
Abstract
Meaningful engagement is a key dimension of quality of life among persons living with dementia, yet little is known about how to best to promote it. Guided by grounded theory methods, we present analysis of data collected over a 1-year period in four diverse assisted living (AL) communities as part of the study, “Meaningful Engagement and Quality of Life among Assisted Living Residents with Dementia.” Our aims are to: (a) learn how meaningful engagement is negotiated among AL residents with dementia and their care partners; and (b) identify how to create these positive encounters. Researchers followed 33 residents and 100 care partners (formal and informal) and used participant observation, resident record review, and semi-structured interviews. Data analysis identified “engagement capacity” as central to the negotiation of meaningful engagement. We conclude that understanding and optimizing the engagement capacities of residents, care partners, care convoys, and settings, are essential to creating and enhancing meaningful engagement among persons living with dementia.
Keywords
Background
Maintaining access to meaningful activities and experiences to the highest degree possible is essential for quality of life and quality of care of persons living with dementia (Adlbrecht et al., 2021; Burgess et al., 2022; Fazio et al., 2018). Engagement is meaningful when the “the act of being occupied or involved in an external stimulus” (Cohen-Mansfield et al., 2009, p. 2.) provides value to or spurs interest of the person involved. Meaningful engagement and interaction are vital to well-being and are potentially effective non-pharmacological strategies for addressing negative behavioral and psychological expressions (e.g., anxiety, depression, apathy, agitation, and aggression) (Mansbach et al., 2017). People living with dementia typically want to participate in activities, including leisure activities, that bring them joy and allow them to contribute (Genoe & Dupuis, 2014). Prolonging meaningful engagement and access to everyday activities and routines that maximize choice and control are important for quality of life amongst people living with dementia (Bamford & Bruce, 2000; Genoe & Dupuis, 2014). Engagement can improve social connection, personal autonomy, physical health and mental stimulation (Phinney et al., 2007; Roland & Chappell, 2015). However, opportunities for meaningful engagement among this population often are limited, especially as a person’s dementia progresses (Kontos et al., 2021). Lack of meaningful engagement contributes to loneliness, isolation, and depression and can hasten physical and cognitive decline (Anderson, 2019; Cohen-Mansfield et al., 2009).
Assisted Living (AL), a major provider of residential care for persons with dementia in the United States, includes residential care that is state-regulated, provides at least two meals per day and 24-hour supervision, and in most states, prohibited from providing skilled nursing care (Zimmerman et al., 2022). Residents in AL face challenges staying meaningfully engaged. Potential limitations to meaningful engagement in AL include those related to residents’ physical and cognitive function, staff shortages and turnover, limited skills and training of care partners (i.e., staff, family members, friends, and other care providers), obstacles related to the physical environment (e.g., crowding, noise, inaccessible public space, limited privacy) and lack of individualized activity programming (Bender et al., 2021; Holopainen et al., 2019; Mmako et al., 2020; Vandenberg, et al., 2018). In some cases, staff receive training but lack the resources to develop and engage residents in meaningful activities (du Toit et al., 2020). In addition, social environments can contribute to exclusion and marginalization of some residents with dementia especially as their cognitive function declines (Kemp et al., 2012; Perkins et al., 2012).
Limited opportunities for meaningful engagement and associated health risks worsened during the COVID-19 pandemic, particularly in AL and other long-term care settings where residents were sequestered and denied in-person contact with family, friends, and others (Masterson-Algar et al., 2022; Simard & Volicer, 2020; Suarez-Gonzalez, 2020). As we strive to recover from the pandemic’s detrimental effects and the number of persons living with dementia rises, it is critical to learn how to promote meaningful engagement.
Sensitizing Framework
We present analysis of data from the grounded theory (GT) study, “Meaningful Engagement and Quality of Life among Assisted Living Residents with Dementia,” (R01AG062310 to Kemp), which seeks to identify best care practices aimed at recognizing, creating, and maintaining optimal meaningful engagement. Informed by Corbin and Strauss’ (2015) interpretive GT method, we use prior knowledge as a sensitizing framework (see also Sebastian, 2019), including the Convoys of Care model (Kemp et al., 2013), which derives from a synthesis of theory and previous AL research. This holistic care model places AL residents at the center of the care process, emphasizes the study of relationships, partnerships, and interactions, and, drawing on a socio-ecological perspective, recognizes the contexts that surround and potentially influence care. Consequently, care relations and interactions, including engagement, should be studied in-depth and longitudinally and with a focus on meaning, experience, and relational and contextual influences. Further, achieving a comprehensive understanding of meaningful engagement requires the inclusion of multiple perspectives, in this instance, persons with dementia and the evolving collection of formal and informal care partners who provide support and comprise residents’ care convoys (i.e. networks), including AL staff, residents’ family and friends, volunteers, and external providers. Thus, in addition to directing research attention to stakeholder perspectives and surrounding contexts, the model also informs the study’s design, methods, and analytic approach.
