
Abstract
Background
Every person has the right to autonomy, and to be involved in decisions about their care. When persons with dementia have difficulties in expressing what they want, their autonomy is challenged. Staff should strive to involve the person in care decisions, to obtain consent and to avoid the use of coercion and restraints. However, care without consent exists and coercion and restraints are being used. In order to improve care, further knowledge is warranted.
Aims
The purpose of this study was to explore staff’s experiences of obtaining consent when caring for persons with dementia.
Methods
In total 14 focus group interviews were conducted with staff with experience of dementia care who work in either home care or residential care in Sweden. An inductive qualitative content analysis was used to analyze the collected data.
Results
Three categories were generated describing staff experiences of consent in dementia care: the person as the decision-maker, the staff as the decision-makers, and the viability of the consent. Overall, staff found it difficult to know if they really had consent from the individual. Even if the person verbally gave consent, it was challenging to know if the person really understood what they had consented to. Common to all three categories was the significance of the relationship between the person with dementia and staff: getting to know the person, recognizing the person’s response in terms of their facial expressions and body language as well as being able to explain and justify specific actions to the person.
Conclusion
Staff need better conditions in dementia care, including training and time to reflect on how to obtain consent. A person-centered approach can be one way to develop care and ensure that persons with dementia are allowed autonomy and to share in making decisions.
Introduction
The prevalence of dementia in Sweden is approximately between 130 and 150,000, with an incidence of 20–25,000 persons per year (National Board of Health and Welfare, 2018). Many persons with dementia live in their homes and manage their daily life independently or with support from relatives. In Sweden, persons with dementia in need of help, support and social care can receive either home care or residential care by formal caregivers, after an assessment by needs assessors i.e., social workers. Healthcare is mostly decided by a team of healthcare professionals. The municipalities are responsible for the care of older persons including both social care (SFS, 2001: 453) and healthcare (SFS, 2017: 30) and this involves staff from various professions. Nursing assistants work closest to the person with dementia and can help with performing household tasks (cleaning, shopping, laundry and cooking), assist with personal care (bathing, dressing and mobility), and basic medical issues (administrating prepared medications) (Szebehely & Trydegard, 2012). Most nurse assistants have a 3-year high school education and they are one of the largest staff groups in the entire Swedish labor market (Szebehely et al., 2017). Registered nurses, occupational therapists and physiotherapists are responsible for making assessments and providing health care, assistive technology as well as rehabilitation for older persons, whereas first-line managers have the responsibility for social services, staffing and finances in the care units. All of these positions require a university education (Swedish National Agency for Education, 2011).
Dementia is a progressive disease that usually brings losses of different cognitive abilities, particularly in being able to interpret and understand the environment. The person with dementia may also have decreased capacity to express their own desires, to understand information and to use received information as part of their decision-making process, as well as being unable to communicate their wishes, requests, and choices (Eriksson, 2012; Wangmo et al, 2019). Difficulties in different situations requiring decisions may arise since decisions in care should be made based on the person’s autonomy and this assumes that the person has the capacity to act deliberately (Groen-van De Ven et al., 2016; McCormick, 2021). These decisions may include issues regarding medical treatments and social situations in everyday life (Hamann et al., 2011; Samsi & Manthorpe, 2013; Wolfs et al., 2012). Obtaining shared decision making requires collaboration between the staff and the person with dementia where the person is supported in making decisions about their own life and their values and preferences are incorporated in care (Geddis-Regan et al., 2021). It also means that by Swedish law family members or intimate others are not allowed to serve as substitute decision-makers. It is only the persons themselves that can make decisions concerning their life (SFS, 2001:453). For informed consent to be valid, it should be preceded by the person being informed of the action, the meaning of it and what happens if the action cannot be done (Tunzi et al., 2021). Since dementia results in the person having trouble understanding instructions and the meaning of words, difficulties in getting informed consent arise. Difficulties like these increase the risk of being subjected to restraints and coercive actions in different care contexts (Evans & Cotter, 2008; Moermans et al., 2018). When persons with dementia have difficulties in expressing their own will and preserving autonomy, it poses challenges. Autonomy is not just a mental process, being independent can also mean being able to adhere to certain habits and rules of your choice (Willems, 2000). Staff have reported that issues of consent and autonomy can increase ethical stress in everyday work (Hemberg & Hemberg, 2020; Ulrich et al., 2010; Wangmo et al., 2019). Staff sometimes have to balance what they consider to be good care and the person’s integrity and autonomy. This is especially true when the individual opposes care and assistance that the staff deem necessary (Hofmann & Hahn, 2014), and this can create situations where coercion and restraints are used.
