
Abstract
Parents have a major influence on young children’s diets, food choices and habit formation. However, research concerning parental influence on children’s diets is limited. Qualitative research informs quantitative research with a narrative of ‘what works’ and is a valuable tool to inform intervention design and practice. This article presents a systematic review of qualitative research with parents of preschool children and their influence on their child’s diet. Nine studies were identified. Findings highlight the need to promote culturally tailored programmes to combat specific cultural differences such as attitudes; perceptions and concerns; address common barriers to providing healthy foods and challenges faced by lower income families; the use of food to shape a child’s behaviour; that children will grow out of excess weight; common misconceptions such as a heavier child is healthier and depriving a child’s food request could result in starvation. Research on parental understanding of healthy diets and feeding practices is lacking. Further insights into how to positively influence children’s diets will come from research examining parent feeding practices and nutrition knowledge.
Introduction
Overweight and obesity status has fast become an epidemic throughout Western society. The World Health Organization (2011) states that worldwide rates of obesity have more than doubled since 1980, including approximately 43 million children under the age of 5 years. In Australia, the 2004–2005 National Health Survey classified over half (53%) of people aged 15 years or older as overweight or obese (Pink, 2008). Although recent reports indicate that overweight and obesity have plateaued in Australia in recent times, 21–25 per cent of children aged 2–18 years were recorded as overweight or obese in 2008 (Olds et al., 2009). One of the best approaches to addressing this serious health issue may be to improve children’s diets.
A healthy diet is best developed and encouraged at a very young age as it is well understood that existing dietary practices are more difficult to change, particularly once they have become habitualised (Jager, 2003).The first 5 years of a child’s life are considered formative years when parents are primary educators and role models in the family environment and therefore have a major influence on their child’s diet (Fisher et al., 2002). In order for parents to encourage their children to make healthy food choices, they need to be well informed about both the positive and negative outcomes of healthy versus unhealthy food choices and dietary habits. Parents may also benefit from the implementation of the skills required to create an optimal environment for children to develop healthy eating habits (Golley et al., 2007).
Style of parenting, parental feeding practices and parent nutrition knowledge are among a list of factors identified as having an influence on child dietary behaviours and food preferences. Accordingly, a growing number of researchers are recognising the importance of early intervention and the role of effective parent feeding practices in promoting healthy diets (Birch, 2006). The years before children go to school could be an optimal time for parents to intervene with the promotion and formation of healthy habits. For this review, we have focused on children who are 2–5 years old and starting to learn to make their own decisions and choices while still under the primary influence of parental guidance and family environment.
Parent feeding practices
There is some quantitative evidence indicating that infants and toddlers have an innate ability to self-regulate energy intake (Johnson, 2000), and this has been identified in babies as early as 6 weeks old (Fomon, 1993). Similarly to breast-feeding on demand, infants and toddlers need to eat small amounts of food more frequently (Skinner et al., 2004). Children at age 3 have been reported to stop eating when they were satiated despite food availability, whereas the older children at 5 years reportedly consumed more if it was available, regardless of hunger (Birch and Davison, 2001). Qualitative research posits that this decline in self-regulation of food intake with age not only influences subsequent intake but may also be a reflection of parents using food to shape their child’s behaviour (Baughcum et al., 1998) and could influence the child’s intake via their attitudes towards food.
To date, much of the research on parent feeding practices and children’s diet has focused on restrictive feeding practices. These practices commonly involve higher levels of control, which tend to be associated with an authoritarian style of parenting. This practice removes the responsibility from the child to learn to monitor their own energy intake and/or their ability to respond to internal cues (Birch, 1999; Fisher and Birch, 2002). Consequently, inadvertently encouraging a child to respond to environmental triggers is an eating habit that could persist into their adult years and contribute towards overeating and potentially overweight (Carnell and Wardle, 2007; Faith et al., 2004b; Fisher and Birch, 2002; Moens et al., 2007; Musher-Eizenman and Holub, 2006). However, research suggests that tactics used to limit a child’s consumption of undesirable (unhealthy) food items can be counterproductive (Faith et al., 2004a). For instance, food used as contingency or bribe for reward may predict a decreased preference for that food, whereas restricted, reward foods may become more attractive (Birch et al., 1984). Therefore, instrumental or contingency feeding may have negative results, which is particularly relevant if the contingency food is a healthy food item exchanged for an energy-dense unhealthy option (e.g. ‘eat your vegetables and then you can have dessert’ (Newman and Taylor, 1992)). However, research in this area has not consistently associated restriction with excess consumption or weight (Campbell et al., 2006; Carnell and Wardle, 2007; Haycraft and Blissett, 2008; Powers et al., 2006).
More recent research considers differing types of parental restriction and control such as ‘overt’ and ‘covert’ control (Ogden et al., 2006). ‘Overt’ control describes when a child is aware of the restriction and the food is available in the home, whereas ‘covert’ control pertains to when the child is not aware of the restriction and the food is not available in the home. ‘Overt’ control has been shown to predict increased intake of healthy snacks, whereas ‘covert’ control appeared to predict decreased intake of unhealthy snacks.
Restrictions for weight control or for health reasons are of two differing types that could also contribute to the nature of parent feeding practices and child diet (Musher-Eizenman and Holub, 2007). Restriction for weight appears to predict externally motivated eating (e.g. eating in the absence of hunger during unrestricted times), whereas restriction for health reasons does not (Musher-Eizenman and Holub, 2006). This has been seen longitudinally with children aged 5–6 years and older children aged 10–12 years (Campbell et al., 2010a).
Additionally, a recent review of interventions looking at parental influences on child diet identified five studies that attempted to include parent feeding practices. Despite only one of the studies reporting specific intervention content, there appeared to be positive results in child diet when parents were informed of appropriate feeding practices (Peters et al., 2012). However, research in this area of health promotion and removing unhealthy options from the younger child’s environment is limited.
Parent knowledge of diet and nutrition
In addition to parenting and feeding practices, increased nutrition knowledge in mothers has been associated with healthier diets (lower in fat and higher in fresh fruits and vegetables; Gibson et al., 1998). Recent research suggests that these positive associations may be mediated by home food availability (Campbell et al., 2010b). For instance, home fruit and vegetable availability at 2 and 4 years of age is reported to predict food preference at 8 years of age, suggesting that early exposures to food may mould later food preferences (Skinner et al., 2002). This further supports the claim that ‘the more a mother knows about health and nutrition the better is the overall quality of her child’s diet, for preschoolers more so than older children’ (Blaylock et al., 1999: i). Therefore, promoting nutrition knowledge in parents of young children could be pivotal to the child’s future health and the prevention of overweight.
