
Abstract
Hope is an important but overlooked phenomenon in dementia studies. Few studies have examined how people with dementia experience or perceive hope, possibly because it is seen as a diagnosis without hope. In this article, we report on a doctoral study, the aim of which was to examine the phenomenon of hope from the perspective of younger people with dementia to generate new understanding and enable community-based healthcare professionals to support well-being. The study was conducted in the Midlands, England, and used a modified diary-interview method. Six participants were given a camera and asked to take pictures of whatever made them feel hopeful. During a post-diary semi-structured interview, a conversation about hope took place. Interviews were transcribed and interpreted using the ‘Voice-Centred Relational Method’. Findings show that hope is important to younger people with dementia. Sources of hope were the surrounding environment, keeping connected, taking action, and drawing on internal resources. An over-arching theme was ‘defying dementia’ and participants demonstrated resistance to negative stereotypes. Living with dementia did not curtail hope, although it could be weakened when participants felt ‘cast adrift’ by services. The In vivo codes generated were fear of dementia, threats to identity, disconnection from others, and frustrations and restrictions. It is concluded that hope should be a more central part of practice-based conversations with people with dementia.
Keywords
Introduction
Much has been written about the science and practice of hope, especially in the psychological sciences, where it is seen as an integral part of the human experience. Hope is defined in this context as a ‘positive expectation for a desired future goal’ (Callina et al., 2018, p. 15). Specifically, it refers to “the perceived capability to derive pathways to desired goals, and motivate oneself via agency thinking to use those pathways” (Snyder, 2002, p. 249). For example, someone might regularly do crosswords or word games in the hope of staying cognitively well as they age. Hope clearly has a ‘crucial role to play in the facing of adversity’ (Hicks, 1997, p. 95). Moreover, for people living with a life-limiting condition (like dementia), hope has relevance in the here and now, as well as the future (Callina et al., 2018). Hope for example might be found in spending time with others or taking part in enjoyable activities, not just in anticipating future pleasurable events. In this article, we examine the phenomenon of hope from the perspective of younger people with dementia and argue for more hope-building interventions during the diagnostic process, as this is when people are most likely to feel hopeless.
The concept of hope is particularly salient in the context of younger people with dementia (those under 65 years of age) who it has been argued may have different needs to older people (Millenaar et al., 2017; Oliver et al., 2019). People in their 40s, 50s and 60s are more likely, for example, to be physically fit and active, and to be aware of their problems, increasingly the likelihood of frustration and distress (Jefferies and Agrawal (2009). Younger people are commonly still in paid work when symptoms begin and may need to retire early bringing financial hardship (Roach & Keady, 2016; Silvaggi et al., 2020) especially where there are pre-existing financial commitments such as mortgages and loans (Jefferies & Agrawal, 2009; Kimura et al., 2015). Being younger means people are more likely to have dependent children, who are likely to be impacted by their illness (Gelman & Rhames, 2020; Withall, 2013) especially if the dementia may be genetic (Gilliard, 1999). Younger people typically experience a delay in diagnosis and treatment (Draper et al., 2016; Van Vilet et al., 2013) due to a multitude of factors including unusual symptoms, rarer forms of dementia being common, misdiagnosis (Reves et al., 2018), and lack of experience of younger people on the part of health care providers (Hunt, 2011). There is also concern that younger people and their families may be marginalized, socially isolated and lack support (Bannon et al., 2020; Kaiser & Panegyres, 2006) encountering a lack of age-appropriate services (Withall, 2013).
A series of literature searches was carried out and repeated between 2013 and 2024 using search terms ‘hope AND dementia’, ‘hope AND Alzheimer’s Disease’ and ‘dementia AND positive’. The period covers significant events, including Covid-19, and mounting pressures to health and social care services. Still, only two studies were found which directly examined the hope experience of people with dementia. One used semi-structured interviews to explore the hopes of ten people living with dementia over the age of 65 years (Wolverson et al., 2010). The meaning of hope to participants was discussed, and potential barriers to and facilitators of hope were examined. The other analysed 29 poems on the subject of hope written by people living with dementia (Amponsem & Wolverson, 2023). The researchers found that hope was felt by people with dementia, and an important strength, concluding that health professionals, family and society have a role in supporting people with dementia to maintain their hope.
Other research hints that hope might be important to people living with dementia (Dalby et al., 2011; O’Sullivan et al., 2014; Pipon-Young et al., 2011), including younger people (Pipon-Young et al., 2011). This is because it reaches beyond a solely biomedical view of hope for a cure or medications to ease symptoms (Pritchard, 2017). Studies of the lived experience of dementia have found that a hopeless existence is not always inevitable, with resistance to negative media messages being common (MacKinlay, 2012), and fighting spirit (Clare, 2002; McFadden, 2004; Phinney et al., 2007). In a study by Amponsem et al. (2023), hope was defined as a personal resource that plays a vital role in managing well-being after a diagnosis of dementia. It did so by orientating people to their personal capabilities and current possibilities in the context of dementia while acting as an energising force that facilitated engagement with pleasant activities’.
Despite the importance of hope to people with dementia, individuals seem to experience low levels of hope (Chapman, 2011), and high levels of hopelessness (Harwood & Sultzer, 2002; Lopez et al., 2003). Qualitative studies have similarly found that hopelessness can dominate the dementia experience (Hulko, 2009; Robinson et al., 2005; Svanström & Dahlberg, 2004). Biomedical approaches attribute this lack of hope to the absence of a cure for dementia (Pritchard, 2017), which Kitwood (1997) has termed “no cure, no help, no hope” (Kitwood, 1997, p. 67). However, knowledge about hope from the perspective of people with dementia themselves is limited, therefore it is not possible to draw this conclusion.
Despite the importance of hope to people with dementia, few researchers take hope as their central topic (Pritchard, 2017). Those that have either seek to measure the phenomenon and/or examine it in relation to other constructs or specific contexts. For example, researchers have used the Herth Hope Index to discern that families living with dementia ‘may maintain hope in the face of a potentially progressive illness regardless of cognitive status’ (Hunsaker et al., 2016, p. 596). Others suggest that hope is linked to self-esteem: ‘inspiring hope, enhances self-esteem’ (Cotter et al., 2018, p. 214). Another research team, who conducted a scoping review of ethical considerations during the diagnostic process, concluded that instilling hope must be balanced with truth during the disclosure of a dementia diagnosis (Merl et al., 2022). While this work provides important evidence about the importance of hope to people with dementia, questions remain about how hope plays out in practice for people with dementia.
