
Abstract
Background
Home-based dementia care is common in the Chinese-Australian community. However, dementia education programs for Chinese-Australians in the language of their choice are scarce. The World Health Organization has developed iSupport for Dementia, an online education program for informal caregivers. Cultural adaptation of the program for Chinese-Australian caregivers is an opportunity to address this gap in caregiver support.
Aim
The aims of the study were (1) to understand stakeholders’ perspectives on the cultural and linguistic appropriateness of the Chinese iSupport for Dementia content and design and (2) to explore factors affecting the future implementation of the Chinese iSupport program in Australia.
Methods
A qualitative descriptive design was applied to address the aims of the study. Focus group discussions with Chinese-Australian caregivers and community aged care workers were conducted to collect data. Thematic analysis was used to analyse data.
Results
In total, six focus groups were conducted with 18 Chinese-Australian caregivers and 17 care workers. Six themes were identified and described as follows: (1) appropriateness of the Chinese iSupport content; (2) acceptability of the online Chinese iSupport design; (3) motivations to engage in the iSupport program; (4) desire to interact with peers and professional facilitators; (5) concerns about program accessibility; and (6) the need to extend the iSupport program to care workers.
Conclusions
Engagement with Chinese-Australian caregivers and care workers will inform further revisions of the Chinese iSupport program contents to ensure the program is culturally congruent to Chinese-Australian caregivers. Factors affecting the implementation of the program identified in the study will be considered in the intervention phase of the program.
Keywords
Introduction
Home-based care is common among Chinese diaspora partially due to the strong influence of Confucianism that values relationships and family support, and the care of aged parents or family members (Yiu et al., 2021). Yet, high-level stress in Chinese caregivers has been widely reported, which contributes to poor health and quality of life of the caregivers and those they care for (Liu, 2021; Ma & Saw, 2020). Psychoeducation programs for caregivers are effective in helping them cope with stress, thereby improving their health and wellbeing (Cheng et al., 2020). However, culturally adapted psychoeducation programs for Chinese caregivers in Chinese-minority societies, like Australia and the US, are limited (Ma & Saw, 2020). The World Health Organization (WHO) has developed iSupport for Dementia, an evidence-based online education program for informal caregivers as part of strategies to support the implementation of the WHO Global Action Plan on the Public Health Response to Dementia (World Health Organization, 2021).
Background
In Australia, it is estimated that 487,500 people are living with dementia in 2022 and up to 1.6 million (informal caregivers and care workers) are involved in their care (Dementia Australia, 2022). Chinese-Australians are the largest ethnic minority group in Australia accounting for 1.2 million or 5.6% of the total population (Australian Bureau of Statistics, 2016). There is no information about dementia prevalence in ethnic minority groups in Australia, an indicator of a lack of strategies to address dementia care disparities between people from the mainstream culture and ethnic minority groups (Australian Government and Department of Health, 2017). Most (82%) do not speak English at home, rather Mandarin (46%), Cantonese (22%) and other local dialects (14%) (Australian Bureau of Statistics, 2018). Chinese-Australian caregivers of people with dementia faced greater challenges in managing dementia care at home and experienced more stressors compared to their counterparts from mainstream cultural backgrounds (Leone et al., 2014; Xiao et al., 2013). Factors contributing to their stress include language barriers that significantly limit their ability to navigate, access and utilise dementia care resources and services, and participate in psychoeducation programs provided in English (Brijnath et al., 2021; Leone et al., 2014; Xiao et al., 2013). Moreover, Confucianism has a great influence on Chinese to show filial piety for older people in a family, duty of care for spouses and harmony in a family (Yiu et al., 2021). Chinese caregivers who hold a strong Confucianism belief may perceive that good care is provided by family members. Therefore, they may be less likely to seek help outside of the family (Guo et al., 2019). In addition, migrants usually lose most social networks established prior to migration; therefore, they have limited sources of care in a host country to help them to cope with stress (Brijnath et al., 2021; Meyer et al., 2018).