Examples of coercion and restraints are bed rails, alarm mats, wheelchair lap tray, medicine hidden in food or drink, locked doors and forced nutritional intake (Hamers et al., 2016). Coercion and restraints are often used as preventive measures to protect a person, for example from falls and injuries (Hofmann & Hahn, 2014). Studies show that the risk of staff using coercion and restraints occurs both in residential care and in home care (Beerens et al., 2014; Hamers et al., 2016; Scheepmans et al., 2018, 2020). Between 5% and 25% of older persons in ordinary housing (Scheepmans et al., 2018), and 6%–31% (Feng et al., 2009) in residential care, have been exposed to coercion and restraints, respectively, with a higher prevalence among persons with dementia (31%–64%) (Pu & Moyle, 2022). A Swedish study indicated that the use of coercion and restraints has increased between the years 2000 and 2007 (16% and 18% respectively) (Pellfolk et al., 2012).
Up until year 2010 there were regulations and guidelines on how restrictive actions could be used in Swedish social care (SOSFS, 1992:17). There has been no substitution by new law, but according to the Swedish Constitution (SFS, 1974: 152) every person is protected from deprivation of liberty. This applies to persons in all contexts, including within healthcare and social care, meaning that care actions should not be used against the individual’s will, but must be voluntary. Furthermore, each person has the right to autonomy and to decide how care should be provided (SFS, 2017: 30; SFS, 2001: 453), and home care and residential care must be provided with the consent of the individual (Brodtkorb et al., 2015; National Board of Health and Welfare, 2017). Without consent to actions, there can be negative outcomes for the individual, including physical (e.g., constipation and incontinence, ulcers), psychological (e.g., anger, negative self-esteem) and social (e.g., social isolation) consequences (Hofmann & Hahn, 2014). Thus, staff should strive to obtain consent and avoid the use of coercion and restraints. In the care of persons with dementia, this means that all efforts should be based on a person-centered approach (National Board of Health and Welfare, 2017). This is a holistic perspective focusing on the person behind the disease and involving the person in the care and sharing decisions as well as adjusting care in accordance with the needs of the individual in order to maintain wellbeing and quality of life (Edvardsson, 2015).
To summarize, without consent there can be many negative consequences and so persons with dementia should not be forced into actions during care. However, care without consent exists and coercion and restraints are being used. To improve care, further knowledge is warranted. The aim of this study was therefore to explore staff experiences of obtaining consent when caring for persons with dementia.
Method
Design
The study was carried out as a collaboration between the University and a municipality in southern Sweden. A project group was developed including the researchers authoring this article and staff working in elderly care in the municipality. The project group decided the design and purpose of the research. The researchers collected data and performed the analysis, but preliminary results were continuously presented and discussed within the group.
A qualitative research design was used where data from 14 focus group interviews were inductively analyzed using qualitative content analysis according to Lindgren et al. (2020). Focus group interviews can be viewed as a special type of interactive group discussion (Ho, 2012) where the participants are given the opportunity to share perceptions and experiences. The method is used to understand attitudes and values that underlie behaviors around specific contexts (Krueger & Casey, 2015; Stewart & Shamdasani, 2015). Focus group interviews were used in order to invite staff to discuss and reflect on their experiences of obtaining consent to care actions and thus avoiding the use of coercion and restraints.
Study settings, and sample and data collection
The interviews were conducted during fall 2018 and spring 2019 with staff caring for persons with dementia in different municipal care settings as participants. All data were collected in one municipality with approximately 140,000 inhabitants including approximately 2200 persons with a dementia disease (National Board of Health and Welfare, 2014).
Participants’ characteristics.
*some of the participants did not give exact years in profession meaning there is some missing data.
An interview guide was developed within the project group to capture staff experiences of coercion and restraints being used based on earlier knowledge of the phenomena. One interview question focused particularly on consent: How does the process of obtaining consent from the individual take place? Other examples of questions asked were: Can you give a recent example where you have worked with coercion and restraints? How can the use of coercion and restraints be prevented? All questions were open-ended and the participants were encouraged to discuss them as is the practice in focus groups (McLafferty, 2004). A pilot interview with the dementia team in the municipality was first performed to test the interview guide. Based on the pilot interview, only minor adjustments were made to the questions to better fit the purpose and to be clear to participants.
Two researchers participated in each interview which is in accordance with usual practice in conducting focus groups interviews (Krueger & Casey, 2015). One had the function of a moderator and led the discussion and ensured that all participants were given an opportunity to speak. The other researcher served as an assistant and was responsible for recording the interviews. At the end of each interview, the assistant also summarized what had been discussed to make sure that everything was understood correctly and asked if the participants wanted to add or change anything. All three researchers were involved in collecting the data. The length of the interviews varied between 60 and 90 min as agreed.
Ethical approval
When interviewing staff about their work, no ethical review is required (SFS, 2003: 460), but research must always be conducted in an ethical way. The Helsinki Declaration (1964) was followed when planning and conducting this study. Both written and verbal information about the study were given including information that it was confidential, that they could withdraw their participation at any time without any explanation being required and contact details for the researchers. No personal data was collected. Collected data were stored in accordance with national regulations, General Data Protection Regulation as well as policies at the University.