Informing research
Quantitative research is designed to generate an evidence-based statistical account of intervention effectiveness and significant associations of relevance. However, quantitative research does not consistently identify specific elements of parenting programmes or nutrition information provided in interventions. Therefore, interpretation of specific components that may encourage behaviour change is difficult. In fact, our recent review identified only one study with a feeding practice component that detailed individual intervention sessions, whereas the other four studies included in the review provided a broad concept only (Peters et al., 2012). However, there appeared to be positive results in child diet when parents were informed of appropriate feeding practices. Therefore, qualitative research can inform intervention design with a narrative regarding the content and delivery of what does and/or does not work. Due to the complexity and flexibility of qualitative analysis, this textual research is a valuable tool to inform intervention development by way of focus group discussion, one-on-one interviews and observations. Examples of this include evaluation and understanding of food safety policies and general nutrition knowledge (Sangster et al., 2003); apprising of concepts, opinions and consensus in relation to child diet and behaviour in order to further inform policy and intervention development (Kaiser et al., 2001; Korwanich et al., 2008); understanding of language used for different cultural groups (Hughes et al., 2005, 2006); and post-intervention research to discuss perceived relevance and content evaluation (Condrasky et al., 2006; Haire-Joshu et al., 2008; Horodynski et al., 2004; McGarvey et al., 2004; Schwartz et al., 2007; Wardle et al., 2003). This process of qualitatively collecting data enables the identification of discrepancies and misunderstandings, which can then be rectified to produce a refined, more easily understood culturally relevant and appropriate programme (Hughes et al., 2006; Kasemsup and Reicks, 2006).
Therefore, the purpose of this article is to systematically review qualitative research concerned with parenting practices, parent’s nutrition knowledge and child diet. Common themes about these practices will be identified.
Methodology
This review specifically targeted peer-reviewed qualitative research conducted with parents of children aged 2–5 years discussing parental feeding practices, parent knowledge of nutrition and/or child diet, child food intake and body mass index (BMI).
Search strategies
At the first stage, MEDLINE, PsycINFO®, EMBASE®, CINAHL and CENTRAL databases were systematically searched to identify published research from 1996 to 10 September 2009 using various combinations of the keywords displayed in Table 1.
Concept table of keyword search terms.
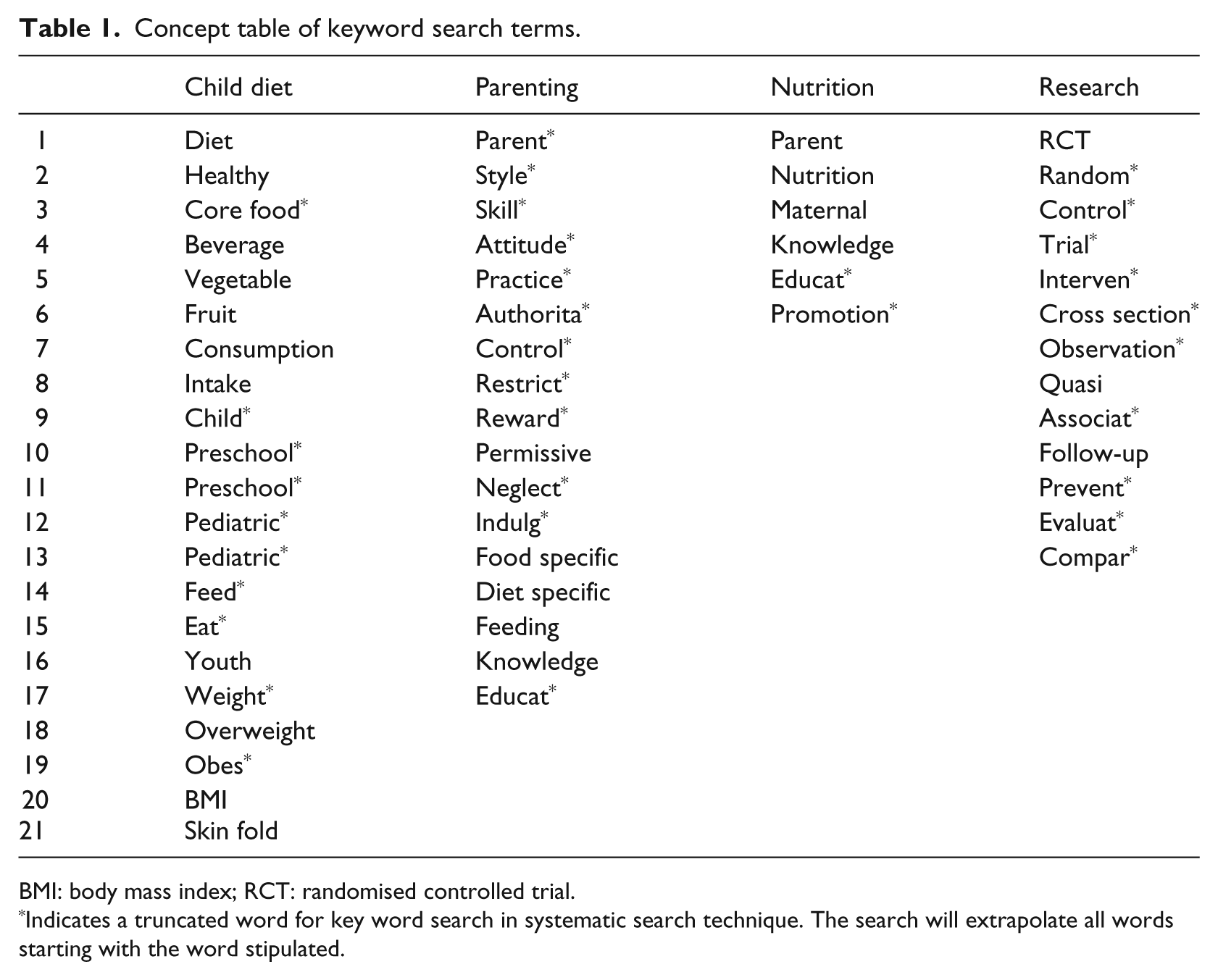
BMI: body mass index; RCT: randomised controlled trial.
Indicates a truncated word for key word search in systematic search technique. The search will extrapolate all words starting with the word stipulated.
