
Abstract
Purpose
We examine care partners’ experience of the Maximizing Independence at Home (MIND) intervention, a multicomponent, home-based dementia care coordination program designed to provide high quality, wholistic care coordination for people and families living with dementia. The goal of the study was to understand 1. the unique dementia-related needs of Black care partners and barriers and challenges to caregiving experienced within the Black community, 2. perceived benefits of the MIND program, and 3. ways to improve the program and make it more culturally responsive to the Black community.
Method
We conducted three focus groups totaling 20 care partners of people living with dementia; who participated in the MIND intervention (2014–2019); all Black/African American and English speaking. Verbatim transcriptions were independently analyzed line-by-line by two coders using inductive approaches.
Findings
Participants noted three overarching themes related to dementia care needs and challenges in the Black community: difficulty finding and accessing dementia information and relevant services and supports; familial conflict/lack of sibling and familial support; and lack of effective communication about dementia within Black Communities. Regarding MIND at home program benefits, four themes emerged: 1. perceived to help locate resources (formal and informal); 2. provided care partners an opportunity for socialization and interaction; 3. included comprehensive assessments and helpful linked information; and 4. resulted in a “much needed break for care partners.” Increased diversity of the MIND program personnel, greater clarity and consistency in MIND program promotion, and better communications were themes for how the program could be improved.
Conclusion
Care partners participating in the MIND program perceived common benefits in aspects related to care for the persons living with dementia as well as benefits to themselves, believed the program addressed important challenges and gaps in education, services, and social support, and could be enhanced in its delivery and cultural responsiveness.
Keywords
As the fourth leading cause of death in the older Black population, dementia prevalence in under-resourced communities has become an important public health focus (Olivari et al., 2020). An estimated 6.2 million Americans are currently diagnosed with Alzheimer’s disease and related dementias. That number is expected to increase 6.7% within the next 5 years with Mid-Atlantic and Southern States feeling moderate to high impacts (Alzheimer’s, 2021). Care partners of people living with dementia, for example, unpaid family members, friends, extended relatives are challenged to provide care to multiple persons while also maintaining employment. The impact of caregiving across populations shows varying differences in caregiving prevalence. For instance, when comparing the prevalence of caregiving by race or ethnicity, Black American (20.3%), Hispanic (21%), and Asian (19.7%) populations report more instances than the White population (16.9%), (Friedman et al., 2015). Outcomes of research show that Black Americans tend to provide care to family members with dementia themselves rather than using external sources, even for more demanding caregiving task (Dilworth-Anderson et al., 2002; Schrauf & Iris, 2012). Further, studies report that Black Americans who care for people living with dementia are less likely to utilize opportunities to obtain respite from their responsibilities, have more of a positive attitude toward aspects of providing care than White care partners, and have a more positive approach toward life in general (Parker et al., 2008; Roth et al., 2015). Understanding dementia care and needs, and effective engagement of Black communities in a culturally responsive manner is critical to guide interventions that best support care partners of people living with dementia and ultimately to reduce inequities in health.
Background
One of the most crucial roles of the care partner is to support quality of life for people living with dementia. Those who take on the responsibility of caregiving may be spouses, children, siblings, other family members/friends, and/or even church members, but the role remains demanding and impacts physical and mental health (Mittelman & Bartels, 2014; Wang et al., 2020). In many cases, fulfilling the role as an informal care partner of a person living with dementia is compounded with additional job demands outside of the care recipient with an influx of working hours leading to the likelihood of a poorer quality of living (Wang et al., 2020) as well as decrease of work productivity (Fujihara et al., 2019), placing them at a disadvantage when attempting to care for their loved ones and themselves. This form of responsibility overload in conjunction with significant financial strain could also instill in caregivers, increased feelings of role captivity (Liu et al., 2019).
