
Abstract
Introduction
Most studies of the Latin American immigrant experience and care for relatives living with dementia have been in the United States (US). In the United Kingdom (UK), unlike the US, most Latin Americans are first generation immigrants and are a rapidly increasing population. Therefore, we aimed to explore the UK experiences of Latin Americans caring for a relative with dementia.
Methods
We purposively recruited UK-based Latin American family carers of people with dementia ensuring maximum diversity. We conducted semi-structured qualitative interviews (in English or Spanish) with 11 family carers, stopping recruiting when we reached thematic saturation. We took an inductive thematic analytic approach.
Findings
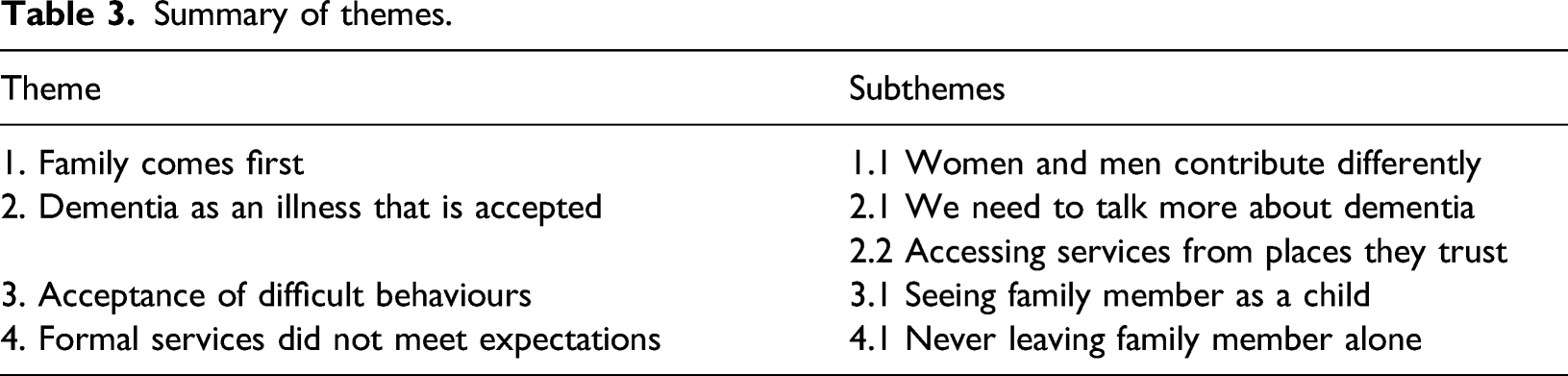
Four main themes were identified: (1) Family comes first, particularly older people, leading to an obligation to care; (2) dementia as an illness that is accepted and talked about, which is regarded as positive with close networks but not wider society; (3) difficult behaviours are not the responsibility of the person with dementia, who is often conceptualised as a child; and (4) caring expectations lead to incompatibility with formal services, and a reluctance to leave people with dementia alone.
Conclusions
Familial obligation is the driver for family carers and acceptance of the illness helped despite adversities. Openness to talk about dementia with close networks was distinctive and helpful, contrasting with wider society, where greater awareness of dementia is needed. Considering the person with dementia as a child did not seem to undermine personhood and enabled maintenance of compassion. The relative with dementia was a priority. There was a lack of culturally and linguistically appropriate services, thus restricting family carers’ ability to fulfil other roles, such as parental.
Keywords
Introduction
In the United Kingdom (UK), there are around 850,000 people living with dementia, a number estimated to reach 2 million by 2050 (Prince et al., 2014) and increasing more quickly among minority ethnic communities (Rees et al., 2012). Although there is little known about Latin Americans living in the UK, studies conducted in the United States (US) show that Latin Americans have higher dementia incidence than non-Hispanic Whites and Asian–Americans, partly because of a higher prevalence of diabetes, hypertension and cardiovascular disease (Alzheimer’s Association, 2018).
In 2013, there were around 250,000 Latin Americans in the UK, 145,000 lived in London, representing the second fastest growing non-EU migrant population in the city (McIlwaine and Bunge, 2016). The majority of Latin Americans in London work in low-skilled jobs despite high education levels, live in inadequate housing and have experienced police harassment, workplace abuse or racism. Nearly a third report very little or no English language, and 20% never having been to a GP (McIlwaine, Cock, & Linneker, 2011). The community is almost invisible in the UK, partly related to lack of official recognition in census and population forms (Mas Giralt & Granada, 2015).
Earlier US-based research found Latin American family carers have higher distress and depressive symptoms than White and other minority ethnic carers (Covinsky et al., 2003; Harwood et al., 1998). It has linked low dementia service use with family values that reject non-familial support, and conceptualised dementia as a normal part of ageing or a disease of ‘crazy’ people rather than a medical condition (Gallagher-Thompson et al., 2003; Neary & Mahoney, 2005). A study assessing public health messages to encourage adult Latin Americans to seek medical advice and detect early dementia for their parents found that the words ‘dementia’ and ‘brain health’ had negative connotations as it related to mental illnesses and thus stigmatised, and was thus stigmatised; causing concerns among participants about their relatives being judged by others as 'crazy' (Balbim et al., 2020). This research also noted the strong cultural expectation of caregiving as a responsibility of women, with participants considering pictures depicting male caregivers as unrealistic and as challenging traditional gender roles.