Inadequate preparation for informal caregivers contributes to high-level caregiver stress and uncontrolled dementia-associated symptoms, high rates of complications and hospital admissions of care recipients (Anderson et al., 2020; Bott et al., 2019). Systematic reviews confirm that psychoeducation interventions for caregivers can develop caregiver self-efficacy, enable them to manage dementia care at home more effectively and significantly reduce caregiver stress and distress (Cheng et al., 2020; Frias et al., 2020). However, psychoeducation programs are predominantly designed for caregivers from the mainstream culture, which significantly affects access and utilisation by ethnic minority groups (Chua & Pachana, 2016; Gallagher-Thompson et al., 2010). Moreover, use of interpreters to translate face-to-face education programs for caregivers is reported in Australia (Leone et al., 2014; Xiao et al., 2013). This approach is viewed as disregarding the cultural adaptation of programs which leads to questionable effectiveness of the program (Bernal & Domenech Rodríguez, 2012b). In addition, relying on interpreters for access to education programs constrains caregivers’ autonomy to direct their own learning and violates adult learning principles (Knowles, 1984). Online psychoeducation improves accessibility for caregivers, especially those living in rural and remote areas where education resources are scarce, and overcomes time constraints for working caregivers (Egan et al., 2018).
WHO iSupport for Dementia is an evidence-based online psychoeducation program which was developed through international collaboration (World Health Organization, 2019). The program was implemented and evaluated in India using an online self-study approach. The outcomes showed a significant effect on caregivers’ person-centred attitude towards people with dementia they cared for; but did not show a significant effect on caregivers’ depression and perceived burden, self-efficacy and mastery (Baruah et al., 2021). In addition, a low recruitment rate (44.67%) and a low retention rate (36.42%) were reported in the India study (Baruah et al., 2021), which might have affected the outcomes. The lessons from India regarding the low recruitment and retention rates were learned in the study on the culturally adapted Chinese iSupport for Dementia in mainland China. Caregivers in the study in mainland China were recruited from hospital memory clinics, received support from a trained program facilitator who was a registered nurse, and were engaged in weekly online chats and monthly online meeting with peers (He, 2022). The 6-month trial demonstrated a significant effect on caregivers’ mental health-related quality of life, self-efficacy, social support, reactions to changed behaviours and a significant effect on the quality of life of people with dementia (He, 2022). These previous studies on iSupport for Dementia indicate the need to undertake the present study to culturally adapt the program to the Chinese-Australian community.
Systematic reviews in healthcare reveal that culturally adapted interventions are more effective than those without cultural adaptation (Hall et al., 2016; Spanhel et al., 2021). Chinese-Australians migrated not only from mainland China but Taiwan, Hong Kong and other regions. Depending on where they migrated from, they use simplified Chinese (mainland China) or traditional Chinese (Taiwan, Hong Kong and Macau) (Australian Bureau of Statistics, 2018). Most importantly, the contextual environment that shapes Chinese-Australian caregivers’ practices in Australia differs from that experienced prior to their migration. In this study we adapted the definition of cultural adaptation of healthcare intervention for an ethnic minority group in a country by Bernal and colleague (Bernal & Domenech Rodríguez, 2012a). We describe the definition as follows: (1) reviewing and revising the intervention program to ensure cultural and linguistic appropriateness for the users and (2) determining implementation strategies to enhance the intervention outcomes of the program. This definition values stakeholders’ lived experiences in dementia care in a socio-cultural context and embraces eliciting their perspectives of the Chinese iSupport program as a prerequisite for cultural adaptation of the program in Australia.
Ecological validity framework to inform the cultural adaptation
The study is embedded within a larger ongoing project that includes the cultural adaptation of Chinese iSupport program in phase one using a qualitative study and an evaluation of the program in phase two using a multicentre randomised controlled trial across six study sites in Australia and Greater China including mainland China (two sites), Taiwan, Hong Kong and Macau. The study protocol for phase two is published elsewhere (Xiao et al. 2022). In this study, we applied the ecological validity framework described by Bernal and Domenech Rodríguez (Bernal & Domenech Rodríguez, 2012a), Durlak and DuPre (2008) and Spanhel et al. (2021) to inform the cultural adaptation of the program. The framework emphasises eight components and we interpret these components as follows: (1) language: ensuring translation accuracy of the original program; (2) persons: identifying informants and stakeholders, engaging them in the program adaptation and eliciting their perspectives on cultural and linguistic appropriateness of the program; (3) metaphors: symbols, sayings and case scenarios used in the program are culturally meaningful for users; (4) content: embedding values, customs and traditions that enhance care; (5) concepts: eliciting stakeholders’ perspectives of implementation strategies or models and embedding these into the intervention protocol to enhance intervention outcomes; (6) goals: co-designing the online program with stakeholders to meet their expectation for a user-friendly program (i.e. easy access and use); (7) methods: developing procedures, guidelines and training activities that support the implementation of culturally and linguistically adapted intervention programs; and (8) social context: considering contextual factors, for example, Chinese-Australian community organisations, ethno-specific care service providers and the social care system in Australia that promote and sustain the program.
