
Abstract
Objectives
To obtain a deeper understanding of the phenomenon of sexuality within the couple relationship when one of the partners has received a diagnosis of Alzheimer’s Disease. This study aimed to listen to the voices of both partners, and to investigate how their intimate relationship has been impacted by an Alzheimer’s diagnosis.
Methods
This study adopted a qualitative phenomenological approach, and the method used was Interpretative Phenomenological Analysis. The data was collected based on interviews with six couples, where one of the spouses had a mild to moderate Alzheimer’s diagnosis. The interviews were recorded and transcribed, and a detailed analysis of each interview was performed.
Findings
From the detailed analysis of the transcribed interviews, six main themes emerged: Sexual expression today; Alzheimer’s and sexuality; desire to be a sexual being; different sexualities; sense of couplehood; and uncertain future.
Conclusions
The findings of this study provide a deeper insight into experiences of sexuality for couples living with Alzheimer’s. Sexuality and intimacy of couples living with Alzheimer’s continues to be an important aspect of the relationship, and in general, the partners wish to have the opportunity to express their sexuality. The construction of a sense of couplehood during the marriage tends to be a significant factor to sustain the changes that arise in the intimate relationship because of the diagnosis. However, despite the growing recognition of the existence and importance of sexuality in later life, persons with Alzheimer’s have only recently starting to be recognized as sexual beings who wish to be heard.
Introduction
Sexuality has always intrigued humans, but this interest often wains when we consider sexuality and ageing, and even more so when we include dementia. Sexuality and sexual expression are, for many people, fundamental to well-being throughout life, and despite the prevailing image of older people having little expectations of a satisfying sexual relationship, many older people continue to be sexually active, even at more advanced ages (Bauer et al., 2013; Srinivasan et al., 2019; Vieira et al., 2016). Sexual expression and being a sexual being do not simply disappear with a dementia diagnosis and increasingly dementia is becoming part of our reality.
Dementia can take various forms, including Alzheimer’s disease, vascular dementia, Lewy body dementia, and Parkinson’s dementia. It is estimated that today, one in 10 people lives with dementia, and it is predicted that cases will exceed 150 million worldwide by 2050 (World Health Organization, 2012).
Given the rapid changes in demographics, the significant increase in life expectancy during the last 50 years and the highest risk factor for dementia being age (Livingston et al., 2020), there is a need to become more aware of what it means, subjectively, to live with dementia. There is a significant absence of discussions of how memory loss and cognitive impairment impact the individual’s intimate life and couple relationships.
In contemporary society, old age is made invisible through the pathologization of the ageing body, and its associations with illness and malfunction. Rarely do we find positive images of older people’s bodies; an ageing body is more often associated with physical frailty and rarely associated with sexuality or fantasies of sensuality and intimacy. Many elderly people internalize and generalize negative attitudes towards their own sexuality and avoid sexual expression out of fear and shame (Bauer et al., 2016; Youell, 2015). When these prejudices are internalized, the pathological language we use to describe sexuality and aging then becomes normalized, and this is even more evident when we think of dementia.
Despite the growing recognition of the relevance of sexuality in later life, (Bauer et al., 2016; DeLamater & Koepsel, 2015; Sinković & Towler, 2019; Srinivasan et al., 2019; Traeen et al., 2019), people with dementia are seldom seen as sexual beings with sexual needs. Research into sexuality and dementia has often focused on the later stages of the illness, when the person with dementia is more cognitively compromised and the focus is on the problematic aspects of their sexuality (Sandberg, 2020). Nevertheless, it is evident that people in the earlier stages of dementia continue to regard themselves as sexual beings (Albert, 2021; Harris, 2009; Sandberg, 2020; Youell, 2015). A dementia diagnosis does not erase sexuality but may alter the way in which love and affection are given and received. Embracing persons with dementia as sexual beings, who have something to say about their own sexuality, and who have physical and intimate needs is essential for understanding their lived experience, in all its dimensions (Albert et al., 2022; D’Cruz et al., 2020).
