
Abstract
Background and objectives
Family caregivers of people with dementia experience high burden making medical decisions for their loved ones. Undertaking Advance Care Planning (ACP) can help reduce burden and stress. Having experiences making medical decisions for someone else may influence the way people make decisions for themselves. Therefore the aim of this study was to assess the willingness of family caregivers of people with dementia to undertake ACP for themselves, using the Theory of Planned Behavior.
Research design and methods
Face-to-face interviews were conducted with 195 family caregivers of people with dementia. A structured questionnaire was used to assessed participants’ attitudes, subjective norms, perceived control, anticipated regret, the wish to prolong life and caregiver burden. Hierarchical regression analysis was performed to test the contribution of the variables to the willingness to undertake ACP.
Results
Overall, participants expressed moderate willingness to undertake ACP. Among the various options for undertaking ACP, the highest willingness expressed was to appoint a durable power of attorney and the lowest willingness was to have informal conversations with their doctor. The hierarchical regression revealed that attitudes, subjective norms and anticipated regrets were main determinants of the willingness to undertake ACP.
Discussion and implications
Interventions should be developed to encourage family members to undertake ACP for themselves, which emphasize the advantages of the process and involve significant others in the formal and informal aspects of ACP.
Introduction
Family caregivers
Family caregivers—spouses and adult children—provide informal and unpaid care for their relatives with dementia (Llanque et al., 2016). Caregiving tasks include helping with activities of daily living, such as bathing, and with instrumental activities of daily living, such as shopping and making medical appointments (Pearce et al., 2012). While caregiving might be associated with some positive effects such as self-efficacy and spirituality (Stansfeld et al., 2017), most caregivers experience significant physical, psychological, social and financial burden (Llanque et al., 2016; McCabe et al., 2016). One of the most difficult duties for family members of persons with dementia consists in making fateful medical decisions for the person with dementia mainly in moderate and advanced stages of the disease, when the person loses capacity to make decisions for himself or herself and near end-of-life (Ashton et al., 2014; Whitlatch & Orsulic-Jeras, 2018). Knowing a person’s preferences for end-of-life treatment may help reduce burden and mitigate some of the negative feelings associated with making medical decisions (Poppe et al., 2013). One way of communicating wishes for end-of-life treatments is undertaking Advance Care Planning (ACP).
Advance Care Planning
ACP is a process that helps adults understand and share their personal values and preferences for future medical care during serious and chronic illness (Sudore et al., 2017). A key purpose of ACP is to preserve the person’s autonomy and self-determination at end-of-life (Detering et al., 2010; Seymour et al., 2010). ACP includes formal aspects of signing Advance Directives (ADs) or appointing a Durable Power of Attorney (DPOA), as well as informal aspects of having conversations with family members or professionals (Institute of Medicine, 2015). The laws concerning ACP, medical and surrogate decision making differ among countries (Greco et al., 1991; Ingravallo & De Panfilis, 2019; Van Wijmen et al., 2010). In Israel, “The Dying Patient Act” was passed in 2005 in order to provide options for autonomous decision-making when a person is unable to make medical decisions (Bentur & Sternberg, 2017; Steinberg & Sprung, 2006).
Undertaking ACP has several advantages for the person with dementia as well as for their family caregivers. For the persons with dementia, it allows the person’s wishes and values at end-of-life to be respected, thus ensuring higher quality of care that is consistent with their preferences and avoiding unwanted medical treatment at end-of-life (Brinkman-Stoppelenburg et al., 2014; Dixon et al., 2018). For family caregivers, knowing their loved one’s wishes can reduce the stress, anxiety, and depression caused by taking crucial medical decisions for somebody else (Brazil et al., 2018).
Recent literature has examined the perceptions of family caregivers of people with dementia toward end-of-life care and ACP (Bolt et al., 2019; Durepos et al., 2019; Sellars et al., 2019). These studies showed that family caregivers experience end-of-life as a complex process and need support to make medical decisions regarding end-of-life care. Despite the importance of these studies, to the best of our knowledge no study has assessed yet how caregiving experiences affect family caregivers’ decisions and preferences regarding end-of-life care in general and willingness to undertake ACP for themselves in particular.
Therefore, the main purpose of the present study was to assess the willingness of family caregivers of people with dementia to undertake ACP for themselves using the Theory of Planned Behavior (TPB) as a theoretical framework.
