
Abstract
The term dementia-friendly hospital is increasingly used to describe a variety of initiatives and strategies that are implemented to meet the challenges faced by patients with dementia during hospitalization. However, no definition of the dementia-friendly hospital currently exists. This qualitative focus group study aimed to describe stakeholders’ perspectives of the dementia-friendly hospital. Four stakeholder groups were included: people with dementia, relatives, hospital staff, and representatives from the Danish Alzheimer Association. The thematic analysis suggests that a person-centered approach is a key feature. This approach is described as a continuously reflexive awareness of how to see the person behind the dementia diagnosis. We discuss possible revision of the current dementia discourse and the implications of the findings for future practice and research.
Keywords
Background
Hospital admissions for people with dementia are expected to increase in the future due to increasing numbers of people with dementia (Patterson, 2018) and the comorbidities that are commonly associated with a dementia diagnosis (Galvin et al., 2010; Lin et al., 2013). Hospitalizations often cause a downward health spiral for patients with dementia, as the care of these patients in hospitals tends to be suboptimal and trapped in medical and task-orientated routines (Allwood et al., 2017; Dewing & Dijk, 2016; Featherstone et al., 2019; Innes et al., 2016). Some of these suboptimal outcomes are described as negative patterns of resistance (Featherstone et al., 2019), increased confusion (Allwood et al., 2017), and a lack of dignity in care (Innes et al., 2016). A broad array of political requirements has resulted in several dementia-friendly hospital strategies and initiatives worldwide (Dementia Action Alliance, n.d; Grey et al., 2018; Ministry of Health and Care, 2016; The Scottish Government, 2017), and the Danish national dementia strategy includes a focus on the development of dementia-friendly hospitals (Ministry of Health, 2017).
Introduction to dementia-friendly hospitals
The term dementia-friendly hospital is most commonly used in relation to educational initiatives and environmental design, with a focus on improving care and treatment of patients with dementia (Hebert & Scales, 2017). There is an emerging body of evidence about dementia friendliness in hospitals deriving mostly from the United Kingdom. This evidence suggests that educational initiatives have a positive impact on the knowledge and competencies of hospital staff (Scerri et al., 2017; Surr & Gates, 2017), though a sustainable effect is unknown. Further, there is some evidence that changing the physical environment toward dementia friendliness may improve the safety and well-being of these patients in acute settings (Brooke & Semlyen, 2019; Eastham & Cox, 2017; Parke, 2017), revealing sparse knowledge about general hospital settings. However, the current state of dementia friendliness in hospitals is questioned, and an important inquiry is whether these implemented initiatives actually create dementia friendliness in hospital settings. A qualitative evidence synthesis with the aim of exploring the perspectives of patients with dementia in acute hospital settings showed that patients with dementia prefer that their “person” is valued and identified some deficiencies with acute hospital care of patients with dementia, for example, paternalistic and task-focused approaches, despite the increased focus on dementia in hospitals (Reilly & Houghton, 2019). Furthermore, dementia friendliness appears to be far from internalized in hospitals from the carers’ perspective. A systematic review found that the dignity is missing in acute hospital care, and the support for patients with dementia to handle basic needs is insufficient (Beardon et al., 2018). Additionally, a metasynthesis showed that hospital staff in general hospitals find it challenging to deliver person-centered care to patients with dementia and that hospital staff tended to have negative attitudes toward patients with dementia (Turner et al., 2017).
In summary, some of the challenges in implementing dementia friendliness in hospital settings could be due to the difficulties in combining hospital routines and person centeredness. Furthermore, a shared pathway concerning dementia friendliness among hospital staff is requested (Reilly & Houghton, 2019). Additionally, some of the challenges of applying dementia friendliness in hospitals may be due to different operationalizations of the term dementia-friendly hospital across settings and disciplines, as suggested by Hebert and Scales (2017). These authors advocate for continued research focus on such terms in the expectations that more precise definitions will lead to better identification of dementia-friendly initiatives (Hebert & Scales, 2017).
The continued development of dementia-friendly initiatives in hospitals requires the inclusion of important stakeholders’ perspectives (Heward et al., 2017). A comprehensive understanding of how to approach patients with dementia in hospitals must draw on these perspectives (Prato et al., 2018; Xidous et al., 2019).