Components 1–4 of the ecological validity framework constitute a surface structure of a culturally adapted program which is concerned with language, culture and core content in the program, whilst components 5–8 are viewed as a deep structure that addresses enablers and barriers in program implementation (Durlak & DuPre, 2008; Spanhel et al., 2021). This study is phase one of a large project mainly focused on the surface structure of the Chinese iSupport program. However, factors affecting the deep structure of the intervention phase were also explored. The applications of the eight components of the ecological validity framework are outlined in Table 1). Applications relevant to phase two, a planned randomised controlled trial (RCT), are included in the table, but not detailed in this paper.
Aims
The aims of the study were (1) to understand stakeholders’ perspectives on the cultural and linguistic appropriateness of the Chinese iSupport for Dementia content and design and (2) to explore factors affecting the future implementation of the Chinese iSupport program in Australia.
Method
A qualitative descriptive approach was applied to address the aims of the study (Doyle et al., 2019). This qualitative approach allows researchers to collect data in a naturalistic setting that reflects actual perspectives of participants regarding the proposed culturally adapted Chinese versions of iSupport for Dementia.
Study setting and participants
The study was conducted in an Australian state. Chinese-Australian caregivers were invited to participate in the study if they were (1) 18 years of age or above, (2) a primary caregiver for a person with dementia, (3) in a caregiving role for at least 1 year; and (4) able to comprehend written Chinese as they were required to review and comment on the written format of the Chinese version of the iSupport program. We also invited care workers who provided community-based dementia and aged care services for older Chinese-Australians to the study if they were (1) from a Chinese background and (2) currently employed as a caregiver support group coordinator, social worker or direct care worker in a aged care organisation.
Participants were recruited from a large Chinese ethno-specific aged care organisation that provides care services to older Chinese-Australians. Researchers attended meetings with Chinese caregivers to introduce the study and address any questions or concerns. Hard copies of information packs, including participant information and consent forms in Chinese, were distributed to potential participants during the meetings. Potential participants who were interested in the study contacted a researcher by phone or WeChat, a social media platform used by Chinese, to arrange a face-to-face meeting to discuss informed consent and focus group details. The recruitment process commenced in February 2021 and was completed in April 2021.
Data collection
Focus group discussions were conducted to collect data using a semi-structured discussion guide (see Supplement file). The guide was adapted from a previous study adapting the English version of WHO iSupport program to an Australian socio-cultural context (Xiao, McKechnie, et al., 2021). These questions helped researchers to elicit participants’ perspectives of (1) language, culture and core program content or the surface structure of the program (i.e. question 1–4 for caregivers or question 1–5 for community care workers) and (2) enablers and barriers in program implementation or the deep structure of the program as described in the Ecological Validity Framework (i.e. question 5–10 for caregivers or question 6–11 for community care workers).
Six focus groups were conducted in total, two with caregivers (8–10 participants in each group) and four with care workers (4–5 participants in each group). Focus group discussions with caregivers were held in the seminar room of the ethno-specific aged care organisation and were facilitated by two bilingual and bicultural researchers (LX and MY). Focus group discussions with care workers were conducted in Zoom online meetings held in the evening as this group of participants worked mainly on day shifts and had difficulties attending face-to-face meetings. These focus groups were facilitated by two bilingual and bicultural researchers (LX and YZ). During focus groups, the researchers displayed the test online Chinese iSupport website to demonstrate the program and facilitate discussions. Each focus group discussion was held for approximately 60 minutes.
Prior to focus group discussions, each participant was given 2–3 written learning units from the draft Chinese iSupport manual, either in simplified Chinese or traditional Chinese, to review. They were also asked to reflect on their experience in dementia care and comment regarding the cultural and linguistic appropriateness of iSupport.