Although this aligns with the general body of research describing stigma for mental disorders in the Latin American culture (Mascayano et al., 2016; Unger et al., 2012), the experience of providing care once a relative has been diagnosed with dementia may evolve differently. For instance, in a US study, Latin Americans report coping with challenging behaviours by accepting dementia as a disease, demonstrating love, creative problem solving and creating routines (Turner et al., 2015).
Familial interconnectedness, family roles and obligations among Latin Americans caregiving for older relatives have been described under the concept of familismo (John et al., 1997; Losada et al., 2010; Mendez-Luck et al., 2016; Shurgot & Knight, 2004). Familismo, ‘a strong identification and attachment of individuals with their families (nuclear and extended), and powerful feelings of loyalty, reciprocity, and solidarity among members of the same family’ (Sabogal et al., 1987), is relevant to most cultures. In the Latin American culture, it is considered a core value and principle that shapes family and social structures (Fuligni, 2001; Mendez-Luck et al., 2016; Schwartz, 2007). In terms of caregiving, a recent review on Latin Americans caring for a family member with Alzheimer’s disease found that for some these strong family bonds facilitate caring and are associated with less burden (Gelman, 2014; Losada et al., 2010; Shurgot & Knight, 2004), whilst for others familismo has no impact on the caregiving decision or experience (Gelman, 2014), and for others is associated with frustration, guilt, and distress (Gelman, 2014; Losada et al., 2010; Mendez-Luck et al., 2016). In this last group, family carers were often reluctant to provide care and felt obligated due to familismo, perceived a lack of support from social and family networks, or resented cultural depictions of family caring as mostly positive. All these US-based studies exhibit the varied interplay between familismo and caregiving experience and outcomes with family members with dementia.
On the other hand, research on minority ethnic families caring for relatives living with dementia in the UK has focused on Black Caribbean and South Asian carers (Berwald et al., 2016; Cook et al., 2019; Lawrence et al., 2008; Mukadam et al., 2011, 2019), while most studies on Latin American family carers have been in the US, with carers whose experiences may differ from UK-based Latin American carers. Key differences include the relative invisibility of the UK Latin American population, different health and social care systems (McIlwaine et al., 2011); and the UK Latin American population mostly being first generation immigrants (85%) whereas most are native born in the US (McIlwaine et al., 2011; Trevelyan et al., 2016). Native born Latin Americans in the US are more acculturated than their first generation counterparts and have lower familial connectedness and parental respect (Abraído-Lanza et al., 2016; Pew Research Center, 2013).
One of the few studies of Latin American families in London, described Latin American women looking after children, older and ill relatives in confined spaces, whilst also going to work and performing household chores, with restricted, often entirely informal, support (Turcatti, 2021); but this study did not focus upon caring for a relative living with dementia.
We therefore conducted the first UK qualitative study of Latin Americans caring for relatives with dementia. The objectives of this study were to: (1) explore the experiences of family members caring for relatives with dementia and (2) elucidate the needs of this fast-growing community.
Methods
Ethical approval
Ethical approval was sought by submitting a non-substantial amendment to a study interviewing minority ethnic carers of someone living with dementia in the UK. This was approved by the Health Research Authority Research Ethics Committee (IRAS ID 234808) in December 2018.
Participants
Eligible participants self-identified as Latin American, lived in the UK, spoke either Spanish, Portuguese or English; and were currently caring for a relative with dementia or had previously done so. Participants were purposively recruited to ensure variation in age, nationality, gender, educational, occupational and marital status; relationship to care recipient and care recipient’s gender.
Recruitment and setting
Participants were recruited through either. (1) Facebook posts about the study on groups created for Latin Americans living in the UK. (2) Approaching community groups for Latin Americans in London who shared information about the study via social media and their news boards. To facilitate recruitment and engagement, two centre managers invited
(deleted for blinded review) to provide an information session on dementia to service users. (deleted for blinded review) visited both sites a few times to meet service users and delivered a psychoeducation session in Spanish on dementia.
Data collection
Participants who expressed interest in participating were given a Participant Information Sheet in Spanish or English, according to their preference. Participants had the option of being interviewed in either Spanish, Portuguese or English at a time and place of their convenience. Interviews were conducted according to participants’ preference, in their homes, the Latin American community groups from which they were recruited, or in the University offices. On the day of the interview, all participants gave written, informed consent, and filled out a demographic questionnaire.
Initially, the main aim of the interviews was to capture Latin Americans views on caring for someone with dementia to guide changes and cultural adaptations in the START intervention, a manual that supports the wellbeing of family members of someone with dementia (Livingston et al., 2014). The topic guide initially included an explanation of the programme and a summary of each session, questions regarding participants’ caring experience, the professional and non-professional support used to aid in this role, their opinion on START and ideas on how to make it fit the needs of their community (see Supplementary Appendix 1). It was created from a previous study assessing START with family carers of relatives with dementia from South Asian communities and based on the literature about minority ethnic groups experiences in the UK in caring for relatives with dementia.