Prior analyses of study data revealed substantial variation in opportunities for and experiences with engagement among residents with dementia (Ciofi et al., 2022; Kemp et al., 2021) and also contribute to our sensitizing framework. We initially identified key approaches used by care partners who successfully promoted meaningful engagement: (1) knowing the person (e.g., understanding likes, dislikes, habits, social history); (2) connecting with and meeting persons where they are (e.g., joining people in their realities; not arguing); (3) being in the moment (e.g., pivoting, adjusting to the situation); and (4) viewing all encounters as opportunity (e.g., seeing every interaction as potentially significant) (Kemp et al., 2021). Subsequent analysis focused on residents’ experiences going outside or offsite found that doing so was meaningful and important for quality of life among most, but not all, residents with dementia (Ciofi et al., 2022). Both analyses advanced knowledge of engagement among persons living with dementia. Yet, neither holistically examined meaningful engagement by taking into account how it arises within the conditions and contexts of daily life and care routines.
Aims
In this analysis we seek to provide an in-depth holistic understanding of meaningful engagement. Our aims are to: (a) learn how meaningful engagement is negotiated among AL residents with dementia and their care partners, including how opportunities become meaningful experiences; and (b) identify how to create these positive encounters. Consistent with Corbin and Strauss’ (2015) GT approach, our methods involve researchers engaging with and interpreting data with the ultimate goal of identifying processes linking structure and other phenomena together and constructing theory. Gaining theoretical understanding based on residents’ and care partners’ lived experiences is important for advancing research and designing effective programs and policies aimed at promoting meaningful engagement.
Methods
Study Sites, Data Collection, and Participants
Select Characteristics and Data Collection Details by Study Community.

Responses to people, activities, and other stimuli. Following grounded theory, data collection and analysis took place simultaneously and informed one another.
We varied visits by day of the week and times observing both structured (e.g., mealtimes, activities) and unstructured activities (e.g., family visits, spontaneous engagement) throughout each community. Researchers documented observations in fieldnotes noting for example, residents’ engagement opportunities, care partner interactions, and their verbal and non-verbal communication.
Select Resident Participant Characteristics by Community.
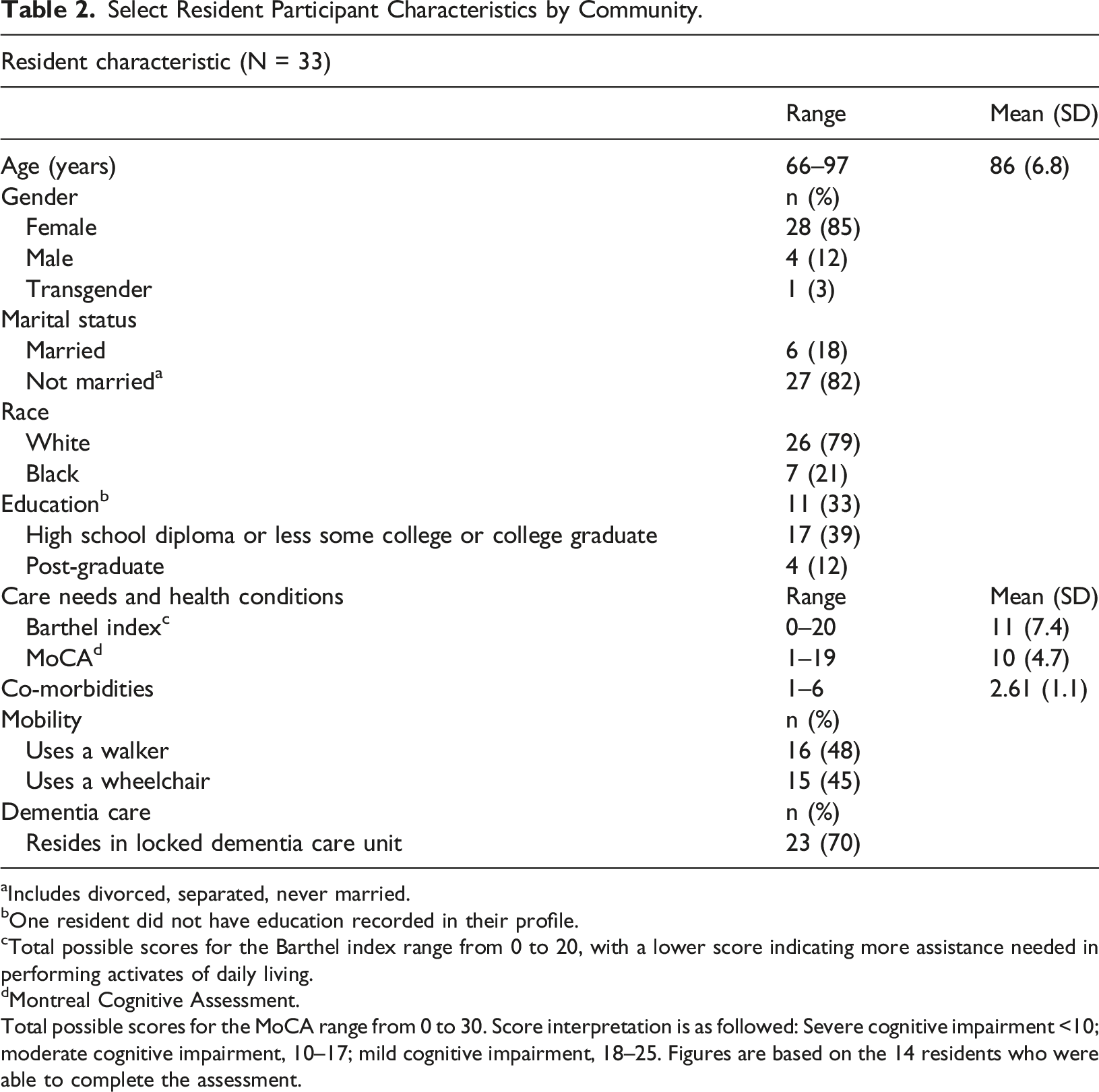
aIncludes divorced, separated, never married.