Refined searches resulted in a total number of 663 references as listed in Table 2.
Number of search hits for each database.
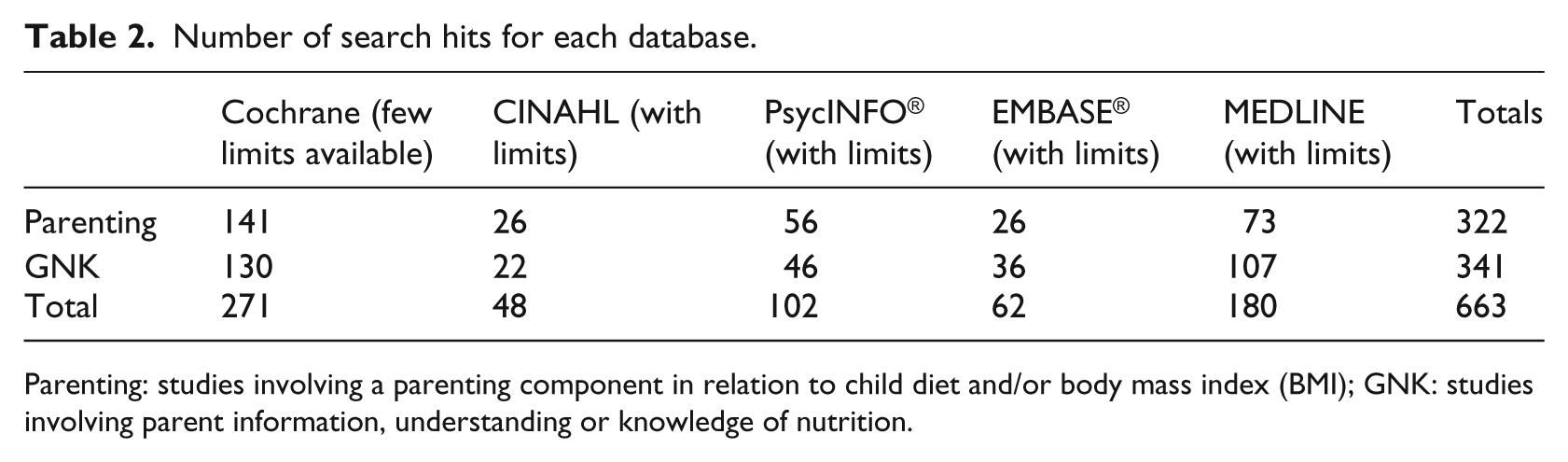
Parenting: studies involving a parenting component in relation to child diet and/or body mass index (BMI); GNK: studies involving parent information, understanding or knowledge of nutrition.
Specific search criteria produced a total of 352 articles. Exclusion criteria eliminated articles focusing on malnutrition, eating disorders and primary-school-based recruitment. Further scanning reduced the total to 133 abstracts for review. The first and second authors, Jacqueline Peters (J.P.) and Natalie Parletta (N.P.), reviewed abstracts and resolved discrepancies, resulting in a total of 95 articles, which were organised into three groups: (1) intervention research (n = 17; Peters et al., 2012), (2) qualitative research (n = 9) and (3) observational research (n = 69). The purpose of this article was to review the nine qualitative articles (Figure 1).
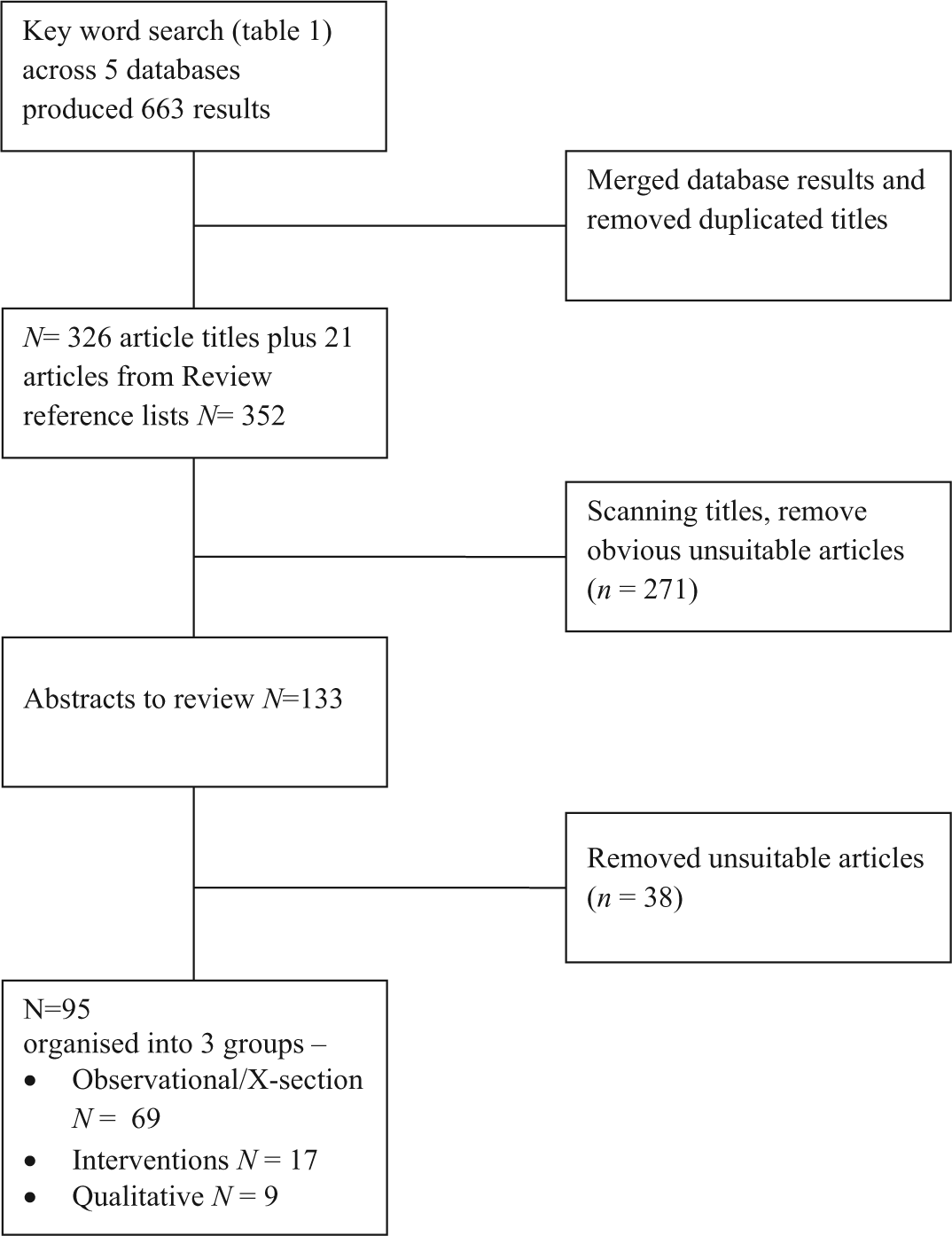
Flow chart of literature search.