Data analysis
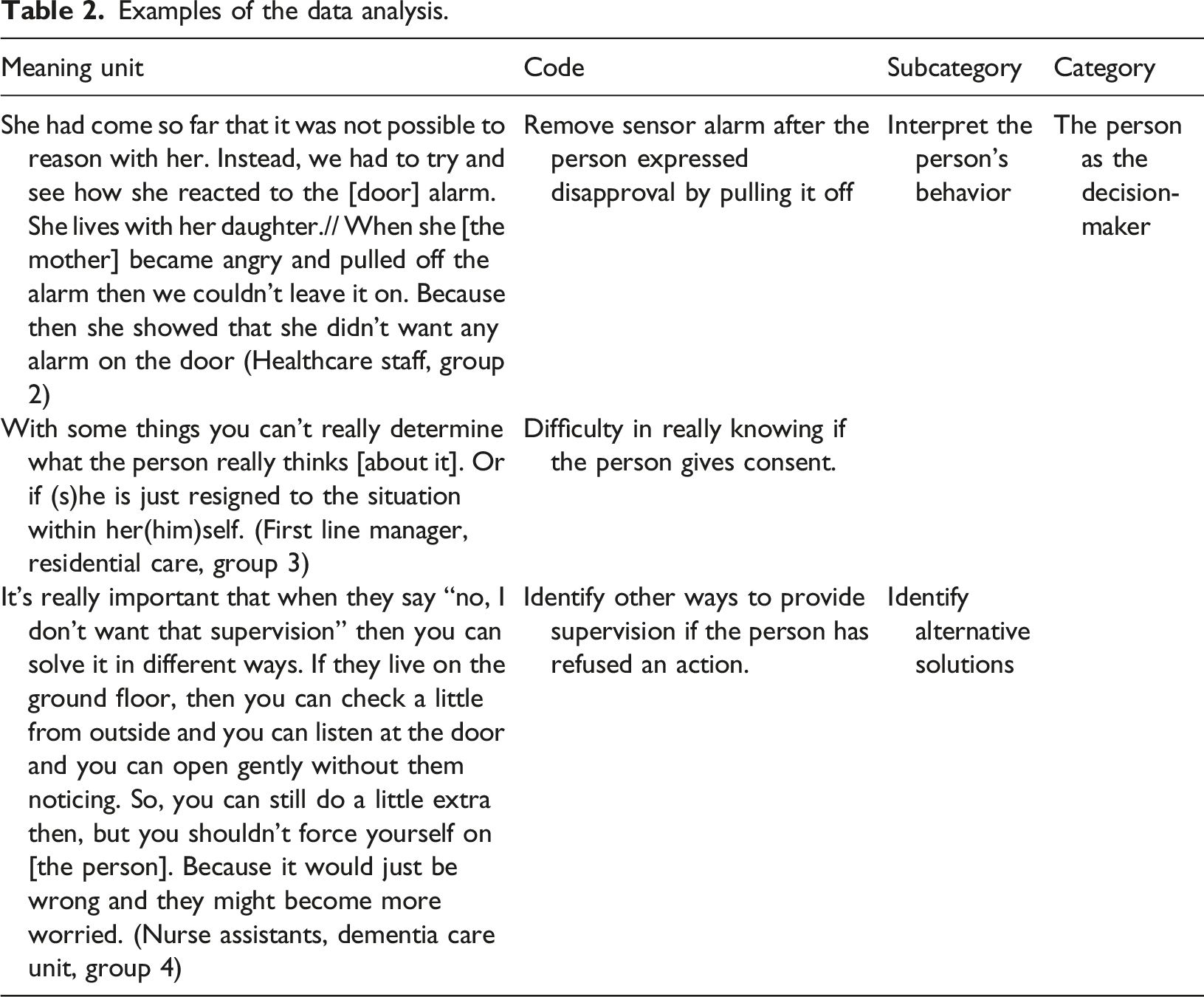
Each focus group interview was recorded and transcribed verbatim. An inductive qualitative data analysis was then performed to condense and abstract the collected interview data (Lindgren et al., 2020). The analysis started with all researchers reading the transcript carefully a couple of times to get an overall impression of its content. With regard to the aim, meaning units were then highlighted so that important text from the interviews related to staff experiences about consent were identified. Most of the meaning units identified were relatively long with more content than usual for meaning units, which was done in order to illustrate this complexity in a thorough way (Lindgren et al., 2020).
Examples of the data analysis.