There are supportive care programs for care partners of a person living with dementia; although implementation varies, with services fragmented and often inaccessible (Backhouse et al., 2015). In a meta-analysis of the effectiveness of community-based coordinating interventions, authors reported 14 randomized controlled trials that found positive effects on the behavior of people living with dementia and reduction of care partner’s burden (Backhouse et al., 2017). A more recent systematic review and meta-analysis of non-pharmacological interventions found positive outcomes in psychoeducation (characterized by equipping caregivers with supportive resources, basic coping skills, and psychotherapeutic techniques to improve coping and emotional resilience), with multicomponent interventions supporting the reduction of burden/stress (Cheng et al., 2020). However, other studies report that even though community interventions are prevalent, unmet needs of care partners who provide care to someone living with dementia, continue to exist and may be further exacerbated for Black American care partners (Abramsohn et al., 2019; Black et al., 2019).
While studies have documented commonalities associated with informal caregiving, research specifically centered around interventions to improve outcomes for care partners of those diagnosed with dementia in diverse populations is understudied (Dilworth-Anderson et al. 1999; Navaie-Waliser et al. 2001). A cross-sectional study with a sample of 2241 Black, Hispanic, and White informal care partners’ examined commonalities and differences in challenges and found Black care partners were more likely to provide care of a “higher intensity” while having unmet needs related to care provision (Navaie-Waliser et al., 2001). However, Black care partners are also less likely to report difficulty with providing care, suggesting the need for further understanding of the intricacies in caregiving and the nature of unmet needs. In addition, there is more to learn about barriers to available community programs that support care partners of people living with dementia and influences that simultaneously serve as protective factors.
Non-pharmacological interventions such as community care-coordination programs are shown to delay transition from home and use of institution-based care by supporting the capacity of caregivers to continue to provide care within the home (Olivari et al., 2020; Samus et al., 2017; Tanner et al., 2015). Therefore, it is essential that programs are intentionally curated to educate and address the unique frustrations experienced by informal care partners of people living with dementia in the Black community including barriers to access services and managing care recipient’s behavioral symptoms and functional deterioration (Cheng et al., 2020).
This paper reports the experiences of Black American care partners of people living with dementia and who participated in two concurrent MIND at Home studies to better understand their perspectives of the program and experience of providing dementia care. The National Institute of Aging-funded MIND at Home Randomized Control Trial (RCT) and the Centers for Medicare and Medicaid Health Care Innovation (HCIA) Round II award were completed in the Baltimore Washington Metropolitan areas between 2014 and 2019. The MIND at Home RCT is a trial of a care coordination program testing the effectiveness of a model that assists community-residing elders with cognitive disorders and their caregivers to obtain needed dementia-related care and services. It took place between August 15, 2014 and April 30, 2019. The MIND-HCIA is a round two demonstration project that took place September 1, 2014, through November 30, 2017. Further study details and recruitment methods are described and published elsewhere (Samus et al., 2017, 2018). Additional information of the MIND recruitment and sample is in Appendix A.
Method
Design
Through qualitative focus groups that took place January 2019 through February 2019, researchers sought to gain impressions about 1. the unique dementia-related needs of Black dementia care partners, and barriers or challenges to caregiving experienced within the Black community, 2. perceived benefits of the MIND intervention, and 3. ways to improve the MIND intervention to increase access, delivery, and receptiveness in Black American communities. Investigators used content-coding to explore the nature of these topics.
Participants
Participants consisted of Black care partners who previously agreed to be contacted for future research studies focusing on Alzheimer’s disease and related dementias. These participants were referred form several sources of community-level marketing techniques (e.g., Alzheimer’s Association, AARP Maryland, and community events), and community organization mailings and e-blasts. Inclusion criteria were: 1. current or previous participation in the MIND program; 2. participation for at least six months, 3. the ability to understand and provide informed consent, and 4. a willingness to participate in the focus group for up to 75 min.
Recruitment
A non-probability method of purposive sampling from the two pooled MIND interventions was used to recruit participants. Institutional Review Board approval was obtained from Johns Hopkins School of Medicine prior to focus group data collection. The recruitment pool consisted of previous MIND-RCT and MIND-HCIA participants who live in Maryland, within proximity of study location. An investigator unknown to potential participants contacted participants by phone and mail to ascertain interest in the study. All efforts to contact potential participants were completed by the first author (167 calls made), yielding three focus groups (n = 20). A letter of invitation providing a study brochure and investigator contact information was mailed to potential participants without a valid phone number. A study brochure and copy of the oral informed consent was mailed if an interest was indicated during the investigator-initiated phone call or return contact from the mailed letters of invitation. Reasons for unsuccessful contact with a potential participant included an inactive phone number, no return call from message left, or return mail. Work schedule conflict, lack of transportation, care recipient decline in function, a deceased care recipient, care partner did not wish to participate, or no show on the day of the focus group were reasons for the small sample.