The Theory of Planned Behavior
The TPB main assumption is that a person’s behavior is rational and based on information available to make a decision or perform a behavior. The central concept of the TPB is “behavioral intention”, which is the person’s motivation to engage in a specific behavior (Ajzen, 1988). The three determinants of behavioral intention are: attitudes, subjective norms, and perceived behavioral control. (i) Attitude toward a behavior is the degree to which performance of the behavior is positively or negatively valued. (ii) Subjective norms refer to the person’s subjective judgment regarding significant other’s support to perform or not perform a behavior. (iii) Perceived behavioral control is the person’s perception of his/her ability to perform a behavior (Ajzen, 2019; Werner, 2004).
In addition to the main variables in the original TPB model, and in accordance with the suggestion of including additional variables to increase the prediction value of the model (Conner & Sparks, 2005; Werner, 2004), we added Anticipated regret (AR) as an additional determinant of the intention to complete ACP. AR relates to the consequences of (not) performing a behavior, and was found to have an important effect on behavioral intention (Ajzen & Sheikh, 2013; Sandberg & Conner, 2008). Moreover, two other variables were included because of their relevance to the topic under study: The wish to prolong life, which is defined as the cognitive expression of an individual’s desire and commitment to staying alive (Carmel, 2001) and caregiver burden which is defined as a multi-dimensional response to the negative appraisal and perceived stress resulting from taking care of an ill individual (Kim et al., 2012).
Methods
Participants
A total of 210 dementia family caregivers of people with dementia were contacted, and 195 participated in the study (response rate of 93%). The main refusal reasons were the reluctance of caregivers to share personal experiences and lack of time. Inclusion criteria were being a spouse or an adult child of a person with dementia, and Hebrew speaker. Exclusion criteria included being cognitively impaired.
Most of the caregivers were females (N = 155, 79.5%) born in Israel (N = 140, 71.8%), married (N = 158, 81.0%), secular (N = 132, 67.7%), adult children caring for a parent (N = 120, 61.5%), with a mean age of 65.5 years old (SD = 11.6, range 30–92) and a mean of 15.2 years of education (SD = 2.9, range 1–20). Most of the participants lived separately from the person with dementia (N = 111, 56.9%), were caring for the person with dementia for a mean of approximately 4.8 years (SD = 3.3, range 1–20), and provided on average 38 weekly hours (SD = 43.1, range 1–168), meaning that the care provided by family caregivers was extremely wide-ranging. Regarding the care-receivers, most of them were female (N = 100, 51.3%), with a mean age of 84.0 years old (SD = 8.3, range 61–101), living with dementia for a mean of five years (SD = 3.3, range 1–20).
Measures
Willingness to undertake ACP: Six items were used to assess participants’ willingness to formally and informally undertake ACP (see Table 1). For example: “I intend to sign Advance Directives”. The items were rated using a seven-point Likert-type scale ranging from 1 = not willing at all to 7 = very much willing. An overall index was calculated by averaging the items, with higher scores indicating higher willingness to undertake ACP. The internal reliability of the index was high (Cronbach α = .83).
Willingness to undertake ACP (N = 195).
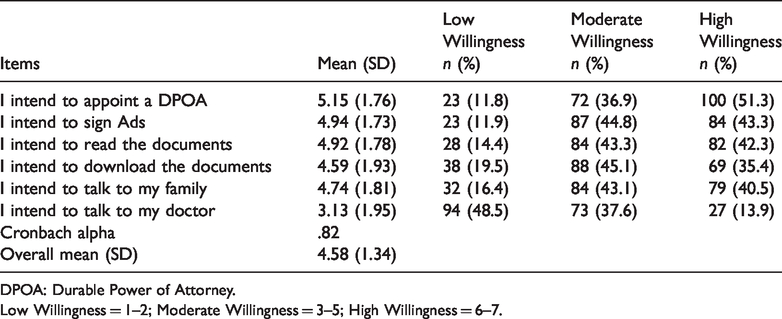
DPOA: Durable Power of Attorney.
Low Willingness = 1–2; Moderate Willingness = 3–5; High Willingness = 6–7.