The recognition that dementia is not experienced in isolation by the individual but within a relationship recognizes that couple intimacy is complex and paradoxical, and the expression of sexual intimacy often emerges as ambivalent and ambiguous (Albert et al., 2022; Youell et al., 2016). A significant proportion of people with dementia live in their own homes, and are often cared for by their spouses, which means the couple relationship is often sustained throughout the progression of the disease. The progressive nature of the disease means that it constantly presents challenges to the relationship, and to maintaining intimacy and a sense of ‘couplehood’, (Hellström et al., 2007), or a sense of “us” or “we” within the relationship is often one of the greatest challenges (Sandberg, 2020).
Until relatively recently, the assumption that older people were not sexually active, or if they were they would not be willing to take part in research, was widespread and was an obstacle to research in this area (Gott & Hinchliff, 2003). Over the last two decades the evidence base has grown, together with the understanding of sexual health issues and the different forms of sexual expression for the older adult. Evidence of this change can be seen in the number of studies that now collect data on the extent and range of sexual activities older people engage in (Barrett et al., 2018; Bauer et al., 2013).
These studies have clearly demonstrated that despite differences in physical health, older adults can and do engage in the same types of sexual activities as younger persons, and like younger adults, they may be satisfied or dissatisfied with their sex lives, which is also the case for couples where one spouse has dementia (Hillman, 2012). However, dementia and sexuality is still an underdeveloped area of research, given the complexities involved and the stereotypical views held about the sexuality of persons with a dementia diagnosis. The majority of papers published in this area have focused on only one spouse from the couple dyad, the care partner; consequently, the understanding of sexuality for a couple living with dementia is often only partial (Davies et al., 2010; Youell et al., 2016). This study is one of a few qualitative studies that include both spouses of the dyad as research participants, and thus offers a more comprehensive understanding of the shared couple experience (Daniels et al., 2007; Harris, 2009; Sandberg, 2020). This relationship-focused approach acknowledges couples as the interdependent and dyadic unit they represent and understands dementia as an illness that impacts relationships rather than individuals alone (Henderson & Forbat, 2002; McGovern, 2011).
Method
Data analysis
This research is a qualitative study based on semi-structured interviews, which were analyzed using Interpretive Phenomenological Analysis (IPA), developed by J.A Smith in 1996, supported by the theoretical concepts of Edmund Husserl (1964) and Martin Heidegger (1962), i.e. phenomenology, hermeneutics and idiography, and these theoretical ideas were operationalized by Smith et al. (2009) and Peoples (2021).
Interpretive phenomenological analysis focuses on the individual’s subjective experiences and aims to produce a coherent description of these experiences, and thus involves the thought processes of both the participants and the researcher. An interpretative analysis of these experiences is made within a certain social and cultural context, enabling the researcher to reflect on the meaning of the experiences reported.
The analytic account was developed based on the transcribed interviews, coded for experiential and meaning-making content, focusing on vocabulary and key words used, expressions employed and any emotions expressed. The interviews were coded independently by SCA and MSCP and revised together, and subsequently reviewed by JEM. Patterns in participants’ expressions and understandings of their experiences were extracted individually and collectively. From the coding, sub-themes and master themes were identified that were grounded in the data collected. For this research, the Consolidated Criteria for Reporting Qualitative Research guidelines (COREQ) were adopted (Tong et al., 2007).
Participants
Studies that adopt IPA as a research method recruit a small sample of participants, given that they are concerned with ‘understanding particular phenomena in specific contexts’ (Smith et al., 2009: p. 50). For the purposes of this study, couples who attended the Geriatrics and Gerontology out-patients clinic at Jundiai Medical University, (Brazil), were invited to participate in a research project focusing on their intimate couple relationship, six couples agreed to participate and be interviewed together. This sample was considered appropriate to allow an in-depth analysis of each couple and also to explore the unique and particular experiences of each case.