Data analysis
Thematic analysis, described by Nowell et al. (Nowell et al., 2017), was applied to the study. Voice data was transcribed verbatim by YZ and MY and verified by LX to ensure transcript accuracy. Two bilingual researchers (LX and MY) read the transcripts several times to become familiarised with participants’ views. Meaningful words were extracted and highlighted from data to generate open codes. The researchers then constantly compared the codes across focus groups to identify clusters of codes based on similarities. The authors identified redundant answers to the interview questions (or data saturation) in the final focus group of each participant group. Regular team meetings were held to elaborate potential themes and sub-themes based on the study aims. Findings with excerpts were translated from Chinese into English by the first author and verified by a team member (LX and YZ).
Ethical consideration
Ethical approval for the project was granted by the Human Research Ethics Committee of Flinders University (Project number: 2782). Researchers discussed the project with each participant and provided sufficient time for them to discuss their participation with family members and friends. Informed consent was signed prior to focus group discussions and document review. Participants were assured of their rights to participate or withdraw from the study. They were also reassured that personally identifying information would remain confidential in any reports of the study.
Study rigour
Strategies were implemented in the current study to ensure credibility, dependability, confirmability and transferability of the qualitative study (Lincoln & Guba, 1985). First, two bilingual researchers (LX and MY), who share the same first language as participants, were the facilitator and observer in focus group discussions. The cultural and linguistic concordance enabled the researchers to build rapport with participants and elicit opinions through interactive dialogues. Focus group discussions were audio recorded and transcribed verbatim for data analysis by two bilingual researchers (MY and AZ) and checked by another bilingual researcher (LX). These processes ensure credibility of data. Second, the bilingual researchers (LX and MY) analysed the data independently. Findings and excerpts were translated into English by MY and checked by LX and YZ. Member checking in the research team was used. All members in the project (all authors listed in this article) were given opportunities to review and comment on the themes and excerpts. Disagreements on the themes were discussed in monthly team meetings or via email communication and were resolved based on data and team consensus. Additionally, data collected from caregivers and aged care workers and the comparisons of findings demonstrated data triangulation. These processes ensure confirmability. Dependability was achieved by adhering to the study design and methods. Transferability was shown by detailed descriptions of sub-themes and themes using excerpts.
Findings
Of 18 Chinese-Australian caregivers and 17 care workers who participated in the study the majority (22 participants or 63%) were from a Mandarin speaking background; 13 participants (37%) were from Cantonese speaking backgrounds. The mean age of Chinese-Australian caregivers was 69 years; 67% were women and 60% were spouses of the person with dementia and 40% were adult child caregivers. The average year in their role as a caregiver was 4 years. The mean age of the person with dementia they cared for was 85 years. The mean age of care workers was 42 years, and 65% were women. Care workers on average had worked in dementia care for 4 years, with 76% holding a diploma in aged care and four had a master’s degree in social work.
We identify six themes from data analysis and described as (1) Appropriateness of the Chinese iSupport content; (2) acceptability of the online Chinese iSupport design; (3) motivations to engage in the iSupport program; (4) desire to interact with peers and professional facilitators; (5) concerns about program accessibility; and (6) the need to extend the iSupport program to care workers. Themes 1–2 reflect the surface structure, whereas themes 3–6 indicate deep structure concerns when culturally adapting the Chinese iSupport program in Australia, as described in the ecological validity framework above. These themes are elaborated below.
Appropriateness of the Chinese iSupport content
Participants discussed the appropriateness of the Chinese iSupport program. First, they confirmed that the content of iSupport and the language used in the program were appropriate based on their pre-focus group review and comments on the manual. The few suggestions for changes included (1) using the Chinese word ‘失智症 (shizhizheng)’ rather than ‘痴呆症 (chidaizheng)’ as the latter is viewed as stigmatising people with dementia; (2) using both Chinese and English words when introducing aged care services and resources; and (3) increased use of Chinese diet, music and photos throughout the program to enhance cultural appropriateness, as care worker FG 3 discussed: Care worker: Diet examples could be more suitable for the Chinese, such as rice or porridge, or add a few recipes. These features would stimulate their interest to learn. Care worker: iSupport mentioned thickening food. It is better to add English words next to the Chinese word so that if older people need to buy a product, they can show the English name to the chemist of what they want. Care worker: Need to provide them with a service directory. Let them be aware there are relevant support services for them.
Overall, caregivers and care workers were satisfied with the core content of the iSupport program.