bOne resident did not have education recorded in their profile.
cTotal possible scores for the Barthel index range from 0 to 20, with a lower score indicating more assistance needed in performing activates of daily living.
dMontreal Cognitive Assessment.
Total possible scores for the MoCA range from 0 to 30. Score interpretation is as followed: Severe cognitive impairment <10; moderate cognitive impairment, 10–17; mild cognitive impairment, 18–25. Figures are based on the 14 residents who were able to complete the assessment.
Care partner participants by type.

aIncludes three Registered Nurses (1 Executive Director, one Resident Care Director, and one Hospice Nurse).
bWe interviewed at least one informal care partner associated with each of the 33 resident participants.
Includes niece, friend, or volunteers.
Select Study Characteristics.

Credibility
In qualitative research validity and reliability are subsumed under the concept of credibility (Patton, 2015), which depends, in part, on rigorous techniques for data collection and analysis. The credibility of our data was achieved through the standard techniques of prolonged engagement, negative case analysis, triangulation, and member-checking (Lincoln & Guba, 1985). Prolonged data collection facilitated a heightened in-depth and longitudinal understanding of individuals and settings. Triangulation included reliance on multiple data sources, perspectives, and investigators, and member-checking. Our 19-member research team (see Table 4) met twice monthly to discuss observations, new lines of inquiry, and insights. Each researcher memoed their theoretical and methodological insights from data collection and coding. Member-checking activities involved discussions with participants throughout our data collection and analysis processes to present and validate our interpretations. Finally, we created resident and care community profiles to facilitate in-depth understanding and comparisons across residents and settings over time.
Analysis
We stored and managed our data in NVivo (QSR International), a qualitative analytic program, which also facilitated coding and analyses. We coded throughout data collection using codes derived from our aims, existing research, and observations. Examples include: “nature of activity,” “resident response,” “resident factors,” and “care partner factors.” These codes represented broad categories that enabled the multi-pronged coding (Corbin & Strauss, 2015) described below (see also Table 4).
During initial coding, we reviewed and coded data relevant to our present research aims. Example initial codes included, “missed engagement,” “care partner strategy,” and “resident enjoyment/pleasure.” Next, using axial coding we connected initial codes to codes designating conditions and contexts, including influential factors. For instance, we found that care partners’ dementia knowledge, communication skills, engagement resources (social, material), and assumptions about residents’ skills shaped engagement strategies. Combined, these care partner influences impacted resident engagement opportunities and experiences and responses. Similarly, we found that resident influences such as interests, mood, care needs, and function influenced engagement. We also found interaction between resident and care partner influences and those in the setting. During selective coding, we refined and integrated codes across residents and sites, organizing our concepts around the core category, “engagement capacity.”
Findings
Engagement opportunities among residents with dementia ebbed and flowed throughout and across days, months, and seasons. We documented solitary, one-on-one (i.e., resident and another individual), and small- and large-group activities. Opportunities were active (e.g. exercise, games) and passive (e.g., reading watching movies or listening to music), scheduled (i.e., based on an activity calendar) and unscheduled (i.e., unplanned/spontaneous), and largely facilitated by AL staff, family, friends, volunteers, external care workers (e.g., hospice aides, therapists), and other providers (e.g., musicians, salon workers). Despite commonalities across settings, engagement experiences varied widely. Our core category, “engagement capacity,” provides an explanatory framework for understanding the process through which AL residents with dementia experienced meaningful engagement.