Attitudes towards undertaking ACP: Were assessed using 11 items, developed on the basis of an elicitation study conducted prior to data collection (Kermel Schiffman & Werner, 2020). An example item: “Signing Advance Directives or a Durable Power of Attorney may enable me to take responsibility for my life”. All items were rated on a seven-point Likert-type scale, ranging from 1 = not at all to 7 = very much. An overall index was calculated by averaging the items, with higher scores indicating more positive attitude. The internal reliability of the index was good (Cronbach α = .75). As the index was negatively skewed (skew = −1.34, SE = .17), it was exponentially transformed for performing the analyses.
Subjective norms towards undertaking ACP: Based on the elicitation study, these were assessed by two items: (i) “Most of my family members whose opinions I value, support me to undertake ACP”, and (ii) “My family members’ opinions are important to me”. The items were rated on a seven-point Likert-type scale from 1 = not important at all to 7 = very much important. An overall index was calculated by averaging the items, with higher scores indicating more positive norm. Both items were significantly correlated, reflecting good internal consistency (rs = .14, p < .05).
Perceived control toward undertaking ACP: Based on the elicitation study this was assessed using three items rated on a seven-point Likert-type scale ranging from 1 = strongly disagree to 7 = strongly agree. An example item: “If the forms will be easy to complete, it will encourage me to undertake ACP”. Due to a non-normal distribution of the items, they were converted dichotomized, with scores of 1–4 defined as 0 = meaning not important, and scores of 5–7 defined as 1 = meaning important. An overall index was built by summing the three items, with higher scores reflecting higher perceived control to undertake ACP.
Anticipated regrets: Was assessed using three items examining regret to undertake ACP. An example item: “If I will not undertake ADs or appoint a DPOA I may regret in the future”. The items were rated on a seven point Likert-type scale ranging from 1 = strongly disagree to 7 = strongly agree. An overall index was calculated by averaging the items with higher score indicating higher ARs. The internal consistency of the index was good (Cronbach α = .70).
The wish to prolong life: Was assessed using five items developed by Carmel (2001) and examining the wish of participants to prolong life. An example item: “I would accept any medical treatment in order to prolong my life”. The items were rated on a five-point Likert-type scale ranging from 1 = completely disagree to 5 = completely agree. An overall index was calculated by averaging the five items, with higher scores indicating higher wish to prolong life. The internal reliability of the scale in this study was high (Cronbach α = .84).
Caregiver burden: Was assessed using the Zarit Burden Interview Short Form (ZBI-SF), a shortened 12-item version of the original 22-item ZBI (Zarit et al., 1985). The questionnaire was available in Hebrew (Bachner & Ayalon, 2010). An overall index was calculated by summing the items, with a higher score indicating higher burden. The internal reliability of the scale in the present study was high (Cronbach α = .82).
Procedure
Participants were recruited from support groups of family caregivers in Israel and using snowball sampling. Face-to-face interviews were conducted between May 2017 and June 2018, using a structured questionnaire. At the beginning of the interview a definition of ADs and DPOA was read to the participants.
Statistical analysis
The data were coded and analyzed using SPSS version 25.0 (SPSS, IBM Corp, 2017). Descriptive statistics were used to describe the characteristics of the sample and the main variables. Pearson and Spearman correlations were used to examine the associations between willingness to undertake ACP and the variables in the extended model of TPB. Hierarchical regression analysis was performed to test the contribution of the variables of the TPB to the willingness to undertake ACP. In the first step, the traditional variables were included (attitudes, subjective norms and perceived control). In the second step, the variable of the extended model of the TPB—ARs—was analyzed. In the third step, the variables the wish to prolong life and caregivers burden were added. Finally, the research model was examined with path analysis (AMOS ver.25).
Ethical considerations
The study protocol was approved by the Ethics Committee of the Faculty of Social Welfare and Health Sciences at the University of Haifa (148/16).
Results
Willingness to undertake ACP
The distribution of the six items used to assess willingness to undertake ACP are presented in Table 1. Participants’ overall willingness was moderate, and the highest willingness reported by the participants was to appoint a durable power of attorney. Moderate willingness was reported toward signing ADs, downloading and reading the documents and talking to family members. Participants expressed low willingness to talk to their doctors regarding undertaking ACP.
