
Abstract
Individuals with dementia with Lewy bodies (DLB) commonly die from dementia-related causes, but little is known regarding caregiver experiences during the end-of-life period in DLB. This reflects a critical knowledge gap given the high frequency of informal caregiving for individuals with dementia, high caregiver burden in DLB, and the fact that most individuals with DLB die from this disease. Investigators conducted telephone interviews with family members of individuals who died with DLB in the last 5 years. Investigators used a qualitative descriptive approach to analyze interview transcripts. Participants included 15 children, 13 spouses, and 2 other family members. Interviews averaged 31 min. Major themes included caregivers as the main drivers of care for individuals with DLB throughout the disease course and at the end of life, the impact of DLB features (e.g., fluctuations, hallucinations, and delusions) on end-of-life experiences, experiences relating to the caregiving role, death and post-death experiences, and supports employed by caregivers in the end-of-life period. End-of-life experiences for caregivers of individuals with DLB built on the accumulated burden of the disease course, where caregivers were often responsible for driving DLB care—from making the diagnosis to educating healthcare professionals and double-checking medical decisions. While some end-of-life experiences were consistent with those described in dementia palliative care more generally (e.g., financial stresses, poor sleep, being overwhelmed, and needing increased education and support), many DLB features specifically affected end-of-life caregiver experiences, such as the presence of delusions. Improving caregiver experiences at the end of life in DLB will require improved diagnosis and care for individuals with DLB throughout the disease course and also better strategies for treating behavioral symptoms. More research is needed regarding drivers of quality end-of-life experiences for individuals with DLB and their families and how drivers and strategies may differ between dementias.
Keywords
Introduction
Understanding the experiences and roles of informal caregivers (hereafter referred to as “caregivers”) is critical given the frequency with which family members provide informal dementia care. In 2015, 3.4 million adults aged 65 and older lived with dementia in community settings in the United States. Almost all (95%) of these individuals received informal care, provided by an estimated 5.7 million caregivers (Chi et al., 2019). Unpaid care was the only support for 63% of these individuals with dementia, most commonly provided by spouses and adult daughters (Chi et al., 2019). Increasing research explores drivers of caregiver burden in dementia, but literature examining caregiver roles at the end of life in dementia is limited. Most caregivers of individuals dying with dementia report feeling unprepared for their loved one’s death (Armstrong et al., 2019a, 2019b; Hovland-Scafe & Kramer, 2017). A systematic review of qualitative studies with individuals with dementia and caregivers regarding advance care planning and end-of-life dementia care identified five themes: avoiding dehumanizing treatment and care, confronting emotionally difficult conversations, navigating existential tensions, defining personal autonomy, and lacking confidence in healthcare settings (Sellars et al., 2019). However, the supporting studies included individuals with various dementias and often occurred when participants were anticipating death, rather than with bereaved family caregivers.
No existing studies specifically examine the experiences of informal caregivers at the end of life of individuals with dementia with Lewy bodies (DLB), despite the fact that caregiver burden is higher in DLB compared to Alzheimer disease (AD) dementia (Lee et al., 2013; Ricci et al., 2009; Svendsboe et al., 2016). Dementia with Lewy bodies is one of the two diseases (along with Parkinson disease dementia) under the Lewy body dementia umbrella. Lewy body dementia is the second-most-common neurodegenerative dementia in the United States after AD (Barker et al., 2002). Individuals with DLB have dementia plus core features including fluctuating alertness, visual hallucinations, REM sleep behavior disorder, and parkinsonism (McKeith et al., 2017). Supportive clinical features include sensitivity to antipsychotic medications, excessive daytime sleepiness, autonomic dysfunction (including orthostatic hypotension, constipation, and urinary incontinence), postural instability, falls, non-visual hallucinations, delusions, anxiety, depression, and apathy (McKeith et al., 2017). This symptom profile explains why caregiver burden is higher than DLB than other dementias: patient characteristics that drive informal caregiver burden most strongly in dementia are the presence of behavioral and psychological symptoms and the physical limitations/functional status of the person with dementia (Cheng, 2017; Chiao et al., 2015). Many of these features worsen as individuals with DLB approach the end of life (Armstrong et al., 2019a, 2019b).
Furthermore, individuals with clinically diagnosed DLB progress more quickly to death than individuals with AD dementia (Price et al., 2017; Williams et al., 2006). Individuals with clinically diagnosed DLB live a median of 3–4 years after diagnosis (though with a wide range) (Armstrong et al., 2019a, 2019b; Larsson et al., 2018; Price et al., 2017; Walker et al., 2000). Most die from dementia-related causes including failure to thrive and aspiration pneumonia/swallowing difficulties (Armstrong et al., 2019a, 2019b; Garcia-Ptacek et al., 2016). Given the frequency of informal dementia caregiving in the United States, the unique symptom profile in DLB compared to other dementias, the known high rate of caregiver burden in DLB, and dementia-related causes of death in DLB, we aimed to investigate the end-of-life experiences of informal caregivers of individuals with DLB who died within the prior 5 years.
