; Peeters et al., 2012; Van der Roest et al., 2009) and worries about meeting new people and losing independence (Durand, James, Ravishankar, Bamrah, & Purandare, 2009). Most of the studied day care facilities offer single support to the person with dementia. But ‘combined interventions’, interventions targeted at supporting both the person with dementia and the family carer, appear to be more effective than single interventions (Olazaran et al., 2010; Smits et al., 2007; Van’t Leven, Prick, Groenewoud, Roelofs, de, & Pot, 2013). Examples are a Tailored Activity Programme (Gitlin et al., 2008), Community Occupational Therapy in Dementia (Graff et al., 2007) and the Integrative Reactivation and Rehabilitation Programme (Bakker et al., 2011), with effects found in the persons with dementia (e.g. on agitated behaviour, activities of daily life, depression and neuropsychiatric symptoms) and family carers (for example on sense of competence, burden and mastery).
An example of an effective combined intervention in the setting of a day care centre, widely provided in the Netherlands for more than 25 years, is the Meeting Centres Support Programme for community-dwelling people with dementia and their family carers (Dröes, Meiland, de Lange, Vernooij-Dassen, & Van Tilburg, 2009). These Meeting Centres are offered at easy-access locations such as community centres and aim to provide timely and attuned care that effectively supports community-dwelling people with dementia and their family carers in adapting to and coping with the consequences of dementia (Dröes, Breebaart, Meiland, van Tilburg, & Mellenbergh, 2004). Repeated multi-centre studies have shown that Meeting Centres are more (cost-) effective than traditional nursing home-based psychogeriatric day care centres that do not offer a carer support programme (from now: NH day care centres). After six months of participation, persons with dementia had less behaviour and mood problems and better self-esteem. Their carers felt less burdened and more competent to care for their relative. Furthermore, there were strong indications of delayed nursing home admission (Dröes, Meiland, Schmitz, & Van Tilburg, 2004, 2006). Also in an international multicentre study into the added value of the combined Meeting Centres Support programme compared to care as usual, positive effects were found on quality of life and mental health for people with dementia (Brooker et al., 2018) and decreased burden in carers (Evans et al., accepted 2018).
Despite the evidence on combined support programmes such as the Meeting Centres Support Programme, very few NH day care centres in the Netherlands adopted the combined Meeting Centres model. To stimulate further dissemination, an implementation study was started to gain insight into the conditions of successful transition of NH day care centres to community day care centres with carer support (from now on named: ‘CO day care’) and potential differences in outcomes and costs of the two types of psychogeriatric day care. Six NH day care centres made the transition to CO day care centres. This transition meant, among other things, moving to an easy-access building in the community, offering day care in an open setting, based on the principles of the adaptation-coping model (this means assisting participants to deal with the practical, emotional and social consequences of dementia), starting a support programme for carers who can freely make use of it if they have a need, training staff and integrating psychomotor therapy and other therapeutic activities in the daily routine of the CO day care centre. We reported on the conditions for successful transition to CO day care in a previous paper (van Haeften-van Dijk, Meiland, Van Mierlo, & Dröes, 2015). We also explored the effects of newly developed and longer existing CO day care versus NH day care on people with dementia and found indications that after six months in new CO day care centres, people with dementia had less neuropsychiatric symptoms, and in longer existing CO day care centres, they had less care needs compared to participants of NH day care (van Haeften-van Dijk, Meiland, Hattink, Bakker, & Dröes, 2016). Moreover, participants and carers of CO day care were more satisfied with the day care atmosphere, location, contact with staff, the activities at the centre and the received support compared to participants of NH day care and their carers (van Haeften-van Dijk, Hattink, Meiland, Bakker, & Dröes, 2017). The aim of the present study was to investigate if implementing the Meeting Centres Support Programme in traditional nursing home-based day care has added value for carers as well. Therefore, we compared the needs, feelings of competence and experienced burden of carers after using the CO day cares or the traditional NH day care centres for a period of six months.
Method
Study design
For this explorative evaluation, which was part of an implementation study, a pretest–posttest control group design with non-equivalent groups and three measurements (at zero, three and six months) was used. The experimental group consisted of family carers as part of a dyad with people with dementia, who received support from a CO day care. The control group consisted of family carers as part of a dyad with persons with dementia who received support in traditional NH day care. The study was registered in the Netherlands Trial Register under Trial NL2773 (NTR2913).