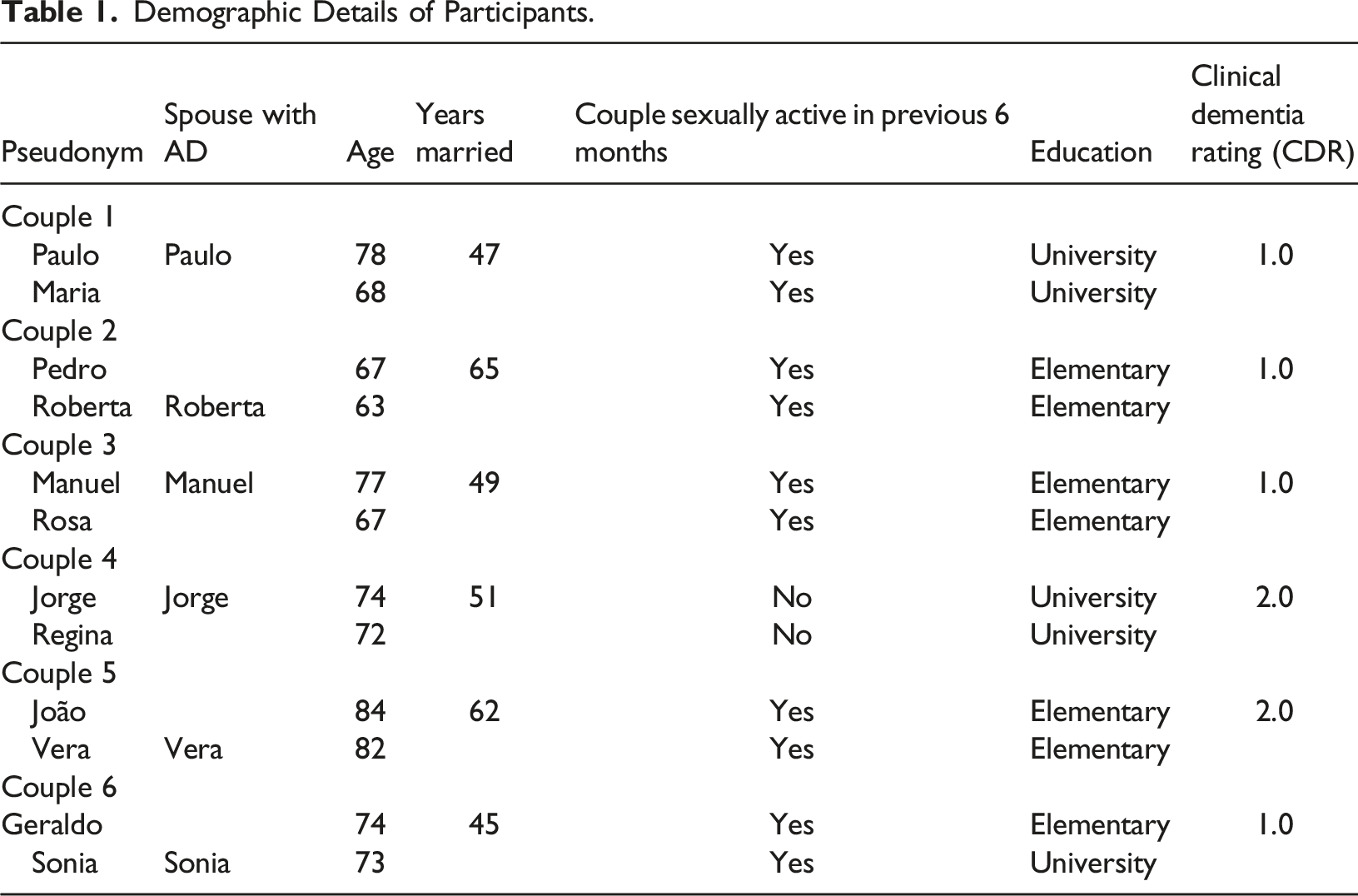
The participants consisted of six heterosexual couples in stable relationships (married for more than 10 years), aged 60 or older (the study was undertaken in Brazil, where persons aged 60 and over are legally characterized as “senior citizens”), in which only one of the spouses had a diagnosis of Alzheimer’s disease (AD), with a CDR (Clinical Dementia Rating) of between 0.5 and 2.0, as previously diagnosed by a geriatric through a detailed clinical anamnesis and a neuropsychometric evaluation. Only people with a diagnosis of Alzheimer’s disease were invited to participate in this study given the differences in manifestations between the different kinds of dementia. For example, frontotemporal dementia involves greater disinhibition and lower sexual drive than Alzheimer’s disease, which may create different issues in couple relationships (Sandberg, 2020).
Demographic Details of Participants.
Procedure
The couples were contacted before the interview to determine the place they felt most comfortable being interviewed. The interviews were conducted in the following locations: (a) the couple’s residence (4 couples); (b) the researcher’s consulting office (1 couple); and Videoconference call, given the restrictions caused by COVID-19 (1 couple).