Results
The analysis revealed three categories describing staff experiences of consent in dementia care: the person as the decision-maker, the staff as decision-makers, and the viability of the consent. The categories and associated subcategories are presented in detail below and in Figure 1. Overview of the categories and subcategories and the importance of the relationship as the common thread.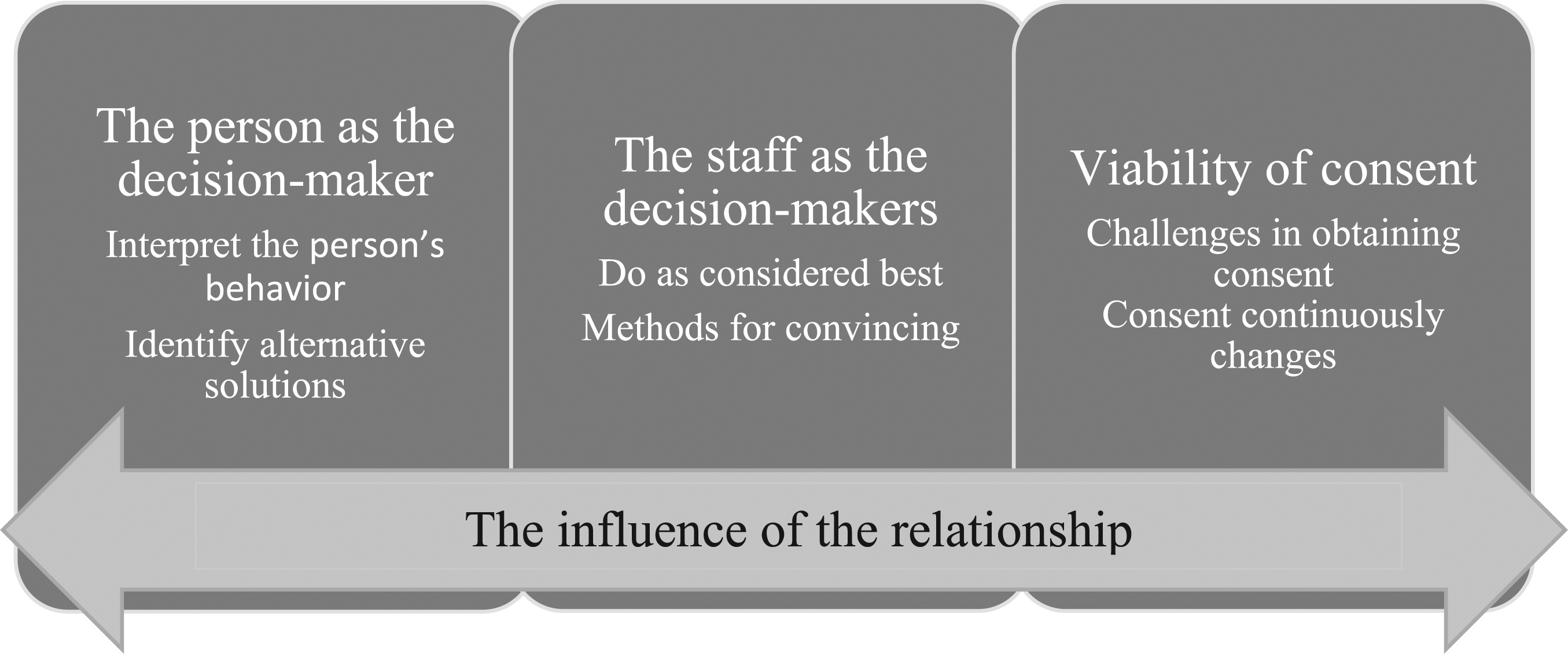
Overall, staff found it difficult to know if they really had consent from the individual. Even if the person verbally gave consent, it was challenging to know if the person really understood what they had consented to. Also, a person might consent on one occasion but not on the next. For non-verbal persons, the staff interpreted facial expressions and body language, with the risk of misinterpretation. This was especially true when staff did not really know the person.
Common in all three categories was the significance of the relationship between the person with dementia and the staff member. Staff talked about how important it was to build a relationship in order to get to know the person, to recognize the person’s facial expressions and body language, and to be able to explain and justify specific actions to the person. Meeting the person on a regular basis was stated as important, as it takes time to get to know the person. Having a close relationship was considered to be a success factor in obtaining consent as well as important when trying to identify other solutions: “If you know the person well, you can interpret their body language and you can see in their eyes and their behavior even if they are unable to say something.” (Nurse assistants, dementia care, group 4)
The person as the decision-maker
The person as the decision-maker describes the staff member’s efforts to allow the older person to be in control of the care actions and included the subcategories: (1) interpret the person’s behavior; and (2) identify alternative solutions.
Staff are well aware that the interventions, assistance and support they provide to persons with dementia should be subject to the volition of the person and that they must obtain consent for the various forms of support they are offering as it is otherwise considered to be coercion and restraint. Staff strived for consent in the person’s everyday life, for example by asking where the person wanted to sit or if the staff were allowed to enter the person’s apartment. However, staff stated that receiving verbal consent could be difficult and that persons with dementia sometimes had trouble expressing their consent. Therefore, situations arose where staff interpreted the person’s behavior in different ways. The person might signal dissatisfaction for example by facial expressions and body language, or by trying to remove an aid: “If they have a belt and they sit and pull it, then it’s pretty clear that they don’t want it. So, then you have to read the person. It is important (to them) and then you remove it.” (Nurse assistants, residential care, group 12)
Some participants stated that they were able to see in the eyes of a person if (s)he was satisfied or dissatisfied. To be able to interpret the person’s behavior adequately, staff really had to know the person, meaning that there had to be a relationship between the person and the staff member. Once a relationship was established, staff could understand and read the person more easily, for example notice the signals the person was sending if (s)he did not want a specific action. They could then detect that the person was panicking for example, by the person acting paralyzed or grabbing the staff roughly. “Yes, but then you have to interpret their behavior, you can see it in a person, if you know the person. If I'm familiar I mean. You might not be able to do so if you are meeting the person for the first time, but if you have met this person a few times you can see their facial expressions.” (Nurse assistants, dementia care, group 4)
There was a fear among the staff that they might interpret the person’s signals incorrectly. This risk was greater when meeting the person for the first time or if they had not had the opportunity to get to know the person well and thereby did not know how the person usually behaved in similar situations. This could result in situations where staff did not know how to best help the person. Staff stated that they sometimes had an internal discussion about whether an action would be better or worse for the person and what the person would have preferred if s(he) had been in a healthy state (i.e. without dementia).