Understanding Engagement Capacity
Engagement capacity was central to understanding the mechanisms through which meaningful engagement was created among residents with dementia. In this context, capacity refers to the amount and nature of engagement resources associated with individuals, care convoys, and settings. As shown in Figure 1, each resident and care partner had an individualized dynamic capacity for engagement. Care convoys and settings also possessed capacity for engagement, and exerted influence on resident engagement. The extent to which a resident’s engagement capacity was recognized and supported by others largely relied on the individual and collective capacity of convoy members and their surrounding environments, including the immediate engagement location (e.g., activity space), AL community, local neighborhood, and relevant social, industry, and regulatory contexts. Optimizing Engagement Capacity.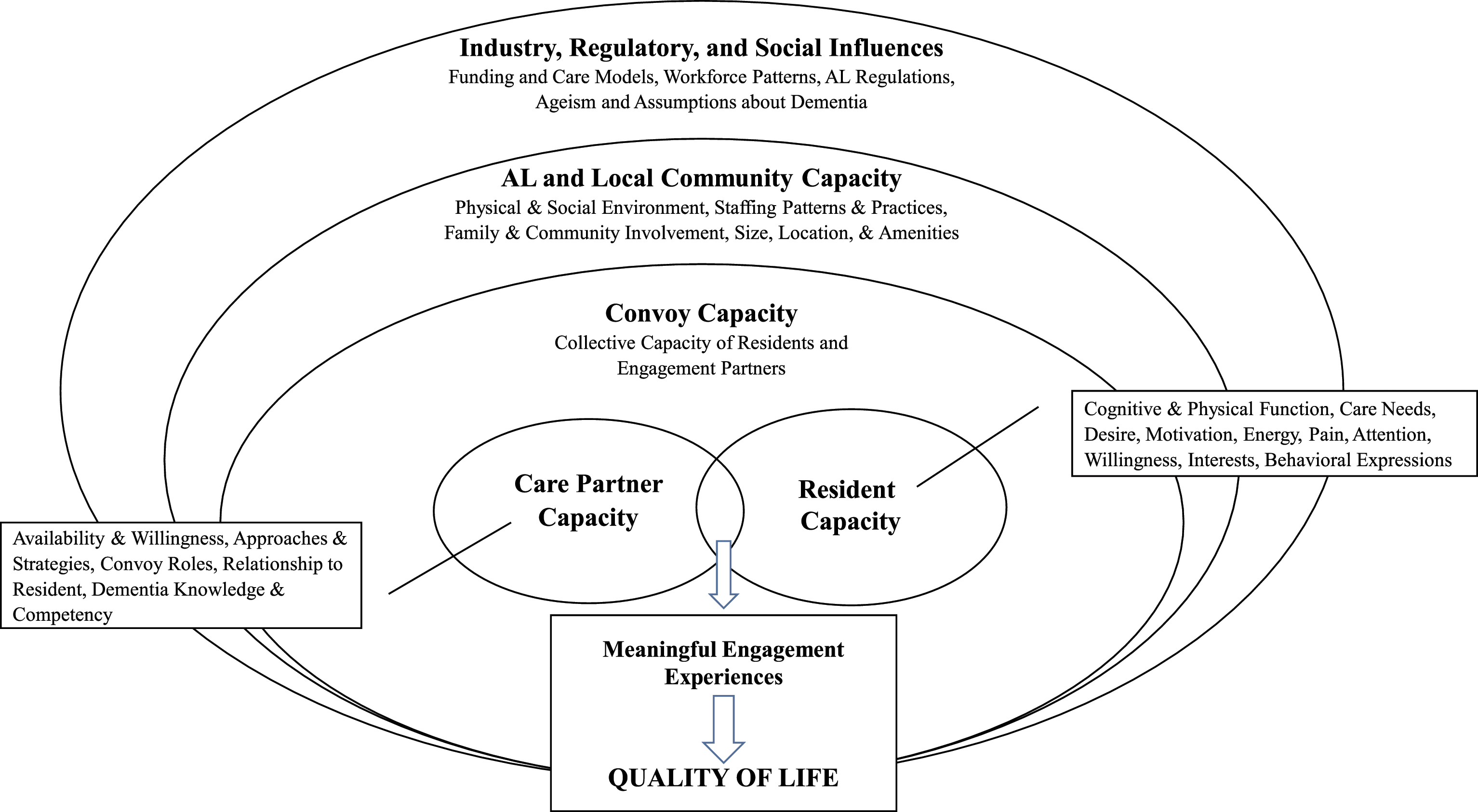
Each individual’s engagement capacity was consequential and intersected with the engagement capacity of other members of residents’ convoys and setting capacity on an ongoing basis to shape opportunities for meaningful engagement over time. These dynamics of coming together and interacting constituted a process through which meaningful engagement was negotiated among AL residents with dementia and their care partners, including how opportunities became meaningful or did not. Consequently, we found that creating and enhancing meaningful engagement among AL residents living with dementia requires optimizing both the individual and collective engagement capacity of all care convoy members, including that of residents themselves.
Resident Engagement Capacity
Engagement capacity for residents living with dementia existed on a continuum ranging from broad to extremely limited and was influenced by their unique and dynamic situations. Multiple factors shaped residents’ capacity, including degrees of cognitive and physical function and accompanying care needs, levels of pain, motivation, energy, and attention, behavior, interest in each activity or care partner, as well as the opportunities presented by others and their surroundings.
Residents with broad engagement capacity had a wider range of options and experiences for meaningful activities relative to others. Residents with higher function and interest in participating were most active, in part because, as Holly House’s care coordinator noted, “they can most do for themselves and say what they want.” Holly House staff said of Elisabeth, one such resident, “she always engages, unless she’s sick. But even when Elisabeth is sick, she’s gonna do something. She participates in anything.” Garden’s resident, Sarah, was described by staff as being “like an icebreaker” who “brings so much to the group.” Despite her broad engagement capacity Sarah lamented not “being a busy person” which she felt “bad about” because she was not taking charge with activities by saying, “Let’s do this now.” Nevertheless, Sarah was mobile with her walker, had wide-ranging interests, was still able and enjoyed reading independently, had regular visits from family and friends, and participated in most activity programing.