Setting and participants
To enable detection of medium size effect (d = 0.5) in carers with a power of 0.80, alpha 0.05, and taking into account an expected drop-out rate of 15%, it was calculated that a total of 150 carers (75 experimental and 75 controls) was needed (Cohen, 1988). All NH psychogeriatric day cares in the province North Holland of the Netherlands were invited for an informative meeting about the implementation study, and six NH day care centres (control group), who were willing to take part in the implementation study, were included and made the transition to (new) CO day care (experimental group). The control group was recruited in the NH day cares in the period before the transition to CO day care. After transitioning, only new participants of the CO day care were recruited for the experimental group. In order to increase power of the study, five longer existing CO day care centres were also recruited for the experimental group in the south-east of the Netherlands. Five NH day care centres from the same region served as control group. Thus, a total of 11 CO day care centres and 11 NH day care centres participated in the study. The total number of included persons per day care centre varied from 1 to 23. New participants (family carers as part of a dyad with a person with dementia) of CO day care (experimental group) and NH day care (control group) were invited to take part in the research via an informed consent procedure (see Procedure). The only inclusion criterion for family carers was that they took care of a person with a diagnosis of some type of dementia visiting CO day care of NH day care.
The interventions in experimental and control group
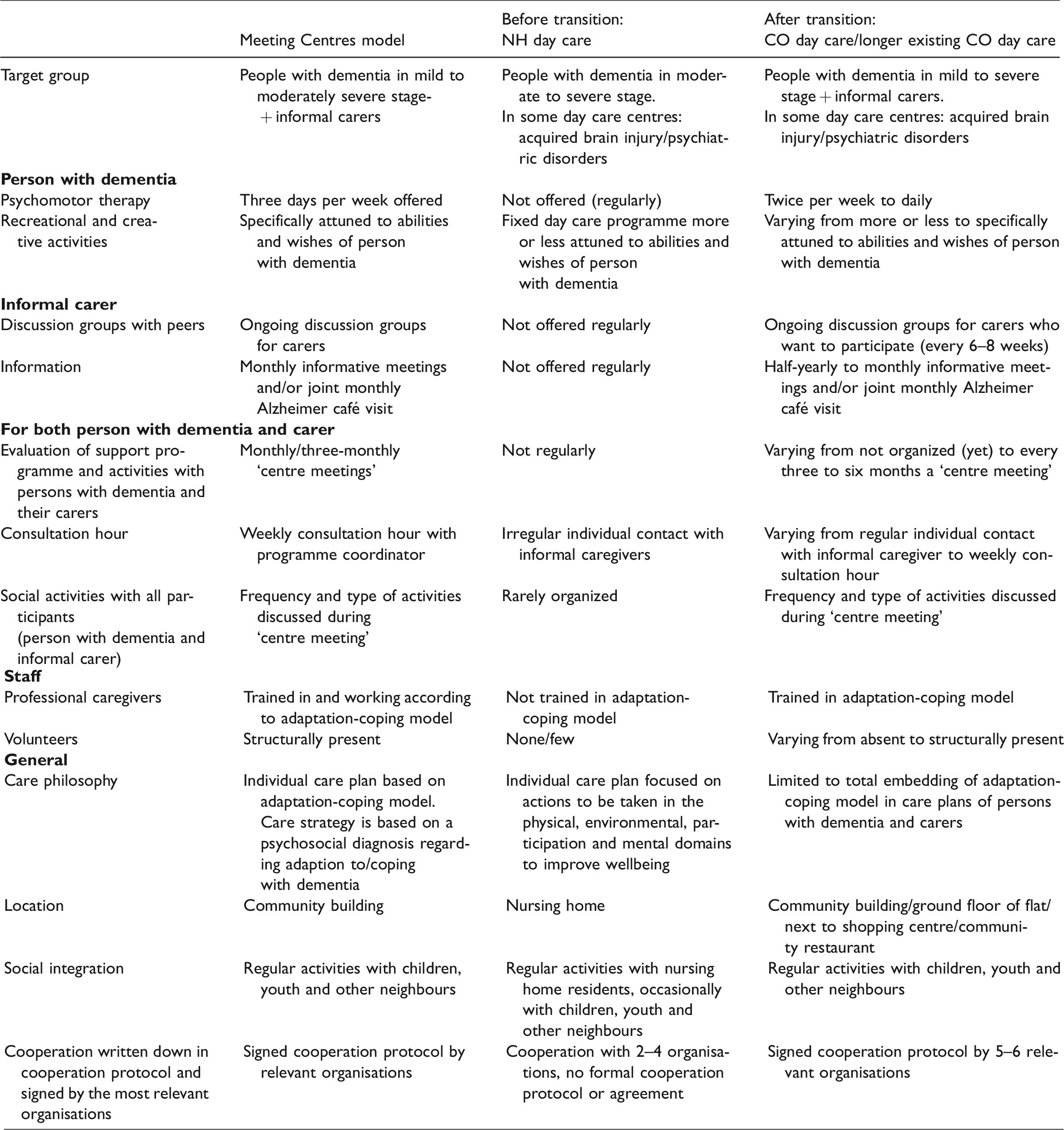
The support programme of CO day care is based on the combined Meeting Centres Support Programme for people with dementia and their carers. The target group of CO day care consists of community-dwelling people with mild to severe dementia and their carers. Care and support are offered in a community-based, socially integrated, easy access location. During various days a week, the persons with dementia can participate in a personalized activity programme (including recreational and creative activities, music, reminiscence and psychomotor therapy). The carers are free to join the informative meetings about dementia-related topics (for example the diagnosis, dealing with behaviour changes and available professional care and support in the neighbourhood) and the ongoing discussion groups with peers if they feel the need for it. The day care for the person with dementia serves as respite care for the carers. In addition, both the persons with dementia and the carers can utilize a consulting hour, receive case management, participate in social activities and outings and in centre meetings where all parties involved (patients, family carers, volunteers and professionals) can exchange experiences and express their wishes concerning the support programme. The care and support in the CO day care centres are offered by a small fixed team consisting of a programme coordinator, activity therapists, care assistants and volunteers who are supervised and assisted by a psychologist or elderly care medicine specialist from the care organisation that the day care is linked to. The centres organize the support programme in cooperation with local care and