After the first two interviews, the authors changed the interview schedule, incorporating emerging themes from interviews and checking that the questions made sense to the participants when interviewed in Spanish, as part of an ongoing reflective process based upon both the emerging perspectives of the participants and the interviewer (Agee, 2009). By this point it was clear that participants were overall content with START and did not have many comments on the programme but wished to discuss their general experience of caring and barriers and challenges more broadly. The topic guide was amended accordingly. Questions on START were reduced, and additional questions were added reflecting emerging themes on gender differences in roles and family importance.
(deleted for blinded review), speaks Spanish and conducted all interviews and audio recorded them. (deleted for blinded review) transcribed and translated 10 interviews, into English. One performed in English was professionally transcribed. All data was entered into NVivo software 11. As in previous recommendations for qualitative research with immigrants from Latin American (Lopez, Figueroa, Connor, and Maliski, 2008), participants were given the option to interview in their native language with a bilingual/bicultural interviewer who was knowledgeable on the topic of investigation, and who could then carry out translations according to the meaning they would have in its respective region and context. However, (deleted for blinded review) was the only Spanish-speaker researcher, so we were not able to verify translations with another bilingual researcher, as recommended.
Data analysis
The analysis followed an inductive thematic analysis approach according to the steps identified by Braun & Clarke (2006). (deleted for blinded review) familiarized herself with the interviews. The initial five transcripts were then independently coded by (deleted for blinded review), (deleted for blinded review) and (deleted for blinded review), to identify potential themes corresponding to the research questions. Consequently, (deleted for blinded review) developed a coding framework that was further revised by (deleted for blinded review) and (deleted for blinded review). (deleted for blinded review) independently coded the remaining six transcripts with the finalised coding framework in mind, adding new codes when data did not fit within existing codes. (deleted for blinded review) did the same. (deleted for blinded review) and (deleted for blinded review) met to resolve discrepancies on data interpretation. We ceased interviews at thematic saturation, when neither of the researchers coding interviews identified new codes and when the authors’ reflections on additional interviews resulted in no further emergent themes. We sought respondent validation by sending participants summaries of the findings, allowing them to comment on the accuracy and credibility of interpretations (Mays & Pope, 2000). We did not receive any response from this process to alter findings or interpretations.
Findings
Participants
15 family carers were invited to participate in the study and 11 were interviewed (73.3% response rate). Reasons for not participating were: not having time (n = 2), not being able to travel to London (n = 1), and no longer being interested (n = 1). Most participants (n = 10) decided to be interviewed in Spanish, despite some reporting understanding and speaking English well (n = 7). Interviews lasted an average of 98 minutes (range 56–116).
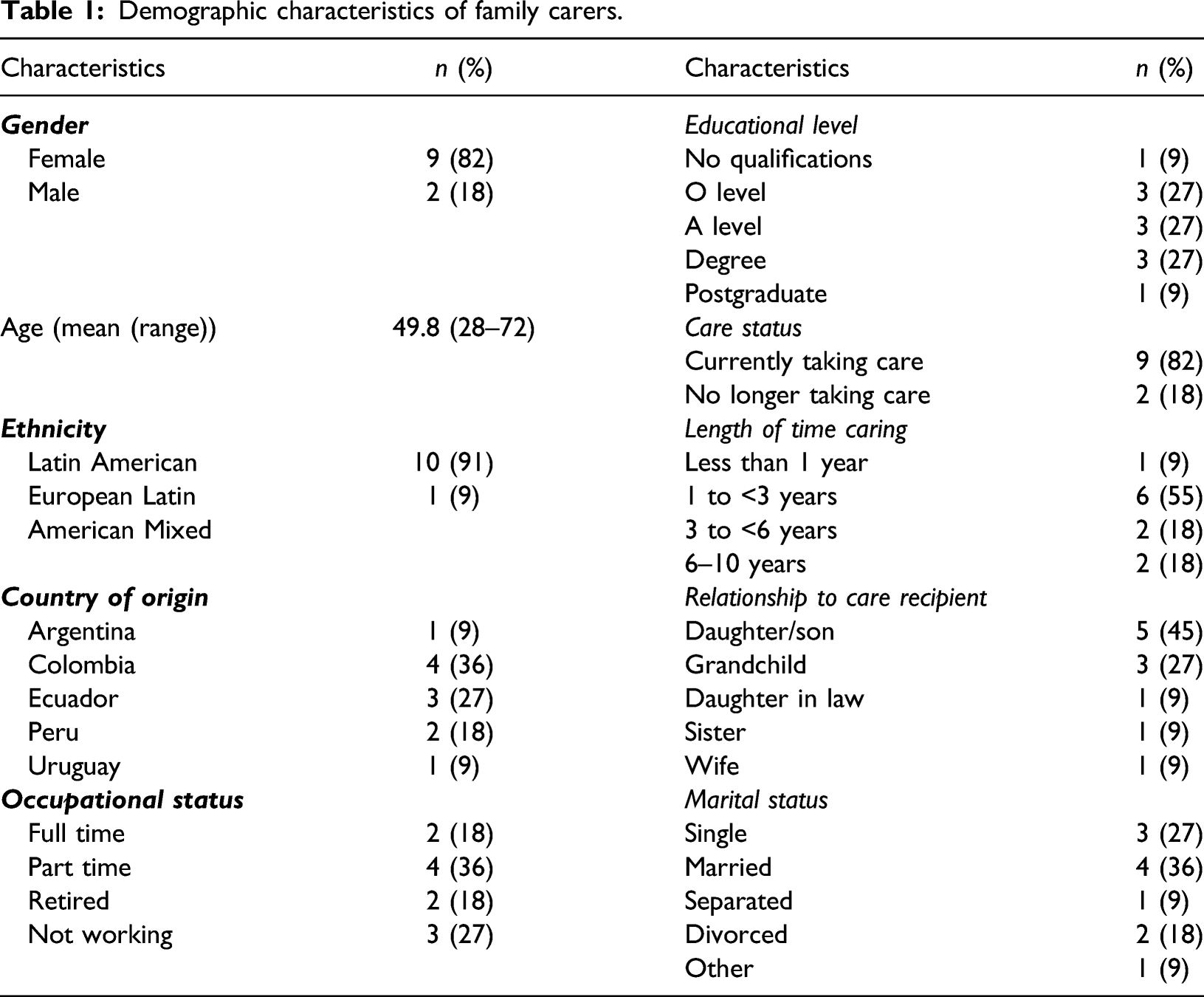
Demographic characteristics of family carers.