If the person, either verbally or in other ways, expressed displeasure, staff thought it meant that they had to stop using that action, since the person’s wishes should guide their care. To make sure the person received the necessary care in a safe way and with high quality, staff sometimes had to identify other solutions: “I mean, you always check what kind of person you are dealing with. Some can answer “yes” or “no” for example. Even though they have cognitive impairment some might be able to say it. And if they can’t you can perhaps get help from a relative who knows the person. Or you can try to, if you aren’t able to get any reasonable answer, you might, yeah, then we do this and then we will see how the person responds and then you have to interpret their behavior and continue from that. Either remove the thing or... do something else.” (Registered nurses and allied health professionals, group 8)
Staff described several alternative solutions to ensure that care was based on the person’s wishes and at the same time protective. For instance, if a person refused bed rails but had a high risk of falling from the bed, a solution was to lower the bed very close to the floor and put an extra mattress on the floor. In another case, one participant expressed that there was only one staff allowed to help a person with showering. Therefore, to fit the person’s wishes and preferences, staff organized the schedule so that the particular staff member was working on the days for showering. “But there are those who say like: “I’ll just have her to come to [help out with] my shower”. So, there are those who really don’t agree with this, but then there is consent and we note that the person just wants to be showered by their contact person so ... it happens.” (First line manager, home care, group 7)
The staff as the decision-makers
The staff as the decision-makers describes situations when the staff feel a need to help the person but are unable to obtain verbal consent. Nevertheless, they need to find ways to be able to provide support. In this category, two subcategories occurred: (1) do as considered best; and (2) methods for convincing.
Obtaining verbal and direct consent to a specific action was often described as difficult. Ethical dilemmas occurred when the staff needed to choose between two available options where neither was considered good. “So, she might go out and fall again. It’s sad. I think when you can’t get access to the problem really. The person doesn’t know their own best so it’s hard.” (Nurse assistants, home care, group 6)
Staff claimed that they had to do as considered best for the person. This meant that when the older person did not fully understand what was best for him/her, staff had to make decisions over the head of the person. This was more common when the person had severe dementia symptoms. However, even with the best intentions, the balance between the person’s self-determination and giving safe care was perceived as a challenge. It was reasoned that if staff made decisions based on their skills and experience, this could be considered as appropriate. Also, always following the wishes of the person might lead to doing nothing, which may result in neglect or put the person in danger. Consequently, sometimes staff justify their decisions as having been done with the best interests of the person, for example: “Yes, but it’s not just sedative medication we give, but it can be for some heart problem or diuretic that she had to take and had certainly taken her whole life maybe, so... so you don’t think that [you]force them when you give them medicine, I don’t think so anyway.” (Nurse assistants, dementia care, group 4)
Occasionally, some staff knew the person in need of care better than their colleagues, which can make it easier for those staff to interpret the person with dementia’s actions and give support. Those particular staff members sometimes also served as a proxy in relation to other colleagues and explained how to interpret and understand the person.
Staff reasoned that they sometimes interpreted consent in a way that was favorable to them in terms of what they considered to be in the best interests of the person. This meant that staff were usually satisfied when a person said yes to an action that could, without consent, be considered as coercion or restraint such as bed rails even if it was unclear if the person had fully understood what s(he) had agreed to. If a person instead refused an action, staff interpreted this as if the person had not fully understood and they tested the action anyway. Consequently, staff did not always interpret a verbal “yes” and “no” from the person with dementia similarly, resulting in staff deciding what was the best for the person without actually being sure of the person’s own wishes.