Methods
Study design
The current study represents the second part of a two-part study investigating end-of-life experiences in DLB. The first part of the study consisted of a survey investigating cause of death and end-of-life experiences in DLB to better understand the breadth of end-of-life experiences (Armstrong et al., 2019a). The second part of the study involved interviews with a subset of survey participants to investigate the depth and details of caregiver and family experiences.
The principal investigator conducted the interviews with family members of individuals who died with a diagnosis of DLB. A qualitative descriptive approach (Colorafi & Evans, 2016) was used to analyze interview transcripts. A qualitative descriptive approach involves reporting and summarizing straight-forward accounts of participants’ views without an intent to generate or test theory. This approach is particularly relevant in healthcare research as it is grounded in the principles of naturalistic inquiry and summarizes factual responses about how individuals feel about or have experienced a particular issue (Colorafi & Evans, 2016).
Population and recruitment
Participants were recruited through an online-only survey investigating cause of death and end-of-life experiences in DLB (Armstrong et al., 2019a). Survey eligibility required respondents to be fluent in English and an informal caregiver, family member, or friend to an individual who died with DLB in the prior 5 years. The Lewy Body Dementia Association website recruited for the survey. One survey question queried respondent willingness to participate in a telephone interview. If they answered affirmatively, they received the principal investigator’s contact information to learn study details. Individuals e-mailing the principal investigator received the informed consent form and semi-structured interview guide. Volunteers were invited largely sequentially but with purposive sampling to achieve representation of roles (spouses and children) and genders.
The University of Florida Institutional Review Board provided approval (IRB201701657). The study was conducted under a waiver of documentation of informed consent. After questions and verbal consent at the beginning of the call, recording and interviewing started.
Data collection and analysis
The principal investigator drafted the semi-structured interview guide based on existing literature and questions derived from clinical care and revised it based on suggestions from three caregivers for individuals who died from DLB, Lewy Body Dementia Association staff, and two Lewy Body Dementia Association scientific advisory board members. The final guide included 11 open-ended questions, starting with a question about general experiences and ending with questions about specific aspects of the end-of-life experience (Supplemental Material 1). The principal investigator, a DLB specialist, conducted the phone interviews. She had no prior relationship with participants. A professional service transcribed the interviews verbatim. Member checking of themes was not performed. Participants could opt to receive study findings.
Investigators used tables in Microsoft Word® 2016 to organize data and a qualitative descriptive approach to identify and organize themes (Colorafi & Evans, 2016). Overarching themes were shaped by the topics covered in the semi-structured interview guide (e.g., experiences at end of life, decisions which had to be made, and hospice use), but specific coding themes were derived directly from participant statements. A research assistant with qualitative experience but no DLB expertise independently analyzed five interviews to create a draft log of themes and related quotes (open coding) (Auerbach & Silverstein, 2003). The principal investigator served as the second coder and reviewed and revised the draft coding. Consensus was reached regarding emerging themes and this consensus was used to establish the analysis codebook. The research assistant analyzed remaining transcripts using a constant comparative technique, revising themes and subthemes if needed (axial coding) (Auerbach & Silverstein, 2003). The principal investigator reviewed and revised coding again after 20 and 30 interviews. The principal investigator assessed saturation during interviewing; both primary coders reassessed saturation during analysis. Co-investigators gave feedback after the initial coding. The current analysis focuses on caregiver experiences; interview themes relating to the dying experience and barriers to quality end-of-life care are reported separately (Armstrong et al., 2019a, 2019b). Consolidated criteria for reporting qualitative research guided study reporting (Supplemental Material 2) (Tong et al., 2007).
Findings
Data collection and participant demographics
The Lewy Body Dementia Association posted the survey link on 9/1/2017. Over 400 individuals completed the survey and over 60 volunteered for the interview within 1 week, so investigators removed the survey question querying interview interest. Investigators contacted 36 volunteers. Thirty completed interviews, four did not respond after their initial query, one opted not to participate given scheduling difficulties, and one failed to attend a scheduled interview. Investigators notified 47 volunteers that recruitment targets were reached. Interviews occurred between 9/15/2017 and 10/30/2017.
Themes and subthemes regarding the caregiver experience at the end of life of individuals with dementia with Lewy bodies.