Demographic characteristics of relative with dementia.
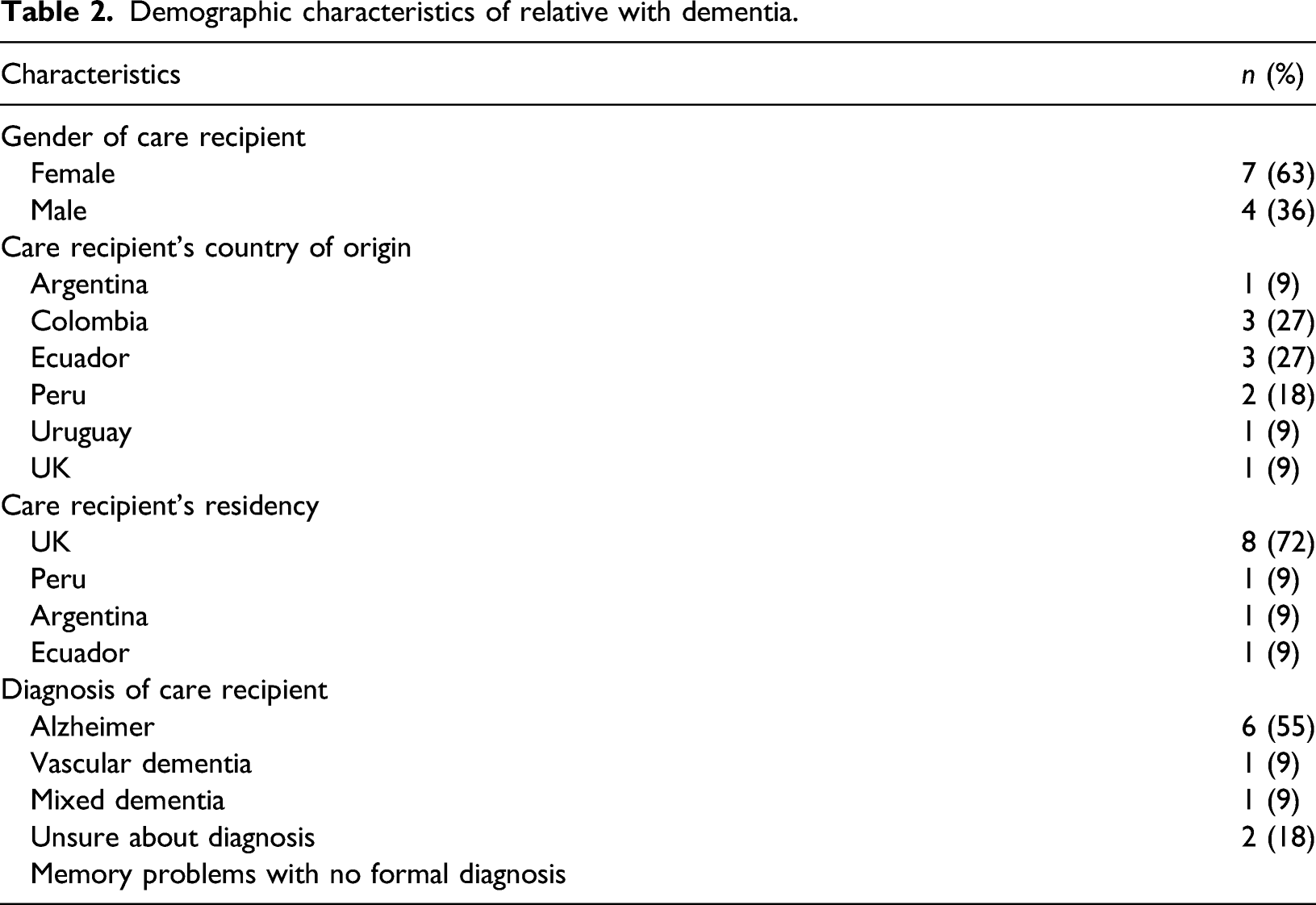
Most participants were female (n = 9) taking care of a female with dementia (n = 7) who resided in the UK (n= 7). Two were delivering care by going back to their countries for months at a time, and around half (n= 6) lived with relatives with dementia in the UK.