The aim of this study was to explore and describe stakeholders’ perspectives of a dementia-friendly hospital. Additionally, we sought to identify similarities and differences in the aspects of importance to the stakeholders in relation to the description of a dementia-friendly hospital.
Method
Study design
We used a qualitative design based on focus groups to explore the subject and provide in-depth descriptions (Halkier, 2016). The descriptive approach guided us to stay close to data in order to produce rich descriptions (Sandelowski, 2000) with a focus on emic knowledge, which can then be used to guide implementation of initiatives and interventions (Bradshaw et al., 2017), such as dementia-friendly initiatives.
Participants and recruitment
Focus group interviews with the four following stakeholder groups were conducted. People with dementia were invited in order to get a firsthand perspective. Relatives were invited, as they are close to the people with dementia and know about most of the needs of people with dementia in hospitals. Hospital staff with extended knowledge of dementia were invited. Representatives from the Danish Alzheimer Association were invited in order to represent the interests of people with dementia, and further, this organization has an active voice in dementia strategies and politics in Denmark. The inclusion criteria for all participating groups were their respective belonging to the groups. In addition, we searched for participants among people with dementia and relatives who had experiences with hospitalization, which was the case for all participants in these groups.
Demographic information of the stakeholder groups.
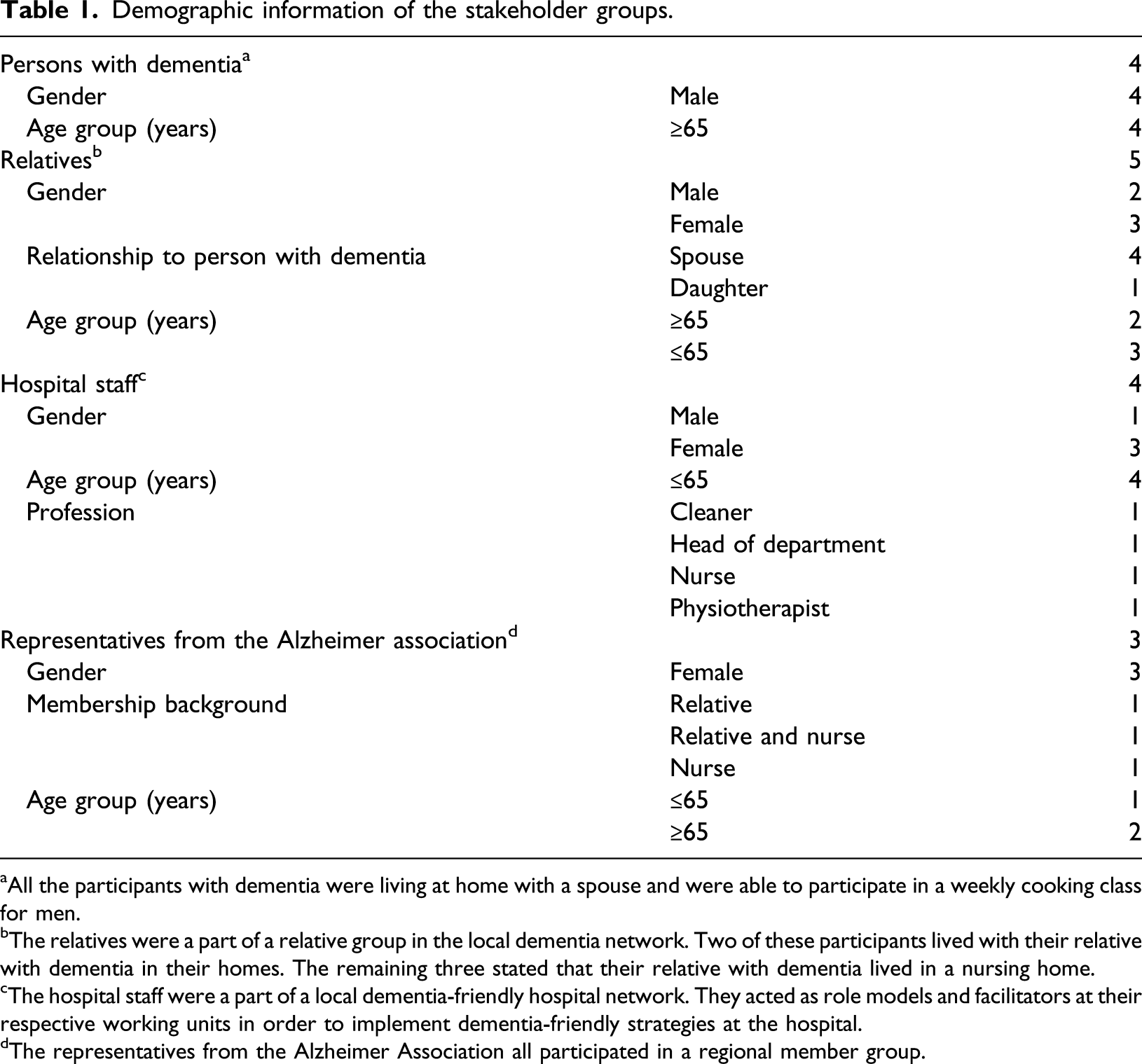
aAll the participants with dementia were living at home with a spouse and were able to participate in a weekly cooking class for men.
