
Abstract
Although the impact of multiple adverse events in childhood is well known, it is equally accepted that the variation in individual trajectories and outcomes is significant. Resilience focuses on positive adaption in the face of adversity, offering a counterbalance to deficit-based research and risk averse, procedurally driven practice. Positive relationships and secure attachments are widely considered to be the cornerstone of resilience, yet, within social work practice, there is a tendency to consider attachment only in relation to children and adults. Three biographical narratives are used to explore resilience and attachment through a narrative identity framework, exploring parents' experiences of multiple adversities over their lifespan, their close relationships, and their experiences of child welfare interventions. It argues for the importance of narrative in social work assessment, particularly in relation to families with complex needs, illustrating how this enables a richer, more nuanced understanding of mothers and fathers as individuals in their own right, and provides insight into how alternative narratives might be better supported and developed.
Introduction
The presence of multiple adverse experiences in childhood has a well-established association with an increased likelihood of harm throughout the lifespan (Felitti et al., 1998), damaging children’s health, intellectual development and mental well-being as well as impairing their ability to form meaningful relationships as adults (Ehlert, 2013; Kendall-Tackett, 2002). Nonetheless, there are the vast individual differences in acute and long-term responses to childhood adversity with some children exhibiting significant effects (Luthar, 2003, 2006) and others appearing “resilient” to negative consequences Daniel and Wassell (2002). Resilience is a dynamic developmental process rather than a fixed trait, and while there are a range of protective factors and person characteristics associated with increased resilience, five decades of research suggest that ‘resilience rests, fundamentally, on relationships’ (Luthar, 2006: 780). Secure attachments develop most optimally when children have positive relationships with significant others, usually parents or carers (Bowlby, 1988; Feeney and Collins, 2014; Ungar, 2012). However, where secure parental relationships are unavailable, evidence suggests that a supportive adult can help to build resilience, encouraging the development of functional coping behaviours (Norman et al., 2012). Studies also indicate that positive marital or co-habiting relationships can ameliorate the impact of adversity experienced in childhood, resulting in improved parenting (Rutter, 2012), and improved physical and mental health and emotional stability in adulthood (Bano et al., 2013). These close and caring relationships are undeniably linked to health and well-being at all life stages, helping to alleviate the risk of developing emotional or mental health problems (Feeney and Collins, 2014).
Although resilience and attachment theories are widely used in child welfare both have been critiqued for their lack of clear definition and varied terminology across studies (Barth et al., 2005; Luthar et al., 2000). Resilience, in particular, has come under attack for being overly focused on individual factors and traits that make up the ‘resilient’ individual. However, over time, it has increasingly been constructed as a multi-dimensional concept with theorists such as Ungar (2010; 2013) making a strong argument for a social ecological approach to resilience which incorporates individual, family, community and cultural factors. Arguably, the strongest critique has been the lack of a consistent and objective measure of what precisely a resilient outcome is, who defines this and across which domain(s) (Luthar et al., 2000).
Given that the operationalisation of resilience can be hugely varied and individual, narrative identity theory provides a valuable framework for not only understanding the stories resilient individuals tell about their lives, but capturing the subjective nature of individual biographies. Building on Erikson’s (1963) theory of psychosocial development, McAdams and McLean (2013) proposed a formation of identity model through narrative, arguing that the stories we tell about ourselves provide powerful insights into who we are, how we came to be and where we think we are going in the future. The model identifies four themes which are considered universal to life story narratives and which reflect many of the key protective factors identified in the resilience literature: communion (interpersonal connection and attachment), agency (motivation and ability to effect change), redemption (deriving good from bad experiences, meaning making), and contamination (good experiences going bad). A growing number of both quantitative and qualitative studies demonstrate that an ability to construct meaning from adverse experiences is central to the resilient narrative and is closely associated with psychological well-being and generativity in adulthood (Adler, 2012; Dunlop and Tracey, 2013). Within this framework, resilience is an emergent quality of the life-story grounded in the narrator’s ability to generate a redemptive narrative which focuses on agency, communion and growth.