Correlations among TPB variables
As can be observed in Table 2, willingness to undertake ACP was significantly correlated with attitudes, subjective norms, perceived control, ARs, and the wish to prolong life. The strongest relationship was found between willingness to undertake ACP and attitudes and between willingness to undertake ACP and ARs. There were no significant associations between willingness to undertake ACP and caregiver burden.
Correlation coefficients among determinant variables and willingness to undertake ACP.
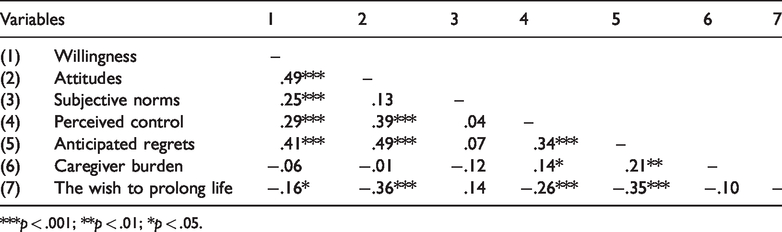
***p < .001; **p < .01; *p < .05.
Determinants of willingness to undertake ACP
As can be seen in the first step of the hierarchical regression analysis (Table 3), the three classical variables of the TPB model (attitudes, subjective norms and perceived control) explained 25% of the variance in willingness to undertake ACP, with attitudes being the main determinant, followed by subjective norms. In the second step, the inclusion of ARs added an additional 3% to the explained variance. Finally, in the third step, caregiver burden and the wish to prolong life added an additional 2% to the explained variance even that this was not found to be statistically significant. Overall, all the variables explained 30% of the willingness to undertake ACP.
Regression analysis of the model’s component on willingness to undertake ACP (N = 195).
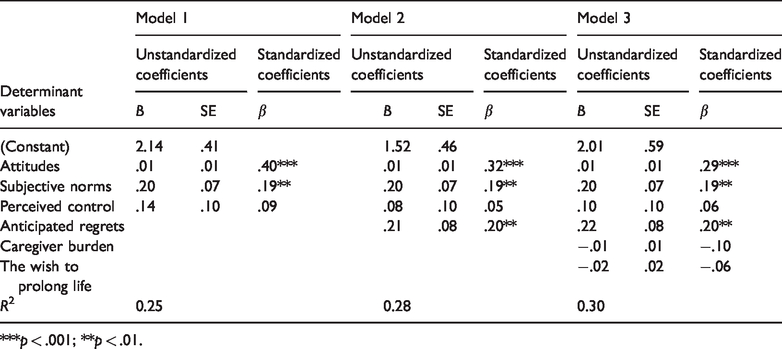
***p < .001; **p < .01.
Path analysis
The study model was found to fit the data well: χ2(10) = 12.85, p = .232, NFI = .949, NNFI = .953, CFI = .987, RMSEA = .040. As shown in Table 4 and Figure 1, attitudes toward ACP and subjective norms were positively related with the willingness to undertake ACP, yet perceived control was unrelated with it. Further, the wish to prolong life was negatively related with both the attitudes toward ACP and perceived control; AR was positively related with the attitudes, perceived control, and the willingness to undertake ACP; and caregiver’s burden was unrelated with any of the other variables. Several indirect relationships involving the wish to prolong life and AR, as independent variables, and attitudes toward ACP as a mediator, were significant. Analysis of the indirect relationships revealed that the total indirect effects stemming from the wish to prolong life (standardized indirect effect = −.072, SE = .032, p = .015) and AR (standardized indirect effect = .158, SE = .041, p = .003) are significant, yet the indirect effect of caregiver burden on the willingness to undertake ACP is non-significant (standardized indirect effect = −.065, SE = .033, p = .055). Thus, and as may be observed in Figure 1, the attitudes toward ACP may mediate the relationship between both the wish to prolong life and AR, and the willingness to undertake ACP. These possible mediations were examined with Selig and Preacher’s Monte Carlo method for assessing mediation with bootstrapping (Selig & Preacher, 2008), and were found significant. Results reveal significant mediated relationships for the wish to prolong life (95%CI = −.198, −.043) as well as for AR (95%CI = .069, .257). A lower wish to prolong life and higher AR were related with more positive attitudes toward ACP, which in turn was related with a greater willingness to undertake ACP.
Direct relationships between the variables (N = 195).