Consent was also described as “a modified truth.” This meant that staff might ask only once a month, for example, if the person accepted the use of a belt even if they thought that the person didn’t really understand the question but did not show disapproval. Staff argued that, if done in a correct way, they would have to ask for consent every time the belt was used and that asking just once a month was not sufficient. However, it was also highlighted that asking every time an action was used could create insecurity and anxiety in the person with dementia. Therefore, it was considered that it might be better to just see if the person accepts the action (s)he agreed to earlier: “It will only worry more if you ask about consent. For they would, as you say, not understand what it was really about. And then thoughts would start; “what is this about? What is it now they want to talk with me about? What have I done now and what is it all about?” Yes, it would create anxiety.” (First line manager, residential care, group 3)
Staff described how they tried to get consent by different methods of convincing, such as motivating, coaxing and persuading in order to make the person accept a certain action or support. For example, when staff assessed that there was a need of an action, they convinced the person to at least try it, even if the person had said no or in a non-verbal way expressed that (s)he wasn’t interested in the action. Not trying to convince the person to accept actions sometimes also felt wrong as the actions were done to help and support the person and increase their wellbeing, and were sometimes even vital: “Sometimes it feels like you... with persuasion make them agree to things. That is, you ... Yeah. Actually, they may not want to, but they agree to it in the end// Then maybe they think it will be fine.” (Nurse assistants, home care, group 14)
Some persons were considered to be easier to encourage, which staff thought was related to whether the person dared to question the authority of the staff. Staff explained that sometimes the older person was resigned to the action being taken, meaning that the person agreed to an action as a result of not wanting to argue with the staff anymore.
Viability of consent
The category viability of consent focuses on the complexity of knowing how long a consent is valid for and whether the person has understood the given information. This category contains two subcategories: (1) challenges in obtaining consent; and (2) consent continuously changes.
Not knowing if the person has understood the situation or remembers what they have been asked about poses challenges in obtaining consent: “I mean if you have received consent once, they may have forgotten it.” (Nurse assistants, home care, group 6)
Some persons never refused actions. The challenge in these situations was to assess if the person really had given consent and what it was worth. Staff wondered if a yes always was a yes or if the absence of a no was related to the person’s lack of capacity to understand the question or situation. “Yes, I have probably never experienced that they have said no. Maybe they don’t really understand what it means”? (Nurse assistants, residential care, group 13)
Staff expressed that consent continuously changes. The change depended for example on the condition of the older person in a particular moment, but also on whether the staff asking for consent had managed to establish a relationship with the person. An action that was considered acceptable to the older person just a short while ago could suddenly make the person upset or anxious. These continuous changes were described as very challenging for the staff. “It would be wrong to say that we have consent too, I think. If we get a consent one moment but then don’t have it in the next it will just be a masquerade of this consent.” (Needs assessors, group 5)
Usually, consent was obtained every time the action was used but since difficulty in remembering is a prominent symptom of dementia, many persons did not remember being asked about a particular action and thus were unaware of what they had consented to. However, this continuous asking for consent did not always happen. For example, persons with sensor alarms were usually asked about consent before installation but seldom asked if they wanted to continue to use the alarm or not. At the same time, actions could be followed up during team meetings. Sometimes staff had to be patient and give the person time to get used to a certain action in order to obtain consent. After observing the person for some time, the staff discussed whether the person seemed to be dissatisfied with or accepting of the action in the team and made decisions on whether to continue with the action or not. This resulted in the person not being asked about consent every time an action was used. Staff also mentioned that team meetings in themselves could be tricky, since the person should be informed that (s)he is discussed during these meetings according to current regulations. However, a common reason for not informing the person was to avoid anxiety.
Discussion
The results provide an insight into the complexity of obtaining consent when working with persons with dementia, in particular because the viability of consent was unclear as it continuously changes. To work in accordance with the wishes of the person it was therefore important to build a relationship. Either the person with dementia, or staff, was described as the decision-maker. The person as the decision-maker established that the wishes of the person were guiding the care actions and that the staff therefore needed to interpret what the person wanted. Staff as decision-makers showed that if the staff did not get verbal consent, they did what they considered to be preferable and then tried to convince the person to accept the actions.
This study reveals the difficulty of obtaining consent from persons with dementia, including not knowing if a person has really understood information as well as for how long consent is valid. There are few studies on how decision-making takes place in connection with coercion and restraints and the knowledge about how consent is obtained is limited (Pu & Moyle, 2022). For a person with dementia, it may be difficult to have an overview of one’s decisions and consider what will be best for them (Nedlund & Taghizadeh Larsson, 2016). In our study, staff expressed that they wanted to do what was best for the person but at the same time this was difficult as the person might give consent at one point but a moment later refuse the action. A reason for this is related to the symptoms of dementia, i.e., loss of cognitive functions such as the ability to interpret and understand the environment (Nedlund & Taghizadeh Larsson, 2016). Changes in consent could also be due to the feeling of not being allowed self-determination. For staff to facilitate consent, it is important to treat the person with respect and to share decision-making (Ericsson et al, 2013). However, results from a Swedish study among older persons in residential care revealed that they did not always experience respect or feel valued which sometimes resulted in anger or resignation (Hellström & Sarvimäki, 2007). Furthermore, Brodtkorb et al. (2015) found that when a person resists an action, this can lead to an emotional reaction in the staff member and risk resulting in a stressful situation for both staff and the person with dementia. As a result, staff sometimes instead made decisions without actually having consent from the person and this resulted in the use of coercion and restraints. This, not taking the wishes of the individual into account when providing care, can be considered to be manipulative behavior by the staff (Brodtkorb et al., 2015). In practice, it is rather common that staff act as deputies and make decisions for the person, even though neither the staff nor relatives can legally act on behalf of persons with dementia in Sweden. Additionally, if staff does not fully know the person, it may result in staff making a decision that does not correspond to the person’s will or wish. This situation makes the person with dementia more vulnerable. It is therefore of great significance that the person that acts as a deputy is someone who knows the person with dementia well. This can ensure the deputy safeguards the person’s norms and interests, as well as having a better understanding about what decision the person would probably have made him/herself (Sulmasy & Sulmasy, 2015).