welfare service providers in order to reduce fragmentation and improve integration of care. In the six CO day care centres that made the transition from NH day care during this study, it took some time before the full combined support programme was offered: the activity programme for persons with dementia (which also provides respite to family carers) started immediately, whereas support for the family carers started within one month after opening in three of the new CO day care centres, and after seven months in the other three centres. After the transition, there was more emphasis on cooperation between staff and family carers, which was reflected by more frequent contact by telephone and/or during centre meetings and discussion groups (van Haeften-van Dijk et al., 2015).
The traditional NH day care centres are located in specialized units of the nursing home. The target group consists of community-dwelling people with mild to severe dementia. They offer social activities and psychosocial interventions such as reminiscence and activity therapy for the persons with dementia. Treatment is offered by multidisciplinary teams consisting of the social, psychological, paramedical and medical discipline. Compared to the CO day care, the support programme for family carers is much less intensive and structured: often there are only incidental contacts with family carers and one or two informative family meetings a year. Few NH day care centres offer discussion groups with peer carers. For a full overview of the differences between the Meeting Centres and NH day care, please refer to Table 1.
Description of Meeting Centres model, community day care with carer support (CO day care, experimental group) versus nursing home-based day care (NH day care, control group).
Measuring instruments
Background characteristics
Socio-demographic characteristics of persons with dementia and family carers were collected at the first interview with the family carer. Information on the diagnosis was collected via the coordinator of the day care centres or the general practitioner. The severity of cognitive impairments of the person with dementia was assessed with the Mini Mental State Examination (MMSE; range 0–30; Folstein, Folstein, & McHugh, 1975); the number of behaviour and mood problems with the Neuropsychiatric Inventory questionnaire (NPI-Q; range 0–12; Cummings et al., 1994; de Jonghe, Kat, Kalisvaart, & Boelaarts, 2003).
Carers’ use of the support programme of CO day care
Family carers’ use of and subjective experiences with the support programme were assessed by means of a survey, sent after six months participation. This survey was developed by Dröes, Breebaart, Ettema, van Tilburg, & Mellenbergh (2000) in interaction with the first users (people with dementia and family carers) of the Meeting Centres Support Programme. Also in later studies, this survey was used for the evaluation of the Meeting Centres Support Programme (Dröes, Meiland, Schmitz, & Van Tilburg, 2011).
For the analyses in this study, we only used carers’ answers to questions about their involvement in the day care and/or carer programme (e.g. ‘Did you take part in the discussion group with peers?’ (yes/no, and if yes: how often) and overall satisfaction, measured with the question to give a general evaluation of the support programme on a scale between 1 (very bad) and 10 (very good).