Data collection
Participants in the MIND intervention studies reflected upon their experience of the programs. Information from the MIND study team of experts and literature review influenced development of focus group questions. Focus groups took place either at the location of investigators or at a local community library. Provision was made for transportation fare and parking. All focus groups were facilitated by the first author, (D.S.) who is trained in qualitative methods. Oral informed consent took place at the beginning of each focus group giving participants a second opportunity to ask questions. De-identified participant characteristics collected included age, sex, racial background, education, work-related roles, marital status, and living arrangements. Participant relationship to care recipient was ascertained from previous data captured during the MIND studies. Open-ended questions were used to initiate conversations. Questions included the length of time caring for someone diagnosed with Alzheimer’s Disease and Related Dementias, probing to learn about some of the things that were helpful to the care partner when he/she first learned about the diagnosis. Conversation was guided to include the following questions 1. Please tell us about your greatest concerns or challenges in your current role as a care partner to someone with this diagnosis? 2. What kinds of programs, health care or other resources have you used? (probe: Which were most helpful? Which were least helpful?) 3. What kind of help related to this illness could you really benefit from now)? 4. You all had an experience with the MIND at Home care coordination program. What did you like about the program and how would you suggest the program can be improved? 5. As a person of color, do you believe there are any particular challenges or roadblocks that exist that have made it more difficult to receive help or the care you needed for dementia? and 6. In what ways could the providers of the MIND program work to better understand and help persons of color in dealing with dementia? Focus group sessions were audio recorded.
Data analysis
Focus groups ranged from 5 to 7 participants each, lasted approximately 90 min, were digitally recorded and transcribed verbatim by a professional transcriptionist and then reviewed for accuracy and quality by one researcher (D.S.). Three authors, (D.S., M.S., and T.P.) individually reviewed transcripts to become familiar with the data and gain initial impressions. Transcripts were analyzed using an inductive thematic approach (Elo & Kyngäs, 2008). First, transcribed interviews were entered into MAXQDA software to sort and generate codes by two research team members (M.S. and T.P.). Coding discrepancies were identified by a third team member (J.H) discussed and resolved. Members of the research team met multiple times to ensure coding consistency and accuracy prior to generating themes. Emerging domains were shared with the MIND RCT principal investigator Q.S. and team. The team agreed with developed themes.