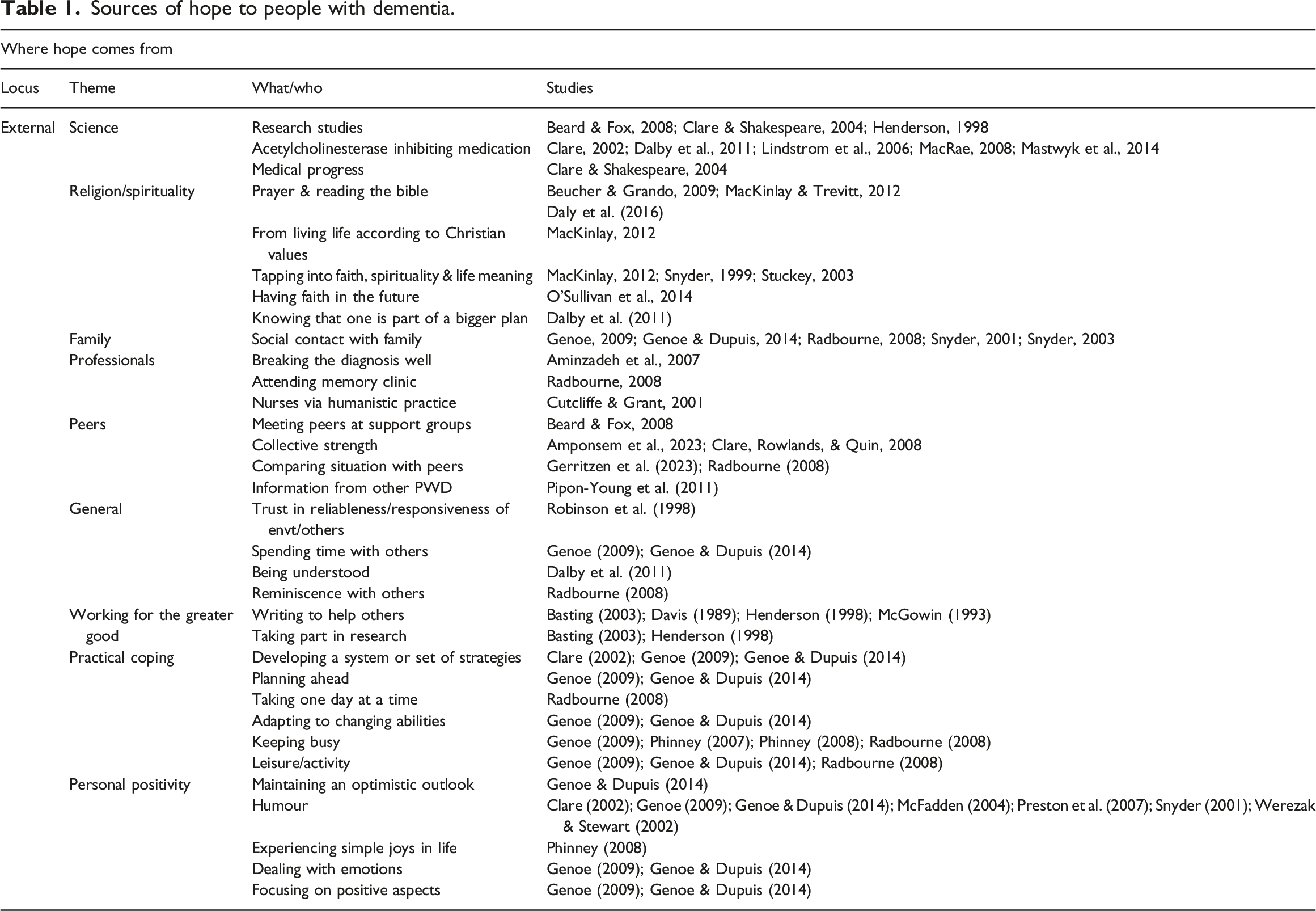
Sources of hope
Sources of hope to people with dementia.
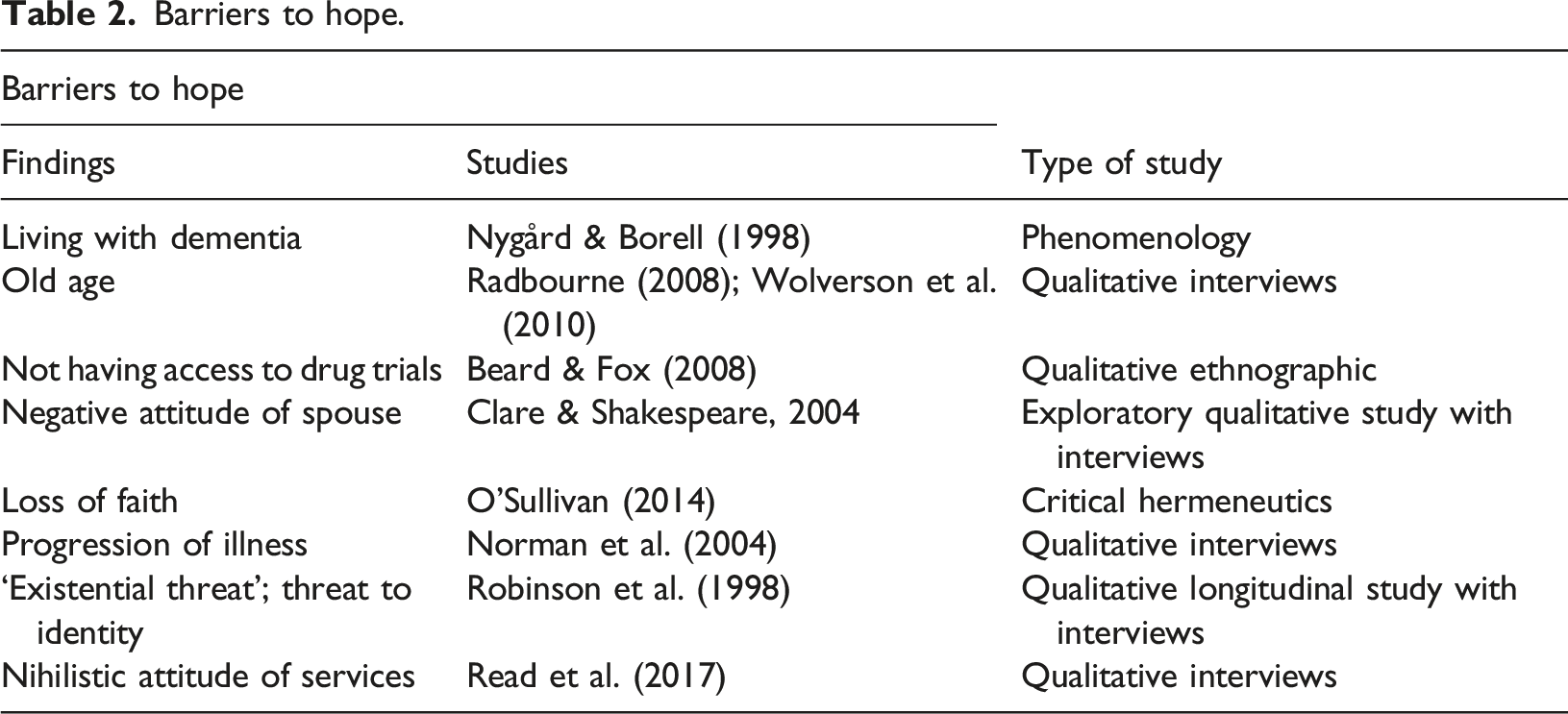
What makes people with dementia less hopeful
Barriers to hope.