bThe relatives were a part of a relative group in the local dementia network. Two of these participants lived with their relative with dementia in their homes. The remaining three stated that their relative with dementia lived in a nursing home.
cThe hospital staff were a part of a local dementia-friendly hospital network. They acted as role models and facilitators at their respective working units in order to implement dementia-friendly strategies at the hospital.
dThe representatives from the Alzheimer Association all participated in a regional member group.
Data collection
One focus group interview in each participant group was conducted from November 2018 to January 2019. The order of the interviews was: relatives, people with dementia, representatives from the Alzheimer Association, and hospital staff. This order was guided by availability/accessibility of the participants and practical circumstances. The interviews lasted between 50–70 minutes. The first author, who is a trained nurse, was the primary interviewer, and the last author acted as a moderator in the interviews with relatives, hospital staff, and representatives from the Alzheimer Association. A fellow PhD student acted as a moderator in the interview with persons with dementia. In the interviews with the participants with dementia and the relatives, the gatekeeper nurse participated as a listener.
The interview guide was refined from the current literature about persons with dementia in hospitals and dementia-friendly initiatives, policies, and local-implemented strategies. The interview guide had a structured form, as recommended in qualitative descriptive studies (Neergaard et al., 2009), and was dynamic, as the discussions in one interview led to topics and questions that could be elaborated in the next interview. Each interview included an introduction to the term dementia friendly and the status of the definition of this term. Different opening questions were used to introduce topics and start discussions. These questions had different phrasings depending on the focus group participants. Following examples serve as an overview of open-ended and topic-guided questions: “Can you recall an experience from the hospital with a patient with dementia?,” “What is the first thing that you think of when I say hospital?” followed by “Do you like to be at a hospital?,” “What are your thoughts about what constitutes a dementia-friendly hospital environment?,” “What do you think should be the characteristics of hospital staffs’ dementia-friendly approach?,” and “What are your thoughts about the entire workforce in the hospital being educated in dementia topics?” Additionally, specific question-guided discussions, for example, questions about the “life storybook” as a tool during hospital stays. The interviews were audio recorded and transcribed verbatim by an external assistant.
Ethical considerations
The study followed the Helsinki Declaration (World Medical Association, 2013). Informed consent was obtained from all participants orally and in writing. Further, all participants were informed that it was possible to withdraw at any time. To assure that the participants understood their involvement in interviews, all focus group interviews started with the interviewer repeating the aim of the study orally and written material was provided if the participants wanted it. The group of participants with dementia required additional considerations concerning the recruitment (West et al., 2017) due to the affected memory of these people (Drageset, 2019). Therefore, this interview started with short information about the study combined with small talk about their attendance in the current cooking course. This was done to create a positive atmosphere and to assure that the participants with dementia were supported to participate in an informed basis (Hellström et al., 2007). Concerning informed consent, this was sought as a process of consent (Rivett, 2017). This entailed that we returned to the aim of the interview several times in order to clarify what the interview was about.