No quality assessments of these qualitative studies were conducted because ‘precisely how “weak” qualitative findings should be attenuated or excluded in any synthesis is not yet clear’ (Dixon-Woods et al., 2006: 35). Consequently, no further articles were omitted from the list and the final review was based on the nine identified qualitative articles. An extraction tool was developed to systematically obtain research specifics and identify methods used for each project. Extracted information is compiled in a quick reference table (Appendix 1).
Results
Search criteria targeted qualitative research conducted with parents of children aged 2–5 years; however, results produced some studies that extended this range to include children from 12 months to 8 years. The nine included studies examined a variety of settings: childcare/preschool (n = 6), community (n = 1), paediatric practice (n = 1) and a mixed setting (n = 1). Although some of the interventions included other components, such as physical activity or parent’s weight, only information relevant to this review will be summarised. Group and project details, and discussion content, varied substantially (see Appendix 1). All summaries appear below, grouped by setting.
Preschool/childcare settings
Haerens et al. (2009)
‘Identification and Prevention of Dietary- and Lifestyle-induced Health Effects in Children and Infants’ (IDEFICS) is a standardised healthy eating community intervention aimed to increase the likelihood of behaviour change. To inform the development of this programme, focus group research was conducted across eight different European countries and touted to be ‘the first international study’ of this calibre. Involving three groups, namely, (1) children aged 6–8 years (n = 155), (2) parents of children aged 2–4 years (n = 106) and (3) parents of children aged 6–8 years (n = 83), each location received a protocol manual outlining requirements and methodology to ensure standardisation. Results relevant to this review included a recognised difficulty for young children to prepare fruit provided for snacks when they are outside of the home environment (e.g. school, preschool) and parental concern that the child could be stigmatised for being the only one with healthy snacks.
Parents generally had a positive attitude about the food policies and the ability of kindergartens to facilitate healthy eating habits in their children. However, they commonly identified barriers to healthy feeding practices as time constraints with healthy food taking longer to prepare, children’s unhealthy food preferences, high cost of fresh healthy food products, high availability of unhealthy foods in the home and difficulty reading food labels. Facilitators of healthy eating habits were identified as parents actively modelling healthy eating behaviours, offering healthy snacks that appeal to children, availability of healthy foods and not having unhealthy foods in the home environment. Low socio-economic status (SES) groups were less likely to restrict unhealthy foods, and mid- to high-SES groups were influenced by quality rather than quantity. This research suggests that intervention strategies need to recognise that priorities and influences are likely to differ between SES groups and should aim to promote environments in which ‘healthy eating behaviours are the easiest choice’ (Haerens et al., 2009: 388).
Horodynski et al. (2009)
This research evaluated the maternal feeding practices of 27 African American low-income mothers of toddlers aged 12–36 months recruited from two Early Head Start centres in the United States. The first of four main themes to emerge was in relation to maternal perception of a healthy child, which included eating well and being active and happy. The second theme pertained to child food choices and revealed limitations in offering fruits and vegetables due to perceived child preference. Third, the expectation of the child’s autonomy and self-regulation led some parents to use encouragement to eat. The last theme involved mealtime context and interaction, which included mealtime duration, location and the role of family socialisation at meals. Concerns included maternal fear that children who were picky eaters were at risk of malnutrition and appeared to prompt authoritarian style practices such as force-feeding. One mother explained her deliberation between buying a smaller quantity of healthy fresh food and purchasing a larger quantity of energy-dense, unhealthy food for the same cost, which she believed was better value for money and more likely to satiate her child. This research identified the important challenges faced by lower income families such as cost, convenience and quality versus quantity in food choices (Horodynski et al., 2009).
McGarvey et al. (2006)
To identify cross-cultural differences and to further inform a childhood obesity intervention, 25 mothers were allocated to one of four focus groups. There was one focus group per ethnic group and each was conducted in the native language of the participants: White (n = 8), African American (n = 6), Hispanic (n = 6) and Vietnamese (n = 5). No child age range could be ascertained from the report, although all children attending the Women, Infant and Children (WIC) centres were aged 5 years or younger. However, this research does refer to ‘older’ children as well. Group discussions targeted prevention strategies, specifically with parent perceptions, attitudes, knowledge, beliefs and barriers with reference to child feeding practices and behaviour (including physical activity). In relation to influences on child feeding practices and dietary intake, comments were made in both the African American and White groups that their own mother’s knowledge would be outdated, whereas the Vietnamese group considered it a traditional influence dating back thousands of years. Apart from the Vietnamese group who trusted a child’s claim to have eaten enough, all other groups expressed a broad range of views in relation to children’s inability to determine if he or she has eaten enough and admitted to incidences of overriding child display of satiation.
White and Hispanic women were concerned about overweight once a child started school due to stigmatisation and health issues; however, African American and Vietnamese women were more concerned with underweight. A common perception was that if a child experienced overweight at 3 or 4 years of age, they would outgrow it. All groups reported using food to shape behaviour (as a contingency and/or reward), and many parents believed child feeding problems to mostly originate outside of the home environment (e.g. child care, preschool, grandparents) (McGarvey et al., 2006). The key information gathered from this research was used in the development of Fit WIC, a preschool child obesity prevention programme.
Crawford et al. (2004)
Accessing five WIC sites across California, semi-structured focus groups were used to further inform and update nutrition education methods by evaluating the attitudes and beliefs of 43 Latino mothers towards their 2- to 5-year-old child’s diets. All participants attended a 2-hour session wherein 15 main themes emerged across four domains.