In contrast, certain residents possessed narrower engagement capacity, stemming in part from their levels of function, interests, and behaviors. Parkview resident, Don, for instance, needed assistance to ambulate in his wheelchair and was overweight. Yet, his relatively high level of cognitive function allowed him to enjoy intellectual pursuits. His ex-wife explained, “I don’t know if the other people are capable of focusing that much, but Don has a fairly high threshold ‘cause he’s smart—it has to be a little bit [intellectually] challenging for him to even be interested.” Parkview programming mainly catered to a collectively lower level of cognitive functioning and frequently lacked meaning for Don. He experienced disinterest or frustration with certain activities that required recall or following rules and disliked physical activities. His ex-wife noted, “In exercise, he doesn’t focus. It’s not fun for him, and it doesn’t really engage him.” These nuances reinforce the need to understand individual preferences and abilities to optimize engagement capacity and experiences.
Certain residents had high physical mobility and derived joy from movement, especially dance and music. Some required assistance, a supportive context, and cuing to optimize their engagement capacity. Holly House resident, Anna, for example, diagnosed with young onset alzheimer’s, was physically strong, steady on her feet, and extremely mobile, yet she required cuing from a care worker to optimize her activity participation capacity, as the following passage illustrates: Anna knew all the lyrics to all the songs that played in the morning. Anna was among the most receptive to dancing, but her cognitive limitations meant she needed total instructions on what to do, including encouraging her to stand, move her hips, and her shoulders. She followed the instructions, all the while smiling, laughing, and singing.
This strategy was not universally used among care partners working with Anna or similar residents.
Among residents with limited ability to be self-directed, engagement depended largely upon care partner capacity. The three largest AL communities had a resident subset who typically was placed in common areas, yet infrequently engaged in group activities. Billy, for example, non-ambulatory and visually and hearing impaired, was rarely invited to engage and often slept. With encouragement, though, he was receptive. The following fieldnote passage illustrates Holly House’s activity director’s capacity to recognize, act upon, and optimize Billy’s own engagement capacity: Katie went out of her way to be sure that everyone, including Billy, had an opportunity to participate. She commented that he couldn’t see, but somehow could catch the ball and throw it back. He seemed to perk up with the attention. Before Katie came around to include him, Billy was seated in his wheelchair with his arms folded and head down.
For some residents, facilitating engagement required helping physically. As the Garden’s occupational therapist explained, some residents need, “one-on-one with your hand over their hand. . . if you’re not engaging in it to make them engaged, they’re not gonna do it.” Meanwhile, behaviors, such as expressions of depression, anxiety, or distress (e.g., walking around, searching, or aggression), constrained engagement capacity. Marjorie, for example, regularly demonstrated anxiety, often in search of someone. The following excerpt captures a researcher’s encounter: Marjorie began yelling at me to “come on” and “hurry up” and “stop standing around like a silly girl.” I walked over to join her and she grabbed my arm, pulling me along. . . Marjorie walked at a very fast, almost frantic, pace. She then spoke clearly and said that she had to find her husband. She said that he had to get there or we would be late.
Marjorie’s anxious expressions and confusion about time, place, and context impeded staff capacity to facilitate meaningful engagement, as well as her capacity to experience it. Yet, we observed moments and exchanges that appeared meaningful, especially during music therapy and visits with family and friends.
Residents nearing end of life, especially those on hospice, had among the most restricted engagement capacity and were highly dependent on care partners’ capacities. Edna, for example, stayed in bed and was in and out of consciousness prior to death. Her daughter, Beth, visited daily, making efforts to engage. A researcher observed: Beth used her cell phone to play gospel music for Edna and set it up on the table beside the bed. She told me that she’s been playing music this way and every once-and-a while her mother would open her eyes and sing along. As if on cue, Edna began singing, “He Walks with Me” and knew all of the words. Beth encouraged her and told her how nice it was to hear her sing and again told her how beautiful she is. Edna opened her eyes and smiled before closing them again.
Meaningful interactions among residents with such limited capacity required deliberate intervention.
Residents’ circumstances were dynamic and varied by individual, situation, and over time, shaping their engagement capacity. Brian, for example, explained, “if they’ve got a program going where I can be supportive to it, I join it. If I can’t give it my all, I don’t bother.” Another resident, Margaret commented on her changing engagement patterns, “I’ve had some health issues. I haven’t been to Sunday school or a church service now in a good while.” Care partners also noted dynamism in residents’ capacity. Sally’s sister commented, “If Sally is tired, I could be in and out [quickly] 'cause she’ll tell me she’s tired. Other times she can sit and talk for an hour. We sit and listen to the music.” Meanwhile, Marjorie’s son explained, “Mom’s ability to derive joy from things has become real narrow. The things that were sure bets to give her joy, oftentimes, don’t do anything for her, anymore.” Optimizing meaningful engagement among residents depended on care partners’ abilities to understand each resident’s engagement capacity, including how best to overcome barriers, optimize potential, and adapt to changing circumstances.