The needs of younger people
Younger people with dementia have been described as a marginalised and understudied group (Kaiser & Panegyres, 2006), whose needs and social circumstances are different to that of older people. There has been concern about a lack of age-appropriate services, social isolation, and a lack of support (Beattie et al., 2002). This study therefore focuses on the needs of younger people with dementia to help bridge this gap, and to build on the work of Radbourne (2008), this time with participants under the age of 65, and the addition of photo diaries.
Methods
Aims
This study addressed the following research question: How do younger people living at home perceive hope, and how might their perceptions inform and improve community nursing practice?
The aim of the research was to examine the phenomenon of hope from the perspective of younger people with dementia (those under 65), to generate new understanding, and to enable community-based healthcare professionals to support people’s well-being.
Research design
This in-depth, interpretive study drew on narrative approaches to elicit each person’s story. It used qualitative methodology to achieve this through a modified diary-interview method involving photo diaries. It was hoped that the use of a photo diary would reduce the burden on participants to remember, allowing them to record their thoughts in the form of photographs in their own time at their own pace (Bartlett, 2012). Photographs were used to facilitate discussion and allow a richer insight into their world.
Setting
The study took place in the Midlands, England and involved participants who lived in their own homes because this is where most people with dementia live. The community setting has much in common with previous empirical work that has highlighted hope as being important to people with dementia.
Sample size
Six adults under 65 years with a formal diagnosis of dementia were recruited to this doctoral study. This was considered to be a number which was manageable both conceptually and practically, allowing for repeat interviews and for a sufficient depth and quality of rich data to be generated. The Voice-Centred Relational method is also complex and time consuming (Mauthner & Doucet, 1998) which is a factor in choosing this relatively small sample size.
Inclusion criteria
All participants needed to be able to give informed consent in line with the process consent method (Dewing, 2007), and demonstrate insight into their illness. This was considered an important inclusion criteria as participants not aware that they had dementia might see hope in a different way, and it could be argued that the presence of hope was only due to a lack of insight. It was therefore ascertained by the researcher in an initial interview that each participant was aware of their diagnosis and were willing to talk about how it affected their perceptions of hope. Participants with any type of dementia were able to take part (those with visual processing difficulties such as PCA were not excluded as the photography part of the study was not compulsory) providing this had been formally diagnosed. A formal dementia diagnosis was needed for the reasons explained above.
Exclusion criteria
Only participants over the age of 65 at time of diagnosis could take part as this was a study of younger people with dementia. Those currently living in care homes, and people staying in hospital could not take part in the study as the effect of their environment may have confounded the results. People with co-morbid conditions which impacted significantly on day-to-day life (e.g., severe depression) were also excluded for the same reason. There was no restriction in place based on level of cognitive impairment, and provided that the person was able to demonstrate insight into their illness they were able to take part. Participants who were unavailable for interview within a reasonable timeframe (2 months), those who were unable to speak fluent English (people with severe language deficits were not able to take part) and people unavailable to be interviewed in the local area, for logistical reasons, could not be take part in the study.
Participant selection and recruitment
Purposive sampling methods were used to recruit six people to the study. All participants were recruited through an organisation for younger people with dementia. Interviews took place in participants own homes. Participants who met all the inclusion criteria were asked to sign a consent form confirming that they agreed to take part, including consent to be audio recorded.
Process
Participants who wanted to take part in the photography part of the study (this was all participants) were given a disposable camera, chosen for ease of use, with written instructions on how to operate it, they could also use their own camera if they preferred. Participants were asked to take pictures over the coming month of anything that made them feel hopeful. A written reminder of their task was provided and left with participants in order to reduce the cognitive burden on participants to remember the instructions. Phone calls and face to face visits were made available if the person felt that they needed this to complete the task (although none required this). Participants were advised that ideally, they should complete this task within a month, and that they did not need to use up all of the pictures if they did not want to. The pictures once developed formed a photo diary. Photo diaries have used by Bartlett (2012) and Genoe (2009) with people with dementia, while Moore (2012) has also used the technique to explore hope in older adults. The photographs were not used as a primary source of data in this study, and instead were used to facilitate discussion during an interview, in the hope that it might enable insight into the participant’s world in a way that might otherwise not be possible.
Data collection
During a post-diary interview a conversation about hope took place, which lasted approximately an hour. The conversation was recorded using a digital audio recorder. Photographs were used to facilitate discussion rather than being a primary source of data. Question prompts about hope were available to the researcher, most of which centred around the photographs taken. A question was asked about whether anything made the person feel less hopeful, but overall, the conversation was free flowing.
Data analysis
Interviews were transcribed and interpreted using the ‘Voice-Centred Relational Method,’ a Feminist approach based on the work of Gilligan (1982). The ability of the method to uncover power dynamics (Paliadelis & Cruickshank, 2008) was felt to be crucially important to the study of people with dementia who experience considerable negative attitudes in the social discourse (O’Sullivan et al., 2014) and unequal power relationships. The methodology requires the researcher to conduct four readings of the data; firstly, the story and who is speaking, secondly in what body (how people speak about and appear to feel about themselves), thirdly ‘telling what story about relationships’, and lastly in which societal and cultural frameworks (Brown & Gilligan, 1992). These readings enable an in-depth insight into the person’s world. The Voice-Centred Relational Method can assist with reflexivity because it requires the researcher to document their own responses to the person, and to examine their own assumptions and beliefs as part of the first reading. In this study reflections were written directly onto transcripts as part of the data analysis process. These were also discussed with project supervisors during analysis of a sample of the transcripts. Data were analysed for patterns related to hope, including; what participants hoped for, where their hope comes from, what and what hinders hope. In vivo codes were identified to characterise how participants spoke about their situation, these included: ‘fear of dementia’, ‘threats to identity’, ‘disconnection from others’, and ‘frustrations and restrictions’. Themes and higher order themes were then generated from the readings of these data and in vivo codes, as outlined in the findings section below.
Ethics consent and approval
Approval was granted by the University of Southampton’s Research Governance Office, and the NHS Research ethics committee. Throughout the research process there was no deception involved. Participants were fully briefed about the purpose of the study in an open and honest way.
Findings
The study took place in 2016, six people were recruited to the study; no one dropped out. All opted to take part in the photo diary element of the research, one person used two cameras due to his enthusiasm for the task. As expected, interviews took approximately 1 hour.