The first domain pertained to parent health beliefs in relation to child weight. Heavier children were perceived to be healthier, whereas thinner children were perceived as unhealthy. Parents did not believe that ‘extra weight’ on children was unhealthy if the children felt good about themselves and appeared happy in the family environment. The second domain reflected beliefs about the causes and effects of childhood overweight. These mothers predominantly believed that childhood overweight was a result of genetics or a condition their child would outgrow. However, they also recognised that being overweight caused children to be inactive and lethargic provoking negative stigmatisation from their peers. The third domain included themes regarding the impact of life values and concerns. These included how money, time constraints and convenience foods threaten cultural beliefs and compromise a parent’s capacity to offer nutritious food to their children. Finally, the fourth domain spoke to strategies that parents used to instigate changes in children’s dietary (and physical activity) behaviours. Parents strongly believed modelling to be a key strategy in child behaviour change. There was also a preference for facilitated group discussion to inform mothers of necessary nutrition information and provide a setting where they could share ideas and experiences with each other, rather than continue with traditional teaching methods (Crawford et al., 2004). This research project highlighted the need for consideration of cultural differences and beliefs in prevention programme design as well as focusing on a positive message of healthy eating rather than weight loss.
Jain et al. (2001)
Three focus groups of six mother/child pairs who were predominantly overweight or obese were recruited mainly from WIC centres. The project assessed maternal perceptions in determining weight and overweight, why children become overweight and barriers to preventing or managing overweight. Results indicated that generally the mothers did not accept the health professional classification of overweight in children and believed that the height–weight charts were not relevant for their child. Parents only considered weight to be a concern if they were purchasing clothing too frequently, if the excess weight impaired the child’s ability to be physically active or if weight was a point of stigmatisation/teasing from peers. Low self-esteem and physical inactivity appeared to be the two most critical points considered by these mothers. However, some believed that excess weight caused inactivity, and not vice versa.
Although some mothers accepted that parental role modelling could influence a child’s behaviour, most believed their child’s weight to be biologically predetermined or that the child would grow into their weight. In relation to weight management, difficulty in limiting food was expressed. Mothers derived pleasure and emotional reward in nourishing their child and believed denying a perpetually hungry child of food was tantamount to starving the child. It was also revealed that due to their own childhood weight history, mothers were more inclined to protect the child’s mental health and promote buffers against being teased rather than address their physical health by preventing or treating a weight condition (Jain et al., 2001). This research identified that although neither health professionals nor mothers agreed on the definition of overweight, they did agree that children should have healthy diets, and thus that promoting health should be the focus of future research rather than labelling weight status.
Sherry et al. (2004)
A total of 12 diverse groups of mothers with children aged between 2 and 5 years were recruited to examine the impact of SES and culture on attitudes, concerns and practices with child feeding and on perception of child weight. Of the 12 groups, 9 groups were of low SES, 3 of which were White American (n = 22), 3 African American (n = 24) and 3 Hispanic (n = 27). The remaining 3 groups were White American middle-income earners (n = 28). Six key themes were identified: (1) goals and beliefs, which encompassed what constituted good nutrition, included encouraging children to eat more nutritious food, less sweet-processed and high-fat foods, plus increasing availability of healthy foods while decreasing availability of unhealthy foods; (2) determinants of food availability, encompassing cost, was key in 6/9 low SES and all the middle SES groups, whereas Hispanic groups were concerned that ‘what the child needed’ was nutritious, preferable and convenient; (3) mealtime environment and promoting consumption in young children, which encompassed food preparation, mealtime structure, conflicts regarding food, food preferences and portion size; (4) strategies to persuade children to eat, which encompassed preparing preferred foods, actively encouraging eating, use of food bribes and rewards for eating and using desirable foods and beverages as rewards; (5) reactions to child claims of satiation with mothers’ interpretation of a child’s expressions of fullness revealing little confidence in a child’s innate capacity to regulate food intake with most mothers interpreting ‘fullness’ as boredom, whereby consequently, mothers actively encouraged or pressured their child to eat; and (6) the last category was in relation to concerns and beliefs about child weight with most groups expressing a belief that underweight was cause for concern, whereas others believed overweight to be an indicator of wellness. The African American groups all believed the child would outgrow excess weight, while other groups (3 low SES, 3 middle SES and 1 African American) believed both genetics and environment determined child weight (Sherry et al., 2004). This research identified the need to verify cultural and income differences in concerns, attitudes and practices in relation to child feeding and perceptions of child weight.
Community-based setting
Adams et al. (2008)
Three different American Indian (AI) communities participated in focus group research, which aimed to describe parental perspectives regarding child health, diet and physical activity. Participants were parents (n = 42) of 5- to 8-year-old children and were recruited from the Wisconsin Nutrition and Growth Study. A total of 10 to 12 interviews and observations were conducted at each location. Six main themes emerged from the following two constructs: (1) environment, which mainly involved discussions in relation to physical activity, also included family support with time-consuming chores such as food preparation and cleaning up; and (2) health, which pertained to risk and child safety (physical activity oriented), parental views and perceptions of child health and beliefs about parenting. The research highlighted that some parents did not want to control their children or dictate food choices, which was particularly so if the parent had also been controlled as a child. Other parents communicated having no control over their child’s diet.
Interestingly, parents wanted their child to eat healthier foods but did not provide the right environment to facilitate this, displaying incongruence between intention and behaviour. There was also a ‘leniency’ in parents who appeared to be focused on the immediate outcomes of the ‘here and now’ of child diet, rather than considering the longer term outcomes. An explanation for this could be that the main priority for families in these communities was survival in the present ‘just living for now’. Therefore, this research highlights the influence of the AI culture on parent’s values, beliefs and priorities. Information obtained from this research was subsequently used to ‘design a family-based healthy lifestyles intervention for families of 2–5 year old AI children’ (Adams et al., 2008).
Paediatric practice setting
Bolling et al. (2009)
Parents of children aged 2–6 years were recruited from private paediatric practices in suburban, rural and urban areas. Focus groups ranged from 3 to 7 participants per group with duration of approximately 90 minutes, or until responses to themes reached saturation. Specific areas of interest to this review were as follows: (1) identifying health risks that motivate parental behaviour change, (2) perceived barriers to modifying dietary behaviour and (3) general recommendations for paediatricians to help modify the feeding practices of parents with overweight preschool-aged children.
Many of these parents shared the common misconception that fruit juice consumption was the equivalent of whole fruit consumption. Therefore, their main dietary barrier to providing a healthful diet was restricting the consumption of 100 per cent fruit juice due to juice being included in the sweetened beverages group. Another common barrier to providing a healthful diet was increasing fruit and vegetable consumption to 5 servings a day. Children reportedly did not like vegetables and ‘would go hungry’ rather than eat them (Bolling et al., 2009: 174). This often resulted in a struggle that contributed towards parent–child conflict and child tantrums. Parents also expressed a desire to have paediatricians give advice on appropriate nutrition requirements to both parent and child, with a general consensus that early intervention to address child weight concerns would be advantageous.