Acceptability of the online Chinese iSupport design
Participants shared their thoughts on how to help caregivers easy access the program through the online program design and suggested these functions:
Care worker: For older carers, it is better to use a voice recognition function or key words to search for the information and services they need in the program. The majority of Chinese-Australians use WeChat. Establishing a WeChat Mini-Program may help them easily access and utilise the program (Care worker FG 3).
Participants also suggested diverse iSupport program formats to accommodate the preferences of different user groups as discussed in Caregiver FG 2: Caregiver: Nowadays we like listening, like the radio. The best solution is an audio program you click on and the audio program starts. Then we can use a smart phone to listen to it while doing some housework. Caregiver: Audio is the best as you can listen to it, rather than read it. Tell some stories for us via an audio program. Caregiver: Older people may have some difficulties in reading the program. If they read too much, they feel tired.
Care workers mentioned that some older people have poor literacy. Therefore, ‘Short videos would increase their interest in the program (Care worker FG 2)’. Findings indicated participants’ concerns about functional decline in older caregivers and the impact of this on older caregivers’ ability to use the iSupport program. An audio version was the most popular format suggested by participants.
Motivations to engage in the iSupport program
Caregiver participants showed motivations to provide good care for their family members and to search for assistance and knowledge to support their caregiving performance. Therefore, they were keen to engage in the Chinese iSupport program in order to provide the best care they could for a loved one: Female spouse caregiver: I would read at least two hours a day because my main job is to look after him [husband]. I have nothing else to do. I only want my husband to live longer, make sure his dementia would not progress too quickly… (Caregiver focus group [FG] 1).
Care workers echoed caregivers’ views regarding motivations to learn from the iSupport program: Care worker: Carers are under high pressure when they look after family members with dementia … if incidents happen suddenly, they have nowhere to go to get help …That is why I wish this iSupport could provide advice to solve problems in a timely manner (Care worker FG 1).
Learning from iSupport could enhance self-help strategies as described by caregivers in FG 1: Caregiver: I would use it because I can get more resources to help me look after my grandmother. I have encountered difficulties such as assisting her to the toilet and showering her. Caregiver: I need it and I would look for it as my online dictionary for self-help. I wish I could access the program anytime when I need it like I use the online English dictionary.
Spouse caregivers indicated that ‘Time is not a problem’ (Caregiver FG 2). They described: ‘We have plenty of time since retired (Caregiver FG 2)’. This situation was further explained by care workers, ‘They [caregivers] are hungry for dementia care knowledge due to very few dementia care programs currently offered in a Chinese language for them (Care worker FG 4)’.
Desire to interact with peers and professional facilitators
In addition to self-learning, caregivers suggested establishing peer support groups and having professional facilitators as they elaborated in Caregiver focus group 2: Caregiver: It should establish iSupport WeChat groups for those from mainland China or WhatsApp groups for those from Hong Kong and Taiwan to have some interaction. Caregiver: We should have some interactions with professional facilitators, like you [the researchers], who are from the same language and cultural background so that we can ask some questions. They can even give us lectures if it is needed. That is what I want to include in iSupport.
Similarly, care workers made suggestions for encouraging interaction between iSupport program participants: ‘If there is a space for questions and answers, carers would be more interested in the program (Care worker FG 3)’. Care workers further discussed the benefits of incorporating support groups within the iSupport program: ‘The best support is to provide these carers with some avenues to relieve their pressure. …I think sharing is the best way to relieve their stress (Care worker FG 4)’. Another added: ‘If the program builds a forum for carers to share their experiences, they will use it more frequently and possibly use it long term (Care worker FG 3)’. Although iSupport is designed as a self-learning tool for caregivers, stakeholders also considered this program to be an opportunity to enhance peer and professional support.
Concerns about program accessibility
Care worker FG 4 were concerned about low computer literacy among caregivers impacting on accessing the program: Care worker: It could be a bit difficult for older people to find the program online. Many of them only use computers to watch videos, rather than a tool for education. Care worker: I just thought that elderly have barriers to using the internet to search for information in English, rather than being reluctant to learn. Care worker: My concern is whether they know how to use a computer? Many of our clients do not have an email address or they often forgot their passwords to access. These will be the barriers for them to search and use iSupport. They might think it too troublesome and therefore, do not use it.
