
Abstract
Objective
The purpose of this investigation was to understand the dynamics among dementia caregiving, vigilance, and home and community-based service use.
Methods
This paper is derived from a larger, mixed-methods study on caregiving. We used a descriptive qualitative approach to analyze interview data of 30 family caregivers of relatives with dementia.
Results
We found five domains of vigilance in which caregivers felt “on duty”: ensuring attentiveness, ensuring safety, ensuring resources, ensuring healthcare, and ensuring closeness. Formal service use did not necessarily give caregivers relief from vigilance, with the language of risk often employed by caregivers.
Conclusion
Because service use could contribute to feelings of vigilance, rather than give caregivers a break from a sense of watchfulness, these findings support calls for dementia-specific training for service providers. In future caregiving research, the relationship between vigilance, caregiver distress, and role captivity should be explored.
Many family caregivers of persons living with dementia tend to develop a sense of watchfulness, or vigilance, to ensure that they are meeting the physical, psychological, and social needs of their family member (Mahoney, 2003). Vigilance is characterized by watching or being available to a person living with memory impairments or other cognitive problems associated with dementia (Krutter et al., 2020). On one hand, vigilance can give caregivers a sense of purpose as they ensure the comfort of their relative experiencing dementia symptoms (Parsons, 1997). On the other hand, over time, increasing and unrelenting vigilance can be psychologically burdensome as family caregivers become consumed with the demands of their caregiving role (Balbim et al., 2020; Kazmer et al., 2018; Saragosa et al., 2022).
Home and community-based services (HCBS) may have the potential to alleviate caregivers’ need for constant vigilance (O’Shea et al., 2019). Although there is a dearth of empirical evidence in the literature specifically addressing HCBS use in relationship to caregiver vigilance, other research suggest that respite provided by HCBS can reduce caregivers’ feelings of burden, stress, and other adverse psychological states such as anxiety and depression (Zarit et al., 2014). Yet the degree to which using HCBS provides caregivers relief from unrelenting vigilance is unclear (Falzarano et al., 2022; Laparidou et al., 2019), especially if caregivers or their relative living with dementia experience separation anxiety when they are not together (Coelho et al., 2020). The purpose of our study was to investigate the experience of vigilance and HCBS use among family caregivers of people living with dementia.
Caregiver vigilance
Mahoney (2003) identified five dimensions of vigilance common among dementia caregivers: watchful supervision, protective intervening, anticipating, on duty, and being there. Likewise, in a grounded theory study of family caregiving, Corcoran (2011) uncovered four styles of caregiving and theorized about the relationship between caregiver intentions and action within each style. Regardless of caregiving style, caregivers practiced vigilance. Three of the four caregiving styles identified (i.e., facilitating, advocating, directing) focused on the needs and wants of the care recipient, ensuring that the caregivers were engaged in constant vigilance. Specifically, facilitators engaged their care recipient in meaningful activities; advocators carefully monitored their relatives’ need for help and interactions with formal care providers; and directors were explicitly focused on the physical health of their relative. Yet even caregivers who had a balancing style (i.e., balancing their own well-being with that of the care recipient) engaged in supervision by using technological resources (e.g., remote monitoring device) and asking for help from others to interact with the person living with dementia when needed (Corcoran, 2011).
The relationship between vigilance and outcomes for family caregivers and their relatives living with dementia is unclear. Vigilance is associated with higher quality of care when caregivers anticipate the needs of their relative (Miron et al., 2019; Wackerbarth & Tarasenko, 2018). However, unrelenting vigilance, or difficulty of relinquishing one’s caregiving role even when relief is offered (Saragosa et al., 2022), can take a psychological toll on caregivers. For example, regardless of age or family role, caregivers often reported lack of good-quality sleep due to the pressure of being vigilant caregivers (Simpson & Carter, 2013), suggesting that a state of constant vigilance may be detrimental to caregivers’ psychological and physical health. Unrelenting vigilance may also result in poor outcomes for the person living with dementia. Grace et al. (2016) reported an association between high levels of vigilance among caregivers and use of psychotropics for their family members (e.g., Valium, Ativan), which are associated with higher rates of mortality for persons living with dementia.