Mixed setting
Baughcum et al. (1998)
With an aim to gain perspectives from both dieticians and lower SES mothers about beliefs and practices associated with childhood obesity, this research consisted of three groups of mothers and one group of nutritional professionals. The professional group (n = 15) consisted of only WIC dieticians, two groups (n = 3 each) consisted of mothers who were recruited from one particular practice and one group (total n = 8) consisted of all teenage White American mothers (n = 3) and African American mothers (n = 5) who were recruited during postnatal home visits. A major theme was the perception (misconception) that a heavier infant was healthier and considered to be indicative of successful feeding practices and parenting skills in general. These mothers often attributed their child’s overweight condition to family genetics. The second theme related to the concern that the child was not eating enough. A consequence of this concern was the likely introduction of solid foods at very young ages. Mothers reported this as more convenient than preparing separate meals for individual family members, which were also considered to be cost-effective when family members all ate the same foods. However, this rationale led to feeding the child the same ‘table foods’ as the adult and as frequently. Mothers from these groups set few limits on their child’s intake, allowing them to eat what they wanted and when they wanted. Therefore, they believed, despite health professional advice, that depriving a child a requested food item that had already been introduced into their diet was tantamount to ‘starving’ the child. The last theme related to using food as reinforcement or as a coercive tool to shape behaviour or to placate an unsettled child rather than to satiate hunger.
Despite the small sample of mothers in this study, consistent beliefs and practices regarding child feeding practices were found between groups. These themes were confirmed by the perceptions of the dietician group in relation to their experience with client concerns. This research identified the common misconception that a bigger child is a healthier child. There was also fear among these mothers of underfeeding their child, resulting in early introduction of solid foods. Additionally, mothers admitted to using food to reward and shape behaviour or placate an unsettled child (Baughcum et al., 1998).
Discussion
This article evaluated peer-reviewed qualitative literature conducted with parents of children aged 2–5 years discussing parental feeding practices, and/or parent knowledge of nutrition with child diet, and/or BMI, published from 1996 to mid-September 2009. Findings from only nine qualitative studies that met the inclusion criteria highlight the need to promote culturally tailored programmes to combat specific cultural differences such as attitudes, perceptions and concerns, address common barriers to providing healthy foods and challenges faced by lower income families, the use of food to shape a child’s behaviour, that children will grow out of excess weight, common misconceptions such as a heavier child is perceived as being healthier and depriving a child’s food request could result in starvation. Therefore, despite the increased attention obesity prevention and management research has gained over the years, it would appear that this area of research demands further attention, particularly with reference to young children in the areas of parental nutrition knowledge, parent perceptions of child weight and cultural sensitivity in intervention design.
All qualitative reports reviewed in this article included a focus group component. Apart from one research project that did not report number of sessions (Baughcum et al., 1998) or two that did not report the time frame (Baughcum et al., 1998; McGarvey et al., 2006), focus groups were conducted over one session ranging from 60 to 120 minutes. Despite group diversity, all groups discussed a parenting component in relation to child diet. However, only four of the groups included a nutrition knowledge component (Adams et al., 2008; Horodynski et al., 2009; McGarvey et al., 2006; Sherry et al., 2004), with just three groups either recording or discussing child BMI and/or weight status (Baughcum et al., 1998; Bolling et al., 2009; Jain et al., 2001). A majority of the research reviewed here focused on low SES groups, one included middle SES groups (Sherry et al., 2004), one included all SES groups (Haerens et al., 2009) with one considering middle SES only (Bolling et al., 2009). Limitations and/or problematic areas of the research were discussed in seven of the nine studies (Baughcum et al., 1998; Crawford et al., 2004). However, all of the research appeared to be clearly conducted with appropriate questions and analysis, which further contributes to an existing body of research.
When evaluating perceived barriers, a common theme expressed among low and middle SES groups regarding the provision of healthy foods to children included the perceived/real barrier that this involved increased cost. Unhealthy food products were perceived as cheaper, tastier and/or more readily available (Baughcum et al., 1998; Haerens et al., 2009; Horodynski et al., 2009; Sherry et al., 2004). Many parents believed that healthy food was more expensive and less satiating, and therefore not considered value for money and more time-consuming to prepare, whereas the energy-dense options were often pre-prepared (Adams et al., 2008; Bolling et al., 2009; Crawford et al., 2004; Haerens et al., 2009; Horodynski et al., 2009; Sherry et al., 2004). Interestingly, this barrier was mentioned across all SES groups.
Another barrier to be identified was cultural differences in attitudes, perceptions and concerns regarding the promotion of a healthy child diet (Adams et al., 2008; Crawford et al., 2004; Horodynski et al., 2009; McGarvey et al., 2006; Sherry et al., 2004). Inconsistencies among parents of the different cultural and SES groups, such as variations in both the definitions and interpretations of ‘health’, highlight a need to promote culturally specific programmes with operationalised definitions. A further example is differing values and beliefs surrounding food, such as displayed in the AI communities who, despite having knowledge to the contrary, were influenced by the priority of day-to-day survival (Adams et al., 2008). Therefore, successful programmes would need to account for these differences and endeavour to understand cultural priorities as these differing values may contribute to excess weight (Adams et al., 2008; Crawford et al., 2004).
Common themes across different cultural and SES groups included the inability of many parents to correctly identify their child as overweight or obese. Many did not believe weight and/or overweight to be a concern in the preschool years with the common misconception that a heavier child was a healthier child and indicative of good parenting (Baughcum et al., 1998; Crawford et al., 2004; McGarvey et al., 2006; Sherry et al., 2004). There was also a tendency for parents to believe their child had a genetic predisposition to excess weight and/or that their child would outgrow the condition (Baughcum et al., 1998; Crawford et al., 2004; Jain et al., 2001; McGarvey et al., 2006; Sherry et al., 2004).
Some parents expressed concern that their child was a picky eater and/or would not eat enough, revealing that child food preferences often directed food availability in the home (Baughcum et al., 1998; Haerens et al., 2009; Horodynski et al., 2009). Many parents were under the misconception that denying their child a specific food request was the equivalent to starving the child (Baughcum et al., 1998; Jain et al., 2001) or could lead to malnutrition (Horodynski et al., 2009). Food was also used to shape behaviour in the form of reward, as a contingency or to placate the child (Baughcum et al., 1998; McGarvey et al., 2006; Sherry et al., 2004).