The informed consent document was discussed prior to the interviews, all interviews were recorded using a digital recorder, and lasted on average 90 min. Given the sensitive nature of the research topic, the interview began with a broader enquiry into the nature of the couple relationship, which then led into questions concerning the intimate and sexual relationship.
Interview questions
Initial question You have been married for several years, can you tell me a little about your relationship, how you met and some important memories and moments during your marriage? Follow-up questions Can we talk about your intimate relationship? How would you describe your sex life? How do you show affection for each other? Has your sex life always been an important part of your life? Have you noticed any changes in your sex life recently? What do you attribute these changes to? How do feel that the Alzheimer’s diagnosis (memory lapses) has impacted your intimate relationship? When thinking about your intimate sex life, how do you feel about the future? What are your expectations?
Ethical issues
The capacity of a person with dementia to consent to sexual intimacy is paramount in all discussions of sexuality; consequently, this study focused on persons who were diagnosed with mild to moderate Alzheimer’s. As such, all participants with a dementia diagnosis actively participated in the interviews. The study was approved by the national ethics committee. Each of the 12 participants was given a verbal explanation of the study details and if they agreed to participate, they signed a consent form. Couples were assured that their information would be kept confidential and that their identifies would not be revealed in any published articles.
Findings
This study found 6 principal themes that captured the key experience of the meaning of an Alzheimer’s diagnosis on the sexual and intimate couple relationship: sexual expression today (divided into 3 sub-headings); Alzheimer’s and sexuality; desire to be a sexual being; different sexualities; sense of couplehood; and uncertain future. From the six phenomenological themes identified we were able to develop a better understanding of the complex and subtle experiences of intimacy and sexuality lived by the couples, as expressed in their own words.
Sexual expression today
All couples, without exception, took pleasure in narrating their shared stories, which included talking about intimacy and sexuality. They all continued sleeping in the same bed together and cuddling and kissing was an integral part of the majority of the relationships; however, this behavior was seen as an expression of companionship rather than sexual activity. Sexuality was understood to be confined to penetrative sex within a couple relationship, which often meant that other forms of sexual expression were not recognized as such.
Five of the six couples continued to be sexually active, or had been within the last 6 months, with different degrees of satisfaction reported. Consequently, this theme of ‘sexual expression today,’ has been divided into three sub-themes: Active and satisfactory; active but unsatisfactory or sporadic; and absent but loving.
Active and satisfactory
Two couples (C1 and C5) stated their current intimate relationship was active and satisfactory. During the interviews the ways in which these couples interacted together provided important insights into the intimacy of the relationship, which appeared to reflect the quality of their intimate sexual relationship during their marriage and the experience of their sexual intimacy today. This was expressed by Paulo (C1): It's part of life… if you have what’s down there and don't use it, it shrinks!! So, use it, right? So, within our possibilities, our limits, we use it, I think we need to use it, to keep us alive. [Both laugh]
And Maria, his wife, adds:
It has been wonderful, so much understanding, I would be happy repeating everything that we went through, (…) we always talk about everything. (…) We have always had an active sex life, we never stopped. It has always been good (…)
Couples C1 and C5 were still sexually active and were satisfied with their sex lives. It was evident that the care partner from these couples was active in managing the flow of the conversation and ensuring that their spouse was heard during the interviews and were attuned to the spouse’s needs and feelings.
Active but unsatisfactory or sporadic
Three couples (C2, C3 and C6) confirmed that their sexual lives were still active but unsatisfactory or sporadic, with 2 couples, C2 and C6, also stating that during their marriages they had often felt dissatisfied with their intimate relationship.
In the case of C6, the lack of dialogue throughout the marriage was evident, and the first sexual experience of the couple was remembered as extremely negative, particularly by Sonia, who said she felt ‘abused’. This experience appeared to overshadow their sexual intimacy throughout the marriage, and no attempt had been made by the couple to reflect on this experience and work towards developing a healthy satisfactory sex life. The dissatisfaction with their sex life is evident in this dialogue: C6 Geraldo: We still have sex, but more time goes by, 10 days, 15 days, if I let a month go by without approaching her, she doesn’t make an effort, it always come from me, it’s difficult for her to take the initiative. C6 Sônia: We hug and are affectionate, we live well, the problem is sex, today I am not very interested.