Primary outcomes
The primary family carer outcomes were support needs and sense of competence. Support needs of the carer were measured by two items of the Camberwell Assessment of Need for the Elderly (CANE; Reynolds et al., 2000). Besides care needs of the elderly, this instrument comprises two needs sections for the carer, one with regard to information and one on psychological distress (test–retest reliability of kappa = 0.40 and kappa = 0.70, respectively; Van der Roest, Meiland, van Hout, Jonker, & Dröes, 2008). The sense of competence of family carers was measured with the Short Sense of Competence questionnaire (SSCQ; kappa = 0.76, range 0–7; Vernooij-Dassen et al., 1999). The SSCQ is a seven-item questionnaire that assesses the degree to which family carers feel capable of caring for a person with dementia on a five-point scale (that is dichotomized for the analyses, according to the instructions of the authors; Vernooij-Dassen et al., 1999).
Secondary outcomes
The secondary outcomes were the emotional burden felt by the carer in relation to neuropsychiatric symptoms of the person with dementia, care-related quality of life, objective burden, subjective burden and nursing home admission of the person with dementia.
Burden caused by neuropsychiatric symptoms in people with dementia was assessed using the emotional burden subscale of the NPI-Q (α = 0.88; range 0–36; Cummings et al., 1994; de Jonghe et al., 2003). For each of the 12 neuropsychiatric symptoms of the NPI-Q, carers were asked to indicate on a six-point scale how emotionally distressing the symptom was for them (from ‘not emotionally distressing’ to ‘extremely distressing’).
The CarerQoL-7d (Brouwer, van Exel, van Gorp, & Redekop, 2006) was used to measure care-related quality of life. The CarerQoL-7d measures subjective burden of caring on seven dimensions. A weighted sum score is calculated from these items with a range from 0 (negative caring situation) to 100 (positive caring situation; Hoefman, van Exel, Rose, van de Wetering, & Brouwer, 2014).
Objective burden was measured by asking carers how many hours per week they assisted the person with dementia in personal care, household, administrative support and going with them to doctor’s appointments. Subjective burden was assessed by asking ‘how burdensome is caring for your partner/mother/father/etc?’ on a range from 0 (not burdensome) to 10 (very burdensome).
Nursing home admission of the person with dementia was recorded, and the percentage of participants being admitted to a nursing home after six months was calculated.
Procedure
The study was approved by the medical ethics committee of VU University Medical Centre. At the start of participation in one of the day care programmes, the staff of the day care centre provided oral and written information on the study to the person with dementia and the carer and invited them to participate in the study. When the carer and the person with dementia indicated their interest in participating in the study, the researcher received contact details of the dyad and contacted them to explain the research in more detail. If they agreed to take part, both were invited to sign an informed consent form. All but one of the interviewers (n = 20) were students (BSc or MSc) with experience in interviewing, either through their education or through (voluntary) work. All interviewers received half a day of training in how to administer the measuring instruments in this study and were supervised by the researcher. After six months, carers received a questionnaire by mail about their use of and satisfaction with the support programme offered in the CO or NH day care centre.
Data analysis
The data were analysed using SPSS 20.0. In case of missing values at baseline, caused by people not (yet) willing to participate when starting in the day care, or being referred too late to the researchers (after the first month of participation), the three-month measurement data were imputed for the baseline. These participants were also considered ‘completers’. This procedure was based on results of previous studies of Dröes et al. (2000, 2004) that showed no statistically significant differences in outcomes between Meeting Centres and NH day care within three months of participation. We therefore based our effect analysis on the data collected at baseline and after six months of participation.
Descriptive analyses were performed on data of all participants and subgroups, including non-responders at the start of the study, and drop-outs during the study in order to study selection bias or attrition bias. To test for differences between these groups, we used chi-square (χ2) tests for nominal variables and Kruskal–Wallis and Mann–Whitney U tests for ordinal and interval variables. Characteristics on which the groups differed at baseline and which were related to the outcome measures were included in the analyses as a potential confounder. Subsequently, we identified potential effect modifiers by assessing from literature which characteristics are expected to be related to our outcome measures. We examined in SPSS if these characteristics of the person with dementia or the carer (e.g. severity of behaviour and mood problems of the person with dementia (Neuropsychiatric Inventory Questionnaire (NPI-Q)) and carers’ subjective health and sense of competence at baseline (SSCQ) were indeed related to our outcome measures by including interaction terms in the univariate covariance analyses (ANCOVA). If the interaction term was significant on a p < 0.05 level, we treated the characteristic as effect modifier in the data analysis and presented the results separately for the different groups (e.g. low versus high sense of competence at baseline).