Findings
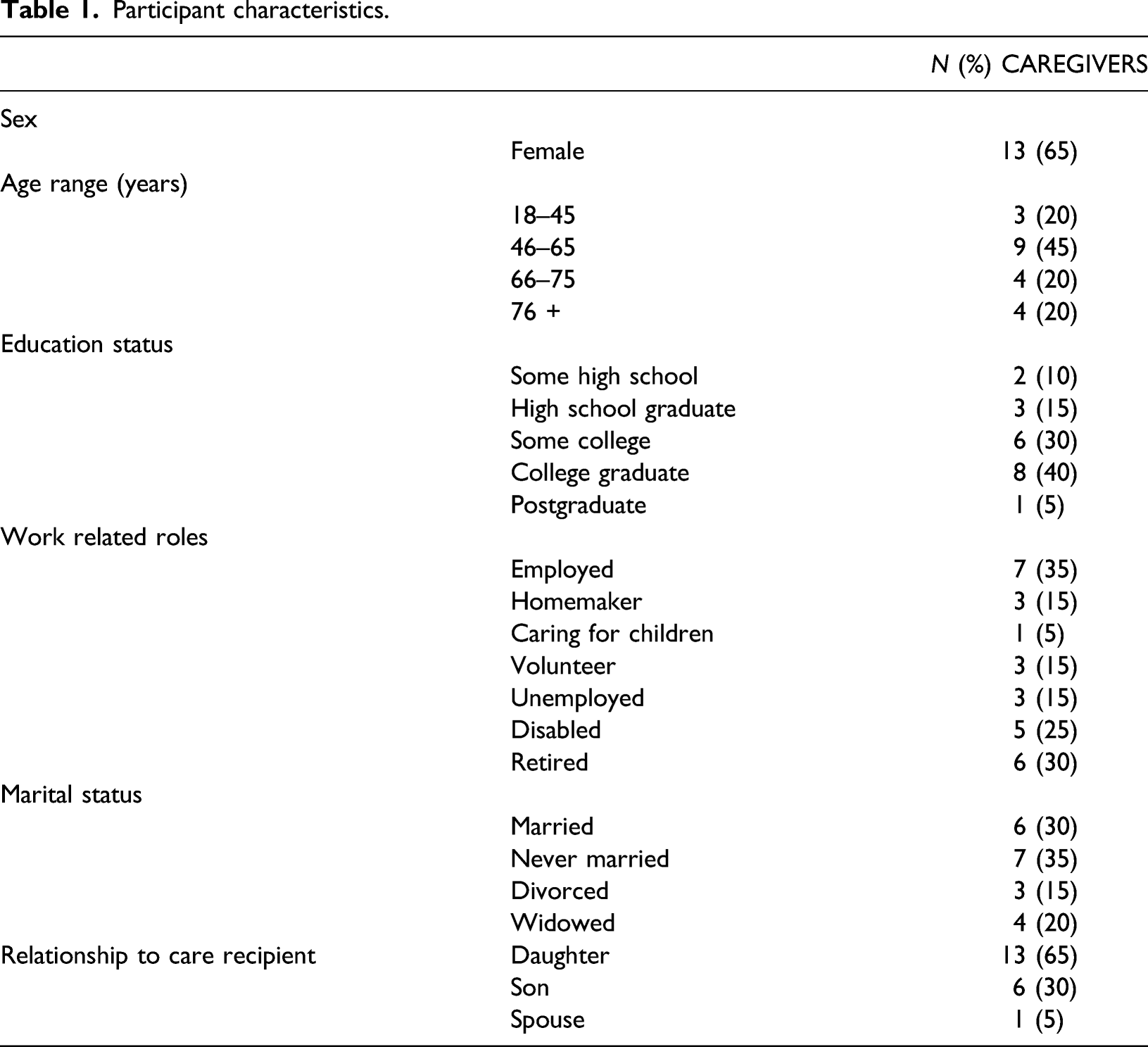
Participant demographics
Participant characteristics.
Thematic findings
Focus group questions.

Categories, themes, and definitions.

Challenges in the BLACK community
“When the dementia really began to be evitable to us, well, I lost all my siblings, except my older sister, who’s not able to do anything to help me because she’s sick herself”
Themes for this category include lack of sibling and other familial support or conflict; communicating with and in Black communities; and obstacles in receiving dementia help or care.
Participants spoke of challenges in caring for their loved one diagnosed with dementia, specifically, the theme of the “lack of sibling and other familial support or conflict” and “not helping with caregiving responsibilities” (11 coded segments). Black care partners feel isolated and alone commenting: That’s the difference between our community and other communities. I notice that when I’ve run into care partners, they’ve got back-up in their family members.” and another “I have four brothers and sisters. I am the youngest, but it’s like I’m the only child.”
The theme, “communicating with and in Black communities” (health providers) exposed the need for understanding, cultural awareness, cultural sensitivity, and respecting cultural and individual beliefs relating to informal care versus formal care of people experiencing dementia, (7 coded segments). “Likely, an important cause of miscommunication,” a participant remarked” they (health care providers) just need to know and understand that not all Black American families are the same…they need to know how to handle situations like a family’s refusal to nursing home admission for their loved ones.”
The group spoke about the lack of understanding of the Black community in general stating: “You’ve got to know our culture.” “If you grew up in a neighborhood that is gated and then you come into a neighborhood that has police on the corner, … or if you have poverty, you’re (health care provider) not going to identify with the things that you need in that community. So, you need to have someone who’s a little more seasoned and can identify. And it doesn’t necessarily have to be race, because you have some that are Caucasian that come from our neighborhoods.”