Analysis
The analytical process was inspired by inductive reflexive thematic analysis as described by Braun and Clarke (2006, 2019). Furthermore, the comparison group approach was applied to broaden the insight into the descriptions of the important elements of the dementia-friendly hospital (Lindsay, 2019). The analytical process started with the reading and rereading of each transcribed interview to obtain familiarity with the data. This was followed by an initial coding of each transcript individually, identifying a mix of semantic and latent codes across the dataset. The analytical question “How are important elements that constitute a dementia friendly hospital expressed and described by participants?” served as guidance in the initial coding phase. Then, the codes were sorted into potential themes within the whole dataset, and a comparison between groups identified similarities and differences.
The last step in the analytical process resulted in the development of one overall theme (seeing the person behind the dementia diagnosis) and two themes (balancing knowledge and facilitating protection) with subthemes (significant knowledge about the person, significant knowledge about dementia, protective surroundings, respectful disclosure of the dementia diagnosis, and significant others). The identified themes and subthemes were reviewed across interviews to ensure coherent descriptions and unique content with minimal overlap. Next, the themes were applied to the transcripts to assure applicability. The first author did the initial coding and the identification of themes and subthemes, and the first, second, and last authors named and defined the themes and subthemes. All authors discussed the final themes. The data were handled manually.
Findings
The findings in this study are illustrated in the thematic map in Figure 1 and elaborated below. In line with the descriptive analytical approach, the findings include manifest descriptions of data that stay close to the participants’ voice, and latent levels that go beyond the surface of data, through interpretation (Braun & Clarke, 2006, 2019). Quotes (group and participant number) from the interviews illustrate opinions throughout the findings section to ensure transparency and close connections between data and findings. Thematic map showing themes and subthemes.
Seeing the person behind the dementia diagnosis
The overall theme was consistent throughout the expressed descriptions in the data and represented a person-centered approach viewed as essential to the description of a dementia-friendly hospital. All participants across the groups were in agreement that if this approach was missing, the implemented initiatives would only make a slight difference. The hospital staff expressed that they were concerned that dementia-friendly strategies were just a new quality marker, and that the department would revert to previous routine over time, based on earlier experience regarding implementation of different initiatives in the hospital setting. One participant described specifically that knowledge on how to maintain a continued focus on the person and dementia is of crucial importance if a dementia-friendly hospital intends to meet the individual expectations and needs of patients with dementia: “Implemented initiatives must not result in overlooking the persons with dementia in new dementia friendly routines” (Hospital staff 4).
Most of the participants were convinced that if a hospital is going to succeed in being dementia friendly, there is a need to focus more on “friendly” than “dementia” as this prioritization will diminish stigmatization. A way of exemplifying this was visible in the following quote: “If you say dementia friendly, this indicates that the diagnosis is more important than how you approach the person” (Hospital staff 4).
The participating groups all emphasized a friendly person-centered approach, with everyday expressions being used to describe the quality of the approach in encounters between people as an answer to the question: “Describe the most important element in a dementia-friendly hospital”: “The cliché about warm hands is not dead. Patients with dementia are dependent on these” (Hospital staff 1) “It all depends on the eyes—I mean: observe and sense beyond the visible signs and symptoms” (Representative from the Alzheimer Association 1) “The most important element in dementia friendliness is staff with a heart” (Relative 3) “True kindness is important—some persons have this innate kindness others don’t” (Person with dementia 4)
These quotes solidify that dementia friendliness goes beyond what can be taught but also depends on an intrinsic quality of how you recognize other people.
An important aspect of the person-centered approach described by all participants was to recognize the full potential of the patient with dementia. This was expressed as a continuation of a narrowed focus on meeting the needs of patients with dementia to a more holistic approach. The participants in all groups agreed that even though you have dementia there is a need to be treated as persons with potential and not in a regressive way. Participants described this in various ways. One of the participants with dementia said: “They have to include me in the decisions and not ignore my ability to contribute” (Person with dementia 5).
Supplementary, a relative expressed: “I know that my wife’s answers to specific questions do not always make sense, but that doesn’t mean that she should be excluded because she has opinions about how she wants things to be done. I think that it is important to respect that” (Relative 1).