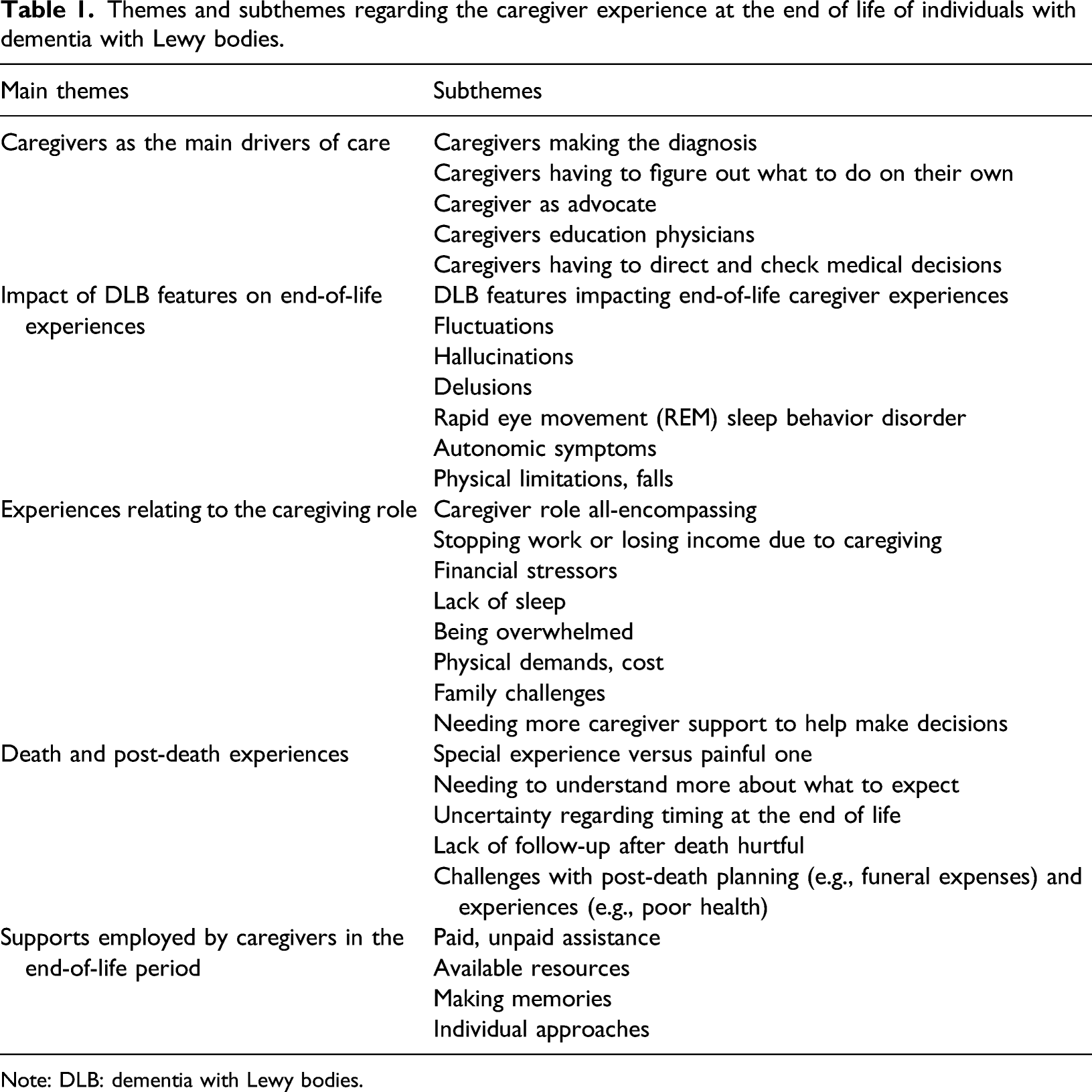
Note: DLB: dementia with Lewy bodies.