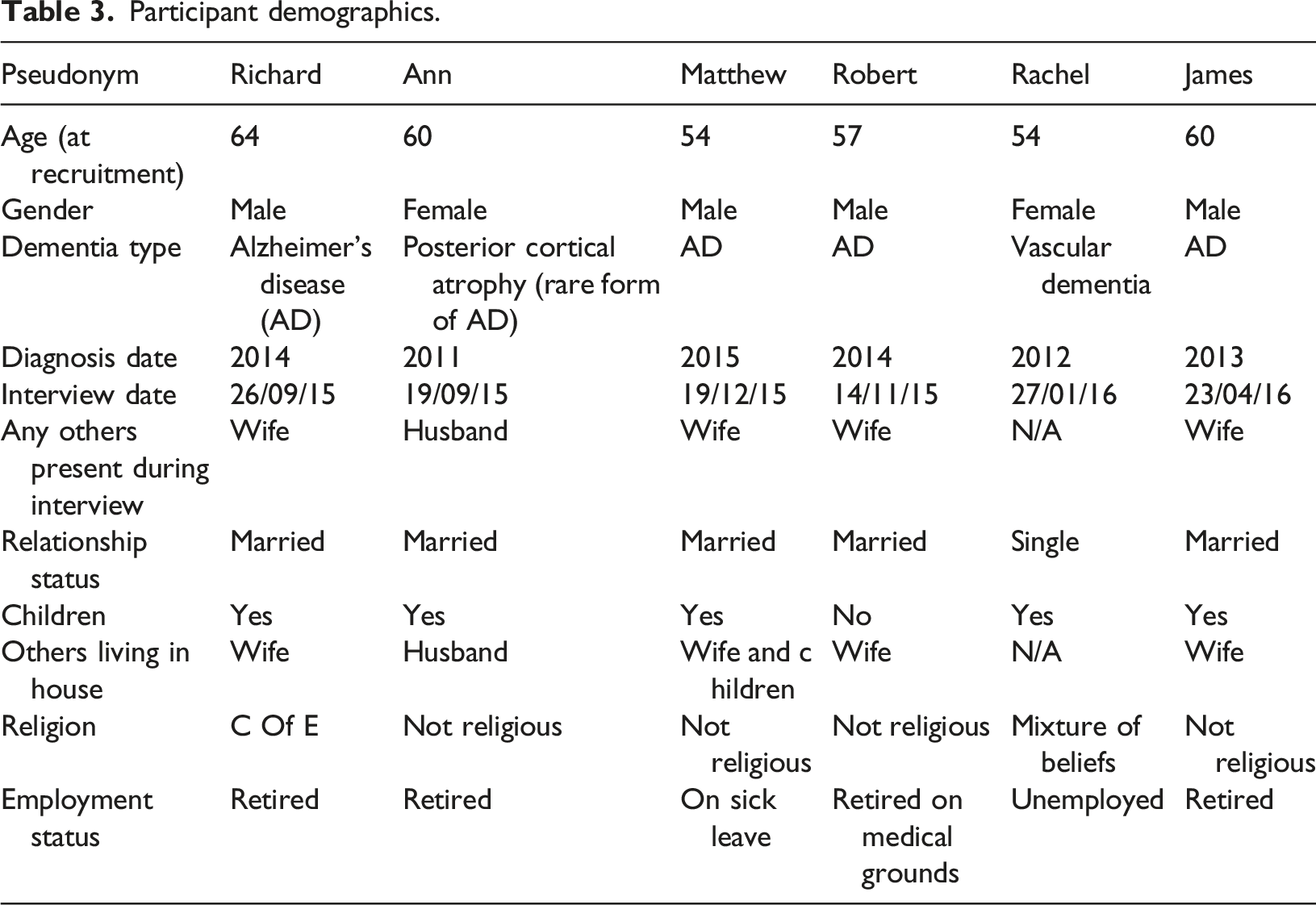
Profiles of participants
Participant demographics.
Themes
Hope despite dementia
Hope was present in all participants. It was a realistic hope, and none yearned for more than they had. Ann said, “I have more good things in my life than bad things” and Richard, on being asked what he hoped for replied; “oh I think we’ve got most of what we want here.” All participants said that hope was important to them, with the exception of Richard, who said “not to the point that I worry about it”. Ann meanwhile gave a very different answer: “Well, if you don’t have hope what do you have?… really…at the end of the day? Doesn’t matter what your trouble is…you know if you don’t have hope to get through it you might as well just kill yourself…do you know what I mean?”. Ann
Having dementia made Matthew less hopeful at times, however he tended to stay positive; “do you know that I’m happy most of the time actually”. James expressed similar satisfaction with life; “life’s good at the moment”. Ann had the following advice for other people with dementia: “Perhaps the only thing I’d ever say to somebody with something like this is…never let hope go…d’you know what I mean? Keep hopeful…and erm…you know that you can’t get better, but you can still….have a jolly good time!”. Ann
Fighting dementia
Adversity was something all participants faced in the form of their dementia, and they fought back in order to reclaim a normal life. Many spoke of the thrill of upcoming holidays. Ann wished to do a wing walk for charity, and Richard spoke of climbing up to a castle high up on a steep hill: “Not many of us actually got to the very top…I was absolutely determined I was not going to be beaten by it…it would have been so easy to say…oh no…I’m not going to do that”.
Metaphors
Hope could be seen in metaphors, which photographs seemed to elicit particularly effectively. Sunshine was a recurrent theme in participant’s accounts, while rainbows were something that held special significance for Rachel; “I love rainbows…it is a symbol of hope…absolutely”.
Rachel also took photographs of a historic building severely damaged by fire and covered in scaffolding. She was able to see beyond the destruction, finding meaning. For her the fire symbolised renewal, and it increased her faith in humanity knowing that people were taking the time to rebuild.