ANCOVA’s were carried out to compare outcome measures at T2 (after six months) in the experimental and control group, while the baseline data (T0) and potential confounding variables were included in the analysis as covariates. This strategy is recommended in small samples (Cole, 1988). We used two-tailed tests with a significance level of 5% and the Bonferroni correction to counteract the problem of multiple comparisons. To calculate the effect sizes of the outcomes, we used Cohen’s d (for ANCOVAs) and Cramer’s V (for chi-square (χ2) tests). Cohen’s d was interpreted as small (0.20), medium (0.5) or large (≥0.80). Cramer’s V was interpreted as small (0.10), medium (0.30) or large (≥0.50). We used chi-square (χ2) tests to examine statistical differences in nursing home admission between the groups. Correlations between nursing home admission and severity of dementia (dichotomized) and behaviour and mood problems (NPI-Q) at baseline were examined using Spearman’s rank correlations.
Results
Study participants and drop-outs
Figure 1 displays a flowchart of the recruitment of study participants (n = 131). The experimental group (new or longer existing CO day care) consisted of 67 carers, and the control group (NH day care) consisted of 64 carers.

Flow chart of the study.
The number and reasons for non-response and drop-out at the different time points of the study are included, resulting in 37 completers in the experimental group (22 in experimental group 1 (E1) plus 15 in experimental group 2 (E2)) and 35 completers in the control group. Table 2 shows baseline characteristics of all respondents (including drop-outs) in the experimental group and control group, and the baseline characteristics of the completers. The experimental group consists of the respondents in E1 (new CO day care) and the respondents of E2 (longer existing day care). Respondents in groups E1 and E2 did not differ in background characteristics.
Socio-demographic characteristics of the study participants (informal carers of people with dementia).
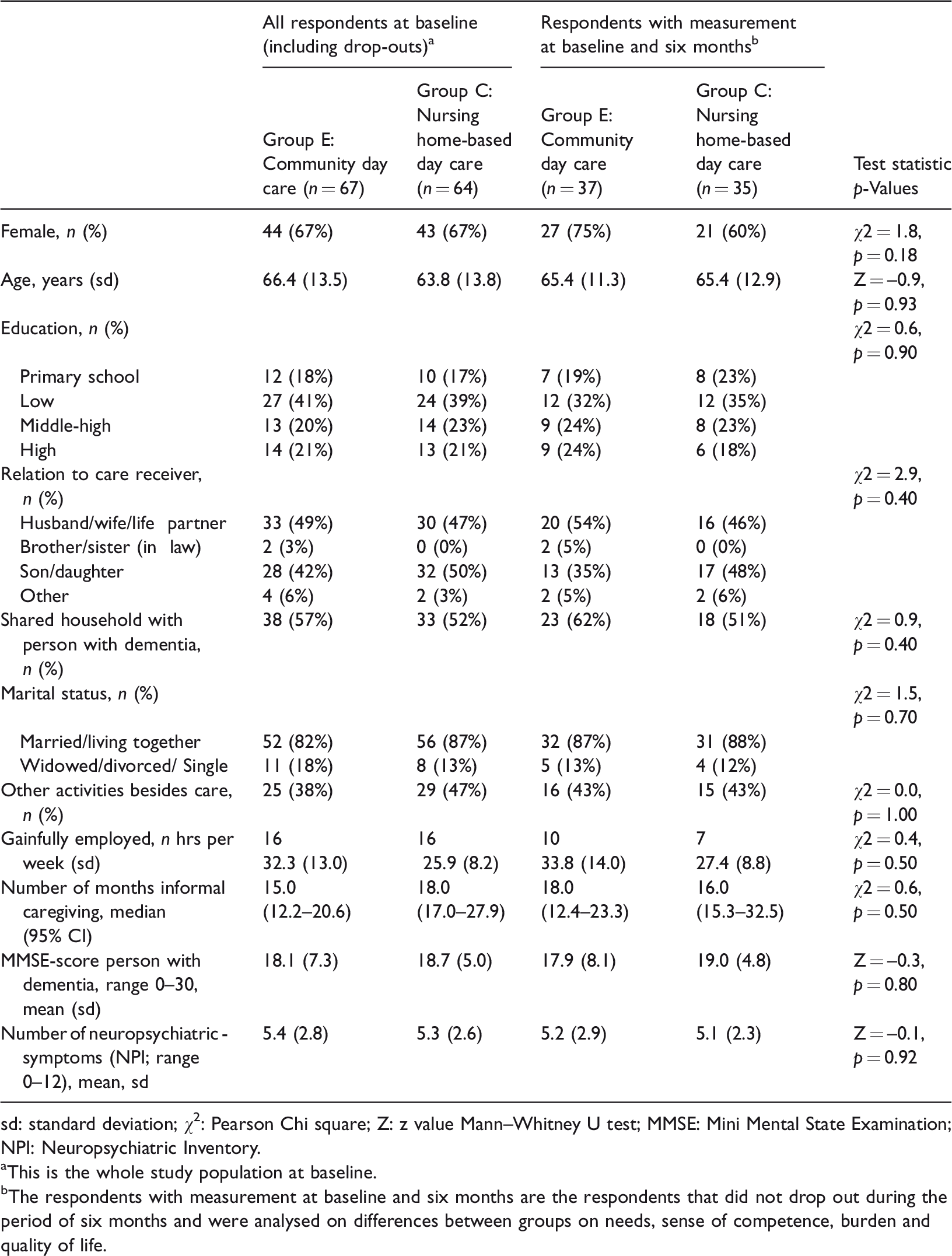
sd: standard deviation; χ2: Pearson Chi square; Z: z value Mann–Whitney U test; MMSE: Mini Mental State Examination; NPI: Neuropsychiatric Inventory.