Dementia caregiving and barriers to service use
Despite the potential for HCBS use to relieve feelings of unrelenting vigilance, as well as the practical benefits of having help, overall service utilization is low, with only about 22% of dementia caregivers using any type of service (Feldman et al., 2021; Parker & Fabius, 2020). Barriers to using services include cost, availability, resistance to outside help, and perceived quality of care.
Families in the U.S. needing services may be unable to afford the cost of HCBS, yet may not qualify for Medicaid supported services available for low-income, low-asset individuals (Norman et al., 2018). Additionally, Wolfe and colleagues (2016) found that caregivers who provided more help with healthcare (e.g., medication management) were more likely to use services than caregivers who provided limited or no healthcare-related help to relatives, supporting the view that as the medical needs of persons living with dementia increase, so does the use of HCBS (Parker & Fabius, 2020; Saragosa et al., 2022). However, how receiving help with healthcare tasks relates to caregivers’ feelings of vigilance is unclear.
HCBS, such as personal care services, Adult Day Services [ADS], and short-term respite in long-term care facilities, are intended to provide relief from the demands of caregiving. Caregivers often face barriers to service use including lack of awareness of services (Bayly et al., 2020), cost (Henning-Smith et al., 2019), and availability (Macleod et al., 2017). Other barriers, such as a person’s resistance to care, are more personal and complex (Black et al, 2019). For example, ADS use typically relieves caregivers’ psychological distress (Bangerter et al., 2021; Maffioletti et al., 2019); however, when a person living with dementia objects to attending an ADS program, or does not want a personal care aide in the home, caregivers may defer to their parent or spouse and honor their care preferences (Roberto et al., 2021). In these cases, a person’s resistance to care can be barriers to service use, interfering with caregivers’ attempts to get relief from constant vigilance.
Another infrequently addressed barrier to using HCBS is that service use may be an additional source of perceived stress and risk for caregivers. Informal caregivers need to feel that when they involve paid caregivers their relative will receive appropriate attention and assistance (Saragosa et al., 2022). A common barrier to using services is the perceived lack of professional competence and appropriate supervision of the person living with dementia (Moon, 2016). Family members may worry that their relative will be neglected or exploited by people they do not know coming into the home (Macleod et al., 2017). Thus, rather than seeing HCBS as a means of relief from their vigilance, family caregivers may worry about potential risks of using services and maintain or increase their vigilance instead.
The purpose of this investigation was to explore the concept of vigilance among dementia family caregivers who used HCBS. Analyzing in-depth interviews with 30 dementia family caregivers, we asked: (1) In what care domains do caregivers feel they should be vigilant? and (2) What role does HCBS use play in alleviating caregivers’ feeling that they must be constantly watching over their family member living with dementia?
Methods
The data for this research came from a longitudinal, mixed-methods study of dementia family caregiving (Savla et al., 2022). We recruited family caregivers from a regional healthcare system and the five Area Agencies on Aging in the sampling locale who were listed as the contact person for an older adult diagnosed with dementia (see Savla et al. for full recruitment details). In addition, caregivers all answered affirmatively to the following question in a short eligibility phone call: “Are you the main person caring for your family member who has been diagnosed with memory issues or dementia?”.
The caregivers lived the Appalachian region of Virginia, an economically disadvantaged region of the United States. Generally speaking, people of the Appalachian region are considered an underrepresented group in healthcare by the National Institutes of Health. HCBS in this rural region are a complex mix of publicly-funded and privately-paid resources, depending on town/county location (i.e., historically impoverished areas are eligible for additional federal funding), as well as need and income of persons living with dementia. Typical HCBS available in this region includes meal delivery, personal and respite care, ADS (limited availability), physical therapy, and housekeeping.
For Phase 1 of the study we interviewed 124 family caregivers (Savla et al., 2022). Approximately 2 years later (September through December 2019), we conducted face-to-face follow-up interviews with 30 caregivers. The aim of the Phase 2 interviews was to learn more about the caregivers’ use of HCBS (see Roberto et al., 2021). For the current analysis, we focused on the in-depth interviews conducted in Phase 2 only, when we spoke with caregivers, usually meeting in their homes (occasionally at a public place). To guide the interviews, we used a semi-structured interview protocol (see supplementary material).