For these 3 couples, the absence of conversations about sexual issues and sexual pleasure appeared to negatively affect their ability to have a satisfying sex life, to cope with changes in sexual function and to negotiate any expectations for a satisfying sexual life in later life.
Absent but loving
Couple 4 stated they no longer had an active sex life, despite having had a satisfactory intimate sexual relationship until the dementia diagnosis, when Jorge lost interest in sex. However, they continued to have a strong sense of couplehood. C4 Regina talks about their intimate relationship:
Today there is no sex per se, but we have had a good sex life. I think it affected me more than him… I think I missed it more than he did, I don't know if it's like that, generally speaking, or maybe because I felt I had more vitality, I have only felt myself getting older in the last couple of years.
Although this couple were no longer sexually active, the spouses confirmed that their relational commitment was still strong, and the emotional connection was still very important.
Alzheimer’s and sexuality
All of the couples engaged in the conversation about whether they felt that Alzheimer’s had affected their intimate relationship and only one couple (C4) stated that they felt their sexual activity was affected as a result of the diagnosis. C4 Jorge had withdrawn from sexual activity, which both spouses attributed to the disease. However, their ability to have sexual intimacy and the possibility for the couple to enjoy sexual activity was in fact still physically viable, but rejected by Jorge.
Regina describes how this change came about: [his loss of] memory, changed how he interacted with me, he [Jorge] became much more of a friend/brother than anything else. He lost interest [in our sex life], he wasn't interested anymore. My family is wonderful, I feel love from all sides, so [sex] is no longer a top priority on the list. Today, companionship is the most important thing. Jorge interrupts: Ah… yes, BUT [emphasizing]… we are sexually distant, but we are still loving. It's very interesting, sexuality has decreased, but as it decreases, other things increase, affection, being together. Regina: It has created an interdependence, right? Jorge: I don't know what it is, but it's very strong. It is beautiful, it is different, we can feel it… and the feeling is VERY [emphasizing] strong.
The understanding of sexuality and sexual expression, for this couple, in particular for Jorge, seems to have been impacted by stereotyped views of aging and sexuality and also of dementia and sexuality. There were no physical limitations; however, perhaps the stigma of a diagnosis of dementia and subsequent memory loss impacted how the couple related to each other, and the denial of intimate sexual activity appears to have been a conscious decision by Jorge. This decision was not welcomed by Regina, but over time, they developed a relationship of companionship and complicity.
Desire to be a sexual being
The desire for intimacy and to enjoy sexual activity was expressed by the majority of the couples, which was seen as a way of maintaining a sense of couplehood. For example, C3 Manuel wants to affirm his sexuality: You know, in our intimate relationship, how can I say… I am more active than her, a lot more active. Whilst Rosa, his wife, expresses her desire to have a more active sex life: I would like to recover our sex life, to have our sex life back. Couple 5, João and Vera, make it clear that they consider themselves sexual beings: João: Sometimes once, twice, three times a month [we have intercourse]. Vera: There is never a wrong time for it [sex]!
Different sexualities
From the interactions and conversations between the couples, it was evident that the couples understood masculine needs and sexual expression to be different from female needs, with the former often taking priority.
Male sexual expression
In this study, masculine expression of sexuality focused primarily on erection and penetrative sex and comparisons with past performance. For the couples who continued to be sexually active, the male spouses tended to compare their current ability to have penetrative sex with the frequency of sexual activity in their earlier years, expressed in the words of C2 Pedro: In the past, we used to have sex once a week, then it was every 15 days, now it is every 20 days… we never stopped having sex.
Five of the male spouses (three of whom were diagnosed with AD) referred to their sexuality in later life with aspirations to continue to be sexually assertive, potent and to able to ‘perform’. Only one male, C4 Jorge, renounced his sexuality soon after receiving a dementia diagnosis. His spouse confirmed that her husband did not have erectile problems but had lost interest in having intercourse. No attempt was made to renegotiate the meaning of intimacy and pleasurable sex between the couple, and Regina’s sexual satisfaction was not discussed.