Balancing knowledge
This theme illustrates that if a hospital is dementia friendly, it is required that the hospital staff have comprehensive knowledge about the patient as a person and the diagnosis of dementia. The sources of knowledge can vary and need to be applied in a balanced way, with the aim of seeing the person behind the diagnosis.
Significant knowledge about the person
All participants across sample groups expressed that knowing the person is of crucial importance; however, there was some disparity about what this entailed. Representatives from the Alzheimer Association and hospital staff argued that a life storybook with pictures of the former life, grandchildren, house, etc. could be a mediator for conversations. This life story perspective could prevent misunderstandings and escalating aggressions and resistance and thereby create a basis for a respectful inclusion in the clinical situations. As one hospital staff said: “If there is available knowledge about their former profession or family relations, this can be an appropriate way of approaching them as persons” (Hospital staff 4).
In contrast to this, the participants with dementia rejected life storybooks as an important element in dementia-friendly hospitals and expressed that there is no need for the healthcare professionals in hospitals to know everything about them. They suggested that an actual status of their condition and daily living could be enough: “If they have some insights into my current challenges, that is enough, as long as they treat me as me” (Person with dementia 2).
As a third perspective of important knowledge about the person with dementia, relatives unanimously agreed that the most important issue is to know how to meet the basic needs of patients with dementia. One relative said: “The most important knowledge to secure a dementia friendly approach is to know if the patient can manage meals by herself, walk, manage toileting, and get dressed by herself” (Relative 3).
Significant knowledge about dementia
All participants agreed to some degree that dementia education for all hospital staff is important as it can create a basis for meeting the needs of patients with dementia in different settings and situations. The idea of educating the whole workforce in a hospital was acknowledged and appreciated across groups. This fundamental basic knowledge was described as an assurance of the right approach no matter where or with whom the patient with dementia interacts. The following quote illustrates this: “If a patient wanders around by the elevators, and it is clear that this person doesn’t know how to manage the buttons. Then a basic knowledge about dementia is of great advantage to a hospital porter because he will approach this patient with caution” (Hospital staff 2).
Similarly, in circumstances with short encounters with different staff and transfer to other departments, knowledge of dementia is a need for all staffing groups, despite the limited time staff interacts with the patient: “It can be overwhelming to go to an X-ray examination. So if the hospital staff know something about dementia, a lot of problems can be avoided” (Representative from the Alzheimer Association 1).
However, it was a clear and common opinion across participant groups that knowledge about dementia obtained through education is in itself not enough to create a dementia-friendly hospital. An expressed concern was that knowledge needs to be continuously nurtured and personalized. This was reflected in the group discussions, as a concern regarding implemented education as being effective as long as it is being implemented, without considerations about how knowledge is translated into practice and how to maintain knowledge in the hospital. Furthermore, the participants across all groups expressed a concern about the tendency to treat all patients with dementia the same, when basic knowledge about dementia provided to all staff is considered and used unreflective. In line with the importance of maintaining dementia-friendly approaches, a participant with dementia described his concern about believing too much in education: “One thing is to attend a class; another thing is to use your knowledge” (Person with dementia 4).
Facilitating protection
Participants across the groups expressed that an important element in dementia-friendly hospitals is to protect the patient with dementia as a person. This overall idea of protection included various elements. The stakeholders’ descriptions appeared with some difference; however, a common point in their views was that the overall aim of protecting the patient with dementia was to facilitate the feeling of safety and avoidance of feeling humiliation.
Protective surroundings
All participants expressed a transparent protective environment as a constitutive element of dementia-friendly hospitals. This included making wayfinding easier through use of signage (such as for toilets/dining rooms), as this could prevent people with dementia becoming lost. One participant described this as follows: “I prefer pictures illustrating the function of the rooms, then I can avoid ending in the chapel instead of the toilet” (Person with dementia 4).
Additionally, most participants said that simplicity in areas like hallways and patient rooms would be of great benefit to patients with dementia, as this can minimize over stimulation. One relative shared her opinions: “If there are too many medical objects in the rooms, patients with dementia can feel uncomfortable and kind of losing themselves. A simple arrangement would be preferable as this gives a feeling of safety” (Relative 1).