Ethics
The 30 interviews were transcribed verbatim, and pseudonyms were used to protect participant privacy. Identifying details have been excluded or changed in quotations used in this paper. The interviewer obtained written consent from participants prior to recording the interviews. This study was approved by the Virginia Tech IRB.
Sample
We used a purposive, maximum variation sampling method to select the caregivers invited to participate in Phase 2 of the study [see Roberto et al., 2021 for rationale and details on sampling method]. Consistent with our analytic method discussed below, we rank-ordered all caregivers interviewed during Phase 1 based on region, race, and relationship to the person living with dementia to ensure the inclusion of underrepresented caregivers in the vigilance analyses. Because we were interested in service use, we also prioritized caregivers who during the Phase 1 interview said their relative had moderate memory and behavioral issues, assuming these caregivers would have a greater need for help by Phase 2 (either paid or informal).
Data analysis
To analyze the data, we used a qualitative descriptive approach (QDA; Kim et al., 2017). QDA has roots in phenomenological healthcare research and, typically, is descriptive rather than theoretical. QDA depends on purposeful sampling to better understand the phenomena in question (i.e., vigilance and service use). We employed coding methods from grounded theory, which is consistent with QDA’s flexible approach to employing techniques from other methodologies (Kim et al., 2017). Grounded theory’s iterative coding process assured us that the emergent patterns were well represented in the data and contributed to a deeper understanding of how caregivers of family members with dementia experience service use in relation to need for vigilance.
Open coding
For the first step of analysis, we open coded the entire dataset (N = 30) using Atlas.ti (v. 8) qualitative data management software. Members of the research team first read through the data set and made jottings (i.e., a list of possible codes derived exclusively from the interview data). On a second read-through of the interviews, we began organizing the jottings into codes. Then we applied the initial coding scheme to four interviews independently and met to discuss our coding. We used this constant comparison method, meeting to discuss any inconsistencies until we reached full agreement. After this iterative development of the coding scheme, McCann