Participants described, “obstacles in receiving dementia help or care,” a theme with key points relating to discrimination in health care, racial inequities in access to services, mistrust of outside care partners, financial challenges, and geographic limitations (11 coded segments).
Discrimination in health care causes a reluctance to trust health providers in general. “I’ve experienced it with my surgeon who wants to refer to me like I’m a homeboy, I was taken aback by that… he’s not relating to who I am … he’s stereotyping.”
There is the feeling that access to services are limited in comparison to other racial groups. “I work with people whose parents are not Black American and get everything. I mean, pay for nothing, get all services, and with little effort. We have to jump through hoops just to get the few things…”
Inequities in care leads to the perceived worth of Black American people, a sentiment expressed throughout focus groups with responses such as “it is a matter of dignity… it’s not distributed evenly” (care and access). And, although formal help may be available, there’s reluctance due to a lack of trust in formal health providers even if the experiences were not personal; “you know, I’ve never worked in a nursing home, but I knew people that lived in a nursing home and I know how they get treated, like, a piece of dirt off the street.”
Benefits of maximizing independence at home
The category Benefits of MIND at Home includes several themes with key points suggesting things beneficial to the Black community, that is, finding resources, a much needed break, socialization and interaction, and patient assessment & information. Themes of resource system navigation; much needed break; socialization and interaction; and patient assessment & information. “It gave me a lot of leeway and a lot of information to help me get to where I am now.” (MIND at Home) "… you need some time to help navigate through the system (health care system). The system can be very punitive at times. So, the navigation through the system would be another way I found her (MIND staff person) to be helpful.”
There was a feeling that MIND staff helped not only find resources to meet participant needs, but also helped them navigate the system to attain helpful resources and services in addition to providing educational materials, resource referrals, and resource needs assessment (11 coded segments).
Mind at Home staff also shared important information with dementia care partners that other care providers had not offered, including dementia information, treatment, and services (i.e., from doctors/physicians and social services), even conducting research to identify supportive resources for identified needs.
A “much needed break” was how one woman put it; having a MIND staff member visit to coordinate care of their loved one with dementia while also being concerned about the care partner’s needs relieved mental stress and burden of caregiving (11 coded segments). “She (MIND staff), actually would call me to find out what is it this week you need for yourself? How are you feeling this week … and whatever I would share with her or whatever I needed she made provisions so that I could get that. I really enjoyed it and I really admired that because, like you said (referring to another focus group member), it took away a lot of stress.”
Great care was given to the person living with dementia as well. Care partners observed the socialization and the effects of interaction with the program staff on their loved one with dementia. “They (staff) took time and talked with her (care recipient) like a friend, listening to their needs as well as my needs.” “When she came by (MIND staff person), she was able to talk with my mom where my mother understood and had a relationship. Staff help to identify ways for the person living with dementia and CG to interact.
The MIND at Home staff conducted in-home assessments to identify and prioritize unmet needs and opportunities for improvement (9 coded segments). The program provided care coordination and shared information on different types of care options available; staff not only identified unmet needs but gathered information about the dyad’s priorities and concerns then devised a plan to address those concerns pragmatically. “They got to be familiar with who we are,” “I didn’t see any People of Color come to visit my mother. I mean, that might help.”
Improving the maximizing independence at home program
The category improving MIND revealed two key observations (themes) and suggestions that entailed a lack of diversity in the MIND personnel, and consistency in promotion and communication of the MIND program’s availability. Participants sought support from individuals who understood their situations and could identify with the community and unique needs of each family unit within the context of the community. The theme lack of diversity in MIND personnel evolved from focus group participants who gave the recommendation to hire racially diverse staff to serve participants and be able to identify with the community being served. (11 coded segments).
There is a need to identify more effective and consistent strategies for “getting the word out” about MIND at Home in Black communities. Several participants indicated there were inconsistencies in how information about the program was dispersed in Black communities and how people in those communities learned about the program (6 coded segments).