The wind meanwhile could be a destructive force for Robert and Ann and threaten some of the more fragile stalks and flowers in Ann’s garden, but it could also bring hope. Ann took pictures of a white, delicate looking flower because despite appearances it was incredibly resilient: “oh the wind flowers…oh they’re beautiful…you must go out and have a look at them they’re the prettiest things in the world…they don’t break…they literally in the wind they DANCE!”. Ann
Where hope comes from
Higher order themes generated suggested that hope came from appreciating surroundings, keeping connected, taking action, and drawing on internal resources. A large number of sub-themes were elicited as shown in Figure 1, and an overarching theme was ‘defying dementia’. Where participant’s hope came from.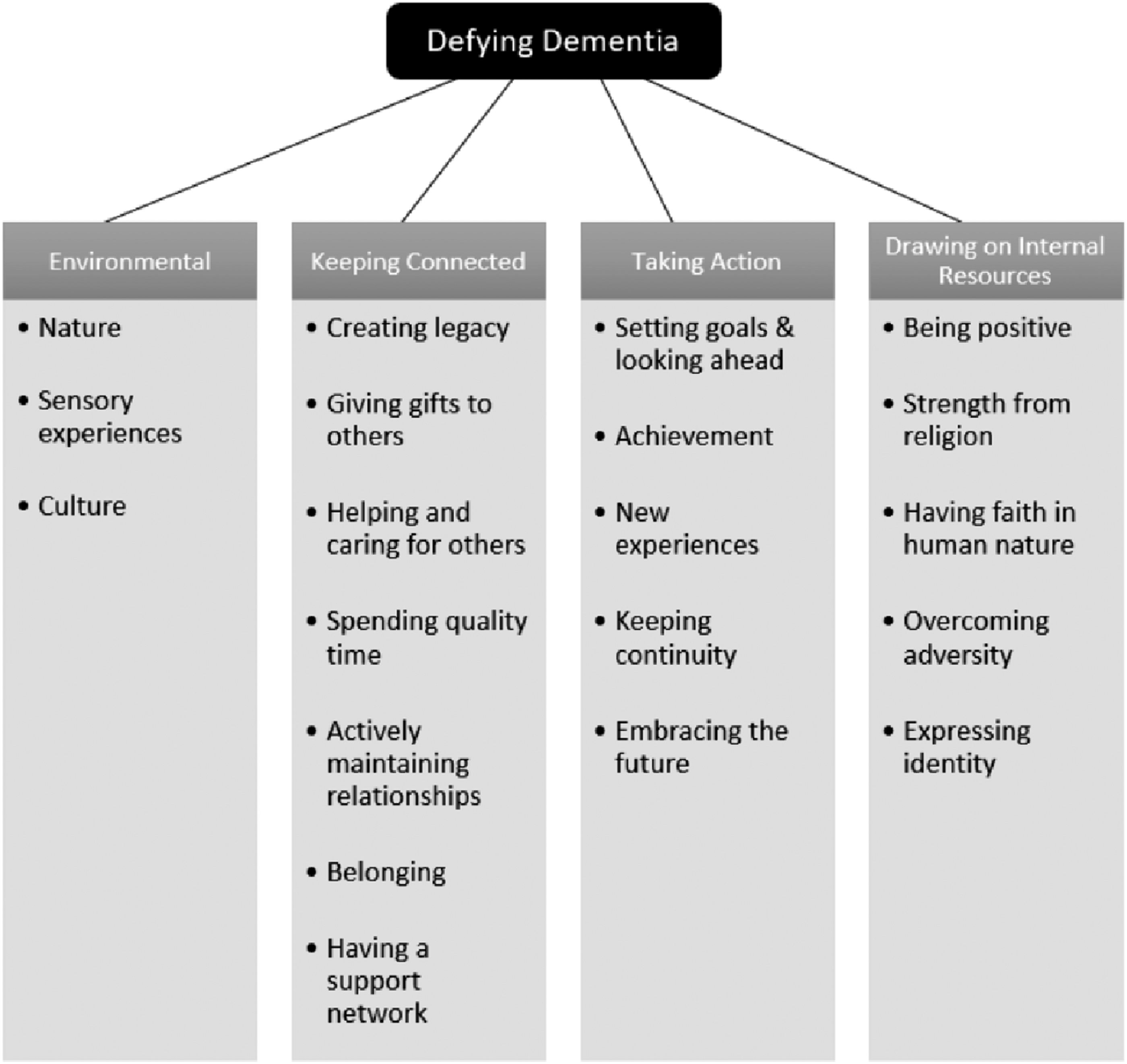
The natural environment
All participants took photographs of nature and seemed to have a deep appreciation for their surroundings. Robert for example took pleasure in viewing his garden as well as watching the birds. Rachel took a photo of woodland she enjoyed walking in, as did James who also took pictures of his allotment. Both Richard and Rachel described the hope inducing nature of sunsets, for Richard it was their beauty, for Rachel her fear of darkness brought with it hope of the sun rising again.
Perhaps due to her failing eyesight, Ann reported a range of different sensory experiences that brought hopeful feelings. Her sense of touch was important to her for identifying her beloved plants, for handling tactile objects, and appreciating the warmth of the sun. Matthew also enjoyed the sensation of sunlight “when you come out of the winter and um you know all of sudden you feel good…quite well because, you know, the sun’s out”. Rachel meanwhile spoke of her enjoyment of food and eating out.
Keeping connected
For Matthew, leaving a legacy through his teaching was important and a notable source of hope. He said: “so that’s the school I used to work in…I feel like I’ve done something and left some…left something”. Bumping into ex-pupils and their families could recharge these hopeful feelings. Like Matthew, Rachel left a legacy, in her case through the mosaics she created and sold. James’ life story book meanwhile reminded him of his accomplishments and what he would leave behind.
Spending quality time with family and friends brought participants hope. They were typically active in maintaining their relationships with others. Rachel for example asked a friend if she could join her next time there was an art exhibition and contacted others through her Facebook groups. Participants far from being withdrawn, reached out and did not allow their dementia to diminish their relationships with others.
A sense of belonging was important to most participants. For Richard this included the place he went to university which he visited regularly; “it’s like another family”. Matthew felt part of something bigger when he joined a cycle club, which he said brought “immense pleasure and friendship”. Being part of a walking group also made James hopeful; “we can have a chat with them and um er a beer and that’s quite nice”.
All participants described the importance of others supporting their wellbeing. Robert said that his wife made him hopeful; “oh…she looks after me”. Ann’s children lived nearby which was important to her, but just having their photographs around the house was comforting: “as long as I can see the children in the pictures…I’m alright…it’s really nice”. Rachel who lived alone, valued seeing her support worker.
Ann’s support worker meanwhile made her hopeful by taking her to visit leafy places, and she was glad of their shared interests. Her young granddaughter was also helpful, making her drinks and cakes: “she’s like a little carer…you don’t even need to say anything to her”.
The dementia café was another important part of Ann’s support network and she felt able to chat to people there; “we’re all the same…more or less!”. Matthew’s cycle club meanwhile also brought considerable hope and strength to him’ “the friends made are now hugely appreciated and they really look out for me”.
Taking action
Participants took action to find hope. Matthew spoke of the importance to him of looking forward and of having goals to focus on. James also liked to know that he had events in front of him: “Yeah, that helps I think, yeah ev-even if it’s just a list of things we write down every now and again er you know it’s going to happen”. James
Most spoke of looking forward to holidays, trips, and family gatherings while James also had plans for his allotment and knew that he would still be gardening even when his illness progressed; “I’ll always be digging”.
Achievement seemed to be especially hope inducing. Richard took a number of photographs of his climb up a steep hill on holiday for example; “I was absolutely determined…I was not going to be beaten by it”. The frequency that James won table tennis didn’t matter to him it was the hope that with the right mindset he could win every now and again, exceeding his own expectations; “well I suppose that you feel a bit euphoric”. Rachel and Robert also coached themselves to improve on their score on the MMSE.