applied the final scheme to all 30 interviews. Then Blieszner and Atkinson verified the coding, and the team resolved any discrepancies on a case-by-case basis. We used four overarching categories from the interview protocol to organize the codes: Caregiver (subcategory examples: Secondary Stressors, Management Strategies); Person Living with Dementia (subcategory examples: Daily Routines, Behavior Problems); Support (subcategory examples: Changes in HCBS, Service Type); and Culture (subcategory example: Community Caregiving Norms). Note that a given quotation could encompass multiple codes.
Focused coding
Examples of coding procedure.
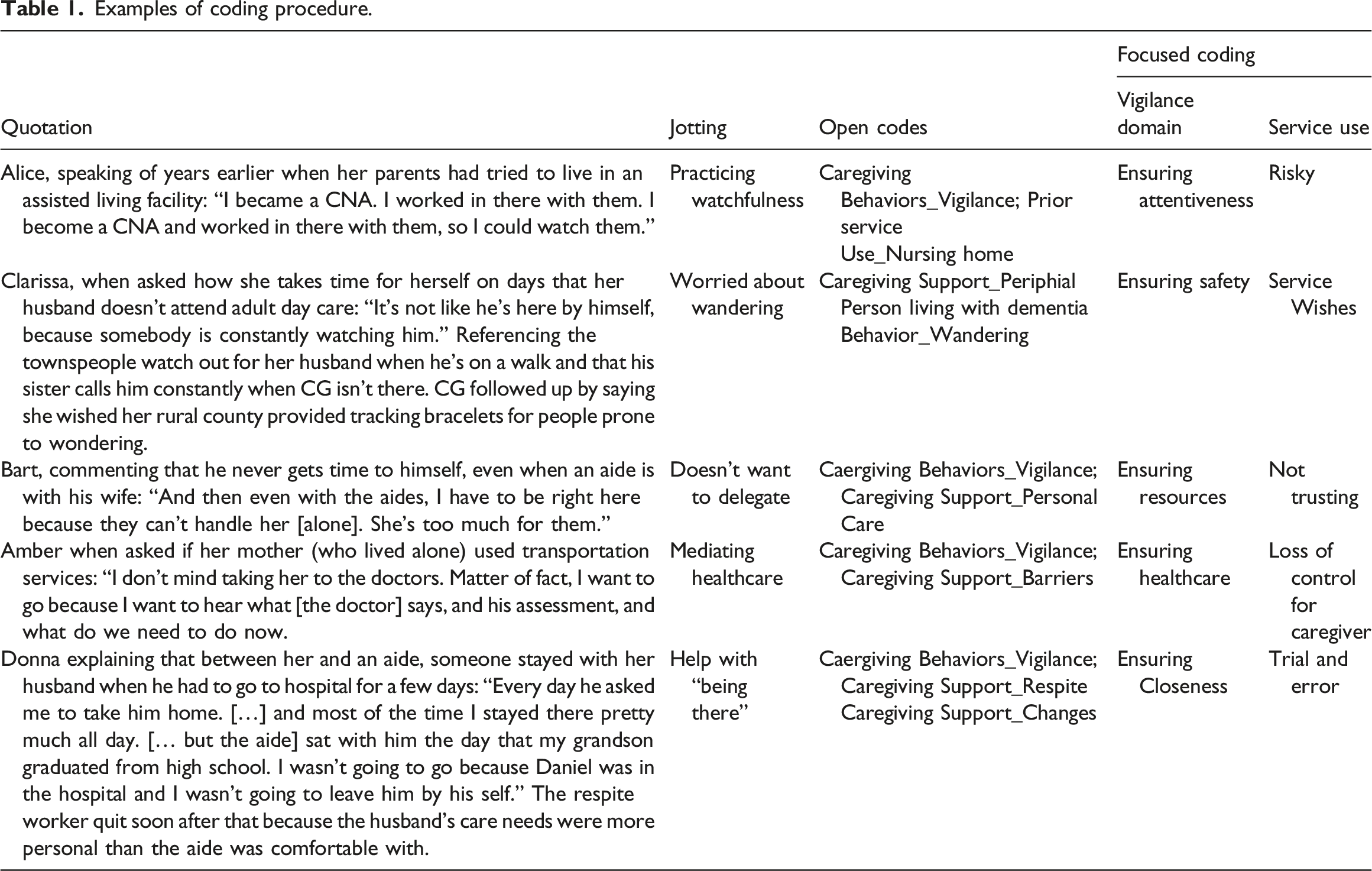
Furthering our analysis, we noticed a pervasive concern of risk across domains of vigilance. Developing theoretical memos, we then considered the relationship between vigilance and risk as a barrier to service use, investigating the ways in which caregivers conceptualized service use as risky. That is, rather than investigating why participants used or did not use particular services, we focused on caregiver’s perceptions of both current and previous experiences with formal services. Although our questions (see Supplement) were specific to HCBS, similar to Carr’s (1998) work on family vigilance in institutional settings, participants took a more wholistic view and often shared their relatives’ experiences with temporary stays in skilled nursing and assisted living facilities as well. Notably, perceptions of services were often conflated with experiences with Certified Nursing Assistants (CNAs). Typically earning minimum wage in our study area, CNAs are employed by skilled nursing facilities and home health care agencies (both public and private), and are hired by individuals in the community. Depending on their employers’ needs, CNAs’ tasks might include any one or up to all four of the following: help with personal care, basic housekeeping, respite, and companionship. Although we asked only about HCBS, the family caregivers, some of whom had been CNAs themselves in both home and institutional settings, conceptualized service use more broadly.
Findings
Overview
Participant characteristics.

Note: Income (US dollars): High = Above $50, 000, Low = $20,000 or below; Non-Medical Help at Home = Housekeeping, Respite, Personal Care, Home Repair; Medical Help at Home = Home Health Nurse, Physical Therapy; Educational = Support Group, Social Worker, Dementia Class; Help Away from Home = ADS, transportation.