aThis is the whole study population at baseline.
bThe respondents with measurement at baseline and six months are the respondents that did not drop out during the period of six months and were analysed on differences between groups on needs, sense of competence, burden and quality of life.
We examined if drop-outs in the experimental (n = 28, 21%) and control groups (n = 29, 22%) differed significantly from the completers (n = 72) on background characteristics and outcome measures. We did not find any significant differences.
For 22 persons, the baseline measurements (T0) were missing because informed consent for the study was received too late, that is more than one month after the start of participating in day care. As described in the Methods, we decided to impute the three-month measurement data for the baseline in this group.
We also examined differences between study participants and people not willing to participate on gender of the carer, his/her relation to the person with dementia, marital status or living situation (cohabiting with the person with dementia or not) and did not find significant differences.
Carers’ use of and satisfaction with the support programme of CO and NH day care
After six months of participation in the CO day care, 18 of the 37 carers (49%) of the experimental group returned the questionnaire about their participation in the support programme for carers. Of these carers, 67% (n = 12) indicated they participated in one or more components of the support programme for carers, e.g. the peer support groups, informative meetings, the consultation hour and/or the centre meeting. Non-participation of carers in the support services was accepted because the carers in CO day care – apart from the respite care – are free to join any of the support activities (unlike the Meeting Centres where carers are expected to utilize the carer support programme). Overall satisfaction with the support programme in both CO day care (mean = 8.1, sd = 0.9) and NH day care (n = 25, response = 71%, mean = 7.9, sd = 0.9) was high and did not differ between groups (F = 0.2, p = 0.66).
Results on outcome measures
Table 3 shows the results of the ANCOVAs on the outcome measures of the experimental and control group after six months. No significant differences were found between the groups on sense of competence (SSCQ) or need for information (CANE). Regarding psychological distress (CANE), we found an increase in expressed needs for support in the CO day care: participants in the CO day care group after six months reported more often having unmet needs and less often having no need for support compared to the control group (χ2 = 7.7, df = 2, p = 0.02, V = 0.3). Further explorative analyses showed that this occurs mainly in the newly developed CO day care centres (χ2 = 9.9, df = 2, p = 0.01, V = 0.4). On the secondary outcomes, care-related quality of life, objective burden and subjective burden, no significant differences were found between the groups.
Results (unclassified and classified) of the ANCOVA analyses on outcome measures in family carers between baseline measurement and after six months of participation in CO day care centres (Group E) and NH day cares centres (Group C).

aUnadjusted mean scores at baseline and at six months
bMean scores at six months are adjusted for baseline scores.
cUnderlined score is the most favourable.
mE: mean score experimental group; mC: mean score control group; sd: standard deviation; se: standard error; d: Cohen’s d effect size (small = 0.20, medium = 0.50 and large≥ 0.80), χ2: Pearson chi square; SSCQ low: score between 0 and 4; SSCQ high: score between 5 and 7; ANCOVA: univariate covariance analyses; CANE: Camberwell Assessment of Need for the Elderly; SSCQ: Short Sense of Competence questionnaire; NPI-Q: Neuropsychiatric Inventory questionnaire.