Critical reflection
As someone born and raised in Latin America, who has looked after someone with dementia and finds herself adapting daily to a different environment away from home, I could not help but find similarities between my experience and study participants. I consider the roots of my culture to be deep in my nature, and thus was highly interested in the topic of investigation. This undoubtedly impacted on the discussions I had with participants and my views on what they shared. For this reason, perspectives from individuals from different backgrounds, such as other authors and reviewers were crucial to develop a richer understanding of the data, which enabled to reflect upon how my own position and perspective was influencing the analysis. Furthermore, by joining the group and engaging in informal conversations, I was able to build trust with Latin American carers in a way that a non-Latin American researcher may not have been able to.
Qualitative findings
Summary of themes.
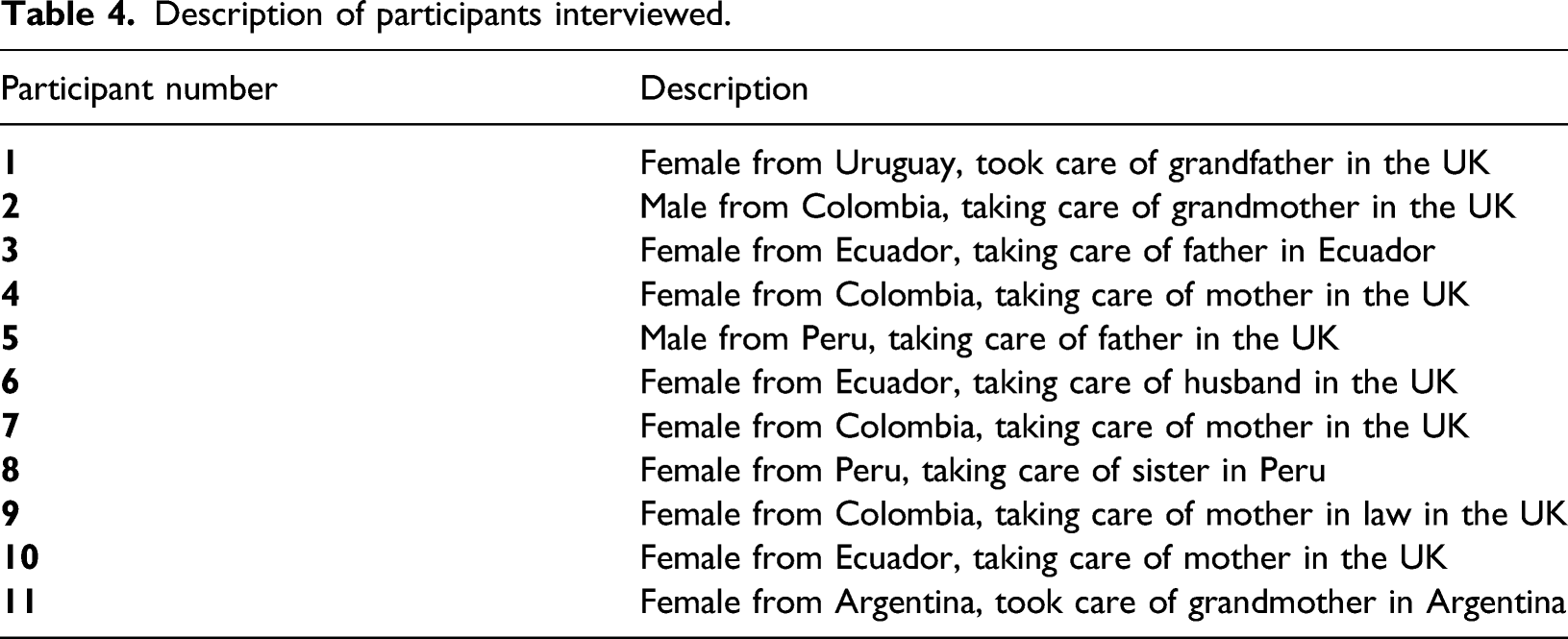
Description of participants interviewed.