Caregivers as the main drivers of care
While the study focused on end-of-life experiences, caregivers described how they drove all aspects of care, starting with making the initial diagnosis. I started reading and I said, “You know, it sounds a lot like Lewy body dementia.” And I was trying to share the information with my mom and my mother would say, “Oh well, you're not a doctor.” And I go, “Well, I realize I’m not a doctor.” But, you know, I'm smart enough to read the symptoms... (9, daughter)
Caregivers reported that because many healthcare professionals (HCPs) were unfamiliar with DLB, the caregivers were responsible for figuring out what to do. Caregivers relied on the internet and also described having to call different places to get advice and guidance. They were surprised at how much they had to do on their own, for example, arranging for nursing home care. Numerous caregivers reported needing to play a large advocacy role on behalf of the person with DLB, particularly in living facilities: It’s the families who are the advocates. It's the families who get themselves educated and can take the time is actually the only person who's going to take care of things right. (3, daughter) I was there all the time, advocating for him, pushing, pushing, pushing. I was there, you know, eight hours a day. (15, wife) She said to me, “You have to remember that you are your husband’s advocate. You are the only one he has and don’t ever feel that you are being a bitch.” And I think those are words that everybody… that has, you know, is involved with dementia, whatever, needs to remember that they, you are their advocate. And don’t ever feel like you shouldn’t bring up something that you know is not right. (21, wife)
This advocacy occurred during all disease stages, including the end of life, when caregivers reported needing to prompt nursing home staff to check on individuals with DLB who appeared uncomfortable as they were dying. In addition to advocating, caregivers described needing to educate HCPs about DLB and safe approaches to treating people with DLB: I educate[d] physicians, “No you can’t use this type of drug.” You know, I would go in with information from the Lewy Body Dementia Association. Here are the drugs… I had to do the education. And, that’s frustrating— being a family member. (13, daughter) I had a bunch of pamphlets on what is Lewy body, and I would literally carry them around with me, and I literally handed them out in the ER… because they have no idea how to handle someone. Not only dementia or Alzheimer’s; they just don’t know Lewy body. (14, daughter) Nobody at the hospital had ever heard of Lewy body dementia. So I had my little, what I call my bible, you know, The Caregiver’s Guide to Lewy Body Dementia? That was my bible, and anytime anybody wanted to do anything, give him any medication at all, I would whip out my little book and get into a discussion with them. You know, I feel like I educated all of [region] Florida… I just feel like I was the educating force in all… (25, wife)
Caregivers struggled at times to get HCPs to pay attention to changes that the family appreciated. Caregivers also reported needing to constantly monitor decisions made at medical facilities: “At one point, he was basically comatose for five days before I realized that they had changed his medication… I had to be on it all the time even though I think he’s in a safe place and there’s people that know what’s going on” (18, wife). Because of these experiences, caregivers often entered the end-of-life period with stress stemming from the responsibility for directing and monitoring medical management. Additionally, caregivers experienced guilt when they did not catch medical errors in time. [The hospice nurse] suggested Haldol. And I didn’t research it… About two, two-and-a-half hours since he had his Haldol, he had a neuroleptic malignant episode… from there, his kidneys shut down, and he was gone by Tuesday morning… And had I been able to research it, like I had been up to that point… I would have questioned it myself. But I just really didn't have the time. (17, wife)
Underlying the theme of caregivers driving care was the frequent comment that caregivers did not receive sufficient guidance from HCPs: “I just didn't feel like I was getting any guidance from anybody” (3, daughter), “I wish I’d been more clued in, or I’d known-known more about that” (24, daughter), “you know, there’s nobody guiding us” (28, wife).
Impact of DLB features on end-of-life experiences
Many features common to DLB affected caregiver experiences from the times leading up to end of life and the end-of-life period itself. Fluctuations were a common experience: “He would go from absolute crazy, to, you know, being lucid” (4, daughter), “he would have these clear moments… those were the fleeting moments” (18, wife), “he would come in and out” (19, daughter). Hallucinations were problematic for some of the caregivers and their loved ones with DLB: “she was in distress, and her hallucinations were never benign; they were always horrific” (8, daughter), “he refused to eat and said there was concrete all over his food” (15, wife), “that was really a very difficult time because he could not comprehend that [the vision he had of people all over the house] wasn’t real” (27, wife). Delusions, infidelity, and physical violence were particularly difficult for caregivers: We did go through a very bad patch of him roaming around thinking he was Mr. I’m Gonna Have an Affair with Whoever I Can Find. That was very traumatic for me… We'd had a very strong marriage… So that was terrible to go through. Terrible, terrible, terrible. If I had known that this was part of what was going on with this disease, it would been dealt with very differently. And I would've—my heartbreak would've been very different. (18, wife) He hit me for the first time ever when he was in the hospital that first time. (10, son) I had to call the police because he started beating up on me. (18, wife) He began to get combative, but it was—I wanted to keep him home. I wanted him to be here, but I was 80 at the time… if I were 20 years younger, I could handle this so much better. But it was very, very difficult. (27, wife)
Several caregivers reported that behavioral symptoms prompted the need for institutional care. While fluctuations, hallucinations, and delusions were the most commonly described symptoms, other experiences included needing to get a hospital bed because the person with DLB was acting out their dreams (REM sleep behavior disorder) and making it even harder for the already sleep-deprived caregiver to rest, struggling with problematic constipation and urinary incontinence, and an inability of caregivers (particularly wives) to help the person with DLB (e.g., lifting) due to physical limitations.