Furthermore, another participant expressed that he preferred to be protected and thereby avoid humiliating himself: “If I don’t know where to go or what to do with things, I make a fool out of myself and afterwards I feel embarrassed” (Person with dementia 2).
Another way of protecting patients with dementia from stimulation like noise and visual impressions was the use of bed partition screens. This was described differently among participants across groups and illustrated how considerations about protection include an awareness of the delicate balance between real protection and pseudo-protection. The participants with dementia and the representatives from the Alzheimer Association expressed that the use of bed partition screens could be misinterpreted help, since patients with dementia often forget where they are, and therefore a bed partition screen can cause unintended fear of being alone as well as in the wrong place, followed by an attempt to escape. In contrast to this, relatives and hospital staff described that the use of bed partition screens to protect the patient with dementia included decisions about how to protect other patients from accidental disturbances. This was expressed as a concern related to protect the patients’ feeling of shame, if they disturbed fellow patients unintentionally.
Respectful disclosure of the dementia diagnosis
In all group interviews, the disclosure of the dementia diagnosis was discussed in relation to protection of the patient with dementia. The discussions revealed that visually showing the diagnosis in one way or another requires awareness of how this information is handled, and both positive and negative views emerged. Positive views were that it could create a basis for an immediate awareness on how to identify and approach the patient with dementia, thereby avoiding misunderstandings and improving communication. The hospital staff described how the disclosure could improve the interdisciplinary collaboration around the patient. One hospital staff said: “If knowledge about the patient having a dementia diagnosis is assessable to the staff involved, it would make transfers to other departments easier and it will be beneficial to the patients when staff is prepared to have an extended awareness of deviations from scheduled routines if necessary” (Hospital staff 1).
Negative views included the risks of neglecting the patient’s ability to contribute to any kind of collaboration in the hospital context and of limiting the focus to the dementia diagnosis. Whether the patient’s dementia diagnosis should be visible in form of a clear sign on the first page of the medical record, a badge, or a bracelet in a specific color was a point of contention. In the group of participants with dementia, there were some concerns and disagreements regarding disclosure. One participant said that if he was lost and had problems with finding his way around, it would be helpful if it was visible for the staff that he had a dementia diagnosis. Another participant said he would reject the disclosure as a badge like visually impaired people due to the stigmatizing effect: “I am afraid that the first impression of me will be that I have dementia and that it doesn’t make sense to include me. I am more than my dementia diagnosis” (Person with dementia 1).
The relatives were clear in their opinions and described the subject of disclosure as balancing on a knife edge between protection and exposure. One relative shared her opinion: “I think that you should consider whether it serves the patient to have this visible and easy accessible knowledge because they don’t have a possibility to judge if it actually reduces them to a diagnosis” (Relative 5).
Significant others
Facilitating protection as a part of dementia friendliness in hospitals also included protecting the patients from feeling lonely and anxious. The participants across the groups agreed that dementia friendliness in hospitals requires the option to have significant others stay nearby during hospital admissions in order to bring the person with dementia to the forefront. All participants appreciated the involvement of relatives during hospitalization. However, this involvement should always be approached in a balanced way in order to protect the patient from being overruled with no opportunity to share their views and at the same time not to expect too much of the relatives’ participation in treatment and care. One member of the Alzheimer Association expressed: “It is important that there is an attention on the relatives’ role during hospitalization. I think that their most important role is to make the patient feel safe by simply just being there” (Representative from the Alzheimer Association 3).
Similarly, most of the participants expressed that the attendance of relatives is invaluable when a person with dementia is hospitalized, as they can create safety spaces by representing something well known. Furthermore, an important point in the interviews was that the relatives can act as mediators when the memory fails, though the views of the person with dementia should not be overlooked. A participant with dementia said that though he preferred to be addressed personally, he feels lost without his wife: “It’s not that I do not get what they say, but I like that she acts as my memory and sits next to me” (Person with dementia 2).
In addition to the importance of relatives’ attendance, some of the participants expressed that the cooperation with relatives also included that they are permitted to take a needed break. Balancing the involvement of relatives was expressed as a part of dementia friendliness, since protection goes beyond the patient with dementia by embracing and respecting the relatives as important persons. “Living with a spouse with dementia can be a full-time job. It should be legal to take a break” (Relative 5).