Similarly, resilience within the social work literature tends to be associated with more strengths-based, narrative and relational practice approaches (Anderson, 2010; Milner and O'Bryne, 2009; Powell, 2012; Ruch et al., 2010). Wilks (2005) contends that the social work assessment itself is essentially a qualitative, narrative process in which the worker constructs a story about the situation in question. Narrative approaches to practice place an emphasis on power-sharing and engagement in the collaborative co-construction of narrative between service user and practitioner (Milner and O'Bryne, 2009). However, inflexible use of standardised assessment tools and over reliance on electronic systems may reduce the capacity of practitioners to both understand and convey the qualitative nature of service user narratives, resulting in more superficial assessments (Featherstone et al., 2014; White et al., 2009). Without an understanding of both past and present, of the dynamic nature of child and adult resilience and the importance of close caring relationships, assessment and intervention can tend to focus on presenting issues (Brandon et al., 2010) ignoring the importance of longer-term needs and missing opportunities to promote and develop resilience. An increasing tendency to interpret child protection as meeting the needs of the child (Featherstone et al., 2014) can also lead to the needs of mothers and fathers being left unattended, their narratives unsolicited or ignored.
Present study
This paper argues for the importance of narrative in social work assessment, particularly in relation to families with complex needs, and views resilience and attachment as complimentary constructs in the debate. It presents findings from a qualitative study using biographical narrative interviews to explore parents' experiences of key adversities over their lifespan, their close relationships, and their experiences of child welfare interventions, in particular engagement and relationships with statutory social work. Three biographical narratives are used to explore resilience and attachment through a narrative identity framework, illustrating how this approach enables a richer, more nuanced understanding of mothers and fathers as individuals in their own right and provide insight into how alternative narratives might be better supported and developed.
Methodology
Aims and design
The study was developed by researchers at Barnardo's Northern Ireland (NI), the National Society for the Prevention of Cruelty to Children (NSPCC), the National Children's Bureau (NCB) and Queen's University, Belfast. It aimed to identify: the range of adversities experienced across the lifespan; services that were involved with the family at different stages, and barriers and incentives to engaging with services.
A qualitative, biographical narrative methodology was used in a two-stage interview process. The first stage involved a “life grid approach” to chart the key life events of service users, identifying the adversities experienced and levels of service involvement at different times. Life grids are visual tools used to elicit a retrospective account of research participants’ life histories (Backett-Milburn et al., 2008; Wilson et al., 2007) through facilitating the respondent’s ‘voice’ when discussing sensitive issues. On completion of the life grid, participants were invited to participate in a second semi-structured interview to explore their experiences of service engagement, particularly social work engagement. This schedule was structured around the key factors and barriers to service engagement developed by Platt (2012), with the flexibility of the semi-structured approach allowing each interview to be tailored specifically the individual participant.