Female sexual expression
Female sexual expression and pleasure appeared not to be a concern for some of the couples. Two of the female participants experienced their sexuality in negative terms, reporting pain and discomfort during intercourse, in the case of C2 Roberta, and aversion to sex and an unsatisfactory sexual relationship, in the case of C6 Sonia. Whilst in the case of C4 Regina, her sexual needs were denied as a consequence of her husband withdrawing from sexual activity.
For two spouses (C2 and C6), it was evident that their main concern was with meeting their partners’ sexual needs and not their own, expressed in the words of C2 Roberta: I worry about not fulfilling his wishes, that’s my concern. In the beginning, when I had a problem, I was very worried he would leave me, because sex for most men is more important than for most women, right?
It appears that penetrative sexual activity remains an expectation of married life, but from which these three spouses derive little personal sexual satisfaction. In the case of C2 Roberta and C6 Sonia, it appeared to be viewed as an altruistic act or necessary for maintaining the marriage, consequently, these spouses understood that their own sexual pleasure was not attainable.
This is not to suggest that penetrative sex is problematic in and of itself, but rather that the construction of penetrative sex as ‘real’ is narrow and serves to reinforce the stereotype of the importance of masculine sexual ‘performance’ rather than affirming the difference of older people´s sexuality. These understandings limit the potential for sexual pleasure, particularly in the face of physiological changes that may make penetrative intercourse difficult.
Sense of couplehood
It can be challenging for a couple, when one partner has Alzheimer’s, to preserve a sense of togetherness and to have the relationship they wish for and had imagined for themselves. All couples, when referring to their relationships and narrating their histories, used positive dialogue when talking about their marriages, with several using words such as gratitude, friendship and complicity when referring to their life together. An interpretation of the couple narratives leads to the understanding that the sense of couplehood, commitment and relatedness, built up during the years of marriage, were fundamental in sustaining a strong sense of couple identity. All couples had been married for several decades and with this came a sense of intimacy and responsibility that seemed to sustain the relationship, and the dementia diagnosis appeared to be accommodated within the dynamic of the relationship. Couple 2 express their feelings in the following dialogue: Roberta: We are always together, we talk a lot, watch movies together, take care of the house, (…) he helps me, we cook together, he makes the food, and I take care of other things, there is complicity between us. Pedro: Besides, we like to be together, right? I think that’s the main thing, right? There are always feelings, being together is nice, when you are apart, you miss them, you want to come back.
When this sense of couplehood was absent, communication and complicity between the spouses was difficult and they missed a sense of togetherness, as was evident when C3 Manuel talks about what he misses: What I miss between the two of us is chatting more, when a couple feels something, first they want to talk, like husband and wife, chat together (…)
Several couples talked about the importance of doing things together, and humor was expressed in several of the relationships, with spouses able to joke about loss of memory. Thus, the couples continued to build on their relationship, creating new stories and new experiences, individually and together.
Uncertain future
When asked about how they envisaged their intimate relationships in the future, the participants preferred not to dwell on the future, but to hold on to the present. it seemed the couples preferred to think that things would continue as normal.
The majority of couples understood that the sexual relationship dynamics would change, but this was attributed to ageing and the normal life course, rather than the Alzheimer’s diagnosis. In the case of C2, there was a certain anxiety about the future, and the hope that Roberta would be ‘cured’. This couple was the youngest in the sample, both in their sixties, Roberta had experienced little pleasure in her sex life, and imagined that she still might be able to enjoy sexual activity with her husband, whose only wish is that she get better. C2 Pedro: I only think about her getting better, I keep thinking that everything will return to normal, I do not think about anything else.
In general, the couples focused on their sense of ‘us’ and the importance of doing things together to maintain a sense of belonging. Their words reflected hope rather than resignation, and it appeared that the commitment of the marriage offered the support for a future together, albeit uncertain. In general, talking about the deterioration in the spouse’s health was avoided, evident in the following dialogue between couple C5: João: (…) we don't talk about bad things at home. Vera: We know things, right? But I pretend not to know (…) pretend not to hear. João: We are going to have some difficulties (…) but we hope that everything will work out, until we die. Vera: Me too, I will do everything to make us happy until the end of our lives, God willing. João: I would like her to get better, but this won’t happen, I feel she is changing. I respect her a lot, I would like her to get well, honestly, but she won't. According to medicine, this will get worse, not better.