Of note was that most participants spoke of enjoying new experiences and doing things they had never done before. Rachel for example enjoyed trying new types of art, and new types of music created hope in Ann. Richard was excited by the unexpected, and Ann enjoyed broadening her horizons by visiting new places. For James going to Australia was a huge turning point in regaining hope after his dementia diagnosis. Richard liked to surprise his wife: “I like doing things that (wife’s name) doesn’t know about because they give her some sort of surprise…hopefully good ones”. Richard
Robert prepared for the future, and this made him hopeful. He spoke cheerfully of having created a low maintenance garden for when he was no longer able to tend to it himself. This preparation had given him a sense of control and had increased his hope, not reduced it. Ann had also made plans; “I’m not going anywhere!” as she and her husband had arranged for the house to be converted for her future use. Rachel similarly thought of her daughter when she tried to keep her possessions to a minimum; “I don’t want my daughter to be burdened…you know when anything happens”.
Drawing on internal resources
Participants were able to focus on their strengths rather than on what they were no longer able to do. Rachel saw snow as an opportunity to build a snowman, and Richard saw the rain as being good for the grass. Fun and humour appeared to be resources that participants particularly drew on and which gave them strength.
Religion was something that two participants also drew strength from. The hope inducing aspect of Richard’s faith was meeting other people in the congregation. For him, the worship was almost secondary. Rachel meanwhile was a very spiritual person whose beliefs sprung from many different religions. For her, crosses were an important symbol: “That’s just some of my mosaics are just crosses they always make me feel really hopeful…for whatever reason”. Rachel
Adversity had links to resilience and perseverance. When Robert told the story of a rescue during a hurricane just recalling it seemed to bring him hope and strength. He similarly described tolerating being in an MRI scanner for several hours as part of a research study and was proud to be the only person to have managed to stay this long. Participants were all able to see that life continued despite dementia.
Robert, Matthew, and Ann’s hope came from activities connected to their gender role. Matthew said conspiratorially of cutting the grass; “yes… (whispered) because it’s my thing! it’s boys…it’s what boys do!!” and Robert spoke at length about his ‘man shed’ where he kept his tools. Ann meanwhile enjoyed being with her grandchildren who saw past her dementia: “It doesn’t matter what you’ve got you know…a Granny is a Granny isn’t she?”.
Being ‘cast adrift’ - barriers to hope
All participants could identify what made them less hopeful. James used the phrase “cast adrift” to describe his feelings when memory services discharged him, and this seemed an apt in-vivo code to use to characterise participants’ overall experiences of living with dementia. Other in vivo codes were identified to capture participants’ perceptions of the barriers to hope, including fear of dementia, threats to identity, disconnection from others, and frustrations and restrictions (see Figure 2). Barriers to hope.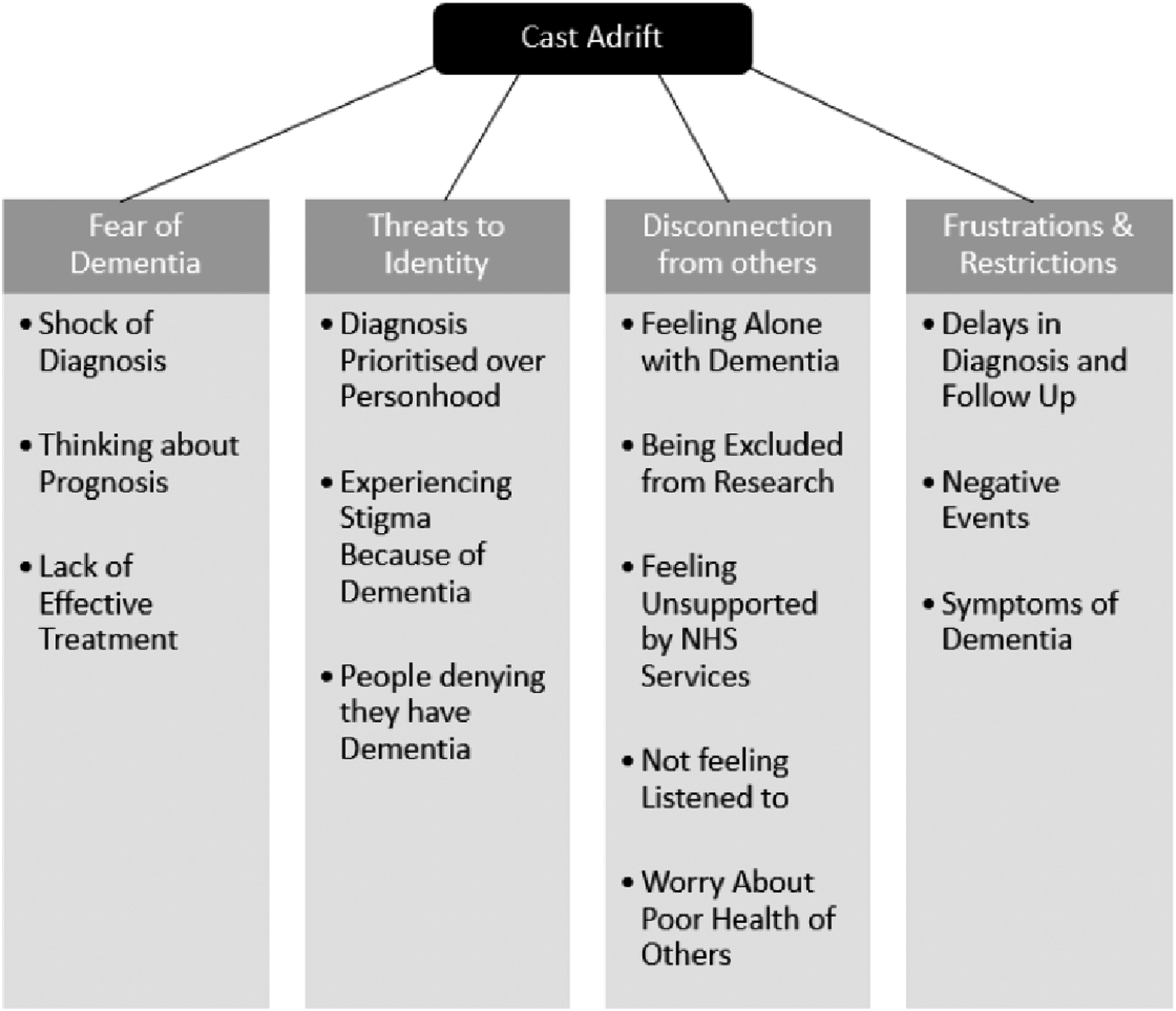
Fear of dementia
James was shocked when he received his diagnosis; “it’s just sort of er it felt like it was sort of almost the end of the world”. He referred to that period as ‘dark days’. He and his wife didn’t take up the offers of support, saying; “we were probably frightened at the time”. Matthew who had been diagnosed the most recently felt similarly traumatised: “It is sort of a bit of a blur…that that period... and I know I wasn’t thinking particularly straight or anything like that”. Matthew
The way in which Matthew’s diagnosis was broken to him was a key factor in his loss of hope, and he expressed anger: “We were just in a ward! You know, it wasn’t even in a private room or anything…”and it was just poor!!! …when you give somebody…life changing news I just think there’s probably lots of very good practice about how to do it and…and that wasn’t what happened really”. Matthew
Mathew put on a brave face, but the future for him was frightening: “That is difficult because you look…you can’t help but looking at people and think… (with sadness) that’s going to be me…”. Matthew
Thinking about his prognosis was at times very painful: “If you’re not in a a great mood you can just (makes pretend weeping noises) um…but…I guess that’s only been a couple of times I guess hasn’t it when I’ve had a bit of a breakdown”. Matthew
Richard also found that his prognosis could threaten his hopeful outlook; “I was only told what was going to happen and…I can cope with some of it”. The lack of effective treatment and support was also an issue for Richard: “The best thing they could do was get a group of other people with the same thing…it didn’t help much really”. Richard
Matthew’s hope was initially bolstered by the thought of taking cognitive enhancing medication, but his hopes were dashed when its efficacy was later played down. Feeling mistrusting, he then wondered whether manipulation of hope was the real purpose of these medications: “I sometimes think…is this just…you know…to keep me busy you know…and feel like something’s happening?”. Matthew
Threats to identity