Care Partner Capacity
Like residents, care partners had individualized and variable engagement capacities, shaped by their availability and willingness to engage, alongside their engagement approaches and strategies, traits related in part to their care roles and relationship to the resident and to their dementia care training, knowledge, and competencies.
Care partners who consistently demonstrated knowledge of the resident and had the ability to adjust to residents’ dynamic realities, be present in the moment, and view every encounter as an opportunity were the most successful at connecting with and engaging residents. Holly House resident Margaret, emphasized the need to “meet people where they’re at” and “show them that you are trying.” Our present analysis identified these approaches as essential to understanding resident capacity and optimizing engagement and thus were integral to exceptional engagement capacity. Yet, exceptional capacity was infrequent across care partner groups, including frontline workers, family and friends, community volunteers, and service providers.
Most frontline workers were not highly attuned to engagement. Researchers routinely documented inactivity, boredom, and disinterest among residents. Daily care routines sometimes were performed tersely or without conversation. Occasionally, workers ignored residents’ presence altogether as the following Parkview fieldnote illustrates. “Stuart was sitting in his armchair with his aide Ismary, by his side. . . another aide came into his room to chat with Ismary. They chatted for about 2 hour. The whole time Stuart just sat looking at the floor.” There were myriad examples of workers overlooking residents while talking to co-workers, using their phones, or resting.
Missed engagement opportunities also occurred during organized activities. Among frontline workers, engagement staff typically were most cognizant of resident engagement. Overall, however, workers with limited training, knowledge, or competencies related to working with persons living with dementia, frequently missed opportunities. In this representative example, Fiona, a Holly House worker who was simultaneously engagement and care staff, led devotional: Residents in the back [of the room] were either sleeping or nodding off. Others on the couches surrounding Fiona occasionally looked at her, around the room, or at each other, some stared blankly or fidgeted with their hands. . . Fiona read quite fast. It was difficult to keep up. . she occasionally looked at the residents, but more so focused her attention on the other workers.
Inattentiveness to residents typically meant little, if any, meaningful engagement.
Certain frontline workers excelled at resident engagement. Most frequently, engagement staff, but also select direct care and other staff. Holly House’s engagement director identified, for example, workers who, “connect with [residents and] take the lead and do things.” Paula, a direct care worker with a 20-years history of working with persons living with dementia, prioritized engagement. She frequently worked shifts with no activity programing or staff and initiated impromptu engagement: Paula connected her phone to the speaker and played Motown music. She announced to everyone in the room that there would be “no sleeping” on her “watch” and that they were going to move their bodies and dance. Paula engaged the residents in dancing.
During this session, each resident received one-on-one attention to facilitate engagement on their individual levels, resulting in laughter, clapping, and singing. Exemplars existed among other workers, including housekeeping, maintenance, and kitchen staff. Frontline workers with exceptional engagement capacity demonstrated in-depth knowledge of residents and how best to relate to and engage them. Some of this knowledge derived from the involvement of residents’ family and friends.
I think that if you come to visit your person and they don’t know who you are, you kind of think, “Well, what’s the point?”. . . as the disease progresses, people probably, do their perfunctory weekly visit, it’s just like 30 minutes or so, just popping in to make sure that everything’s okay and not really hanging around visiting too much.
Similarly, Kerrie, a Parkview care worker explained, “Some families can’t take it. . . [and say], ‘I can’t see her like that.’ They’ll come for a short period of time.”
Other family and friends visited frequently and successfully engaged residents. Those who understood resident capacity, had the ability to adapt, be in the moment, and suspend expectations had greater capacity and success optimizing meaningful engagement than those who did not. During visits to the Gardens, Marjorie’s son explained how he adapted strategies over time: I was bringing a little activity; a very simple puzzle. Bring her a magazine. She was always fond of looking at magazines. Then, she started to lose the ability to focus on those simple things. My strategy of late [is]: I’ll bring a chocolate milkshake. . .She really likes it and it keeps her focused for a short period of time. At least we can have a little bit of interaction.
Similar to Marjorie, Meg’s reduced verbal ability and need for cuing limited her ability to engage in conventional ways, yet she remained socially curious and responsive. Her family took her to restaurants, church, and on car rides. Her son described his strategy, “I try to match the needs that she has at the time and not worry about how it’s supposed to be, is really what’s improved the quality of her life, and our lives as well.” His reduced expectations benefitted everyone, especially Meg.
Knowing the resident and adapting were key. For instance, depending on Anna’s capacity on a given day, her friend Norma might walk with Anna, playing “a game” that involved getting her to read hallway signs. Alternatively, she might appeal to Anna’s musical side, “We listen to the songs, and I tear the lyrics into segments with her a lot to create laughter with her.” Some family and friends, including Norma, found ease in participating in group activities during visits. Doing so provided structured, externally-driven ways to interact and often optimized resident involvement through cuing, assisting, or encouraging.
Family and friends with exceptional capacity tended to visit regularly and assume additional roles in the community including performing or running activities. Emily’s daughter, Cathy for instance, lived nearby and had long-term ties to other residents. A researcher observed, “The mood in the room changes when Cathy is around as she is lively and upbeat, knows everyone, and always takes the time to talk to them.”