It is evident that the couples are not used to talking about Alzheimer’s, rarely do they use the word Alzheimer’s or dementia but prefer to talk about memory failures or forgetfulness. Having the opportunity to talk about and reflect on how Alzheimer’s is affecting their relationship and their own subjectivity is a challenge, but at the same time a welcome opportunity to talk about what had been considered unapproachable. The illness tended to be reduced to a topic that should be addressed medically, not relationally. Thus, talking about dementia and sexuality, and the effects of such, was a new area for reflection for these couples. The tendency is not to link the two, perhaps with the hope that the illness might go away and life will return to ‘normal’.
Discussion
The long history of stereotyping of aged sexuality as being repressed or inactive has impacted the adequate investigation into the sexual needs of older people and people living dementia as they relate to policy, education and clinical guidelines. Nevertheless, more recent studies into sexuality and dementia are recognizing the importance of researching people in the early and middle stages of the illness to gain new insights into the significance of intimacy and sexual expression of those living with dementia (D’Cruz et al., 2020; Harris, 2009; Sandberg, 2020; Youell, 2015).
This qualitative study makes an important contribution towards acknowledging the need to include couples living with dementia in discussions about sexuality and intimacy and recognizes that persons with dementia are able to reflect on their own experiences and make important contributions. The willingness and openness of the couples in this study to talk about their intimate relationships highlights the importance of providing a safe environment where sensitive issues can be addressed and respected. This study contributes to the awareness that sexual and intimate activities of people living with dementia still have a place within the conjugal relationship even after the diagnosis and identifies the need to better prepare health care professionals to address these needs of this growing population.
The diversity in the findings from this study suggest that dementia does not always disrupt intimacy within loving relationships and challenges stereotypes about dementia and sexuality. The study draws attention to the importance of normalizing sexual activity and sexual expression for couples affected by Alzheimer’s and takes a step further in investigating sexuality and aging, to include a marginalized and neglected population, those living with Alzheimer’s.
An important aspect identified from this research was that the nature of the sexual and intimate relationship experienced today often depended on the quality of the relationship during the marriage. When a greater sense of ‘couplehood’ had developed over the years, then sexuality and/or intimacy continued to be expressed positively between the couples. The importance of cuddling, touching and feeling wanted and needed were identified by the couples as important aspects to maintaining a sense of ‘we’ within the relationship. Quality of life of both spouses is dependent on their personal couple histories, how they interact together, and how they are perceived within the couple relationship and their social context (Davies, 2011; Hernandez et al., 2019; Merrick et al., 2016). These findings are important for assisting in developing care practices that are couple-centered and inclusive.
This study permits us to identify elements that could improve the quality of the couple relationship throughout the illness. Inclusive measures adopted by care professionals that understand the importance of inquiring into the sexual activities of the couple, and. providing the couple with the opportunity to address any difficult areas, normalizing inquiries and conversations about such issues, may contribute significantly to improving the quality of the couple relationship over the course of the illness. Raising awareness about sexuality, sexual difficulties, expected changes in sexual expression during later life are important measures to help navigate the challenges that a dementia diagnosis presents to a couple.
This study was undertaken in (country), a culture that reinforces the stereotypical ageist attitudes and gender roles attributed to men and women, particularly with respect to sexual activity and sexual expression. From the research, it is evident that priority amongst the couples seems to have been given to the husband’s sexual needs, with penetrative sex acknowledged as the ‘gold standard ‘of sexual activity. The majority of the women’s experiences and their sexual expression was described as passive and subordinate, with little acknowledgement of their own sexual needs, irrespective of a dementia diagnosis. These expectations about sex, and the right to female sexual pleasure, particularly in later life, reflect and reinforce entrenched ageist and sexist norms (Gott, 2005; Sandberg, 2015). There is very little research and theorizing about older women’s sexuality, perhaps reflecting the difficulty of conceptualizing older women and those living with Alzheimer’s, as sexually desirable (Thorpe et al., 2018).