Selection, recruitment and ethics
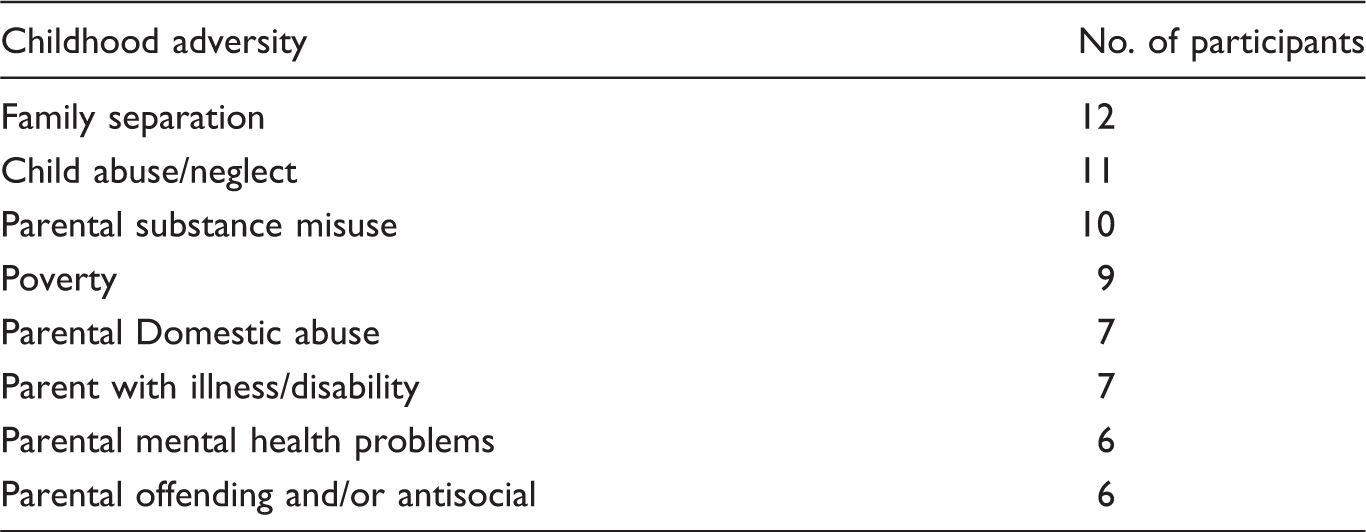
Participant’s experiences of childhood adversity (n = 17).
Manager/practitioners discussed the study with the parent and if she/he expressed interest, and passed on contact details to the research team to follow up. Formal ethical approval was provided by Barnardo’s Research Ethics Panel and all participants were given written and verbal information about the research which emphasised the voluntary nature of participation, made clear the boundaries of confidentiality and explained how data would be securely stored. All participants signed written consent forms for each stage of the research and all those who participated in an initial interview also agreed to take part in a second interview.
Analysis
All interviews were audio-recorded and transcribed. This initial analysis was conducted using content analysis and involved identifying common themes across the cases (Miles and Huberman, 2002; Patton, 2002). While this provided valuable details about the adversities experienced and the relationships participants had with family members, significant adults and professionals (Bunting et al., 2015), it failed to capture the dynamic nature of the life histories in their entirety. Subsequent analysis involved developing a series of case studies which gave a detailed overview of the individual life stories organised around the broad themes of narrative identity theory (McAdams and McLean 2013):
Agency – separation, individual, self-awareness, motivation, insight; Communion – love, intimacy, togetherness, solidarity, close relationships/friendship; Redemption – from bad comes good negative experiences, pain and trauma which result in a stronger sense of purpose, agency and communion; Contamination – from good comes bad, betrayal, trauma, loss and grief which changes the lifespan for the worse.
These themes provided a framework for not only understanding what had happened but the participant’s connections and relationships with others, their hopes and expectations and the extent to which they had achieved or could envisage achieving a different future.
The sample
The overall sample comprised 17 participants who engaged in both stages of the study, completing two interviews each over a 12-month period. On average, interviews lasted 1.5–2 h and were conducted within service premises. Participants were drawn from across all Health and Social Care Trusts in Northern Ireland. Fourteen were females and three males, with an age range of 18 to 49-year-olds and 52 children between them. Of the eight adversities experiences in childhood, family separation was the most common, followed by family separation, child abuse/neglect, parental substance misuse and poverty (Table 1). Additionally, 12 of the participants experienced relationship breakdown in adulthood, 12 had mental health problems, 9 had misused substances and 8 experienced domestic abuse in their adult relationships.
In the majority of cases, the narratives reflected a pattern of continuing adversity across childhood and adulthood. However, some demonstrated high levels of adversity in childhood but limited or less adversity in adulthood while in other cases this pattern was reversed. The three cases studies presented have been selected to reflect this range of changing patterns and the dynamic nature of lifetime adversity. Some minor changes to the specific details of the participant’s circumstances have been made to protect their anonymity.