Experiences relating to the caregiving role
Numerous caregivers described an inability to safely keep their loved one with DLB at home, and challenges relating to finding a memory or skilled nursing facility where he or she would be accepted. Regardless of whether informal caregivers provided care at home or with their loved one in a facility, participants described the caregiver role as all-encompassing: I mean, 24/7… There were times where I would have to… leave the bathroom door open, and listen while I’m going to the bathroom—- in case you heard the door open. At that point, in fact, I was very close to putting locks on the door on the inside. (6, husband) I didn’t take care of myself, I didn’t go on a vacation. I’m not a big vacationer, but I’m from New York. I like to go to the city, go to the theater. I didn’t go away at all for two and a half years. I went there every single day and spent a lot of time trying to advocate for his well-being and his care. (21, wife)
Multiple participants—both children and spouses—reported that they had to stop working or close their business in order to care for their loved one with DLB. Lack of work caused financial stress, as did the cost of home care and facilities. My aunt had saved all her life and didn’t have children… but, you who can afford $24, $26, $28 an hour? Are you kidding me? Nobody can afford that… it’s just ridiculous, the elder care in this country. (7, niece) I alert anyone that has to go into a memory-care facility, the cost is astronomical. It averaged $7,000.00 a month… And as a caretaker, you then get into a little soul—a lot of soul-searching, like, where is this money going to come from? (6, husband)
Some participants had to continue to work, and balancing work, caregiving, and other family responsibilities were challenging: “I couldn’t go out anymore, trying to work, trying—I had children myself. I was going crazy trying to manage everything (13, daughter).” Several children serving as caregivers reported having to quit their job and move back home to care for a parent with DLB or having to travel weekly to provide support, returning home only on weekends for a change of clothes and to sleep in their own bed.
Multiple participants described lack of sleep and fatigue making things more challenging: “the most difficult thing for me through the whole process was having a lack of sleep” (25, wife), “I would go two and three nights of no sleep” (13, daughter), “as a caregiver, you’re already extremely fatigued… it’s just overwhelming” (8, daughter), “I was just so tired and overwhelmed that I just wasn’t thinking straight” (16, daughter). Caregiving also had physical costs from both supporting the person with DLB (e.g., lifting for toileting) and the toll of caregiving generally. Caregiver health problems added further complexity: “At the end I was right in the middle of chemo… they almost came and took him, because I wasn’t here, but my caregiver stayed with him 24 hours a day” (30, wife).
While family could be a source of support, many participants described family challenges negatively affecting caregiving. These included a lack of support from family members—“most of my siblings really didn’t spend any time in those last two years with my dad at all; I bore the brunt” (10, son)—and family members not understanding—“I tried to have his family know what was going on, but when they saw him, he acted half-normal” (4, daughter), “I had a sibling that was in denial” (8, daughter). Caregivers described updating and educating family members by phone as “grueling.” Caregivers also related that it was challenging making decisions with other family members and relatives resenting when they were not included more in decision-making. I don’t know, because I’m still in the middle of it, what would have happened—what could have been done any differently with the rest of the family. And they took it so personally that I didn’t call a big family conference— to ask where he should go in all this. And it was a matter of I couldn’t handle it. There was an opening. I had to do it now. And if I had asked each one of ‘em, we might still be here trying to figure out because each one of ‘em would have had a different idea. (30, wife)
Many participants described needing more caregiver support and more help to make decisions. The stress and the burnout the caregivers experience; there’s just not enough support there. And it’s not just at end of life. (13, daughter) Our experience was prior to his last weeks, it was just a horrible time because making decisions and trying to figure out what to do, we didn't have a lot of help with that. (9, daughter) As I think back, I recognize that I had a lot on me, and I probably wasn't handling it as well as I should have… I think a lot of it has to do with the uncertainty of what this is, how long it's gonna happen. Is he gonna get better? What should we prepare for? … I think trying to deal with the present, not knowing what the future is going to bring was one of the hardest things. (17, wife)
Over half of participants reported regret about the care they provided—that they did not stop working earlier, medical decisions they made, using skilled nursing facilities, and/or missing the moment of their loved one’s death. I have many regrets on my attitude and reaction and responses to a lotta this... Sometimes my impatience and my weariness would get the best of me, and I would lash out, and I would say things that were hurtful, and I would be intolerant and impatient, and just so weary of everything…. And if I could go back and control that and do that again, I would. But I honestly don’t know how you do that… (27, wife) The one thing I regret now, he had been in a rehab… When his whole Lewy body symptoms flared up, he was hospitalized in rehab. It was one of those cases when a hospitalization really was the beginning of it all. And he hated the rehab, and he went downhill there rapidly. (15, wife) I still feel this guilt that I wasn't able to bring her home…. maybe if we had had hospice in the house, she would have been able to actually end her life here at home. (3, daughter)