The importance of promoting positive behaviours and messages regarding healthy eating, rather than negative messages of weight loss or restriction, was discussed in two of the studies (Adams et al., 2008; Crawford et al., 2004). Lower SES Latino participants believed promoting positive messages and identifying positive eating behaviours would be more inclined to motivate change as opposed to focusing on negative behaviours and labelling child weight (Crawford et al., 2004). However, the lower SES AI participants displayed incongruence between intention and behaviour (Adams et al., 2008). Although this group appeared to have the knowledge regarding healthy food requirements for young children and understood the importance of promoting these behaviours, this was not considered the priority, and therefore not reflected in their child feeding practices.
A major theme to emerge from this review is the need to tailor interventions to specific groups in order to maximise opportunities that will motivate and facilitate long-term behaviour change. For instance, participants across this review had differing levels of education, were from different cultures and varied in SES grouping, displaying different needs, perceptions and priorities (Baughcum et al., 1998; Crawford et al., 2004). These antithetical reports support Birch et al.’s (2003) summary that
contrasting parental evaluations of childhood overweight among racial, ethnic, and income groups highlight the need for qualitative and quantitative research in these groups to address links between cultural beliefs and parental goals and beliefs regarding children’s eating and weight status and to determine how parenting practices influence or are influenced by children’s weight status.
Much of the qualitative work reviewed in this article has subsequently informed intervention development and design. The inclusion of understanding regarding community needs, cultural perspectives and the social and physical realities faced by parents when feeding children seems likely to improve the capacity of achieving behaviour change and/or preventative action (Adams et al., 2008; Haerens et al., 2009; McGarvey et al., 2006). Therefore, it is clear that despite conflicting opinion surrounding the importance and validity of qualitative research methods, many intervention studies appear to involve and value a level of qualitative analysis to help inform and/or evaluate ongoing research.
Although limited in number, all of the studies in this qualitative review discussed parenting styles, practices or behaviours in relation to child feeding. However, there appears to be little research that also includes general parental nutrition knowledge and an understanding of what constitutes a nutritious and healthy diet for children aged 2–5 years. For example, four of the projects discussed nutrition, noting a preference for their child to have ‘good’ versus ‘bad’ nutrition, but did not consider what this ‘good’ nutrition would be (Sherry et al., 2004). McGarvey et al. (2006) looked at what infants and children up to the age of 3 years should and do eat and they observed both parent/child behavioural responses with feeding children up to 5 years of age, but not what 3- to 5-year-old children should eat. Horodynski et al. (2009), on the contrary, only considered children up to the age of 36 months. Furthermore, none of the studies appeared to discuss child nutrition and diet in relation to parenting styles and/or practices with parents of these children. Therefore, qualitative studies would be well placed to further explore the quantitative and experimental findings previously identified between parenting styles and parental feeding practices (Blissett and Haycraft, 2008; Hubbs-Tait et al., 2008).
In addition, a majority of this research evaluated lower SES groups who were predominantly Hispanic/Latino and/or African American. However, childhood overweight is a concern irrespective of culture and/or SES grouping. There was also a major focus on discussions around weight loss or food restriction, which appeared to promote a negative feeling of denial or deprival. None of the researchers spoke with mothers of healthy weight children who displayed healthy nutritious diets with a view to understanding what facilitates healthy eating and how these parents behave and interact with their children in the home food environment. There also appears to be a lack of in-depth discussion about ways to overcome the expressed difficulty in encouraging positive attitudes towards healthy foods in children, particularly fruits and vegetables. This may be related to parental attitudes towards healthy foods and role modelling of healthy diets to their children. Therefore, barriers and facilitators of this could be further explored.
Finally, given that this systematic review of qualitative research included only nine studies, of which only four included the nutrition knowledge/information component, it is clear that this area of research has not reached saturation and is in need of further attention. It is evident that by addressing all the major themes to emerge from this review, future focus group research could be conducted to further discuss the following: (1) parent perceptions of effective feeding practices, (2) parental views on the influences of home food availability and accessibility, (3) parent perceptions of what constitutes healthy versus unhealthy child diet (including attitudes towards diet) and (4) facilitators and barriers to providing healthy foods to children. Valuable information could also be gained by comparing this information between groups of parents with children who display a healthy diet and groups of parents with children who do not. This information would be constructive to further inform future intervention design and delivery. Comparisons could also be made with actual child food intake to gain a more direct understanding of the interaction of knowledge and practice and how these factors could manifest in child diet. As stated by Bolling et al. (2009), ‘by soliciting parent perspectives, focus groups can help identify unforeseen obstacles to behaviour change and generate alternative methods of improving nutrition’ (p. 173). Although focus group research is not statistically representative, it is purposively and/or theoretically sampled, has theoretical generalisability and is information-rich. This information could then inform intervention development and programmes that are aimed at addressing these key areas, thereby promoting healthy child feeding practices before unhealthy eating habits have been formed.
Establishing a useful understanding of the contributing factors that can influence the development of child diet requires systematic inquiry. Although all of the studies reported here were focus group interviews which cannot be standardised, this review illustrates the capacity of qualitative research to deepen our understandings across social and ethnic groups, and of likely facilitators and barriers to parents’ capacity to promote healthy eating in children. However, the identification of only nine studies that meet the inclusion criteria highlights an obvious lack in this area of qualitative research. Therefore, future research is required to bridge this gap and aid in promotion of healthy eating behaviours in young children.