Case studies
From good to bad and bad to worse: Caroline’s Story
Caroline’s life narrative reflects a classic contamination story, a good life gone bad because of a key event or trauma, in Caroline’s words it is ‘a life of two halves’. Despite experiencing frequent house moves in her early years because of the ‘Troubles’ and her father developing alcohol problems and displaying occasional violence towards her mother in her teenage years, she describes her childhood as a largely happy one with strong attachment relationships between parents, siblings and extended family. Despite experiences of adversity in her teenage years, she exhibits strong communion with her family which is sustained and developed through her marriage in her early twenties and the birth of her son in her late twenties.
We did have a nice house, I mean we had a bloody big six bed-roomed bungalow … and half an acre of land round us, the wee fella had everything, we lived just in front of the beach, you know it was a lovely big place and we loved it … we weren’t that well off, we were comfortable.
It changed everything, I couldn’t live in the same place where I lived, I didn’t have the same life anymore and it changed me as a person totally … I’ve had a lot of depression and problems, and physical health problems all developed too ….
It was disastrous, I mean I tried to … I overdosed, I tried to slit my wrists, I couldn’t deal with it at all, he left us with no home, living with his parents, no money.
I had to go into the dole office then, that was the first time I’d ever had to claim benefits for myself and Mark ….I was messed up, I just had to do what I had to do to survive you know and to look after Mark, even though I know his parents were taking care of us, you know they were good people, they were devastated with it too ….it all happened and there was no coming back from it …
Noel and I had split for a bit, I was in the house with Jonathan, it was a Sunday and I’d had a whole lot of my benefits cut and I had taken, at that stage I had taken on a few bills, I took on my car and I had an overdraft with the bank which I was trying to pay and a credit card and I’d my TV from the catalogue I was paying off … when my money was cut I was left with how am I going to make these payments now and I had to go to Citizen’s Advice to get help and they’d organised with these uns that, they done an income thing you know incomings outgoings, and I’d no money to spare, he says you’re actually like twenty or thirty pounds short you know nothing to spare, so they organised with these uns that I only paid them a pound a month so that’s helped me out a good bit and that just gets paid automatically by direct debit … that worried me sick and I didn’t know how I was going to cope with it and I just went to pieces so I was just sitting there and Jonathan was in next door with the neighbour in playing with her wee boys next door and I just don’t know what came over me but I just got all the tablets that I had and I tried to overdose again and my niece she’d phoned me in the middle of it and I didn’t know what I was saying to her but she knew there was something wrong, she phoned an ambulance.
I had a good life up until, everything was rosy in the garden until the ex-husband done what he done and from then onwards life’s just been hell … I’m a changed person, I’m totally different from what I was before … I was more easier going back then and happy I suppose, you know ….
I would like to have one (a supporting professional) there yeah, I would still like to be with one cos there’s times I feel that I feel like I’m just about to go under.
somebody you know that’s there that you can get in touch with and say right I need help here either for myself my own mental health or the child needs help with something or I need help with him or I don’t know, I just need life, I just need to stop and start over again, do things differently … .
Will it ever be different – Cheryl’s Story
Cheryl is her forties and has five children from a number of different relationships. Cheryl experienced numerous adversities throughout both her early and teenage years; she and her siblings were subject to physical abuse from her father; both parents were heavy drinkers, particularly her mother; her father was emotionally abusive and occasionally physically violent towards her mother, and Cheryl felt neglected and unloved through much of her childhood.
He did hit her once and she hit him back like but it was more emotional you know like you know like he would have treated her like dirt and put her down and stuff like that there but he would have been he would have hit us like with stuff you know like he would have beat us with slippers or hit us with other stuff, snooker cues and stuff like that there or a belt … .
and then we started moving in together there was domestic violence, he held knives to me and held knives down there {indicates vaginal area}, held knives to my throat but I stuck it like for about I think it was about four years and then I ended up working up the courage to leave him … .he drunk a lot as well and it was more whenever he was drunk the violence was worse you know what I mean … .