Discussion
With no cure for dementia on the horizon, the number of supportive care programs for dementia care partners is increasing to meet the needs of families who experience dementia. Limitless differences in care partner roles exist based upon competing responsibilities (e.g., work, other sick family members, and children), causing complexities for one program to meet all needs. Moreover, programs are not infiltrating all communities, especially those at higher risk for living with Alzheimer’s Disease and Related Dementias including Black communities, which presents serious threats to the equitable receipt of optimal or even adequate dementia care.
Results from this study of Black care partners who participated the MIND at Home dementia care coordination program underscore three overarching themes related to dementia care needs and challenges in the Black community: difficulty finding and accessing dementia information and relevant services and supports; familial conflict/lack of sibling and familial support; and lack of effective communication about dementia within Black Communities.
Common themes among participants at the conclusion of the focus groups found that providing forms of caregiver respite while granting socialization opportunities to the person living with dementia, suggests that home care coordination programs should be incorporated into standardized dementia care. Equipping care partners with dementia-related information and directing them to helpful resources can be associated with positive and resilient attitudes towards caregiving demands.
These findings support previous studies that have assessed the benefits of home care coordination programs and reported similar findings. An earlier study looking at home-based dementia care as a key component of long-term care also found that caregivers struggle with emotional support and well-being while also seeking to have respite time and more disease education (Samus et al., 2018). Regarding benefits of the program, four themes emerged: the program was perceived to help find resources (formal and informal); provided care partners an opportunity for socialization and interaction; included comprehensive assessments and helpful linked information; and resulted in a “much needed break.” The theme that the program’s focus on identifying and facilitating various forms of caregiver respite while granting socialization opportunities to the person living with dementia, was beneficial to Black care partners, suggests the value of addressing respite and social determinants of health and the need to incorporate this component into standardized dementia assessments, and care planning. Care partners’ comments regarding their dementia-related interactions with other medical providers suggest a need to engage and educate health care providers on working with patients and families surrounding the important issues raised.
Finally, there were two major areas in which Black care partners felt the program could be strengthened, which included: increased diversity of the MIND at Home program and personnel and greater clarity and consistency in MIND program promotion and communications. Study participant preference for greater diversity among MIND at Home personnel supports existent calls for the need culturally tailored intervention strategies (Napoles et al., 2010). Future strategies might include recruiting participants from different settings (e.g., churches or community senior center) or using novel recruitment methods. For example, a recent study used a warm hand-off approach to recruit Black dementia caregivers into a multi-site clinical trial, which involves coordination with multiple research team members and potential participants (Epps et al., 2021). More work is needed to understand best practices for sharing information about the scope of the MIND at Home program, since care partners are often overwhelmed by the number of programs, services, and agencies responsible for supporting care recipients (Washington et al., 2011)
There are several notable limitations to this study. Because study caregivers shared their experience in a focus group format, there may have social pressure that could have biased the discussion. Further, there was likely differing baseline levels of general caregiver knowledge and understanding of dementia and terms used in the focus interview guide. Also, reporting on the experience in the MIND at Home program could have been biased by a temporal lag between actual receipt of the service and the focus group interviews resulting in recall bias (some care partners had graduated from the program nearly 12 months prior to the focus groups). Finally, the sample was generally small and didn’t necessarily represent all segments/subgroups of the Black Community or communities in other states.
It is the hope that these findings will reinforce the provision of long-term care coordination in Black, under-resourced communities to assure that end of life care is supported in both people living with dementia and their caregiver(s), minimizing the risk of costly institutionalization and further familial burden. By doing this, we hope that these findings will frame future clinical and public health initiatives to increase the presence of supportive care coordination programs in under-resourced communities with unique multicultural implications.
In summary, our qualitative study of Black dementia care partners receiving the MIND program found that care partners perceived common benefits in aspects related to care for the people living with dementia as well as benefits to themselves, believed the program addressed important challenges and gaps in education, services, and social support; and could be enhanced in the future in its delivery and cultural responsiveness. It’s also important to note the percentage of men providing care to their mother’s (30%) and spouse (5%). There continues to be a lack of awareness about the male dementia caregiving experience, especially in the Black community. Further research is needed to fully and deeply understand the perceived needs of the Black community, as well as other diverse cultures/races/and ethnicities regarding dementia care, to promote and advance the use of more culturally responsive health care services delivery to reduce inequities.