Theme 1: Family comes first
All participants highlighted the central importance of family in Latin American culture, contrasting this with British culture, where they perceived family was less central. “We put a lot of emphasis in family. There is another culture here. My husband is British, and I see things [in his family] I wouldn’t if he were Latin American.” (participant 1)
This not only involved immediate family members but also extended family, including relatives living in South American countries who were a source of emotional support for UK-based carers. “The main thing for us is family, it’s more important than other cultures might consider, e.g., I have a lot of English friends [who say]: my God, you’re so close with your cousins, I barely know mine.” (participant 2)
Taking care of relatives with dementia was often seen as a filial obligation that should not fall exclusively to one person but was shared between family members, although most noted that some members contribute more than others. “We are nine. Not all of them can help because not all are economically stable, but they […] spend the night there, one day, one night, we take turns.” (participant 3)
This not only involved caring for relatives with dementia, but also each other. Here, participants reflected on the importance of supporting relatives to take a break from caring. As such, they expressed contempt and judged negatively those who did not contribute to the same extent as them, both in their families and society. “The person in charge also deserves to make their own life. That depends on other family members, they should be looking out so that she can have her life, not only be locked in with mom” (participant 4) “I think my brothers have some type of mental problem. They are not crazy, they work and such, but totally uninvolved. They are not like us, who say our parents are sick, we have to hire a cook, pay [for] their flat.” (participant 5)
This strong family duty meant family members with previous poor relationships with relatives with dementia also provided care. Sometimes, this provided new perspectives on past memories and resulted in positive changes in relationships. “I resented him […] but, as a result of the disease, I’ve focused on him more, I understand more. I see how he loves us. It [caring] has helped me.” (participant 5)
Beyond the shared perception of caring for a relative as an obligation, caregiving was also motivated by feelings of appreciation. In this way, it was described as a duty made from a place of love. “It’s always an obligation. I don’t see how after everything my grandma has done for me and the way she has cared and loved me [...] if I have the opportunity, literally, I can’t even put into words how insane I find it not to be able to help her. But it needs to come from you.” (participant 2)
1.1 Women and men contribute differently
Certain aspects of caring were felt to be more often and more appropriately carried out by women. “It will be the wife or the daughter, because that is how it is. The caregivers are women.” (participant 1)
This was especially true for personal care and cooking. Men were considered (by women) as incapable of performing these, as they lacked the right strategies and emotional characteristics. “My brothers are not skilled for that [personal care]. My father does not want to, and they have no patience. They don’t know how to tell him; they don’t have the strategy. Women do.” (participant 3) “[For caring] a man needs to be loving, patient. Women too, but men are rougher in that sense.” (participant 6)
Nevertheless, involvement from male family members in other practical aspects was still important, such as taking them to appointments, providing economic support and companionship. “House chores have unfortunately always fallen in hands of the girls. I was in charge of taking them to the hospital […], taking them for a walk or coffee.” (participant 5)
This gender difference may be changing for younger generations. As one participant mentioned, his son would not hesitate to provide care for his grandmother, but other family members believed this should not be his job. “I told him, it is very hard because your uncles are going to say things about your grandma. And he says, ‘Mom I am not hurt by doing these doings for my grandma, did not she clean my butt when I was young?” (participant 7)
Theme 2: Dementia as an illness that is accepted
Within families and close networks, dementia was not seen as an illness that needs to be concealed nor as carrying shame or embarrassment. However, the same level of understanding was not described with other members of society, where participants felt greater dementia awareness is needed. “Close and extended family knew. […] I do not think the disease is a taboo” (participant 1)
Disclosing diagnosis to family members, friends or neighbours was considered beneficial, since it helped others understand and not judge relatives with dementia and meant the relatives received more love and attention. “They all [neighbours] know my father has dementia. They know it is not on purpose if he goes and pees somewhere.” (participant 3) “In Peru all the family knows. A lot of affection [as a result].” (participant 8)
However, for one family disclosing the diagnosis led to their relative with dementia’s acquaintances avoiding them. “People take these things […] like they are going to catch it or something. People isolate. They feel worse than us. Friends are apprehensive about visiting her.” (participant 7)
Furthermore, disclosing diagnosis elicited empathy for carers. Participants considered this a positive source of support, as it encouraged others to share their experiences. “Is good to talk about it because then they tell you ‘oh, I went through that situation’ and you learn.” (participant 3) “When you say it, others feel empathy for you, you tend to feel a little more solidarity.” (participant 5)
2.1 We need to talk more about dementia
Even though there was little stigma about disclosing the diagnosis, this did not equate to an understanding of the disease. A participant reflected on the lack of knowledge about what dementia entails and stated that disclosing the presence of the illness mainly elicits pity but not real conversations on the topic. “It’s a bit annoying when people are like, ahh. What’s ahh? Do you understand what it is? People find it difficult to have conversations about serious subjects like that.” (participant 2)
This was also reflected by family carers hoping conversations around dementia would be more open in the community, and they wished to educate and raise awareness in society about it and about the behaviours that can be part of the symptoms. “People get angry because they [relatives with dementia] say things, offensive, or incoherent. [workshops about dementia] for people to understand that this is something that could happen to all of us.” (participant 4)
2.2 Accessing services from places they trust
Lack of stigma did not equate with ease in accessing help from formal sources. Participants wanted to hear about dementia services from entities known personally and considered trustworthy, such as Latin American community centres, friends and family. “[Latin Americans] are either very stubborn or too proud to admit they need help and go to a doctor about it. But they do go to community centres and [say] ‘look, I need help with this, regarding this.” (participant 2) “[Latin Americans] do know about other institutions, but we don’t really know them. The thing is to know them personally, even just talk to them a bit.” (participant 6)
In the same vein, carers preferred support for themselves to be provided in groups, in order to learn from others and establish lasting, supportive connections. “My intention was to accumulate as much information as I could to help him. […] you only get that with other people’s experiences” (participant 5) “If there is kinship with someone, we can keep chatting and have a friendship outside the group.” (participant 1)