It more or less started whenever the domestic violence started you know what I mean I would’ve sort of turned to drink so I could cope with it you know what I mean … I think it was after I had my first {Child} … .I think it was my way of dealing with all the violence and stuff like that there it sort of blanked it out for me you know the drink … .
In the broad context of narrative identity themes, Cheryl’s story can be characterised as one of continual and increasing contamination. Her attempts at communion, to develop stable and loving relationships, were thwarted during childhood because of parental violence, neglect, and abuse. Tragically, all her adult attempts at communion have also been met with abuse, a pattern which she herself connects back to her childhood and which she feels makes it difficult for her and her sister to show love to their own children. but I think the reason why I went with people like that was because of the way my dad was, know cos he was like angry and always shouting and I think that’s why I went with people sort of like my dad … my sister would be the same, she’s exactly the same … .
I can’t really talk to her … .no, she doesn’t have like the same opinions as me, you know what I mean about social services. She thinks social services just took her kids, you know what I mean and she didn’t do anything wrong. While I know I did do something wrong, you know what I mean. And she sort of blames social services and everything, nothing was her fault. She is different that way. I know it was my fault and it was me done stuff wrong. But she is completely the opposite so I can’t really talk to her about stuff.
I would like to be completely off the drink, although I have been off it now for a good while, but I would like to have the kids and all back and social services haven’t ruled me out but I mean I went to see a psychiatrist and a psychologist and they says to me I have a what do you call it um an addictive personality and they don’t think that I can stop drinking and stuff like that there so I never even got a chance even to go into {HSC Residential Unit} with the kids or to even prove anything you know what I mean … .
I don’t really have any friends, because whenever I tried to stop drinking and all the people that I was hanging about with was just all my drinking friends do you know what I mean so I stopped bothering with them uns and I don’t really have any friends now … .
The redemptive relationship – Kevin's story
As a young child, Kevin lived in another part of the UK until his family returned to Northern Ireland when he was seven years old. Kevin described a relatively happy early childhood although he remembers his dad being stressed through working several jobs. However, everything changed when his parent’s relationship broke down and they divorced at the age of eleven and his mother remarried. Kevin’s memories of what led to the divorce and his mum and dad’s relationship are patchy, although he understands from relatives that his dad was often violent towards his mum. I’ve been told later on what happened but I don’t remember any of it … .like my dad had my mum by the throat one day and em I walked into the kitchen and she says, only I walked into the kitchen and he probably would have kept going you know, but I don’t remember any of that … .
bad, very bad … there was a lot of violence … back then it was never towards mum, and my other brothers were kind of left alone you know, they might have got a bit here and there you know, but for me it was every day … .
she seen it all … like he was extremely violent, there was one time, our living room would’ve have been twice the size of this lengthwise and maybe longer, and he lifted me and threw me up against the wall on the other side of the room and my mum just walked straight past me and I was lying on the floor you know … .
… when she was heading out and never coming home … Between worrying about her and worrying about the two kids, and you were the only one there to look after these two kids and stuff, it is hard to explain … that would have been the lowest point of my life.
Following the loss of contact with his children and the death of a close friend, Kevin developed mental health problems in his mid-twenties. Although he had previous experiences of depression which he linked with the violence and abuse of his childhood, this period of poor mental health was much worse. Kevin describes the loss of his friend as triggering an explosion of negative feelings that he had previously held in. Although work helped him cope during the day, he started using cannabis in the evenings as a coping mechanism. Kevin saw a psychiatrist and took medication for several years but then stopped his appointments. While he had found some aspects of psychiatric support helpful, he described seeking a greater level of interaction and connection than had been provided:
Well I got to talk to somebody who didn’t turn round and say that didn’t happen like that … So that was a kind of help. There wasn’t really much in the way of talking back to me. You know, I was talking to somebody and they were listening, but they weren’t really talking back … l … I would have liked something … just even something like this here, you know the way we are talking, you are asking questions back … .