Discussion
The aim of this study was to explore and describe stakeholders’ perspective of the dementia-friendly hospital and to identify similarities and differences between these perspectives. Through the perspectives of stakeholders, we have been able to broaden the insight into important elements in the constitution of the dementia-friendly hospital. The perspectives of the involved stakeholders support the importance of already ongoing initiatives, as our findings of “balancing knowledge” and “facilitating protection” reflect some aspects of these initiatives (Brooke & Semlyen, 2019; Eastham & Cox, 2017; Surr et al., 2018). Nevertheless, our findings add a new dimension of crucial importance in the description of the dementia-friendly hospital. This dimension goes beyond specific initiatives and supports a need for a continuously reflexive approach toward seeing patients with dementia as persons.
Our findings showed that the participants challenged the term dementia friendly and suggested that friendly should be prior to dementia as an indicator of dementia friendliness in hospitals. This is similarly acknowledged in a study of dementia-friendly indicators pointing to friendly and supportive as important dementia-friendly hospital indicators (Wu et al., 2019). Moreover, the critical view on dementia friendly as a term aligns with the focus in a review of dementia action plans and strategies in western countries (Lin & Lewis, 2015). In the study by Lin and Lewis, they recommend that dementia friendly should be extended as a concept by including dementia capable and dementia positivity. By integrating these terms, the authors suggest that the optimal line for dementia friendliness is encompassed. They argue that dementia friendly stands for involving and including people with dementia, but as a term, it is insufficient as it fails to include how to involve and how people with dementia are viewed as persons. Hence, they suggest the addition of dementia capable in order to ensure that the needs of people with dementia are addressed and met. Further, they suggest that dementia positivity as an additional element to dementia friendly can create a complete fulfillment of the term dementia friendly. This addition includes strength finding as an approach to reflect that people with dementia are viewed as true contributors (Lin & Lewis, 2015). This extension of the term dementia friendly is exactly what the participants in our study requested, as they were in agreement that the fulfillment of care and treatment, as well as the involvement during hospitalization, lies with seeing the patient with dementia as a person of potential.
As a constitutive element in the description of the dementia-friendly hospital, our findings point to a need for a discussion of the current dichotomized dementia discourse between tragedy and living well as described by McParland et al. (2017). According to the stakeholders’ descriptions in our study, dementia friendliness in hospitals primarily concentrates around how to support patients with dementias’ ability to remain a person during hospitalization rather than focusing on the limiting consequences caused by the dementia diagnosis. This coincides with findings from a study describing how patients with dementia experience encounters with hospital staff in general hospital settings (Toubøl et al., 2020). This study indicates that the current dementia discourse seems to challenge how patients with dementia are recognized in hospital settings. It is argued that the personal contribution of the patient is often overlooked resulting in an underestimated importance of sustaining personhood. This is further supported in the results of a qualitative study showing that constructing an identity for patients with dementia within a hospital setting is challenging due to issues about patients with dementia being described in respect to their care needs or in a task-orientated language, leaving the person with dementia as a bystander (Quirke et al., 2019). A new dementia discourse would benefit from being guided by an ethical reflective tool in order to adapt a more supportive approach with a focus on selfhood, seeing the person as a whole, and that persons with dementia have the rights and opportunities to grow and contribute in relationships as described by Reed et al. (2017). This is also the essence of our key findings describing important constitutive elements of the dementia-friendly hospital and is recommendable in shaping future directions of dementia friendliness with the aim of overcoming the dichotomized discourse. To manifest this new dementia discourse could serve as a guide in dementia-friendly initiatives in order to respect the limited resources in persons with dementia and at the same time acknowledge the remaining abilities in order to live a meaningful life (De Vugt & Dröes, 2017).