Considering our research questions, we found that caregivers identified multiple domains in which they were vigilant. Avery, who lived near but not with her mother, offered a typical comment: “I want a life. I have a life, and it gets kind of stressful, trying to do what I want to do and take care of her at the same time. I don't want to be here, just on call all the time.” Nevertheless, HCBS use often did not give caregivers relief from the feeling that they must be constantly watching over their relative. Rather, service use could be a risky proposition with over one-third of the caregivers (n = 11) explicitly using the language of risk as a barrier to service use, and others implying that service use was risky when telling stories about previous experience with services.
Domains of vigilance
We identified five domains of vigilance ensuring: (1) attentiveness, (2) safety, (3) resources, (4) healthcare, and (5) closeness. Although we analyzed data from all 30 participants, the quotes used to illustrate each domain were from caregivers who had experience using services (n = 28) to highlight the relationship between service use and feelings of vigilance. Caregivers often described more than one type of vigilance; thus, the numbers reflect the extent to which each category was saturated, rather than mutual exclusivity.
Ensuring attentiveness
Nearly two-thirds (n = 19) of caregivers talked about a general need for watchfulness because they felt a fear of neglect or the risk of leaving their relative with others or alone. For most of her caregiving trajectory, Bryne had been the primary caregiver for her father, but had lived in her own home. Explaining why she moved in with her father between the parent study and Phase 2 of our study, Bryne said, “So I decided it was just easier to just move in. … It was easier, and I knew how he was taken care of, and I knew things weren't going to disappear and things like that.” Bryne’s description reflects the views of other participants who noted that it was less stressful to do nearly everything themselves than to go through the trial and error of finding trustworthy paid help.
Bart echoed these feelings and mentioned times when having help made caregiving more stressful. Like Bryne, learning to trust personal care workers was difficult for Bart, as he was concerned that he and his wife might be exploited. I found that [it] was kind of like bothersome [because] there was so many people and so many aides, and this one coming and that one going, and you’re watching out for the trust. Who can I bank on? Who can I leave with Miss Betsy? How do I know that I'm not going to get taken? You know, all these things. ... But I always try to make sure I’m right here with the aides unless I have to go, and I’ve learned to trust. When they first started, I had a real lack of trust because … Betsy and I were so close.
For Bart, developing trust of hired caregivers was a long process, and he avoided leaving his home when he first started receiving services for his wife. It was part of his commitment to Betsy to ensure that she received proper care. Likewise, in speaking of finding a personal care aide through an agency, Blaire said, “I’d still want hands-on. … I don't want [personal care aides] in my house to begin with. Because they send some real jewels. They … send these young girls that just sit on their phones and play all day long.”
Other caregivers took jobs at nursing homes when the person with dementia went for a rehabilitative stay so that they could watch out for their family member and ensure suitable care. Others maintained constant contact, like Christopher who stayed with his mother most of the day when she went to a nursing home following hospitalization. He explained that the facility had a bad reputation in the community; after spending time there ensuring his mother’s care, he assessed that the facility was short-staffed. Christopher felt that the staff took a long time to respond to the needs of his mother and others, not because they were ill-intentioned, but because the staff had more work to do than they could manage. Similarly, about half of the caregivers spoke about insufficient staff at facilities or, for care at home, mentioned that their relative needed more than one person with them most of the time.
Ensuring resources
Caregivers felt that they needed to be vigilant to ensure that they had enough trained help balanced with what they were able to afford. Financial concerns factored in due to the complex nature of how service costs are paid; payment for services could be public, private, or a mix depending on the recipient’s family resources. In addition, training care workers on the specifics of the family’s needs was an investment of both time and money. Caregivers weighed these factors in determining whether they wanted to begin the process of finding or retaining current help.