It was not professional assistance but rather the development of his strong personal relationship with Sara that provided the major turning point in Kevin’s life. Friends for many years, they subsequently married and had two children of their own. Kevin describes his relationship with Sara in strongly redemptive terms and through his communion with her is able to narrate a life-story of growth and stability emerging from a chaotic childhood and early adulthood. Within this supportive context, he also describes being able to develop a relationship with his stepfather before he died in his fifties.
Oh massive, a big turning point in my life … we know each other that well, she knows when I am tired, that is why I am upset because I am knackered. And I am the same with her … but it makes so much of a difference. Being able to actually talk.
mine’s hectic [lifestory], mine’s moving from place to place and you know not holding down jobs and stuff like that there, drinking a lot, but with Sara … .she’s had a big influence on me like, she was the one who looked after me whenever the kids were away and I went into depression and she looked after me the whole time like and you know she was completely understanding … .
Kevin came into contact with social services the year before the interview when his children from his relationship with Emily were removed from her care because of household substance misuse, domestic violence and allegations of physical abuse and neglect of the children. Since then, Kevin and Sara have been working hard to secure custody of Kevin’s eldest children, completing various parenting courses and assessments. Kevin's narrative suggested high levels of agency and growth through his learning from the various interventions and his achievement in passing them with flying colours. Despite some delays in the process, Kevin is positive about the future and anticipates that his children will come to live with him and Sara soon.
… I haven’t found it that bad. Anything that they have asked me to do, I have done it, I have passed everything.
Discussion
In keeping with both the resilience and narrative identity literature, close relationships were a key aspect of the stories participants told, providing insight into their childhood and adult attachment relationships. While routinely used by child and family social workers to guide work with children, attachment has received considerably less attention in relation to work with parents. Attachment, or communion in the language of narrative identity, is itself a life-course construct with stable relationships being integral not only to childhood but to adults throughout all life stages. If we take the case of Cheryl, her attachment needs have rarely been adequately met, her close relationships have been characterised by violence and abuse, yet her desire to establish a connection with others is apparent. Featherstone et al. (2014) argue that through the privileging of the risk assessment paradigm, we have lost the vocabulary to talk about the 'irrationalities' of intimate relationships, leaving us unable to engage in conversations about sexual relationships or recognise the powerful feelings of loneliness and fear that parenting alone can engender. Hearing Cheryl's life-story, recognising her need for connection gives us another way to understand her, a way that moves beyond characterising her as an alcoholic, who routinely becomes involved in dangerous relationships and puts herself and her children at risk. It allows us to identify her attachment seeking behaviours as not only normal, but valid and important, worthy of our attention.
We can clearly see from Kevin's narrative the power of the redemptive relationship. From a similar background as Cheryl, he has been able, in part, to recover from extremely negative and disruptive childhood relationships, mental health problems, relationship breakdown and separation from his children Keeling and van Wormer (2011). Having a stable loving relationship in which he is understood was a key turning point in his life and although the problems have not gone away, they are manageable within the context of the emotional support he receives from his wife, providing a sense of resilience. This is in stark contrast to Cheryl's experiences. Without any secure base or network of support to build on, the life changes she has embarked on will likely be difficult to sustain. Understanding Cheryl's lack of connection raises questions as to how she might be supported to meet her attachment needs in a safe way, not just as a means to secure the return of her children but as a person in her own right. How might we build on those small glimmers of resilience that emerge from the bleakness of a lifetime of abuse, how can we support her to maximise the progress she is trying to make, how can we give her hope?