Methodological considerations
This study gave valuable insights of stakeholders’ perspectives of the dementia-friendly hospital, though our findings reflect a small sample of stakeholders (Bradshaw et al., 2017). Their insights are invaluable and requested as they add important knowledge to the current understanding of dementia-friendly hospitals (Bunn et al., 2017; Reilly & Houghton, 2019). The descriptive approach ensured that we gave voice to firsthand knowledge, as the stakeholder perspectives are interpreted consistently to the opinions voiced during interview discussions (Bradshaw et al., 2017; Neergaard et al., 2009). Furthermore, the thematic analysis allowed us to focus on both manifest and latent levels, with no attention to quantify but merely searching for what the participants described as most important (Vaismoradi et al., 2013).
The inclusion of people with dementia is a strength in our study, as their perspectives are requested and needed (Heward et al., 2017). Persons with dementia have been sparsely included in research, though their perspectives contribute an urgently required authentic perspective (Hebert & Scales, 2017). However, this interview was different from the others, since the questions to start the discussions were shorter and more guiding as recommended (Cridland et al., 2016).
During the interviews, the interviewer paid attention to balance between the structured interview questions and the explorative open-ended questions. This was done to assure that the phenomenon of interest: dementia-friendly hospital was covered and illuminated by the participants’ perceptions and not the leading nature of the interview questions.
The sample of participants with dementia represents some limitations, since their perspectives may not coincide with perspectives of those with late stage dementia or those who are younger, or female. Another sample limitation was that all representatives from the Alzheimer Association were female. A third sample limitation was that the hospital staff represented a narrow segment of the different professions in a hospital setting.
The use of gatekeepers in this study entails some limitations that should be addressed (Thoft et al., 2020). Firstly, the recruitment of people with dementia and relatives relied on building a trusting relationship to the nurse responsible for these groups. This relationship involved a close collaboration between the first author and gatekeeper in order to assure that participation in the research process took place in a constructive informed basis. Further, the gatekeepers’ attendance during the interviews signified this necessary close collaboration with the gatekeeper, as we decided to meet the gatekeepers’ wish to protect and sustain the feeling of safety in the groups.
Concerning ethical principles in interviewing people with dementia, some additional reflections are relevant to clarify. Firstly, ethical discretion was applied in the interviews, particularly in the interview with the participants with dementia in order to manage protection and minimize feelings of shame and deficiency when memory lacked. General phrases and humor were used to hide this (Drageset, 2019). Secondly, situational ethical considerations were demanded, as the participants with dementia sometimes needed to disclose some of their private conditions and relations. In these situations, the interviewer assured that the expressions were treated with respect and acknowledged (Drageset, 2019).
Conclusion and implications for practice
Our study described stakeholders’ perspectives of a dementia-friendly hospital and highlighted that a person-centered approach that builds on seeing the person behind the dementia diagnosis, as the most important element in the description of dementia friendliness in hospitals. The description of seeing the person behind the dementia diagnosis is explained as a way to balance the use of significant knowledge in every single situation and to facilitate an appropriate protection that suits the person with dementia. However, there were some differences in the participants’ descriptions of seeing the person behind the dementia diagnosis, revealing that a continuous reflection on how a person-centered approach is applied to every single situation is needed.
The results from this study add important elements to future directions in the development and implementation of dementia-friendly hospital initiatives. Guidance to dementia-friendly initiatives must rely on the principle of seeing people with dementia as equal contributors, though respectfully, as their challenges following the dementia diagnosis are recognized. An “ethical roadmap” as described by Reed et al. (2017) could be introduced as an inspiration to a new way of addressing people with dementia. The “ethical roadmap” is based on the principle of seeing the whole person and supporting this person in continuous growth and engagement as an expert on living with dementia (Reed et al., 2017).
Further research is required concerning how dementia-friendly hospital strategies are translated into everyday practices in hospitals, including the adaptability of the current dementia discourse in such settings. Additionally, a clarification of how hospital staff are supported in sustaining dementia friendliness is needed, including the elements of importance in the implementation of dementia-friendly strategies. Furthermore, future research must include an exploration of the effect of implemented dementia-friendly initiatives in hospitals from relevant stakeholders’ perspectives.
Footnotes
Acknowledgements
We would like to thank the participants in the interviews for sharing their perspectives on the dementia-friendly hospital. We also thank the gatekeepers (the Danish Alzheimer Association, the local community dementia network, and the Dementia Friendly Project team at the University Hospital) for recruitment support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Regional Danish Data Protection Agency approved the study (18/14259).