Complicating matters, caregivers reported the need to be continuously training personal care workers because of the high turnover that often occurs. Dorothy, whose mother needed two caregivers at all times, explained that one of her personal care aides, Dawn, had taken a leave of absence because someone in her own family needed care. She originally met this personal care aide through an agency. After a while, and against their contract with the agency, Dorothy hired Dawn privately and increased her pay. Then unexpectedly, Dawn had to take a leave of absence due caregiving needs in her own family. Dorothy explained: So now, I’ve had to hire somebody [to replace Dawn]. I’m back to training somebody else, and who knows how long before [Dawn] gets back. This is what happens. The people that are helping me are my age, so they’re going through the exact same experience that I am. And [another personal care worker, Dana, needs to be available for her father who had to have surgery and she couldn’t work during that time]. You see what I’m saying? … It’s just a constant. There’s always something, so you never get ahead. You never get ahead. I still haven't had a vacation in [six years].
Dorothy’s comments highlight the changing nature of using home care even after trust has been established. Family caregivers may find wonderful, trustworthy helpers, but lose them due to unforeseeable circumstances and must begin the process anew with a different person.
Carrie, whose family paid for services out of pocket, shared that in addition to the financial burden of having paid help, she had been taken advantage of by personal care workers to whom she gave pay advances: You’re taking a risk when you bring somebody in your home. You don’t know who they are. They have to basically fit in with your family, and that’s hard. You don't know who might take advantage of that. We’ve been burned twice. We’ve had three [personal care workers], and we’ve been burned twice. The risk is there. It just makes you nervous. That’s another stressor on top of [what you’re already dealing with].
Carrie had one trusted personal care worker, and indicated she was looking for one more person to help.
Ensuring safety
Fifteen caregivers spoke of ensuring the safety of the person living with dementia, specifically related to falls, accidents, and wandering. When we asked Aiden about the most challenging aspect of caregiving for his wife who had many physical limitations in addition to dementia, he said, “There’s a constant worry of, is she going to move around, maybe fall? In other words, it's this feeling that you have to watch constantly.” He felt that he or a care aide needed to always have their eyes on his wife, even if she was sitting in her chair watching TV. His concern was common among caregivers whose relatives living with dementia had physical limitations.
Others were concerned about safety due to wandering. Alexandria, who lived about a quarter of a mile from her parents on a country lane, discussed how having her mother attend the local adult day services (ADS) helped reduce the need for constant vigilance. When her mother was at ADS, Alexandria did not have to worry about her mom wandering the roads alone. You can’t leave [mom] at home by herself. Before [mom and dad] ever started going to ADS, Dad would go outside, … and he’d tell her before he went outside where he was going, but then 5 minutes later she’s […forgot and didn’t see him outside]. She came down the road walking one day; she didn’t know where he was. I had to take her back up there and he was right there beside the house.
Later in the interview, Alexandria said that even after her parents started attending ADS regularly, she felt guilty for not being at her parents’ house all the time. She wanted to honor her parents’ wishes to live in their family homeplace independently, but worried that her father did not take proper precautions given her mother’s worsening dementia. When we spoke to her in Phase 2, she was increasingly watching not only her mother, but also her father whose physical health had begun to deteriorate.
Adeline, a spouse caregiver, indicated that making home modifications provided more help than having formal services. Her husband, Aaron, was prone to wandering, and a personal care worker quit because she did not like being confined to the property. Before the care worker got involved, Adeline solved the problem of Aaron’s wandering by installing a lock on the fence gate. When Adeline was running errands one day, the care worker could not open the lock, which made her very upset. Afterwards, the care worker told the agency she did not want to return to help with Aaron. Adeline believed that the care worker did not understand the danger of Aaron’s wandering and as a result, lost faith in having paid helpers. Afterwards, Adeline only ran errands when her adult daughter could be at the house to ensure Aaron’s safety. She said she still qualified for help but did not want to have a similar episode with another care worker.
Ensuring healthcare
Twelve caregivers spoke of vigilance specifically relating to healthcare concerns such as medications, eating and drinking, and doctor visits. Caregivers typically practiced hands-on management of these tasks, such as organizing medication and going to doctor visits, to ensure their relative’s health was optimal. Even if they did not personally manage all these tasks, they used other means to confirm that their relative’s health needs were being met. For example, some caregivers asked helpers (paid or informal) to write down what they did during their visit so that there was a record of medications taken and meals eaten.