Consistency and resident familiarity among this group were not universal. Parkview, for example, drew local high school volunteers, who had limited resident knowledge, guidance, or oversight. The following passage describes student-run bingo: “The kids did not know residents by name. They handed or tossed the winning tickets at the resident who had won bingo that round without ever engaging them.” Researchers observed volunteers from church groups, who likewise demonstrated limited capacity to engage persons living with dementia, despite being well-intentioned.
Care Convoy Engagement Capacity
The engagement capacity of an individual’s care convoy was shaped by the collective capacity of its members and fluctuated over time. Care convoys were dynamic in terms of who participated in resident engagement, when, how, and with what goals, and how members worked together (i.e., levels of communication, consensus, and collaboration). These properties influenced resident engagement, especially, but not exclusively, among those who required greater facilitation than others, affecting the content, quality, and frequency of residents’ engagement experiences.
AL Community Engagement Capacity
Each AL community possessed its own engagement capacity, shaped by size, resources, ownership, location, staffing composition and patterns, engagement programing, organizational structure, policies, practices, and social and physical environments (see Table 1). Community engagement capacity affected residents’ and care partners’ capacity and opportunities for meaningful engagement. Certain community features were fixed; others were modifiable.
What would I do differently?. . I know they say that they're supposed to have a set routine because that helps as far as with the disease, but I feel like if it wasn't so routine that that would be good. Maybe we should switch it up this week. Let's not do devotion in the morning. Let's take them outside for a stroll around the perimeter, or let's start a gardenin' club for all the ladies that like to garden, or maybe we can take 'em out for a woman's-day lunch or a men's day brunch or somethin' like that.
Emphasis on routine, reluctance or inability to try new things, and taken-for-granted assumptions about residents’ engagement capacity sometimes constrained opportunities.
Rosie’s Place used a universal-worker model with staff members doing multiple tasks (e.g., cooking, cleaning, socializing, oversight, care tasks). The owner contracted individuals for weekly activity sessions and twice-monthly musical performances. Residents required minimal hands-on care and frequently engaged in coloring, puzzles, and other self-directed activities. The solitary staff person facilitated residents getting outdoors, watching television, and listening to music, but scarce resources curtailed special events and outings. Communities with formal activity programing experienced staffing-related challenges, including activity director and staff turnover, which negatively affected engagement.
Residents spent considerable time sitting around television sets. At the Gardens, Marjorie’s husband commented, “I wish I could throw a sledgehammer through that television set because that’s what—that’s go-to default place for people to be. There’s a lot of people standing around, staring at the television set, but nobody’s watching it.” Rosie’s Place resident Maria was frail, had limited mobility, and almost no ability to communicate verbally or initiate engagement. Her son said, her “quality of life” related to having activity rather than “watching TV all the time.” Yet, researchers observed some residents enjoying the television, including Molly who always “smiled” and “laughed loudly during the Andy Griffith show.”
Across settings, care partners used cell phones for resident engagement by showing videos or photos, or playing music. However, phone use frequently was a barrier, distracting care partners. One family member noted, “I see staff sitting on their phones. That annoys me because at the very least, even 5 minutes every couple of hours or whatever, you could sit and just go up to mother and sit and talk to her.”
Beyond each AL community’s immediate physical environment, the surrounding neighborhoods shaped capacity. Services, amenities, organizations, and other resources, including potential contractors and volunteers, affected engagement opportunities. Holly House, for instance, had partnerships with several churches and Parkview drew volunteers from a local high school. Accessing opportunities, however, required awareness, interest, and action, on the part of residents and care partners.
External Influences
Engagement capacity was framed by macro-level factors. AL industry features, including low retention and high turnover rates, affected for example, consistent staffing assignment and individual and care community capacity. All communities experienced frequent care staff turnover. Within the three largest communities, turnover occurred among engagement staff with engagement directors turning over at least once in each site. Turnover negatively affected residents’ engagement opportunities, including canceled events, outings or regular programing. Staff changes often were tied to industry factors, including the pull of better wages and opportunities. The Gardens’ administrator spoke, for example, about the frequency of engagement staff leaving to “advance their careers.” State regulations governing training, staffing ratios, and resident care also impacted capacity. Parkview’s administrator noted, “The state regulates…admission criterion. [Residents] have to be able to ambulate to some extent.” Another noted, “the state requires us to have continuous training” and “a certain [staff to resident] ratio.” Meanwhile, social factors including ageism and false assumptions about dementia (e.g., “What’s the point [of visiting]?) as well as public health crises such as the pandemic, negatively influenced care partner capacity. As the end of our data collection period and during the early days of the COVID-19 pandemic, communal dining and activities within the care communities were restricted and barring exceptions on compassionate grounds (e.g., nearing end of life), on-site visits from family and friends also were banned. All communities pivoted to provide virtual access. One son explained, “Dad and I have both done FaceTime calls with Mom. They have gone well albeit a bit one sided.” He continued, “Video chat is a good option but needless to say, it’s not as fulfilling.”