Further research and action are needed that contribute towards developing a greater understanding of the differing sexual and intimate experiences and expectations of men and women living with dementia in order to broaden concepts and an understanding of sex and sexuality beyond penetrative sex. More work is needed to educate health care workers to reflect on attitudes towards sexuality and dementia that contributes towards improving sexual health in older people with dementia. As observed by Hinchliff and Barrett (2018) this absence of positive discourses in relation to older peoples’ sexuality represents an added challenge to older persons being considered sexual beings, especially when the person suffers from dementia.
This study contributes to the growing evidence that some of the negative aspects of a dementia diagnosis may be delayed when the approach to caring includes an understanding of sexuality and sexual expression, and facilities its transformation throughout the disease.
Limitations
In our sample, couples had been married, on average, 49 years, with a range of 39–62 years; as such, there were no short-term relationships. This obviously raises questions regarding couples who do not have a long-term relationship and how dementia may affect their sense of commitment and togetherness. Furthermore, the sample was limited in that it only included heterosexual couples, which may influence the experiences captured in this study.
This study adopted the diagnosis of Alzheimer’s as the defining factor of the research, and did not focus on the specific age or gender of the diagnosed participants, nor how these variables could affect the results. Thus, there is a need for more research, both qualitative and quantitative, to explore the impacts of gender and age on the sexual behavior of couples living with dementia.
As with all IPA surveys, the results of this study cannot be generalized, but offer valuable insight into a sensitive and under-researched area, based on the participants' own words. Rather than assuming others in the early stages of Alzheimer’s will have similar experiences to those in this study, the results reveal the uniqueness and complexity of each participant’s experiences associated with the couple’s intimate sexual relationship when Alzheimer’s is present.
Conclusion
The results of this qualitative IPA study offer insight into how couples' intimate relationships are affected by Alzheimer’s Disease, in the early and middle stages of the illness. This study is one of a few that investigates the intimate behaviors of couples who continue to live in their own homes when one of the spouses has Alzheimer’s. The results provide a more in-depth view of these experiences based on the narratives of participating couples, and thus add to the growing interest in couples’ experiences of living with dementia. This study is part of a growing area of research that recognizes the importance of qualitative research on sexuality and sexual expression that explores the multifaceted and complex dimensions of sexuality for people with dementia and their spouses.
The findings in this current research contribute to the growing acknowledgement that a long term healthy relationship is a key factor in maintaining intimacy and feelings of love and togetherness, which help sustain couplehood during challenging times, such as with dementia, and may help to think about ways of negotiating intimate sexual changes as they occur (Harris et al., 2011; Hayes et al., 2009; Sandberg, 2020; Swall et al., 2019; Youell et al., 2016). From this research it was possible to observe that, for the majority of the participants, sexuality and couple intimacy continued to have a place within the conjugal relationship, despite the dementia diagnosis.
From this qualitative study we can observe that dementia does not significantly affect sexuality any more than normal ageing and that regular intimate and sexual contact can help maintain a positive caring relationship. These findings also add further support to the study undertaken by Tsatali and Tsolaki (2014), which concluded that despite age related changes, an increasing number of older persons with mild dementia continue to enjoy an active sex life. The results of this study also corroborated those of Eloniemi-Sulkava et al. (2002), which concluded that while sexual expression declined over time, a significant number of older persons remained sexually active several years after a dementia diagnosis.
Understanding the sexual needs of older persons with dementia within the framework of ageing and sexuality may help to challenge some of the taboos associated with sexuality and dementia. Sandberg (2013) questions the framing of elder sexuality in relation to youthful sexuality and suggests we should view the ageing process as the ‘continuous production of difference’ (p. 19). This approach understands the importance of viewing older sexuality on its own terms, and not as located somewhere within a hierarchy, with youthful sexuality at the top, and normalized as the reference for sexual performance. Dementia takes a lot away from couples and this study identified that couples living with dementia would significantly benefit from having a platform to talk about their sexual and intimate relationships, expressions and needs, in a climate that de-stigmatizes sex for older adults and where they can feel heard and receive support.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CAPES (Coordination for the Improvement of Higher Education Personnel), a Brazilian Foundation under the Ministry of Education.
Ethical Statement
This study received ethical approval from the Medical University of Jundiai. (C.A.A.E. 92888318.2.0000.5412).
The Brazilian Psychological Council’s ethical framework was adhered to, and all participants provided informed consent to the interviews, and rights to withdrawal and to anonymity were ensured.