Claudia reflected on her belief that paid care workers do not provide the same level of healthcare that she does. Speaking of her daughter who taught her how to do caregiving, Claudia said: If I didn’t have [my daughter], I wouldn’t have done it [be the caregiver]. [Mom] would’ve been in a nursing home and she would’ve probably been dead because [the nursing staff] couldn't have done what I do. [Mom] gets dehydrated a lot because she won't drink, and you have to really sit there, and it takes 45 minutes to drink a cup of something and it’s really frustrating. It’s like, “Just drink it.”
Counterintuitively, later in the interview, Claudia mentioned that she got too much formal help in the beginning of her caregiving journey and had to scale back because managing so many different people in the home made it difficult to keep up with who was coming and going in her home. Claudia was spending more time managing people than ensuring that her mother’s needs were being met. Her comment confirms the notion that managing an overabundance of formal assistance can also be viewed as burdensome rather than helpful and suggests caregivers’ need for increased help with care coordination.
Ensuring closeness
Formal services could not replace the interpersonal impetus for vigilance (i.e., ensuring emotional closeness). Although not a deeply saturated concern across the interviews, six caregivers, four of whom where spouses, spoke about how their relative, or they themselves, wanted to be close by for emotional reasons. For example, Bonnie, who had been waiting to get help at home because of the lack of personal care workers locally, weighed her options. She said, “If I put him in a facility and I'm not there every day or every other day … That’s his fear is that he is just going to end up somewhere and nobody is going to come [visit]." In contrast, Caylee, who has been married to her husband for 56 years, said that she visited him nearly every day during his short-term nursing home stay because she felt so lonely without him at home. The risk of using services here was not about having something stolen or fearing for the person living with dementia’s safety; it had more to do with facing emotional loss when the caregivers were not personally providing care for their relative.
Discussion
The literature on dementia family caregiver vigilance is limited; therefore, the purpose of our study was to investigate the domains in which caregivers’ feelings of vigilance were most salient. We also wanted to understand the role that service use played in possibly alleviating caregiver’s sense that they must be always “on duty” even when they are not doing tasks for their relative living with dementia. We theorized that when caregiving required constant supervision, caregivers would rely on HCBS and see a reduction in their feelings of vigilance. However, that was not the case. Often services contributed to caregiver vigilance rather than alleviating it. The relationship between caregiver vigilance and formal service use was not straightforward. Rather, supportive services—such as personal care, homemaking, or ADS—were characterized as potentially risky and used on and off throughout caregiving journeys as relatives tried to find services that were high quality and relevant to the specific types of help the caregivers needed to care for their relative living with dementia.
Similar to the findings of Mahoney (2003) and Corcoran (2011), caregivers in our study discussed pervasive feelings of vigilance in every domain related to caregiving. Whereas Mahoney examined dimensions of vigilance, that is, the ways in which caregivers practiced vigilance (e.g., intervening, anticipating needs), our focus on the domains of vigilance (e.g., attentiveness, resources, healthcare, safety, closeness) advances understanding of how HCBS use might provide caregivers relief from constant vigilance, or alternatively add to caregivers’ sense of watchfulness.
Reasons for service use or nonuse among dementia caregivers are complex and cannot be predicted by need, availability, and cost alone (Feldman et al., 2021; Laparidou et al., 2019; Parker & Fabius, 2020). Caregivers in our study typically needed to monitor several aspects of HCBS (and care within short-term stays in facilities), including the quality of care provided by personal care workers. Even when the caregivers and their relatives living with dementia trusted their personal care aides, the workers had to be trained on the specific needs of dementia care, supporting O’Shea and colleagues’ (2019) argument that respite must be restorative, relational, and centered on the people living with dementia as well as caregivers. Caregivers were happiest with services when they felt that HCBS providers were as vigilant as they were, such as with ADS or a trusted personal care worker who had a friendly relationship with the person living with dementia (i.e., vigilance associated with ensuring attentiveness, ensuring resources, and ensuring closeness). Task-related vigilance associated with ensuring safety (e.g., watching for wandering) and ensuring healthcare (e.g., administering medications) could be delegated to HCBS more readily; but even then, caregivers wanted to be sure services would provide the same level of watchfulness as they did.