For the outcome emotional burden (NPI) ‘sense of competence’ was an effect modifier. We therefore classified carers with a low (score 0–4, n = 26) and high (score 5–7, n = 43) sense of competence. The carers with a low sense of competence at baseline who participated in the experimental group reported lower emotional burden than carers in the control group (F = 7.4; p = 0.01; d = –1.1).
We further explored if potential effects differed for carers of persons with dementia who participated in the newly developed or the longer existing CO day care centres compared to the control group. However, we did not find significant differences in outcome measures between these groups (data not shown).
Next, we investigated if the changes over six months in need for support regarding psychological distress (CANE) were associated with the emotional burden of carers due to behavioural and psychological symptoms of the person with dementia (NPI). No correlation was found in the total group (r = –0.06, p = 0.68), or in the group of carers with a low baseline sense of competence (SSCQ-score; r = –0.09, p = 0.72), indicating that these measures are not interrelated. We also investigated the possible correlations between carers’ use of and satisfaction with the support programme and changes in support needs regarding psychological distress (CANE; r = 0.25, p = 0.41 and r = –0.06, p = 0.76) and emotional burden (NPI; r = 0.23, p = 0.36 and r = 0.03, p = 0.82), respectively, but no significant correlations were found.
Nursing home admission
After six months of participation, 14.9% (n = 10) of the persons with dementia in the experimental group and 10.9% (n = 7) of the persons with dementia in the control group were admitted to a nursing home. This difference was not statistically significant (χ2 = 0.19, p = 0.66). When making a distinction between the new CO day care centres (E1) and the longer existing ones (E2) on the one hand, and the NH day care centres (C) on the other, the lowest nursing home admission rate (7.7%) was observed in group E2. In group E1, 20.5% had been admitted to a nursing home after six months. However, the differences in admission rates between the two experimental groups and the control group were not statistically significant. We investigated if nursing home admission was correlated to severity of dementia (MMSE; r = 0.00, p = 0.99) and behaviour and mood problems of the person with dementia (NPI-Q; r = 0.07, p = 0.44), or sense of competence of the carer at baseline (SSCQ; r = 0.02, p = 0.86), but found no significant correlations.
Discussion
This study evaluated the effects of CO day care, set up according to the principles of the proven effective Meeting Centres Support Programme model for people with mild to moderately severe dementia and their carers, compared to traditional NH day care on family carer outcomes. Regarding the primary outcome measures (needs and sense of competence), we found that carers in CO day care reported more needs related to psychological distress after six months compared to carers in the NH day care group (medium effect). No differences were found between groups on sense of competence of carers after six months. With regard to the secondary outcome measures (emotional burden, care-related quality of life, objective burden, subjective burden and nursing home admission of the person with dementia), we did not find statistically significant differences between groups. Further explorative analyses pointed out that in carers of the CO day care group who had a low sense of competence at the start of participation in day care, the emotional burden due to behavioural and psychological symptoms of the person with dementia they cared for decreased over six months, whereas it increased among carers in NH day care (large effect). The carers’ need regarding support for psychological distress proved not to be related to this emotional burden, indicating that these are different concepts.
Although the CO day care aims to meet family carers’ needs by providing them support, in this study, CO day care resulted in the expression of more need for support related to psychological distress in the CO day care centres compared with the NH day cares. At the same time, no differences were found between objective burden and subjective burden between the two carer groups. Further exploration indicated that more needs regarding psychological distress were especially found among carers in the newly developed CO day care centres. In these newly developed CO day care centres, the staff of the day care was more aware of the importance to involve family carers and had probably more attention to the carers’ subjective experiences. This may have resulted in carers becoming more aware of their distress, while not receiving sufficient support to meet their needs because the carer support programme was not yet fully operational in every CO day care from the very beginning of the study. Increased awareness in carers about their own support needs can be seen as a first step to seek help, and therefore should not be judged per se as a negative effect. Moniz-Cook, Gibson, Harrison, & Wilkinson (2009) also found negative effects of early combined psychosocial interventions in memory clinics at short-term follow-up (six months), but after 12–18 months, participants in the interventions appeared to have benefitted from the interventions (reduced depression and anxiety in carers; Moniz-Cook et al., 2009). Furthermore, a review of Cooke, McNally, Mulligan, Harrison, & Newman (2001) also showed delayed improvements on carer outcomes, suggesting a delayed impact of psychosocial interventions (Cooke et al., 2001). These studies underline the importance of the long-term evaluation of family carer support to gain information on effective support strategies, although other studies did find short-term effects of combined community day care on stress, burden and depression of family carers (Gaugler et al., 2003; Mossello et al., 2008; Zarit et al., 2011).