Theme 3: Acceptance of difficult behaviours
Participants used various explanations to explain and therefore accept the behaviours of relatives with dementia, especially those that were challenging or distressing. By understanding that the family member was not to blame for difficult behaviours, these explanations facilitated the caring role. A common strategy mentioned by family carers was relating personality and past experiences to current socially unacceptable behaviours of people with dementia. For example, thinking hiding and hoarding behaviours happen because the person with dementia remembers someone once stole jewellery from them. “She hides everything […] You know what happens? When she got married, she had a [cleaning] lady and one day they saw she was stealing. She never forgot that.” (participant 7)
This was especially true for men who were aggressive. Aggression was assumed to be due the time they lived in, where men being aggressive with women was perceived as normative. “My mother told us that when they lived there [village in home country], it was normal that he hit her, and left her with eye bruises. So, it seems that this comes with his character. I don’t know until what point Alzheimer’s gets combined with that.” (participant 8)
In addition, family members commonly accepted behaviours were a result of dementia. “When youngsters in a soap opera kiss, he gets angry. Maybe that would be his conscious reaction, but no […] these are things that the disease makes them do.” (participant 3)
3.1 Seeing relative as a child
Many participants regarded relatives with dementia as a child, and this increased empathy and understanding. However, there were variations in how this was perceived, for example, one participant described their relative with dementia as being ‘less’ than a child. “It’s hard, sometimes she gets angry and says stuff. […] Now that we know she is like a child we listen and understand her better.” (participant 4) “You teach a child and they keep that in their head. Not her. If you teach her one thing right now, she will forget it one minute later. […] she is going backwards.” (participant 7)
Theme 4: Formal services did not meet expectations
Participants discussed an array of strategies that emphasised unconditional love and acceptance as essential for caring. Using tenderness when dealing with dementia symptoms was a common strategy, especially when challenging behaviours arose. For some participants, this was mediated by seeing relative with dementia as a child. “When I took her to bed, she told me ‘I am very afraid, I have a lot of fear’. I hugged her, we sang, prayed, and then she fell asleep.” (participant 9) “If you come close, he starts kicking you. We have to treat him with a lot of love. We all know that if you talk with him fondly and give him kisses, with patience [he calms down].” (participant 5) “I still speak to her as an adult. I’ve always been really affectionate with her, but now I treat her like she’s my baby.” (participant 2)
Formal sources of support that did not provide similar tenderness and commitment were perceived as unhelpful, resulting in perceived incompatibilities with formal services. “We were paying a lady to come 5 hours every day while me and my son were at work, but she was ... cold. She went to do the things she was supposed to do. My mother was next to her and she did not talk to her or anything.” (participant 7) “What I needed [from paid carer] was her help, for her to be with my mother, to take her out for a walk, to talk to her […] Being loving, that’s what matters the most [for paid care].” (participant 10) This was not only about relatives with dementia, but also about what they would expect for themselves. Importantly, they felt these emotional characteristics were inherent to their Latin American culture. “A soft person, normal, familiar, […] so that people [carers] feel better and can express everything.” (participant 6) “Latinos are more familial, sentimental. We [want] someone who understands family is important to you that is more about emotions and love […] so that they are not so cold” (participant 11)
4.1 Never leaving family member alone
Since participants found it difficult to find culturally appropriate services, intensive care was undertaken solely by family. Most also interpreted good care as being with relatives with dementia at all times, which often related to thinking of them as children. This was also associated with being unable to leave them with services which were not appropriate due to language barriers. “[relatives with dementia] are children, they need you there, you cannot leave them, not even for one minute.” (participant 9) “I know there are programs, but my mother doesn’t speak English, so I have to be there with her.” (participant 10) This intensive care often meant family carers curtailed their other roles since the relative with dementia was their priority. “I try to go out with her, to do everything for her. Sometimes my children miss me because they say I spend more time with their grandmother than with them […] We do not have time anymore [with husband], because if I go somewhere, I go with her.” (participant 10)
Discussion
Main findings
This was the first qualitative study exploring the experiences of Latin American families in the UK caring for family members with dementia. Four overarching themes were described, which included: family importance; dementia as an illness that is accepted; not blaming relative with dementia for difficult behaviours, often due to seeing them as children; and expectations from caring that do not align with what is provided by formal services.
Similar to previous research on Latin American families in the US (Neary & Mahoney, 2005; Gelman, 2014) and in line with familismo, caring was perceived as a natural extension of family responsibilities and an act of reciprocity to be shared by many family members and not just one person. As such, participants negatively judged those who did not get involved, although expected responsibilities varied. For instance, there was a reluctance to let men perform certain aspects of caring, as women believed they did not possess the emotional requirements to engage in these activities.
Caring as a familial responsibility has also been observed with other minority groups in the UK, and linked with burden and help-seeking barriers, since using formal services is considered a failure to fulfil familial responsibilities and disrespectful to relatives with dementia’s autonomy or intrusive (Johl et al., 2016; Mukadam et al., 2011). In this study, barriers to accessing services came from participant’s view of what caring should be like, which did not align with what formal services offered. This was in part practical, for example, paid carers not speaking the language as their relative with dementia; but also emotional, feeling that paid care workers could not provide the level of compassion and dedication that they were able to give themselves. Narratives reflected a view of caring that involves actively engaging with relatives with dementia and puts high importance on providing unconditional love and acceptance, which was not on only expected from formal sources of support, but also, from informal networks.
This view also influenced their openness in discussing dementia with others, although these conversations were most helpful within family and close networks, who were more understanding of the relative with dementia and supportive towards caregivers. With acquaintances and others, however, such level of support was not always present; hence, they wished wider education about dementia in society. The relevance of perceived support from others aligns with previous research on factors that influence caregiving among Latin Americans (Gelman et al., 2014); and here extends to how is also perceived as essential for the wellbeing of the relative with dementia.