Limitations
While findings of our study contribute to the understanding of caregiver vigilance, we recognize their limitations. First, we focused only on caregivers in the Appalachian region of Virginia, a relatively homogenous population. Future research with diverse populations is needed to identify individual and situational factors that contribute to acts of vigilance, such as structural conditions (e.g., racism) or personality variables (e.g., connection between anxiety and vigilance), as well as the impact of daily caregiving vigilance on well-being for both caregivers and persons living with dementia.
Second, our analysis focused on a single point in the caregiving journey. Whether a caregiver’s feelings of vigilance change over time or in relation to their relative’s dementia progression is unknown.
Finally, we focused on vigilance especially in relationship to HCBS service use. Our findings suggest that vigilance should be studied as a key mediating variable influencing well-being and feelings of burden during transition points on the caregiving trajectory (Balbim et al., 2020), and as an outcome variable in assessing the impact of caregiving (Gallagher-Thompson et al., 2020).
Research and practice implications
Spouse and adult child caregivers often are reluctant to characterize the work of caregiving as burdensome (Mahoney et al., 2003); thus, focusing on vigilance may be a helpful way to foster discussion of caregiving challenges. Counselors and mental health providers should consider why caregivers feel the need to be constantly vigilant as they develop recommendations for care management, using the five domains of vigilance we identified (e.g., attentiveness, safety, resources, healthcare, and closeness). Caregivers may need help in learning to balance service use concerns with their relative’s and their own well-being (McCormack et al., 2017). For example, Kazmer and colleagues (2018) found that after a cognitive behavioral intervention, caregivers in their study began asking others in their social networks for respite help. Becoming comfortable with taking small risks and asking for help might enable them to develop trust in paid support providers.
Wackerbarth and Tarasenko (2018) argued that interventions should invoke some caregiver vigilance with respect to planning for the future care of their relative living with dementia. Drawing on our findings and the work of Mahoney et al. (2003), we recommend that practitioners assess caregivers for signs of unrelenting vigilance to determine not only for what help caregivers may be qualified, but also what kind of assistance would reduce feeling the need for constant vigilance. For example, Mahoney et al.’s Caregiver Vigilance Scale asks caregivers about their relatives’ ability to be alone, but does not tap into the relationship between primary family caregivers and paid care aides. We suggest adding questions such as: “How long can your relative with dementia be left alone with a care aide or another family member (not primary CG)?” and “For how many hours a week would you (CG) be comfortable with “good enough” respite care?”. It is not enough to assume that service use translates into relief of unrelenting vigilance.
In sum, unrelenting vigilance is arguably related to system level factors, multiple providers, inconsistent providers, and quality of care concerns that are beyond caregivers’ control, yet contribute to the daily stresses and strains of caregiving (Laparidou et al., 2019). Our findings support efforts to professionalize dementia care workers who support and assist family caregivers (e.g., Drake, 2020; Foley & Luz, 2021) so that getting help does not feel risky or burdensome. Too often employing hired help is conceptualized as having a “sitter” rather than acknowledging the psychological and physical skills involved in assisting a person with significant cognitive decline (Scales, 2021). Often this work is invisible or deemed inconsequential until the load of managing everything, including being vigilant towards hired care aides, becomes unbearable for primary informal caregivers. Additionally, as our participants noted, care aides are often underpaid; with increased professionalization should come increased compensation. Our findings show that caregivers need and value dependable, trustworthy hired help and point to improvements in the HCBS system that would support continued care provision for their family members living with dementia.
Supplemental Material
Supplemental Material - Vigilance, risk, and service use among caregivers of people living with dementia
Supplemental Material for Vigilance, risk, and service use among caregivers of people living with dementia by Brandy Renee McCann, Karen A Roberto, Rosemary Blieszner, Jyoti Savla and Emily Atkinson in Dementia
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Aging at the National Institutes of Health (R21AG054682).
Ethical approval
Our study was approved by the Institutional Review Boards at Virginia Tech (#19-627) and Carilion Clinic (#2284). All participants provided written informed consent prior to in-person interviews.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.