The staff also state that they sometimes use different methods of convincing to gain consent to actions from the person. Staff indicated that this was not the ideal way of working, but when caring for persons with dementia situations sometimes occurred where all options to respond could result in negative consequences. In professional ethics this approach is not generally accepted. In the context of care, ethical principles need to be evident to guide care and there should be an expectation that ethical principles will be followed. For example, care should not harm, and everyone should have the right to equal care including the right to decide and give their consent on care actions (McCormick, 2021). Yet, from a clinical point of view the staff in this study expressed that following ethical principles all the time can be complex as they felt that they did not always find any solution to provide good care. Tunzi et al. (2021) discuss that informed consent is mostly understood as an all-or-nothing phenomenon when thinking about it in relation to the meaning of autonomy but argue that getting consent ranges along continuum from formal informed consent through assent to non-dissent. Assent can be understood as when the person express approvement to a recommend action. It can be used in common actions where the person needs to be given some information about the action in order to consent. Non-dissent can be used for multiple actions that are routine actions of care and it can be interpreted as consent if the person does not reject the action. To give information is the core practical challenge when working with persons with cognitive impairments, the process of receiving informed consent is not an easy task and sometimes not even possible. However, staff should make sure that the person is given the opportunity to maintain their autonomy and share decision-making as much as possible, which can be done by supporting relationships and interdependence. When a relationship is established, it will facilitate moving assent closer to full informed consent. But assent could also be weakened in a transition to non-dissent (Tunzi et al., 2021), for example if a person nods to give assent but after a short while shows a facial expression of non-dissent.
Working conditions may act to increase the risk of negatively affecting the autonomy of the person. For instance, staff may lack time to wait for answers from the person or to find alternative solutions when the person says no to an action that the staff deem necessary. To manage such situations, staff need to be aware of their own ethical positions and make assessments and reflect (Scheepman et al., 2018). Beneficence is one of the four ethical principles that Beauchamp and Childress (2009) discuss, focusing on how to minimize risks for the person and also weigh risk against benefit. To work according to this principle, staff need to balance giving the person benefits without inflicting any harm (McCormick, 2021). Protecting patients’ rights; autonomy and informed consent are examples of stressful ethical care issues that care staff encounter frequently, even daily. This frequency of ethical care issues is often related to understaffing and organizational problems. Without adequate staffing, there are difficulties in meeting the ethical standards. Today’s healthcare system in Sweden has inappropriate demands to provide high quality care and to manage costs with diminishing resources (Ulrich et al., 2010).
Edvardsson (2015) reflects on what is needed for ethical practice and states that it requires a true interest in the other person’s life and decisions as well as skills in systematic attention to and analyses of other’s wellbeing. In person-centered care, a core component is to see the person with dementia as a partner and involve the person in everyday matters (Backman et al., 2020; Ekman et al., 2015). Person-centered care starts with the experience of being present with another human being, trying to understand that person’s experience, and coming to know the uniqueness of the person (Molony et al., 2018). Furthermore, person-centered care entails recognition, trust, and respect, as well as prioritizing the experience of the person (Kitwood, 1997). Focusing on the person’s life story can assist staff to work in a holistic and person-centered way instead of focusing on performing a task, or solely on the disease (Gilster et al., 2018). This requires an organization that supports and motivates staff to apply a person-centered approach, including making sure that staff receive sufficient training and education (Kim & Park, 2017). Staff need continuing education, for example through mentoring, online material or written material, practical exercises, group reflection, supervision, drama exercises, and working with cases (Surr et al., 2017). Another tool is to give staff an opportunity to work with reflection teams where they can reflect on specific caring issues under the direction of a leader (Jonasson et al., 2017). According to a literature review by Rosoal et al. (2017) there are several approaches to support staff dealing with ethical issues in clinical practice. For instance, ethical rounds or ethical reflection groups can encourage staff to reflect over ethical issues. Such reflection can result in changed attitudes and increased critical thinking, and it can identify the best ways to act in certain cases. In this study, staff expressed that when they encounter a situation where they do not know how to act, support from colleagues with more experience is crucial. Using the skills that already exist among the staff who work closely with these persons is a successful way for staff to find solutions and thereby improve care (Jonasson et al., 2017).