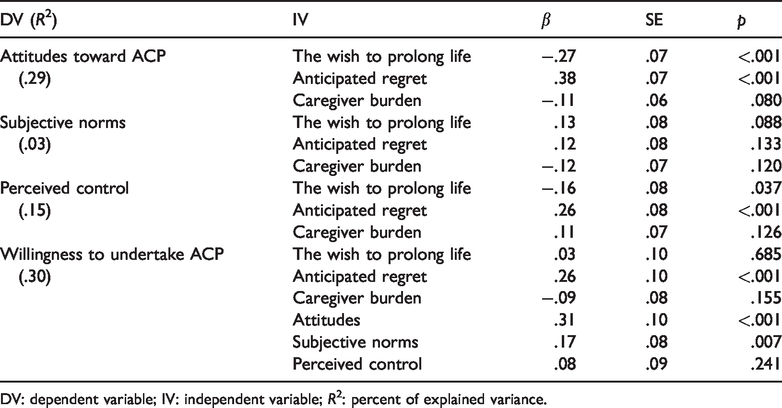
DV: dependent variable; IV: independent variable; R2: percent of explained variance.

Path model of willingness to undertake ACP.
Discussion
The purpose of this study was to evaluate the willingness of family caregivers of people with dementia to undertake ACP for themselves using the TPB. Overall, participants expressed moderate willingness to undertake ACP.
The descriptive statistics of our study indicated that appointing a durable power of attorney (DPOA) was the most preferred option reported. Unlike signing advanced directives, appointing a DPOA means that the person does not need to make fateful medical decisions for him/herself in advance, but rather can leave those decisions to their DPOA who will make these decisions for him/her at end-of-life. Since the appointed DPOA is usually a family member (Sudore, 2019), the high willingness expressed by participants in this study to appoint a DPOA is an interesting finding, considering that the respondents were family members dealing with decision making for a person with dementia who know the difficulties of making medical decisions for someone else. Despite (or because of) this experience, they still expressed high willingness to appoint a family member to decide for them, which could result in future caregivers experiencing the same difficulties that they experience now as caregivers. A possible explanation for this finding may be the participants’ sense of filial responsibility. Filial responsibility is a general societal attitude toward adult children’s duty to care for their aging parents’ needs and what their appropriate behavior should be (Stein et al., 1998). Among older people and family caregivers in Israeli society filial responsibility is considered an important norm (Iecovich, 2018). Given this norm, we can assume that participants in our study expect that their own family members will take care of them and make medical decisions for them in the future just as they do today for their family members.
The lowest willingness reported by participants referred to readiness to talk to their doctor about their preferences for end-of-life care. This is consistent with previous findings: In a study conducted among 1823 community-dwelling older people in England that aimed to assess their attitudes toward ACP only 17% were found to have had discussions about ACP with their physician (Musa et al., 2015). Having conversations about end-of-life requires a dyadic interaction between the doctor and the patient, with the doctor assuming a main role in these conversations. In a systematic review that examined the factors associated with initiation of ACP among people with dementia, it was found that professional caregivers’ initiative or lack thereof was an important factor that facilitated or hindered initiating ACP conversations (van der Steen et al., 2014). Moreover, in order to talk to the doctor about medical decisions for end-of-life, the right opportunities, time and place need to be found to hold these conversations (Dening et al., 2019; Towsley et al., 2015; Venne et al., 2015).
The results of our study indicated that, as assumed by the TPB, attitudes toward ACP, subjective norms and AR were the main determinants of willingness to undertake ACP. Attitudes were the strongest correlate of willingness to undertake ACP. In accordance with the TPB assumptions, findings of our study showed that participants who expressed more positive attitudes toward ACP had more willingness to undertake ACP. Similarly, in a study conducted among 204 older adults living in the United States that aimed to explore their willingness to complete ADs, it was found that participants with more positive attitudes and greater social support from family and friends had greater willingness to complete ADs (Ko et al., 2016). In another study conducted among 60 young and older Chinese Americans, it was found that both generations had positive attitudes toward ACP and believed that ACP was important and necessary. Both generations expressed willingness to have informal conversations with family members, which is an important aspect of ACP (Lee et al., 2017).