Participants suggested that engaging Chinese-Australian community organisations to promote the Chinese iSupport program could address poor computer literacy and language barriers, as discussed in care worker FG 3: Caregiver: Using flyers to disseminate iSupport in Chinese xx [a Chinese organisation] and Chinese xx [another Chinese organisation], Chinese schools and churches will let Chinese families know about the program. Caregiver: Gatherings for Chinese festivals in Chinatown are good opportunities to promote the Chinese iSupport program. You just need to design and printout booklets that introduce the program and bring to the events in Chinatown. Chinese families will look at the information. Caregiver: We will need to use various platforms to promote the iSupport in the Chinese community, for example, the WeChat, community radio and the newsletters of community organisations.
Findings indicated that strategies to raise awareness of the Chinese iSupport program and to address poor computer literacy in older Chinese caregivers will be much needed in order to ensure high uptake of the program.
The need to extend the iSupport program to care workers
Care workers from all focus groups embraced the iSupport program and recognised that they too could learn from it in relation to behavioural and psychological symptoms of dementia: ‘Well, I think professional caregivers like us also need to learn this program. Many times, we encounter clients with Alzheimer’s disease who go ‘crazy’ and we don’t know how to deal with the situation (Care worker FG 3)’. The lack of understanding about responses to difficult behaviours in clients was echoed by other care workers: ‘Quite often, I observe clients with dementia suddenly become hallucinated and I don’t know how to deal with the situation. So, at that time, I wish I could get some help via an internet search (Care worker FG 2)’.
Care workers described a lack of dementia education in the workplace, especially in managing difficult behaviours of clients. They showed their desire to learn from the iSupport program: ‘We do not have someone to teach us how to work with these clients. I found this program is a very good for self-learning (Care worker FG 3)’. The benefit of learning about how to manage difficult behaviours from the iSupport program was even recognised by care workers with a long-term employment in the industry: Care workers: I have been working in this industry for 11 years, but I still feel I don’t know how to help them [people with dementia] when they are very angry. Sometimes I cannot control my emotions and I feel very tired at work. So, I need to learn the iSupport program and I need to talk with someone about how to deal with clients with behaviours and how to help their family carers (Care worker FG 4).
Moreover, workers in a leadership and management position mentioned that the Chinese iSupport program would addresses language barriers in dementia training programs currently available to staff: ‘To be honest, most direct care workers are first generation migrants and have limited English. They encounter difficulties in dementia training courses provided in English (Care worker FG 4)’. However, participants recognised that ‘iSupport is a learning resource for caregivers, the content needs to be changed to be a little more complicated for care workers (Care worker FG 3)’.
Discussion
To the best of our knowledge, this is a very first study on the cultural adaptation of the WHO iSupport for Dementia online program for a large ethnic/migration population in Australia. Like many developed countries, Australia shows an ageing population with 29.8% of the population born in various, mainly non-English speaking, overseas countries (Australian Bureau of Statistics, 2021). Disparities in supporting caregivers of people with dementia between the mainstream culture group and the ethnic/migrant groups is reported in the recent WHO report on ‘Global status report on the public health response to dementia’ (World Health Organization, 2021). This is far away from achieving the global goal that by 2025, 75% of the 194 WHO member countries provide support and training programs for caregivers (World Health Organization, 2021). Culturally adapting WHO iSupport for all caregivers including those from ethnic/migrant groups in a country is a way to address the disparity. Findings in this study add new knowledge and new understandings to the international community regarding approaches to adapting the WHO iSupport program by providing an ethnic/migrant minority group’s views on appropriateness, acceptability, accessibility and implementation strategies of the program, using Chinese-Australians as an example.
The finding that providing the best care for spouses and older people in a family suggests a motive for Chinese caregivers to engage in iSupport program. The finding is in line with other studies on Chinese caregivers in which Confucianism that emphasises filial piety, obligations for caring for spouses and family members, and harmony within a family were reported as motivators (Ma & Saw, 2020; Yiu et al., 2021). In addition, Chinese caregivers often felt that they received inadequate support from services currently available to them in a Chinese-minority society (Ma & Saw, 2020; Xiao et al., 2016). Therefore, they viewed Chinese iSupport as a unique self-help education tool for problem solving.
Our study reveals that caregivers desire to interact with peers. The finding supports previous studies that caregivers are frequently socially isolated due to time commitments of their caregiving role at home and limited social networks among Chinese migrants (Ma & Saw, 2020). The finding that using social media platforms, such as WeChat and WhatsApp, to enable peer support also reflects the wide use of internet and virtual communication by Chinese caregivers in Australia (Caidi et al., 2020). Systematic reviews have confirmed that virtual caregiver support groups would reduce stress and improve health and wellbeing for caregivers (Etxeberria et al., 2020). In addition, virtual caregiver support groups have a benefit of overcoming challenges arising from COVID-19 restrictions (Alzheimer’s Disease International, 2020).
