
Abstract
Eco(logical)-cultural Theory suggests that a daily routine results from individuals adapting cultural ideas to the constraints of a local context or ecology. Using Ecocultural Theory, this research examined family child care providers’ descriptions of daily activities and overall approach to understand cultural models. The results highlighted a predominant cultural model reflecting ideas of “natural” child development facilitated by a structured daily routine. However, an alternative model emphasizing flexibility, intimacy, and relationships was also present. The results suggest that we need to better understand the conditions under which certain models become widely appropriated and enacted.
Keywords
Introduction—family child care a site for complex negotiations
Child rearing in any context is a complex project that involves balancing many competing interests. Caregivers have to make choices about what they will and will not do with limited time and resources. Such choices result from a combination of ideals about how life should be as constrained by the physical and material reality of a local ecology (Weisner, 2002). Caregivers within and across cultural communities often have very different models of what a “good life” can and should be (Hedegaard, 2009). Nonparental child care that takes place in a home setting—a practice I will refer to as family child care but that is also called by a variety of terms in different national contexts, including, family day care and childminding—represents an understudied site for such complex negotiations for at least two reasons. First, it is a site of the traditionally private domain of caring for children, but it involves, at least in some countries, the traditionally public domain of market transactions (Tuominen, 2003). Although regulations vary across international contexts, family child care is frequently perceived to be of lower status and regulated with fewer requirements for training and professional development than center-based care (Davis et al., 2012; Mooney and Statham, 2003). As a result, individuals working in family child care, called “providers” here, are likely drawing from a number of different models for how to organize their daily activity. Indeed, scholars from a range of perspectives have documented tensions that providers face (e.g. between education and care, and between institution and family) in a wide variety of cultural contexts (e.g. Albanese, 2007; Mooney and Statham, 2003; Tuominen, 2003; Zellman and Karoly, 2012). Approaches based in cognitive anthropology suggest that the cultural models humans draw from in organizing their behavior are complex and seldom easily classified (e.g. Gallimore et al., 1993; Gallimore and Lopez, 2002; Tout et al., 2009; Zaslow et al., 2012; Zaslow and Tout, 2010). This article explores what early childhood providers and researchers can gain from understanding family child care from the perspective of Ecocultural Theory (ECT; Gallimore et al., 1993; Gallimore and Lopez, 2002; Weisner, 1997, 2002) with its focus on how the complex, culturally organized ideals of care, or cultural models, held by adults can impact the kinds of activities that children experience in their daily lives. This article presents a heuristic, conceptual framework for researching cultural models along with initial results to demonstrate the utility of that framework.
ECT, cultural models, and family child care
By conceptualizing child rearing as a culturally organized project, cultural theories like ECT foreground the many different ways that caring for children can be accomplished and the many different consequences that can result from that variety (Weisner, 2002). As Rogoff (2003) suggested, there is no “one best way” for children to develop. Differences in how child care providers see their project matter for how they organize their days—projects as diverse as earning a living, preparing children for school, ensuring that children grow up healthy and safe, maintaining a profitable business or protecting children from the discrimination they believe the children will encounter upon entering school. In the published literature, variations across early childhood programs in general are often described in terms of “quality” (e.g. Dahlberg et al., 1999; Lugo-Gil et al., 2011; Owen, 2000), “curriculum” (e.g. Soler and Miller, 2003; Zellman and Karoly, 2012), or beliefs and ideologies (e.g. Dahlberg et al., 1999; Forry et al., 2013; Tuominen, 2003; Zaslow et al., 2009), but it is not clear how each of these relate to daily life in family child care settings. Some researchers focusing on family child care in particular have also examined providers’ ideas about professionalism (e.g. Bromer, 2001; Simpson, 2010) or professional development (Goouch and Powell, 2013). There has been extensive research on “ethnotheories” or the beliefs that adults, usually parental figures or teachers in primary school settings, use to guide their everyday decision-making (e.g. Harkness et al., 2007a, 2007b; Harkness and Super, 1983; Rogoff, 2003; Super and Harkness, 2002). However, very little research examines the diverse cultural models of care that child care providers draw upon as they organize their daily life and make decisions about how to allocate time and resources, particularly in family child care or among providers who are less connected to education, training, and discourses of early childhood.
ECT and sociocultural 1 theory (SCT) have many features in common (e.g. Cole, 1995; Rogoff, 2003). A number of scholars have explored the implications of SCT for early childhood care and education (ECE) practices and settings (Anning and Edwards, 1999; Edwards, 2003, 2007; Fleer, 2010; Fleer et al., 2004; Fleer and Hedegaard, 2010; Smith, 1996), but ECT has been less frequently used for ECE institutions (however, for an ECT analysis of children’s activity in child care, see Grace and Bowes, 2011). Both approaches suggest that children develop through participating in culturally organized activities of a particular local context. However, ECT focuses on how and why adults organize children’s daily routine activities.