Footnotes
Appendix 1
Summary of qualitative studies
| Author | Sample details |
Set | CM | Research focus |
Design | $ | C-age | P-age | SES | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | #G | Min | PS | GNK | BMI | Diet | ||||||||
| Preschool/childcare settings | ||||||||||||||
| Haerens et al. (2009) | 155c, 189p | 20c, 36p | 120 | I | A | ✓ | ✓ | FG | NR | 2–4 years and 6–8 years | m = 36 | L, M, H | ||
| Horodynski et al. (2009) | 27 | 2 | 90 | EHS | A and SN | ✓ | ✓ | ✓ | SS FG | US$25 | 1–3 years | 19–50 years (m = 30) | L | |
| McGarvey et al. (2006) | 25 | 4 | NR | WIC | A | ✓ | ✓ | ✓ | FG | US$30 | NR | NR | L | |
| Crawford et al. (2004) | 43 | 8 | 120 | WIC | A | ✓ | ✓ | SS FG | US$25 or GC | 2–5 years | 18–54 years (m = 32) | L | ||
| Sherry et al., 2004 | 101 | 12 | 90 | WIC | A | ✓ | ✓ | ✓ | FG | US$35 | 2–5 years | 20–35 years | L, M | |
| Jain et al. (2001) | 18 | 3 | 60 | WIC | A | ✓ | ✓ | ✓ | FG | US$50 | 2–5 years | 17–38 years (m = 25) | L | |
| Community settings | ||||||||||||||
| Adams et al. (2008) | 42 | 3 sites | 60–90 | WP | A and SN | ✓ | ✓ | ✓ | FG PO | Food cash | 5–8 years | ¾’s u/30 years | L | |
| Paediatric practice | ||||||||||||||
| Bolling et al. (2009) | 23p, 21c | 4 | 90 | pp | AV | ✓ | ✓ | ✓ | FG | US$20 GC | 3.2–6 years (m = 4.6) | 28.6–45.1 years (m = 37.1) | M | |
| Mixed settings | ||||||||||||||
| Baughcum et al., 1998 | 14m, 15d | 4 | NR | WIC | AV | ✓ | ✓ | ✓ | FG | US$10 | 1–3 years | NR | L | |
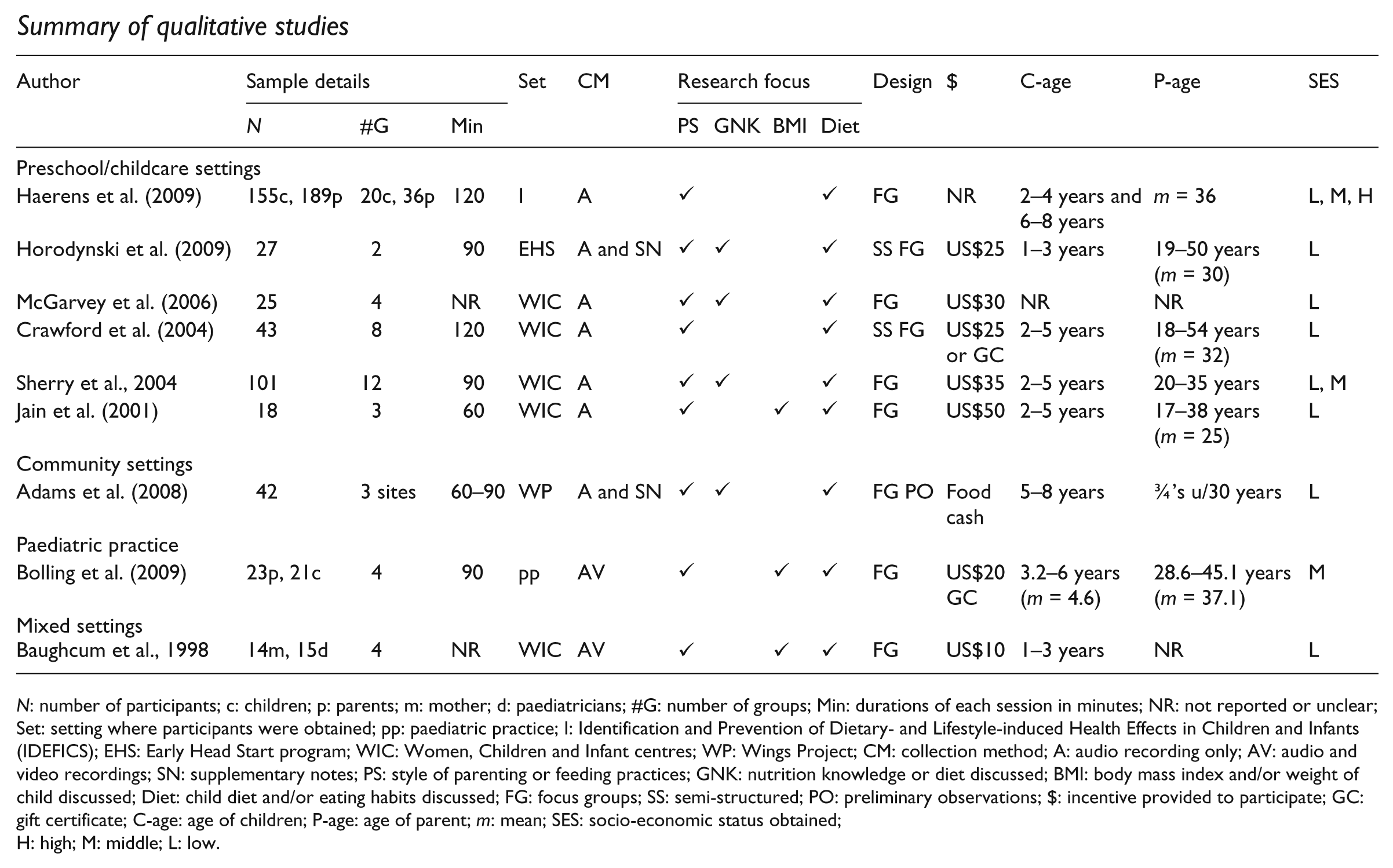
N: number of participants; c: children; p: parents; m: mother; d: paediatricians; #G: number of groups; Min: durations of each session in minutes; NR: not reported or unclear; Set: setting where participants were obtained; pp: paediatric practice; I: Identification and Prevention of Dietary- and Lifestyle-induced Health Effects in Children and Infants (IDEFICS); EHS: Early Head Start program; WIC: Women, Children and Infant centres; WP: Wings Project; CM: collection method; A: audio recording only; AV: audio and video recordings; SN: supplementary notes; PS: style of parenting or feeding practices; GNK: nutrition knowledge or diet discussed; BMI: body mass index and/or weight of child discussed; Diet: child diet and/or eating habits discussed; FG: focus groups; SS: semi-structured; PO: preliminary observations; $: incentive provided to participate; GC: gift certificate; C-age: age of children; P-age: age of parent; m: mean; SES: socio-economic status obtained;H: high; M: middle; L: low.
Acknowledgements
All authors initiated the review concept. The study data were extracted by J.P. and verified by N.P. J.P. prepared the article and all authors contributed to the editing of the article.
Funding
The first author (J.P.) was supported by a PhD scholarship from the University of South Australia N Parletta (formerly Sinn) is supported by NHMRC Program Grant funding (# 320860 and 631947).