Both caregivers and care workers in our study commented that bilingual and bicultural professional facilitators should be appointed to lead caregiver support groups. The finding may reflect challenges caregivers encounter in their daily care activities and difficulties with gaining timely support from professionals from the same language and cultural background (Brijnath et al., 2021). Although Australia has well-established dementia care services from diagnosis to end of life care, even caregivers from the mainstream culture perceived these services as fragmented and hard to navigate to meet their individual needs (Steiner et al., 2020). Chinese caregivers with limited English encountered even more difficulties in identifying and access these services (Ma & Saw, 2020). The desire for having a professional to lead caregiver support group identified in our study also support the current dementia caregiver support model used in Scotland where caregivers are assigned to a link worker as a single contact point for accessing and utilising care services that the person with dementia and caregivers may need for a minimum of 1 year after dementia diagnosis (Alzheimer Scotland, 2019).
Our study also identified that an audio version of the iSupport program is the preferred alternative format for caregivers who are older, physically frail and/or have limited time to engage in an online program. The finding reflects previous studies that caregivers usually provide more than 35 hours of care activities per week and the majority are older people who live with a variety of chronic conditions (Farina et al., 2017). The need for different versions of the Chinese iSupport program is consistent with previous studies that Chinese diaspora in developed countries are from diverse backgrounds (Australian Bureau of Statistics, 2018; Ma & Saw, 2020). Therefore, a one-size-fits-all approach to implementing iSupport may create new disparities for Chinese-Australian caregivers. The need for different implementation models to accommodate the needs of sub-cultural groups is also described in the ecological validity framework (Durlak & DuPre, 2008; Spanhel et al., 2021). Moreover, our finding that community engagement is a crucial approach to addressing access and utilisation issues supports the ecological validity framework in which community organisations are viewed as a meso-condition for promoting and sustaining culturally adapted intervention programs (Bernal & Domenech Rodríguez, 2012b; Durlak & DuPre, 2008; Spanhel et al., 2021).
Surprisingly, care workers in our study perceived Chinese iSupport as a suitable psychoeducation program for themselves. This confirm previous findings among care workers from ethnic minority groups in Australia where the lack of dementia education and training, and the negative impact of this situation on their practice and emotional wellbeing (Nichols et al., 2015). Care workers who provide home-based care for clients with dementia usually work in isolation and have to deal with complex care activities with less support from their peers and management (Leverton et al., 2021; Xiao, Harrington, et al., 2021). There is a lack of research evidence on effectiveness (Cooper et al., 2017), especially evidence related to care workers from ethnic minority groups who may have unique learning needs and preferences.
Limitations of the study
First, participants in the study were self-selected from one ethno-specific aged care organisation and findings may not represent those who were not invited into the study. Second, caregivers participating in the study mainly cared for people with mild and moderate dementia and use the internet to search for health information. Therefore, their views may not represent those who care for late stage dementia at home or those who do not use the internet. In addition, as a qualitative study, findings cannot be generalised but may be transferred to similar socio-cultural contexts such as Chinese migrants living in developed countries.
Implications for policy, resource and practice development, and future research
Application of the ecological validity framework to the cultural adaptation of the Chinese iSupport program.