Our finding, that a subgroup of family carers with a low sense of competence at the start of participation in day care, in particular, benefited from the combined CO day care by experiencing a decline in emotional burden after six months, is in line with a recent review in which several negative caregiver characteristics were found to be related to positive outcomes of psychosocial interventions for carers, such as loneliness, perceived stress and negative beliefs about the caregiver role (Van Mierlo, Meiland, Van der Roest, & Dröes, 2012).
A limitation of our study is the high drop-out rate, which resulted in less statistical power to find potential effects of CO day care compared to NH day care over six months. In all groups, the main reasons for drop-out were nursing home admission or quitting day care. Another limitation is the fact that we imputed three-month measurement data at baseline because of several study participants the baseline measurements were lacking. This resulted in a follow-up period varying between three and six months, which could have influenced the results, most probably an underestimation of the effects.
Another limitation is that we had little information on whether, and how, the support programme was used by carers in the CO day care. Because a characteristic of the CO day cares is that the carers are free to choose if and which support they want to use. We aimed to inventory their actual participation in the different carer support activities by means of the carer survey. Unfortunately, only half of the carers returned this questionnaire. The lack of information on frequency and intensity of support programme utilisation made it difficult to investigate whether the actual received different types of support influenced the effects found in our study. Explorative analyses on our data did not indicate a relationship between the use of the carer support programme and the outcomes on which we found effects.
The study into the added value of the CO day care centres compared to NH day care was performed as part of an implementation study. This implied that the new CO day care centres involved had just made the transition from their traditional NH day care. As a result, especially during the first part of the data collection period, these new day care centres had not yet fully implemented the support programme for the carers, making it less plausible, we would find benefits compared to NH day care as found in earlier studies on the Meetings Centres Support Programme (Dröes et al., 2000, 2004). The majority of centres involved in these effect studies were already fully operational. We tried to counteract this problem by also recruiting carers of people with dementia who participated in several longer existing CO day care centres, but unfortunately, we were able to recruit only a small number of participants from these centres. Moreover, we did not measure ‘a degree of implementation’ of CO day care, so we could not correct for this in the analyses.
Taking into account the mentioned limitations, this study should be considered as a first exploration of the added value of CO day care with carer support compared to NH day care. The added value of CO day care for people with dementia was shown in a previous study: people with dementia had less neuropsychiatric symptoms in new CO day care centres and less care needs in longer existing CO day care centres (van Haeften-van Dijk et al., 2016). Because combined support for people with dementia and their carers has been proven more effective than single interventions, the transition of nursing home-based day care without carer support to community day care with carer support has the potential to more effectively support people with dementia to live in their own home as long as possible (Brodaty et al., 2003; Dröes et al., 2004; Olazaran et al., 2010). Worldwide, there are many different forms of day cares available, and their impact on family carers depends among other things on how the day cares meet the needs of carers (Tretteteig et al., 2016). An advantage of the CO day cares is that they offer a flexible carer support programme. The World Health Organisation also stresses the importance of a variety of support facilities, such as respite care and family carer support groups (World Health Organization, 2012). Because CO day cares are offered in more easily accessible locations than traditional NH day care, barriers to using this type of support may be overcome (van Exel, Moree, Koopmanschap, Goedheijt, & Brouwer, 2006). However, professionals need to be become aware of the effectiveness of these facilities and refer clients to them in a timely manner (van Haeften-van Dijk et al., 2015). To date, the use of CO- and NH-based day care treatment (besides other forms of day care) is still very low in the Netherlands: only 5% of people with dementia utilize it (Dutch Alzheimer Association, 2014). Other studies also found a low use of day care services among community-dwelling people with dementia, varying from 9–18% (Beeber, Thorpe, & Clipp, 2008; Seematter-Bagnoud, Martin, & Bula, 2012; Weber, Pirraglia, & Kunik, 2011).
Conclusion
This exploratory study on the added value of CO day care compared to NH day care for carers of people with dementia showed that overall family carers using CO day care more often expressed a need for support related to psychological distress. For a subgroup of carers in CO day care, we found a decrease in emotional burden. On the other carer outcomes, no differences between CO and NH day care were found. A larger controlled follow-up study is recommended to understand the long-term effects of CO day care over NH day care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VitaValley / Noaber Foundation, ZonMw, Dutch National Elderly Care Programme (Grant ID: 314080401), Foundation Sint Jacob.