In this study, staff talked about how important it is to establish a relationship in order to recognize and interpret the person’s facial expressions and body language, and to be able to explain and justify specific actions to them. Having a trusting relationship has also been highlighted in previous studies as significant in providing a sense of security for the person even if (s)he is not completely positive about an action (Hughes & Common, 2015; Karlsson et al., 2015). Continuity is needed to create a trustful relationship, where the same staff return to the same person and are thus given the opportunity to get to know each other (author blinded, 2020). To give the person with dementia a feeling of significance, Ericsson et al. (2013) discuss the importance of staff demonstrating that they have time for the person in order to make him/her receptive to staff’s suggestions. Accordingly, creating a good environment and relationship takes time. However, time is commonly lacking as a result of the stressful work situation staff are constantly experiencing (Shiells et al., 2020). Not only does time affect care outcomes, but also the professional caregiver’s attitudes and flexibility are of great importance (Ericsson et al., 2013; Gilster et al., 2018). This study revealed that there were certain situations where only one particular staff member was allowed to help a person to shower and to prevent coercive actions the team made sure that this person worked on the days for showering. This example again highlights that staff’s working conditions are a key factor influencing the relationship with the person with dementia and their ability to provide adequate care (Szebehely et al., 2017). Unfortunately, in Sweden the working conditions for staff in elderly care have deteriorated in recent times. In parallel with the deterioration in working conditions for staff, political ambitions regarding the need for improvement of elderly care and the rights of older people have increased. There is a clear trend towards person-centered care, which emphasizes the participation and self-determination of the elderly (National Board of Health and Welfare, 2017). There is a distinct discrepancy between the ambitions of the welfare state and the conditions of everyday work, and staff have expressed that they nowadays have more duties but less time since they care for more people, resulting in increased stress for staff attempting to provide adequate care (Szebehely et al., 2017). For clinical practice it is of great importance to create an organization where staff have the opportunity to build relationships and work in a person-centered way as well as increase staff’s different skills, as these are key components when working with consent and thus avoiding the use of coercion and restraints in dementia care. A Swedish public investigation conducted during the Corona pandemic identified several areas for improvement regarding elderly care including adequate staffing, satisfactory staff continuity and work environment, increased medical competence and more permanent employees. Continuous education for all staff is also called for, where ethical issues also need to be discussed (SOU, 2021: 52). Goh et al. (2022) found that, beyond education, good communication between the employer and the employee is needed regarding, for example, the information that the staff receives about the person they are going to help. If staff receive too little information, they do not know what is expected of them except for specific tasks to be completed. The staff also needs enough time to be able to help the person in a suitable way. Funding is linked to task completion and staff may feel that they are not given enough time to provide the best care. Another important factor in creating good working conditions is to ensure continuity, and that staff stay for a longer period. Since there are many temporary employees (working by the hour), staff can find it difficult to get to know colleagues and find a common working method that also means continuity for the persons with dementia that they are going to help.
The results of this study should be interpreted in the light of its strengths and limitations. When performing focus group interviews, there is no scientific consensus on the needed number of groups to get valid results. But Guest et al. (2017) for instance found that three to six focus group interviews will reveal approximately 90% of the categories. For this study, 14 focus group interviews were conducted, which included two to seven people in each group. Staff participated during working hours when they were able to leave work for approximately 90 min on the day of the planned interview, resulting in some focus group interviews having fewer participants. One of the key points of using focus group interviews is that the participants engage each other while expressing their thoughts and experiences (Krueger & Casey, 2015). In the groups with fewer participants, it is not always possible to get this dynamic happening, but the number of focus group interviews compensated for this, and the data was rich in participant experiences. Also, sampling participants based on availability can result in less variation and bias the results, i.e., negatively affecting the transferability of the study results.
Furthermore, the researcher’s pre-understanding of the phenomenon might have affected the process in this study as it could entail a risk of confirming expectations and reproducing truths rather than reconsidering and enriching current understanding. Using a project group consisting of both researchers and staff from the municipality when planning for the study also made sure it was relevant from a practical point of view. Prior understanding can also help to identify other things that otherwise risk remaining hidden (Alvesson & Sandberg, 2021). In addition, the authors’ (one social worker and two nurses) different experiences and knowledge about the phenomenon were considered to be a strength when analyzing the data.
Conclusion
Staff were aware that they needed consent to provide help, support and care for persons with dementia as it is otherwise considered to be coercion and restraint. At the same time, they stated that it is often difficult to know how to obtain consent because of the difficulty in knowing that the person has fully understood the situation and information. Ethical dilemmas therefore arose. Once a relationship has been established between the staff member and the person receiving care, it seems to become easier to understand and interpret the person’s signals and thus know if you have obtained consent. Consequently, it is important that staff are given the optimal conditions to work with consent including training and time for reflection. A person-centered approach can be one way to develop care and ensure that persons with dementia are treated with respect and allowed self-determination and to share in decisions. Persons with dementia are not a homogenous group, some live at residential care and some live together with relatives in their ordinary homes. Some are in an early stage in the disease while others suffer from later stages of the disease. In the future, more research is needed focusing on older persons’ own unique views on consent as well as the perceptions of the relatives.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.