Death and post-death experiences
The caregiver experience of the death of their loved one with DLB varied. For some families, this was a special experience: Shortly before he died, I came into his room, and he called me by this term of endearment that was—it’s so private that I’ve never repeated it to anybody. It was just a made-up name. All of a sudden—and he hadn’t said anything like this in years. You know, so I hang onto that. (22, wife) I didn’t really have much to do with him for a couple a years, but by taking care of him and everything, all—any karma between us was remedied and equalized and he told me he loved me and that I was pretty… He really made amends towards the end, and he was more open with his feelings, telling me that he loves me... I saved his phone messages where he would thank me for coming over and helping him. (29, daughter)
For other participants, the end of life was painful: She was just kind of in and out and just occasionally mumbling—you could pick up some things—and she just said something like, “You put me in the hospital. I would never put anybody here, ever—anybody.” That was the last thing she said to me. Yeah. It was really hard. (3, daughter) There was no positive feelings… I witnessed my dad die of bone cancer when he was 59. There was a closure at the end. There was— some positive, if you can say this, but there was some positive feelings of, he’s no longer in pain. He’s in a better place. With my mom, that never happened... Even though in your head you say, “I’m doing a good thing by taking care of her at the end of life.” It still doesn’t feel like a good thing. It just feels all bad. (8, daughter)
While many hospice experiences were positive, caregivers described a need to understand more about what to expect and when medications could be administered: It was very surreal, actually. The hospice team was nice. It was a little shocking because we didn’t realize that my dad wasn’t going to be eating or drinking there. (19, daughter) The very end of life was like nothing I’ve ever experienced, obviously, and incredibly painful and confusing and exhausting. I think that it was, again, not really understanding the morphine situation, like when hospice can give morphine. (14, daughter)
Timing was a major theme for caregivers around the time of death, relating to how long their loved one was expected to live, when to bring family to the bedside, and giving medications: When we finally came to the decision with hospice to withdraw food—they told me it would be about 10 to 14 days, but it ended up being more like 3 months. It was awful. (5, wife) I was setting my alarm and just every hour making sure she had her morphine. (24, daughter)
Participants described lack of follow-up after their loved one’s death as hurtful: And during the time that he was dying, you know, they’d all come in in the morning… They took care of me. When he died, I have to say, I never heard from them again, “Oh, we loved [husband]. We’re gonna stay in touch with you.” It was like he’d never existed. But that would’ve helped, you know, if they’d sent us a condolence card or something. (22, wife)
Having to plan a funeral at the time of death was another challenge, with many details to arrange. One caregiver described the onset of health problems after the loss of her husband. Spouse caregivers described support from their children as particularly helpful after the death of their loved one with DLB.
Supports employed by caregivers in the end-of-life period
While the caregiving role and period surrounding the death of the individual with DLB were universally challenging, participants described strategies that helped through this period and afterward: using paid and unpaid assistance, widely available resources such as support groups, making memories, and individualized approaches (e.g., finding value in helping others) (Figure 1). Helpful supports for caregivers at the end-of-life care in dementia with Lewy bodies.
Discussion
Caregivers as the main drivers of care
Many participants reported that they had to drive care for the individual with DLB, from making the diagnosis to directing and checking medical decisions. While interviews focused on the end-of-life period, caregivers emphasized how experiences throughout the disease course affected the end of life. Underpinning the caregivers’ need to drive their relatives’ care was the sense that HCPs were uneducated regarding DLB and provided insufficient guidance for caregivers. This is consistent with experiences described in end-of-life care in dementia more broadly, where insufficient HCP knowledge is a reported barrier to quality care in general (Sanders et al., 2008) and at the end-of-life (Kupeli et al., 2016; Torke et al., 2010). Dementia caregivers report distrust in HCPs’ dementia knowledge and having to make uniformed choices due to lack of support (Sellars et al., 2019). Dementia caregivers desire education, connection to resources, and a caring and compassionate presence to help improve the end-of-life experience (Hovland, 2019).
Concerns regarding HCP knowledge may be heightened in DLB compared to other dementias as DLB diagnoses are commonly delayed or missed (Galvin et al., 2010b; Thomas et al., 2017). Additionally, DLB-specific concerns, such as hypersensitivity to antipsychotic medications (McKeith et al., 1992; McKeith et al., 2017), force caregivers to maintain heightened alertness for potentially inappropriate prescribing practices. Current study findings suggest this was true throughout the disease course including end of life, potentially resulting in increased caregiver burden entering the end-of-life period. Furthermore, caregivers described a continued need to drive care at end of life, from requesting hospice to making sure that antipsychotics were avoided. Because caregivers saw themselves as the main drivers of care, mistakes (e.g., antipsychotic administration) led to heightened regret. These findings reveal a critical need for improved HCP education regarding DLB and increased caregiver support as many caregivers may not be receiving sufficient support and education from the medical team.