Subjective norms were also found to be an important determinant of participants’ willingness to undertake ACP, meaning that participants took into consideration the social expectations of family members in their willingness to undertake ACP. Similar findings were reported in a study conducted among 261 Korean American that aimed to examine intention to discuss ACP for a family member with Alzheimer’s disease. That study found that subjective norms were the strongest determinant of intention to carry out ACP discussions (Hong et al., 2018). The importance that participants in our study assigned to subjective norms can be explained by the strong values of familism characterizing the Israeli society (Fogiel-Bijaoui & Rutlinger-Reiner, 2013). ACP should be done with support from significant others, who can be family members, friends or professional staff. When a person feels that he/she has sufficient support to make medical decisions regarding end-of-life care, he/she may engage in the process.
Perceived control, although found to be significantly associated to willingness to undertake ACP in the bivariate analyses, was not found to be significantly related in the multivariate analysis. We can hypothesize that these results are related to the fact that perceived control in our study refers to external factors such as the difficulty to complete the documents. When a person feels that she/he has support from family member and also has positive attitudes toward a behavior, external factors may reduce the influence of other elements in their decision-making process.
AR was also found to be an important high determinant of willingness to undertake ACP. This can be explained by the accepted notion that one of the main advantages of undertaking ACP is avoiding suffering for both the sick person and the family caregivers at end-of-life. Therefore, if the medical decision that can prevent suffering is not taken in advance it can cause regret. This result matched those observed in earlier studies: In a meta-analysis conducted by Brewer et al. (2016), AR was found to have a strong association with health behavior and intention and was generally a stronger determinant than other anticipated negative emotions and risk appraisals. In another study conducted among 366 adults toward performing 20 health behaviors, it was found that intentions that were more strongly based on AR were significant stronger predictors of behavior (Conner et al., 2016).
It is interesting to note that caregiver burden was not found to be related to willingness to undertake ACP, contrary to prior studies that found that undertaking ACP reduced burden among family caregivers (Brazil et al., 2018; Poppe et al., 2013). This finding can be explained by the inclusion of strong determinant of the TPB—attitudes, subjective norms and AR—that might reduce the influence of caregiver burden on the willingness to undertake ACP.
Limitations
The present study is not without limitations. First, we examined willingness to behave rather than the behavior itself, although according to the TPB, intention to behave has been found to be the strongest predictor of behavior (Werner, 2004). Second, the convenience and homogeneous sampling of the study, e.g. Jewish caregivers limits the ability to generalize the findings to the overall caregiver population. Further research should be conducted among a more heterogeneous sample. Third, the cross-sectional design of the study limits our ability to deduce causal relationships between variables. Fourth, face-to-face interviews can cause social desirability bias of the responses, especially on personal issues, such as caregiving and decision-making.
Conclusions and implications
To the best of our knowledge this study is the first to examine the willingness of family caregivers of people with dementia to undertake ACP for themselves, taking into account that they have experience of being caregivers and making medical decisions for someone else. The results of our study highlight the different determinants in the decision making process for end-of-life treatments, as expressed by family caregivers.
This study has theoretical and practical implications. Theoretically, the TPB was found to be a suitable framework to explain the willingness of family caregivers to undertake ACP for themselves. Our results showed that attitudes, subjective norms, and AR were strong determinants of willingness to undertake ACP. Further research should focus on understanding additional psychological, social and socio-demographic factors that encourage family caregivers of people with dementia to undertake ACP for themselves.
These findings have important practical implications for developing interventions for family caregivers of people with dementia that can encourage them to undertake ACP for themselves, when they still have capacity to make medical decisions and spare the burden that they experience from future family caregivers. The results indicating that participants’ attitudes were the strongest determinant of willingness to undertake ACP can highlight the opportunity to develop programs and interventions to encourage family caregivers to undertake ACP. These interventions should provide family caregivers opportunities to make medical decisions regarding end-of-life care, to emphasize the advantages of the process and involve family members in the formal documentation of end-of-life preferences, along with having informal conversations with significant others about their preferences for medical care.
The low willingness of participants to talk to their doctor about end-of-life care underscores the need to encourage professional staff in community care to initiate conversations with their patients regarding end-of-life preferences, even when they are healthy. There is a need for professional staff to be more involved in the decision-making process. We suggest that having end-of-life conversation should be part of the routine in Health Maintenance Organizations. In order to reach this aim, professional staff should have more awareness and knowledge of ACP and should be trained to initiate and conduct ACP conversations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.