Footnotes
Author contributions
D.H.S., D.J., and Q.S. planned the study and designed the methodology; D.H.S. completed all focus groups; D.H.S., and Q.S. supervised data analysis; T.P., and M.S. performed data analysis, D.H.S., T.P., M.S., D.J., I.A., M.R., C.F., and Q.S. contributed to data interpretation and themes development; All authors contributed to the preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institute on Aging (R01 AG046274, 08/15/2014-04/30/2019, NCT02396082), administrative supplement 3R01 AG046274-04S1 to Dr Danetta Sloan. The funding source was not involved in the study design, collection, analysis, or interpretation of data, writing of the report or the decision to submit the article for publication.
Ethical approval
This study was approved by the Johns Hopkins School of Medicine IRB#00178052
Comparison of maximizing independence at home (MIND at Home) Studies.
Abbreviations: HCIA–Health Care Innovation Award, CMS–Centers for Medicare and Medicaid, RCT–randomized controlled trial, NIA–National Institute on Aging, LTC–long-term care, PWD–person with dementia, CG–caregiver, EMR–electronic medical record, M–months, BL–baseline, JHU–Johns Hopkins University.
MIND-HCIA (CMS HCIA)
MIND-RCT (NIA)
Primary Aims
Effectiveness on Medicare and Medicaid health care costs. Develop MIND certification program. Develop payment model
Efficacy on time to (LTC) placement, PWD and CG clinical outcomes, cost savings (societal perspective) durability, explore moderators
Project period
2014–2017
2014–2019
Design
Quasi-experimental propensity matched
Single-blind, parallel group RCT
Randomization
None
1:1
Sample n
342 participants received MIND
304 (152 MIND, 152 Augmented usual care)
Recruitment
Broad multipronged community outreach
Broad multipronged community outreach
Main eligibility
- Medicare-Medicaid dual eligible or Medicare only beneficiaries
- Community-living
- All-cause dementia [14]
- 40-mile radius from Johns Hopkins Bayview Medical Center
- A study partner (person who has knowledge of PWD daily living)- Any insurance provider
- Community-living
- All-cause dementia [14]
- 40-mile radius from Johns Hopkins Bayview Medical Center
- Eligible informal caregiver as study partner
Primary outcomes
- Time to LTC placement (18, 24 M) (Minimum Data Set administrative data)
- Cost saving to medicaid and medicare (medicaid and medicare administrative data)
- Program satisfaction (survey)
- Intervention delivery (EMR record)- Time to LTC placement (18 M) (proxy reported)
- Cost benefit (societal perspective, direct and indirect costs) (survey, costs estimated from published rates)
- Intervention delivery (EMR record)
Intervention(s)
MIND at Home-Plus (MIND-P) for all participants
Subset (n = 23, 7%) (high behavioral/safety needs) received supplemental occupational therapist-based activities protocol
Usual careMIND at Home-Streamline (MIND-S) (leaner, more targeted, and efficient protocol adapted from original MIND)
Augmented Usual Care
Data collection
Continuous (non-blinded)
BL, 4.5, 9, 13.5, 18, 24 M (blinded)
Intervention delivery endpoint
Death, a permanent transition LTC setting (e.g., LTC, assisted living), a move outside the area, loss to follow-up, or withdrawal
Death, a permanent transition LTC setting (e.g., LTC, assisted living), a move outside the area, loss to follow-up, or withdrawal
Consent
Consent for claims analysis
Consent for future claims analysis
Key limitations on cost evaluation
Administrative claims data limited to self-monitoring period for HCIA (ended 11/30/2017). JHU has MIND PWD and Match Medicare claims data only through 2016. Medicaid data only through 10/2017. No Medicare Advantage data available
Health care and community service use limited to proxy report data collected every 4.5 months—subject to recall bias and errors in monetizing service costs from national data