Willingness to disclose dementia diagnosis and talk about it differed from Latin Americans interviewed in the US (Balbim et al. 2020; Herrmann et al., 2018), and other ME groups in the UK, where family carers are ashamed of the condition, attempt to hide it from others, or only disclose diagnosis with immediate family members (Kenning et al., 2017; Mukadam et al., 2011). Stigma has been associated with lack of knowledge about dementia (Laditka et al., 2013), belief that behaviours are done on purpose (La Fontaine et al., 2007) and blaming the person for the disease (Mukadam & Livingston, 2012). Latin Americans from this study made an effort not to blame the person for the illness and its consequences through several routes, for example, attributing non-socially accepted behaviours to dementia, past experiences or seeing relatives with dementia as children.
Many participants explicitly spoke about seeing their adult relatives as children. Kitwood (1997) coined the term malignant social psychology to practices that devalue and undermine personhood of people living with dementia, such as treating them like children. Previous research shows that infantilization for a person living with dementia is related to limited privacy, social contact and freedom of choices (Liou & Jarrott, 2013). A key distinction here may be between seeing relatives as children versus treating them like one. It seemed participants felt that this approach to their relative did not undermine personhood and actually enable them to maintain a compassionate position; while still speaking to them as adults, engaging them in activities they enjoyed, maintaining their social interactions and giving them choices. Beyond such narratives, we do not know how this infantilization was carried out in practice, or how it was experienced by the people living with dementia themselves, and so it does not constitute a practice we advocate for.
Family members acknowledged caregiving was demanding and valued respite, but since they did not perceive services as fulfilling the relative with dementia’s needs, they did not use them. Thus, the role was intensive and affected other relationships, such as with spouses and children, as the carer often put the person with dementia’s needs before their partner’s and children’s needs.
Overall, this adds to the body of literature that has mainly been conducted in US and relates elements of familismo in Latin Americans with an array of negative and positive consequences of prioritising an ill family member and having high caring expectations (Gelman, 2014; Flores et al., 2009). In this way, findings expand on the complex way care is perceived and performed among immigrants juggling cultural and social expectations based on familial values that act as both barriers and facilitators.
Clinical implications and future directions
Previous research has documented low utilisation of health and social services among Latin Americans in the UK due to previous poor experiences and lack of information (Healthwatch Southwark and LAWRS, 2014). Here, participants were aware of programs available but there was an uncertainty (in some cases motivated by previous experiences) of whether these will assimilate the type of care they were providing. Family members welcomed culturally appropriate help from formal services in line with other UK minority ethnic groups (Herat-Gunaratne et al., 2019; Lawrence et al. 2008). This meant care that was patient, loving and engaging. This is what services should be for all groups but is often not. It is also important to take into account the centrality family members gave to the person with dementia. Services that emphasise the benefits respite care has for the person with dementia may be more appealing and acceptable (Lawrence et al., 2008). Lastly, formal services may be more likely to be accessed if Latin Americans hear about it from informal networks, such as community leaders and friends, and are offered in group settings.
Strengths and limitations
A main limitation of the study is that all analyses are based on translations verified by one person only. Another bilingual researcher would have improved the quality of the translations. Nevertheless, multiple coders were involved in the analyses, we sought respondent validation, and an iterative process was followed, where co-authors met regularly to discuss and reflect on themes and on the position of the main researcher as the one translating and conducting all interviews. Furthermore, the Spanish interviews and the interviewer’s Latin American background may have helped to create rapport and reduced barrier to discussing experiences, as English may not be the best language for Latin American people to explain their needs, but also created an additional limitation where participants could have felt ambivalent about frankness with a member of their community.
Moreover, we were able to access an under-researched group, documented to mistrust and avoid research involvement (George et al., 2014), and to capture a wide range of experiences by recruiting participants with distinct demographics and caring features. Since studies suggest Latin Americans have restricted access to UK’s health services, recruiting from the community ensured a less biased sample. Nonetheless, four participants attended the workshop provided on dementia, which could have influenced their understanding of the condition, although attitudes discussed included time since diagnosis, which often dated years back. Furthermore, four women had worked with older people, so they may be more familiar with the illness and thus better equipped at understanding the illness and handling symptoms.
Conclusion
In this study, we were able to expand upon themes known to be characteristic of Latin Americans and some other minority groups, such as seeing caring as a natural extension of family responsibilities, and a duty of all family members, especially women. Moreover, we found that accepting and loving relatives with dementia was of significant importance and acted as a barrier to accessing services which were seen as not providing tenderness and love. This type of caring was often facilitated by seeing people living with dementia as children and led to being able to talk openly about dementia with their community.
Family importance and lack of culturally appropriate services, resulted in intensive care, where relative with dementia was prioritised over children and partner’s needs and never left alone. Interventions and services for this group should meet Latin American’s for emotional support over practical aspects of caring.
Supplemental Material
sj-pdf-1-dem-10.1177_14713012221076954 – Supplemental Material for Experience of UK Latin Americans caring for a relative living with dementia: A qualitative study of family carers
Supplemental Material, sj-pdf-1-dem-10.1177_14713012221076954 for Experience of UK Latin Americans caring for a relative living with dementia: A qualitative study of family carers by Stefanny Guerra, Tiffeny James, Penny Rapaport and Gill Livingston in Dementia.
Footnotes
Acknowledgements
We thank all family carers who participated in this study and the Latin American community centres in London that aided with recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.