Impact of DLB features on end-of-life experiences
Additionally, DLB-specific clinical features affected caregiver-described end-of-life experiences. Prior research identified that behavioral symptoms including hallucinations and delusions are major contributors to caregiver burden in DLB (Lee et al., 2013; Svendsboe et al., 2016) and dementia generally (Cheng, 2017; Chiao et al., 2015). Fluctuations and physical limitations contributing to impaired activities of daily living also contribute to DLB caregiver burden (Lee et al., 2013; Svendsboe et al., 2016). In the current study, caregivers reported that behavioral symptoms, fluctuations, and physical limitations contributed to their caregiver burden and these symptoms often worsened toward the end of life. It is thus likely that caregiver strain is more common and higher in the end-of-life period of individuals with DLB, consistent with research in dementia generally showing that the odds of high caregiver strain are nearly twice as high at end of life than in earlier dementia stages (35.0% versus 15.4%) (Vick et al., 2019).
Experiences relating to the caregiving role
Participants reported stressors relating to work, finances, lack of sleep, being overwhelmed, physical demands, family challenges, and needs for increased support, consistent with available literature. Financial costs contribute to the burden of family caregivers of older adults (Lai, 2012) and financial issues and the intersection of work and caregiving affect caregiver perspectives on the sustainability of informal caregiving for individuals with dementia (Singh et al., 2015). Caregivers of individuals with dementia have less and worse sleep than age-matched controls (Gao, Chapagain, & Scullin, 2019) and poor sleep is associated with higher degrees of caregiver burden in dementia (Peng, Lorenz, & Chang, 2019). Exhaustion was also a theme reported with end-of-life dementia caregiving in prior interviews (Peacock, Duggleby, & Koop, 2014). Family tensions can interfere with positive end-of-life experiences in dementia (Peacock et al., 2014) and needing increased support is a common theme in research with dementia caregivers in the end-of-life period (Hovland, 2019; Kupeli et al., 2016; McCabe, You, & Tatangelo, 2016; Peacock, 2013).
Participants frequently described regret and guilt regarding their reactions during caregiving or decisions made toward the end of life. Guilt regarding interactions with a loved one with dementia and caregiving decisions is a known contributor to pre-death grief in caregivers of individuals with dementia (Sanders et al., 2008). Burden and guilt from earlier stages of dementia caregiving can carry over into end-of-life care (Peacock, 2013). Caregiver feelings of guilt can persist years after the death of the person with dementia (Corey & McCurry, 2018), which is similar to the current study. This is particularly concerning as doubts and regrets about end-of-life decisions impact caregivers’ abilities to successfully grieve and adjust over months to years (Harrop et al., 2016).
Death and post-death experiences and supports employed by caregivers in the end-of-life period
Many participants described a need for more education regarding what to expect at the end of life. Knowing what to expect is an unmet need described by caregivers in various dementias (Galvin et al., 2010a; Hennings, Froggatt, & Keady, 2010; Jennings et al., 2015; McCabe et al., 2016) including specific needs regarding what to expect at the end of life (Hennings et al., 2010; Hovland, 2019). Bereaved caregivers outside dementia also report needing improved education and communication regarding the end-of-life process (Harrop et al., 2016). Participant experiences were consistent with prior research describing caregiver pain from unreconciled relationships at the end of life (Peacock et al., 2014), abrupt loss of caregiver support after the death of their loved one (Harrop et al., 2016), and declining caregiver health after the death of the individual with dementia (Corey & McCurry, 2018). In this study, caregivers depended on paid and unpaid support, similar to prior studies (Peacock et al., 2014; Peacock, 2013; Sanders et al., 2008). Multiple participants reported helping others as one method of coping. This approach was also described by other former dementia caregivers (Corey & McCurry, 2018), perhaps as a way to find meaning or a “silver lining” from their own experiences (Durepos et al., 2019).
Summary of new findings
This is the first study to investigate the caregiver experience of end of life in DLB, a dementia with unique symptoms that affect end-of-life experiences. The experiences of informal caregivers of individuals with DLB were often consistent with experiences of caregivers of individuals with dementia more generally, as outlined above. However, study findings highlight several issues that are unique to DLB. These will be critical to address in order to improve end-of-life care for individuals and families living with DLB. Caregivers described experiences throughout the DLB course affecting the end of life, emphasizing the importance of improved DLB diagnosis and care even before the end-of-life period. Many respondents described that their medical teams lacked knowledge regarding DLB, underscoring a need for improved HCP education. While behavioral symptoms (e.g., hallucinations and delusions) and impaired physical abilities are known drivers of caregiver burden, the impact of these symptoms is likely greater in DLB than other dementias as these are core features experienced by most individuals living with DLB. Better treatments for these symptoms are needed, as is improved support for caregivers dealing with these challenging issues. Lack of knowledge regarding what to expect was commonly reported. Thus, current descriptive findings can be used to counsel other caregivers of individuals with DLB facing the end-of-life period, including topics relating to symptom changes when approaching end of life, varied death experiences, and strategies other caregivers employed to cope and find meaning.