Discussion
Our research identified engagement capacity among residents, frontline workers, family and friends, care convoys, and environments, as central to promoting and constraining meaningful engagement among persons living with dementia. Building on research about meaningful activity for persons living with dementia from the perspective of a single care partner (e.g. Roland & Chappell, 2015), we focus on the more complex care convoy and the context of long-term care. Understanding engagement capacity at all levels, especially their intersections and ensuring process that minimize barriers and optimize meaningful engagement within this population, including among AL residents, can positively impact care interactions and quality of life (Adlebrecht et al., 2021; Burgess et al., 2022; Genoe & Dupuis, 2014; Phinney et al., 2007).
Meaningful activity for persons living with dementia is traditionally framed as isolated, purposeful or therapeutic interventions, yet everyday activities and interactions also represent opportunities for meaningful engagement (Kemp et al., 2021; Smith et al., 2018). Our research confirms that resident capacity can be maximized when care partners use the four approaches: (1) knowing the person; (2) connecting with and meeting persons where they are; (3) being in the moment; and (4) viewing all encounters as opportunity (Kemp et al., 2021). Our present analysis shows that meaningful engagement can be negotiated within daily routines and involves more than the four approaches, but rather attentiveness to engagement capacity more broadly.
Care partners with exceptional capacity understood and were responsive to residents’ and setting capacity. In contrast to others, their successes demonstrated the importance of tailoring approaches to persons and scenarios. Doing so frequently yielded positive care interactions and meaningful engagement experiences regardless of individual resident’s engagement capacity. Kontos et al. (2021) highlight the importance of considering the embodied and relational dimensions involved in collaborating with persons living with dementia in creative endeavors. Our work likewise reinforces the importance of being observant and attending to verbal and non-verbal expressions among persons living with dementia in the context of negotiating meaningful engagement. Both underscore the need for care models that are person- and relationship-centered as they emphasize individualized approaches to care and foster the relational aspects of care.
Study findings point to the importance of understanding and enhancing care partner capacity, especially among frontline workers, residents’ family and friends, and other community members. Education aimed at improving dementia awareness (e.g. dispels myths), competency-based training (e.g. creative problem-solving, person-centered care, dementia knowledge, communication skills, managing uncertainty in social encounters), and resources (e.g. tools for engagement, care plans, time, job redesign) will enhance understanding and optimize engagement capacity among persons living with dementia. Support within convoys for consensus building, knowledge sharing, communication and collaboration also has the potential to realize shifts in capacity and quality of life (Burgess et al., 2022; Kemp et al., 2018). As part of person- and relationship-centered care planning, convoy members and insofar as possible care recipients, should collaborate to identify strategies for promoting meaningful engagement.
Care partners and convoys need supportive social environments that value time spent with care recipients on meaningful engagement during, before, after and between care activities (Bhattacharyya et al., 2022; Morgan & Ahmad, 2022). Further, stigma, or “collective cultural representation of persons living with dementia as being incapable of purposeful and meaningful communication and interaction” is a persistent barrier to social engagement, meaningful activities and social inclusion (Kontos et al., 2021, p. 714). Organizational policies, practices, and cultures that espouse a team approach where all frontline workers are empowered to support resident engagement, including collaborating with family and friends, can positively influence quality of life for people living with dementia, especially those with limited engagement capacity. Consistent care worker assignment, reduced turnover, and organizational cultures that value meaningful engagement for all persons with dementia regardless of capacity are essential (Güney et al., 2021) to promoting setting capacity. Strategic investment in physical resources and environments (e.g. accessible and diverse types of public and private spaces) also can bolster setting capacity.
Limitations of our work illuminate pathways for future research. Research involving quantitative methods, larger individual participant and site samples, other care setting types and geographic areas, would enhance knowledge. Additional research focused on how social and cultural factors influence meaningful engagement (du Toit et al., 2020) is needed.
In-depth prolonged engagement, multiple data collection methods, research team diversity, and inclusion of all stakeholder perspectives, especially persons living with dementia, are among the study’s key strengths. Despite the centrality of their experiences, research often overlooks the voices of persons with dementia (Allison et al., 2021), especially as dementia progresses. Such inclusivity alongside our attentiveness to care convoys and settings, also frequently overlooked, provides a more complex understanding of engagement among this diverse population, than previously existed. Ultimately, understanding capacity is key to optimizing meaningful engagement, essential for improving quality of life and care among persons living with dementia and their care partners, and requires emphasis in research, policy, and practice.
Footnotes
Acknowledgements
Thank you to all who participated, shared their experiences, and gave generously of their time. We are grateful to Pamela R. Manley, Stephen Duong, Joy Ciofi, Joy Dillard Appel, Emerald Anglin, Anastasia Grosheva, Ginger Heidbreder, Jasmine Sease, Emerald Pullon, Anna Lisa Baidoo, Chien Yueh Chien, April Spring Wood, Dottie Mitchell, Margenta Freeman, and Austin William Smith for their important contributions to the “ME study.” As always, thank you to Mary M. Ball, Carole Hollingsworth, and Patrick J. Doyle. We also thank Kim McCrae and Nancy Kriseman for their guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number R01AG062310 (to Kemp). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
IRB Approvals
Advarra: Pro00029867; Georgia State University: H19198; Emory University: IRB00108144.