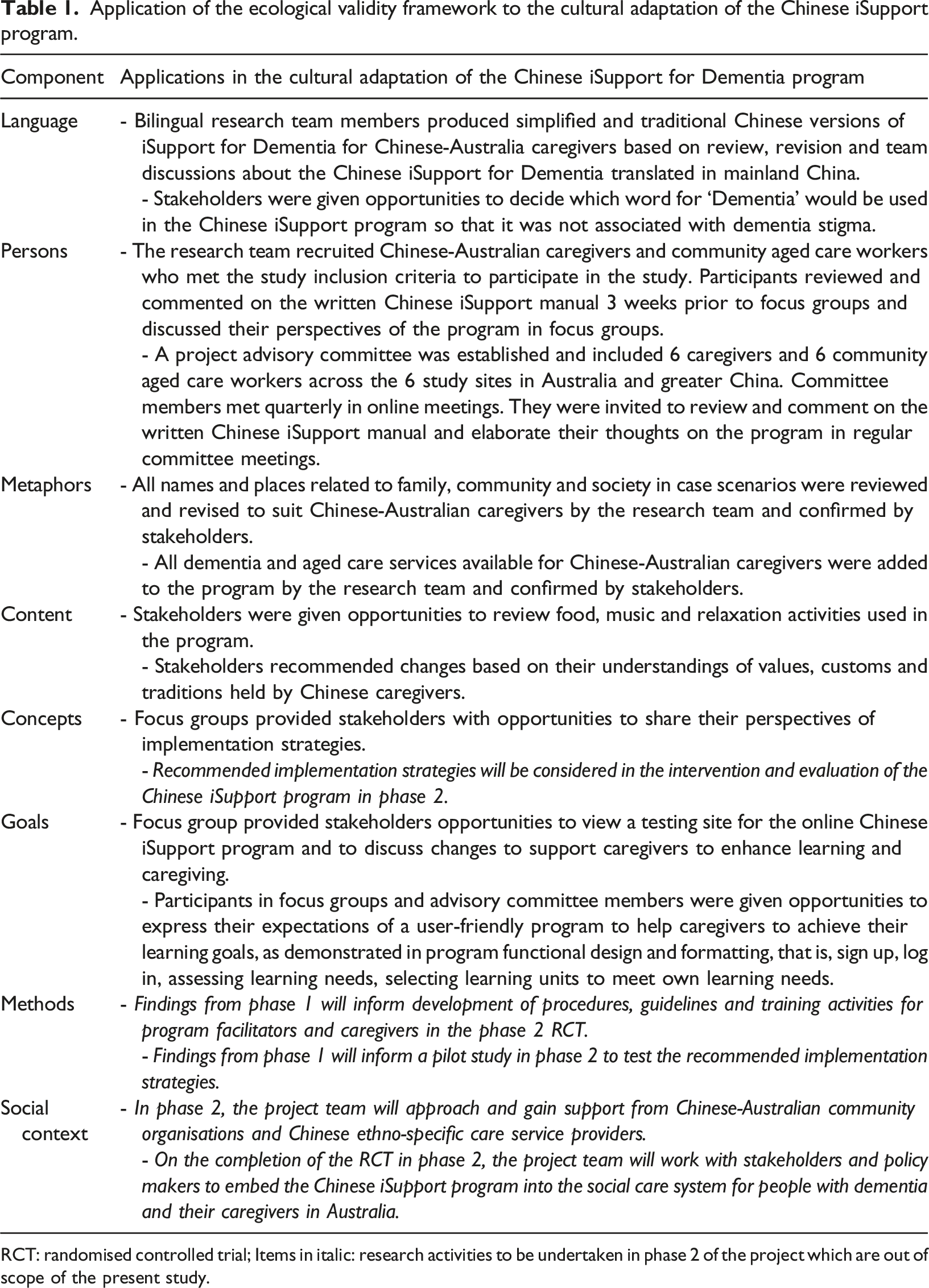
RCT: randomised controlled trial; Items in italic: research activities to be undertaken in phase 2 of the project which are out of scope of the present study.
Conclusion
Application of the ecological validity framework to inform the cultural adaptation of Chinese iSupport program enhanced stakeholders’ engagement in this study. Findings reveal Chinese caregivers are keen to learn from the Chinese iSupport program and hope that the program will include peer and professional support. Care workers also indicated their interest in undertaking a similar program. Barriers and enablers identified in the study will inform the intervention design to implement the Chinese iSupport program in phase two of the project.
Supplemental Material
Supplemental Material - Cultural adaptation of World Health Organization iSupport for Dementia program for Chinese-Australian caregivers
Supplemental Material for Cultural adaptation of World Health Organization iSupport for Dementia program for Chinese-Australian caregivers by Lily Dongxia Xiao, Mei Ye, Yunrui Zhou, Hui-Chen (Rita) Chang, Henry Brodaty, Julie Ratcliffe, Bianca Brijnath and Shahid Ullah in Dementia
Footnotes
Acknowledgements
The researchers would like to acknowledge their appreciation to the participants of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project is funded by the Australian Government via National Foundation for Australia-China Relations in 2020 (project ID NFACR216).
Supplemental material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.