Caroline finds herself in a similarly bleak situation. From a very different background than either Kevin or Cheryl, she experienced a relatively stable upbringing and went on to develop stable relationships in her twenties resulting in marriage and the birth of her child. However, her sense of stability and security was decimated by the unexpected breakdown of her marital relationship. Her loss and grief are palpable, and she is grieving not just for the end of the relationship but the life that was, the identity she had as a married, relatively well-off mother and homeowner. Caroline has been unable, as yet, to construct an alternate identity to develop a narrative which takes her beyond contamination to growth and redemption. She is positive about engaging with services but fearful of being left without social support, recognising her own vulnerability and difficulties in coping.
The narrative identity approach helps us to reframe how we understand the lives of parents like Caroline, Cheryl and Kevin and begins to ask how we might go about changing the narrative, and what kinds of services and social support might help to develop and promote resilience in these circumstances? While narrative theory’s emphasis on co-construction and power sharing may appear at odds with the process driven and risk averse nature of modern practice (Featherstone et al., 2014; Munro, 2011), through assessment social workers are already engaged in the construction of a client narrative (Wilks, 2005). Using a narrative approach means explicitly recognising the voice and experiences of the service user as central to the change process. This does not mean that challenges are ignored but rather that the focus of assessment and intervention is shifted more towards ‘need’ and less toward ‘risk’. Instead of simply identifying parenting deficits, strengths-based and solution-focused approaches to social work practice are used to uncover the individual’s unique survival story and facilitate transformation from a problem saturated narrative to one which celebrates growth (Anderson, 2010; Milner, 2001).
While the case studies highlight how narrative approaches can be used in direct social work practice, they also point to the need for sustained emotional and social support over and above the ‘traditional’ social work interventions that are routinely made available. Innovative approaches which foster identity and relationship building, promote and encourage resilience through social support and community integration are also needed to address isolation and chronic low self-esteem. While many groups are at increased risk of social exclusion and marginalisation, arguably those parents who have had their children removed from their care are the most marginalised group of all. Shame and stigma emanating from the 'spoiled identity' of parental failure, in particular the gendered identity of a ‘bad’ mother, can act as significant barriers to engaging with others.
Lack of social integration in a network of meaningful relationships predicts mortality more strongly than many lifestyle behaviours such as smoking or physical activity (Holt-Lunstad and Smith, 2012). Recognition of this had led to the development of a wealth of community initiatives aimed at building social networks and social capital through befriending schemes, mentoring peer programmes and other community-based activities (Akister et al., 2011; Berrick et al., 2011; Windle et al., 2011). Although social work involvement in such initiatives has clear resonance with the profession’s value and skills base, social work tasks in the UK have increasingly been conceptualised as reactive and risk orientated rather and proactive and supportive. Too often, practitioners report that they are engaged in surveillance rather than support (Baginsky et al., 2010). This raises important questions as to the future role of the profession in developing more preventative, community-based practice. Growing calls from academics and practitioners to “reclaim” social work values and “re-imagine” practice (Featherstone et al., 2014; Ferguson, 2009) suggest that the profession’s own discourse is also evolving. Changing the narrative for both professionals and parents will require a clear vision of the contribution social work can and should make to preventive, strengths-based community services.
Conclusion
This paper argues for the importance of narrative within social work practice, not just as a means of enabling practitioners to better connect with and understand the lives of service users, but as a way of developmentally understanding resilience and attachment and maintaining a strengths-based focus when working with families in complex situations. Focusing on what individual narratives say about the identity of the narrator and their belief in their ability to effect change can act as an important starting point to considering how such narratives might be enhanced or revised and what services might be beneficial in achieving this. A number of the life-stories presented here illustrate that some vulnerable parents lack not just physical resources but internal resources and external support. Put simply, they often have nowhere to go and no one to turn to outside of formal services. Developing ways to actively build support networks and enhance attachment bonds amongst vulnerable mothers and fathers are needed to reduce isolation and build resilience. As social work is pushed more towards risk assessment and surveillance, the role social work can and should play in this development process remains a key question.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.