Three participants reported stigma. Robert mentioned that his aunt could be impatient with him because of his cognitive difficulties, and Rachel that her dementia symptoms could cause her problems at the checkout in shops: “Because you know we’re being slow, or we’ve forgotten how to count our money…or…you know…not getting our money out quick enough or just stuff like that”. Rachel
This had less impact on her hope than it used to as she felt able to assert herself more: “I’m I just…nowadays I’m just too long in the tooth…to to be bothering…and I just say…look…I might not look like it, but I have dementia…please be patient”. Rachel
For Ann, stigma came from her mother; “well she’s ashamed” and she found this particularly hard to bear, saying that she would never forget it as long as she lived.
Far from being in denial about their illness, half of participants became frustrated when others did not believe that they had dementia. The voice-centred relational method revealed that this invalidated their experience and struggles. Rachel found that people could even respond aggressively; “sometimes you get a throwback like ‘don’t talk shit’”. Robert also found that he was not always believed: “he always says, ‘nah you haven’t got Alzheimer’s’ and that and I’m like ‘yes I have!’”.
Disconnection from others
Matthew’s account was powerful, and it was clear that he and his wife felt very alone at the point of diagnosis: “He said…”oh I’m really sorry”…and er he walked off…and there’s no-one around!! And we’re like in this half empty place…there wasn’t anyone there to support us”. Matthew
He revealed the true extent of the hopelessness he felt at that time: “I wouldn’t have that situation whereby you go off on your own…I might have topped myself as a result of that”. Matthew
Matthew felt alone with his dementia even when he went to meet other younger people with dementia as he still found himself the youngest: “We haven’t met very many people…who are sort of…my age…people say ‘oh there’s lots and lots of people…lots of people your age’ and I thought…(disappointed) just show me one…just show me one…and we haven’t seen one have we?”. Matthew
James felt abandoned by NHS services which he said felt like being “cast adrift”. Matthew felt rushed during appointments with his consultant due to the pressures of busy clinics, and Rachel felt unsupported at times, such as when she was asked to get the results of a SPECT scan from Spain by herself; “they were like “well you have to get it” and I’m like well…I don’t know how to do that”.
Rachel also did not always feel that she was being fully listened to and this could make her feel hopeless. She recounted an appointment with a psychiatrist who wanted her to stop a cognitive enhancer that she felt had helped her: “I lost interest in her completely and just shut down…um…but I know I can shut down…and that is when somebody is putting me down…or really not listening”. Rachel
When the health of other people with dementia declined and they stopped coming to the dementia cafe this also had an impact on Ann’s hope; “I’m quite sad if somebody…isn’t there anymore” and she showed concern for their welfare; “I do worry about them”. She also worried that her dementia would lead to increased dependency on others.
Frustrations and restrictions
Delays in diagnosis and follow up could threaten hope. Obtaining the scan results was difficult for Matthew: “Why can’t I be seen now? ...they say we’ll see you and it’s just like a long time away…having to wait…that’s…that’s quite…it’s very frustrating…when you want to know…what have I got? Have I got something? And they say yes and we’ll discuss that in…you know…couple of months…no!!”. Matthew
For Ann her dementia restricted her independence; “when I’ve got a rubbish head I’ll not go anywhere”. This was often the case with Rachel; “I usually…I like to go with somebody because I’ve lost the confidence to just go out”. She had difficulty reading, and this could derail her plans sometimes particularly in busy environments.
Discussion
The importance of hope
Hope was important to younger people with dementia in this study, and participants saw themselves as having a future. This was in line with previous studies (Aminzadeh et al., 2007; Beucher & Grando, 2009; Dalby et al., 2011; O’Sullivan et al., 2014; Pipon-Young et al., 2012). This study adds more context about the sources of hope, and examines barriers to hope also. As found by Clare, Rowlands, Bruce, et al. (2008) and MacRae (2008), hope seemed to be sustaining, was realistic, and helped participants to live in the present as well as the future (Radbourne, 2008; Wolverson et al., 2010). For Rachel hope was brightest in the dark, indicating a strengthening, rather than a weaking of hope at difficult times.
Partial rejection of the biomedical model
‘False hope’ of a cure or an improvement in symptoms was not a feature of participant’s accounts, as with Wolverson et al. (2010). This represented a major departure from some previous studies as none hoped for example that they had been misdiagnosed (Clare, 2002; Werezak & Stewart, 2002), that they would be cured (Lindstrom et al., 2006; Phinney et al., 2007; Radbourne, 2008). Robert hoped that one day a cure might be found, but that it would help others rather than himself. There was only lukewarm feeling about cognitive enhancing medications and biomedical research in contract to other studies (Beard & Fox, 2008; Clare, 2002; Clare & Shakespeare, 2004; Dalby et al., 2011; Lindstrom et al., 2006; MacRae, 2008) and it could be a blocker to hope if the person was excluded from taking part because of their cognitive score, or for other reasons. This implies that hope is not just tied to cure or the absence of symptoms for people with dementia and that a broader understanding of hope is possible.