Study limitations
Most participants were spouses and adult daughters, consistent with US dementia caregiver statistics (Chi et al., 2019). Demographics other than gender and role were not collected, a study limitation. Participants were all US-based except one, limiting generalizability to other healthcare systems. Recall bias was minimized by recruiting only individuals whose loved one died in the prior 5 years. It is possible that reported experiences differed between participants at different times since their loved one’s death, but the duration of time between the death and interview was not collected. Participants may have volunteered because of particular experiences or strong views, but identified themes were consistent with prior research.
Future directions
This study provides detailed caregiver accounts that can be used by HCPs to counsel other caregivers facing similar circumstances. Findings highlight a need for improved HCP and caregiver education regarding DLB in general and at the end of life. Future research is needed on optimal strategies to improve HCP and caregiver education, predictors of the end of life in DLB, symptomatic treatments for DLB features affecting quality of life and caregiver burden, and approaches for improving quality end of life in this population.
Conclusion
End-of-life experiences for caregivers of individuals with DLB built on the accumulated burden of the disease course, where caregivers were often responsible for driving DLB care—from making the diagnosis to educating HCPs and double-checking medical decisions. While many end-of-life experiences were consistent with those described more generally (e.g., financial stresses, poor sleep, being overwhelmed, and needing increased education and support), many DLB features specifically affected end-of-life caregiver experiences and contributed to burden. Improving caregiver experiences at the end of life in DLB will require improved diagnosis and care for individuals with DLB and also better strategies for treating behavioral symptoms. More research is needed regarding drivers of quality end of life for individuals with DLB and their families and how these drivers and strategies may differ between dementias.
Supplemental Material
sj-pdf-1-dem-10.1177_14713012211038428 – Supplemental Material for Informal caregiver experiences at the end-of-life of individuals living with dementia with Lewy bodies: An interview study
Supplemental Material, sj-pdf-1-dem-10.1177_14713012211038428 for Informal caregiver experiences at the end-of-life of individuals living with dementia with Lewy bodies: An interview study by Melissa J Armstrong, Slande Alliance, Pamela Corsentino, Angela Lunde and Angela Taylor in Dementia
Supplemental Material
sj-pdf-2-dem-10.1177_14713012211038428 – Supplemental Material for Informal caregiver experiences at the end-of-life of individuals living with dementia with Lewy bodies: An interview study
Supplemental Material, sj-pdf-2-dem-10.1177_14713012211038428 for Informal caregiver experiences at the end-of-life of individuals living with dementia with Lewy bodies: An interview study by Melissa J Armstrong, Slande Alliance, Pamela Corsentino, Angela Lunde and Angela Taylor in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.J. Armstrong: At the time of original submission, M.J. Armstrong was supported by an ARHQ K08 career development award (K08HS24159); received compensation from the AAN for work as an evidence-based medicine methodology consultant and was on the level of evidence editorial board for Neurology® and related publications (uncompensated); received publishing royalties for Parkinson’s Disease: Improving Patient Care (Oxford University Press, 2014); and had received honoraria from Medscape CME. She serves as an investigator for a Lewy Body Dementia Association Research Center of Excellence. At the time of acceptance, M.J. Armstrong was receiving research funding from the National Institute on Aging (R01AG068128, P30AG047266) and the Florida Department of Health (grant 20A08). S. Alliance: Ms Alliance reports no disclosures. P. Corsentino: Ms Corsentino is employed by the Lewy Body Dementia Association. A. Lunde: Ms Lunde reports no disclosures. A. Taylor: Ms Taylor is employed by the Lewy Body Dementia Association.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of Florida Dorothy Mangurian Headquarters for Lewy Dementia and the Raymond E. Kassar Research Fund for Lewy Body Dementia. The donors for these funds had no role in the design, methods, subject recruitment, data collection, analysis, or preparation of the paper. Subjects were recruited through the Lewy Body Dementia Association (LBDA) and two LBDA employees participated in design, analysis, and preparation of the paper.
Ethical approval
The University of Florida Institutional Review Board provided approval (IRB201701657). The study was conducted under a waiver of documentation of informed consent. All participants provided verbal informed consent. Included information, including quotes, was de-identified.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.