Living well with dementia
Findings show that it is possible for a person with dementia to thrive and to embrace, rather than try to avoid their future. This was also the finding of Wolverson et al. (2023) who found that positive experiences were not only possible in spite of dementia, but possibly sprung from it. As Wolverson et al. (2010) also found, hope remained; “it’s natural to have hope, I suppose there is something in the brain that has been preserved and hasn’t been destroyed” (Wolverson et al., 2010, p. 454). Illness progression surprisingly did not preoccupy participants (unlike Norman et al., 2004), but the burden that this might one day create for others did (as in Radbourne, 2008) and worry over increased dependency was voiced. Participants saw hope as a fundamental part of wellbeing in line with mental health recovery approaches. Nature and the surrounding environment were very strong sources of hope to participants in this study. Other studies have shown that the outdoors is important to people with dementia (Odzakovic et al., 2020), serving as an important location for leisure activities (Genoe, 2009), enhancing people’s quality of life (Brod et al., 1999), and strengthening self-identity for younger people with dementia (Olsson et al., 2013) but this was the first study to explicitly tie the surrounding environment to the concept of hope. Another difference was that hope could be generated in people with dementia from reminiscing about the past. This has implications for reminiscence therapy which perhaps inadvertently creates hope, although this has not been recognised before.
Changes in hope over time
As found by Radbourne (2008) and Genoe (2009), most participant’s hope was weakened when their dementia diagnosis was given (significantly in Matthew’s case) but it strengthened over time as they came to terms with their situation. Participants adapted to changes in their illness (Genoe, 2009), developing strategies to help themselves (Clare, 2002; Genoe, 2009) and kept busy (Radbourne, 2008; Wolverson et al., 2010). There was none of the hopelessness and sense of futility that Svanström and Dahlberg (2004) reported, and they proved that they were able to develop effective coping strategies.
Locus of control
Similar to Amponsem et al. (2023) hope was a strength, and a strategy deliberately employed to boost wellbeing. All six participants had a very striking internal locus of control, exemplified in the overarching theme ‘defying dementia’. As in Radbourne’s (2008) study, hope was something that they actively sought, rather than passively waited for. There were also parallels with the ideas of resistance (MacKinlay, 2012), fighting spirit (Clare, 2002; Genoe & Dupuis, 2014; Phinney et al., 2007) and the “defiant power of the human spirit” (McFadden, 2004). Participants fought the low expectations placed on them, displaying the type of ‘militant optimism’ described by Bloch (1971).
Connection with others
Amponsem et al. (2023) found that peers “uphold hope and cast away the darkness” (p. 130) but surprisingly peers did not feature as strongly in this study as expected, although they were very important to Ann who said it was helpful as “we’re all the same”. For Matthew a lack of local people of his age with dementia was an inhibiter of hope. Conversely seeing others in his situation could also weaken his hope as it made him face the future progression of his illness. Family members and friends were vital sources of support for all participants as in other studies (Genoe, 2009; Genoe & Dupuis, 2014; Radbourne, 2008; Snyder, 2001, 2003; Wolverson et al., 2010). Healthcare professionals in this study were largely absent from accounts and could be barriers to hope as much as facilitators, with participants sometimes feeling ‘cast adrift’ by statutory services. Robert did say that seeing his consultant was helpful however, and the relationships that Rachel and Ann had with their support workers (employed by a charity) were clearly hope inspiring. Connection with others through the church was important to Richard meanwhile.
Study limitations
The main limitation of this qualitative study was the small sample size (n = 6) and lack of diversity. Most participants, were white, and all British, relatively privileged, and with agentic capacities still intact. Therefore, findings will not represent everyone’s experiences of hope. Future research should aim to recruit a larger, more diverse sample of participants, including people living in deprived areas to ensure a wider range of perspectives are elicited. In this way, structural factors could be better explored. Because one person was used to code most the data this could have introduced bias, as may the presence of spouses during five of the interviews. Finally, findings are based on a relatively old dataset and much has changed in the world since empirical work was completed. However, there are no more recent data available and hope remains a current area of interest (Amponsem et al., 2023; Hare, 2023; Wolverson et al., 2023). Thus, despite these limitations, this study makes a useful contribution to the evidence base, particularly around how hope might be applied to clinical practice (see below).
Conclusions
This study provides empirical evidence that hope is important to people with dementia. As scholars of hope theory point out, ‘if there is some meaning that can be found or constructed around life events (such as being diagnosed with a dementia), hope can take root’ (Callina et al., 2018, p. 22).
With the exception of Amponsem et al. (2023) who studied hope through poetry, it appears few studies have observed that the hope people with dementia express may not always be expressed directly, and can also be expressed indirectly through metaphors, storytelling and reminiscence. The photo diary methodology was effective in eliciting rich data about where people’s hope came from and appeared to be enjoyable for participants, including Matthew; “that sort of pushed us on to do something which I guess wasn’t a part of that at all but it’s been really quite nice hasn’t it? it’s been really nice”. Sources of hope were broadly similar to previous work, however this study found a greater importance of hope enhancing environments than has been seen before. People also appeared to create hope through reminiscence which has not been previously described.
Living with dementia did not destroy peoples hope. Hopefulness was strongly linked to resilience, (exemplified by the ‘windflower’) and was employed as a strategy to deal with challenges participants faced. Hope came largely from within people with dementia, however others could also affect their level of hope. Hope was particularly threatened when participants felt abandoned, isolated or ‘cast adrift’ by services, especially if their personhood was threatened.
Implications for practice
This study has highlighted what might make younger people with dementia feel more, and also less hopeful. This has implications for those working in mental health services where hope is often seen as an important goal in recovery. Professionals can support people’s hope by encouraging them to maintain supportive networks, and to draw on their existing strengths and coping strategies. Interactions with people with dementia should be person-centred, with power imbalances minimised, and focus on finding out about people’s dreams, including leaving a legacy.
Healthcare staff should be aware that cognitive enhancing medication and research opportunities are not necessarily the main source of hope for younger people with dementia living at home, and that inconsistent messages about these can lead to disappointment. Care should be taken of the person’s psychological needs during the diagnostic period, a critical time when people may feel hopeless. Increased support should also be considered at this time, and as Matthew said this need not be time intensive; “a phone call…just one phone call.” Professionals can also support people’s hope by encouraging them to maintain supportive networks, and to draw on their existing strengths and coping strategies.
As many participants found the photo diary task enjoyable and even hope enhancing, this raises the possibility that the task could be adapted and used as a therapeutic intervention in its own right similar to the use of poetry suggested by Amponsem et al. (2023). Further research is needed to ascertain whether this would be useful, and whether hope should be a bigger part of what professionals discuss with people with dementia. Similarly more research is needed to determine whether reminiscence could be used as a more targeted way as a hope intervention, and what form this might take.
Footnotes
Author’s note
Also published as: ![]() an exploration of the perceptions of younger people with dementia about hope. Thesis submitted for Degree of DClinP University of Southampton. This manuscript has been solely submitted to the Dementia: the international journal of social research and practice and, has never been submitted to any other journal.
an exploration of the perceptions of younger people with dementia about hope. Thesis submitted for Degree of DClinP University of Southampton. This manuscript has been solely submitted to the Dementia: the international journal of social research and practice and, has never been submitted to any other journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.