According to ECT, daily activities are the visible result of a process of adaptation. Humans have “cultural” ideas, like ideals about how to organize daily life or how things should be, but those ideas are always formed and situated within the physical and material conditions of a particular local context, or ecology. As Weisner (2002) wrote, Activities crystallize culture directly in everyday experience, because they include values and goals, resources needed to make the activity happen, people in relationships, the tasks the activity is there to accomplish, emotions and motives of those engaged in the activity, and a script defining the appropriate, normative way to engage in that activity. (p. 275)
ECT provides a framework and method for talking with adults about the activities that are central to life in a particular ecology, thereby providing a window into both the “culture” and ecology.
In particular, ECT suggests that a particular child care setting includes at least three core components. Daily routine activity is considered the primary conduit for children’s development but must be understood as dialectically constructed within a particular setting, called an ecocultural niche, that has both cultural/ideological and physical/material properties (Gallimore et al., 1993; Gallimore and Lopez, 2002; Weisner, 1997, 2002, 2005). Thus, any effort to understand children’s development in family child care settings, from this view, must remain focused on what people do on a daily basis as understood in relation to what they think in the context of their particular physical and material working conditions. Furthermore, what they think has been conceptualized in ECT as a dynamic system of beliefs that is often unexamined and “messy” and can contain contradictory ideas. In ECT, by comparing particular individuals’ belief systems as articulated when describing specific activities, we can begin to identify patterns of shared belief systems or what will be called here “cultural models” that may reflect larger, more widely held cultural patterns. The core components of an ECT approach to family child care are represented in Figure 1.

An ecocultural approach to understanding daily activity in family child care through daily routines, belief systems, and physical/material conditions.
The research project
In the study reported here, I explored how child care providers viewed the project of caring for children, by focusing on the organization of everyday routines in family child care. The primary goal was to apply and demonstrate the utility of an ecocultural approach for this type of ecocultural niche by focusing on providers’ belief systems in relation to their daily activities. I was seeking preliminary answers to three broad questions. First, how do family child care providers describe their daily routine activities? I was interested in whether there were common daily activities across providers or, alternatively, whether there were patterned variations in the daily routines they described. In other words, is there a cultural form of daily activity in family child care recognizable across participants? Second, what kinds of cultural ideals do providers describe in their responses to questions about their approach overall (e.g. goals, description of own role in children’s lives)? Again, I was interested in whether there were common ideas between providers in descriptions of their approach and whether there were patterned variations in overall approach. These ideals can be considered part of the cultural models these providers hold. Third, how do the ways providers describe their daily activities relate to dominant cultural models (e.g. Dahlberg et al., 1999)? For example, did providers with more structured daily routines also draw upon ideas about children as “Natural” or “Scientific” or, by contrast, were those providers with more flexible daily routines more likely to describe their child care as a “substitute home”?
Surveys and postage-paid reply envelopes were mailed to licensed family child care providers in the first author’s local service area in a region of the Los Angeles area in Southern California. Participants were offered a US$15.00 gift card for returning their completed surveys. Procedures and measures were reviewed and approved by the Institutional Review Board of California State University, Northridge.
The survey included a combination of open- and closed-ended questions and all survey responses were typed for analysis. Of 22 respondents, 11 completed both sections of the open-ended portion of the survey (the Daily Routine and Approach/Philosophy items) and 4 completed just the section about their approach/philosophy. All respondents were female and most identified themselves as “owners” (n = 6) or “providers” (n = 5) with a few identifying themselves as “teachers” (n = 2), combinations of those terms, or other labels. Participants all offered full-time care, with 20 of the 22 also providing part-time care to some children, and 15 and 12 providing after- and before-school care to some children, respectively. Only a small number provided night, weekend, and sick-child care (three, seven, and six, respectively). Compared to the last study of family child care in the region (Burton, 2003), and the Bureau of Labor and Statistics (2014), the providers in this sample had more experience, more general formal education, and more training in early childhood than is commonly reported, and seemed to be less challenged and more rewarded by the work of child care.
Despite offering a gift card, only a small number of providers returned the surveys. Sending the survey in English limited the response rate, 2 and some of the notes and phone calls received suggest that many providers were struggling with the economic downturn (e.g. had given up providing care) in the United States sometimes called the “Great Recession” that began in 2009, which may have impacted the rate of response, and others returned blank surveys stating that they did not work with infants or toddlers. Most likely, the length of the survey (approximately 30–60 minutes) was the biggest factor limiting our response rate among English speakers. Although this sample was limited (i.e. self-selected, English speaking), these results can still demonstrate the utility of the approach.
I began by analyzing responses to open-ended questions about daily routines and philosophy/approach through open or initial coding, or by breaking transcripts up into meaningful units to sensitize myself to the meanings of the participants themselves. Once all transcripts had been read and open coded, codes were integrated into larger dimensions that could be applied across all cases, and which were created with levels: low, medium-low, medium-high, and high. The levels were created based on the range of responses within this study and were designed simply to capture variation. Four levels were selected so I had to articulate what made a provider “high” or “low” and then “more high” and “more low” and to avoid having a “medium” category that would be harder to articulate. Responses were read and ranked into the four levels to provide a basis for defining what differentiated the preliminary levels. Responses were then reread and adjusted, if necessary so that the definitions of levels represented the full range of diversity in responses. In the section that follows, I discuss each of these dimensions and the relationships between them.
Findings—daily routines
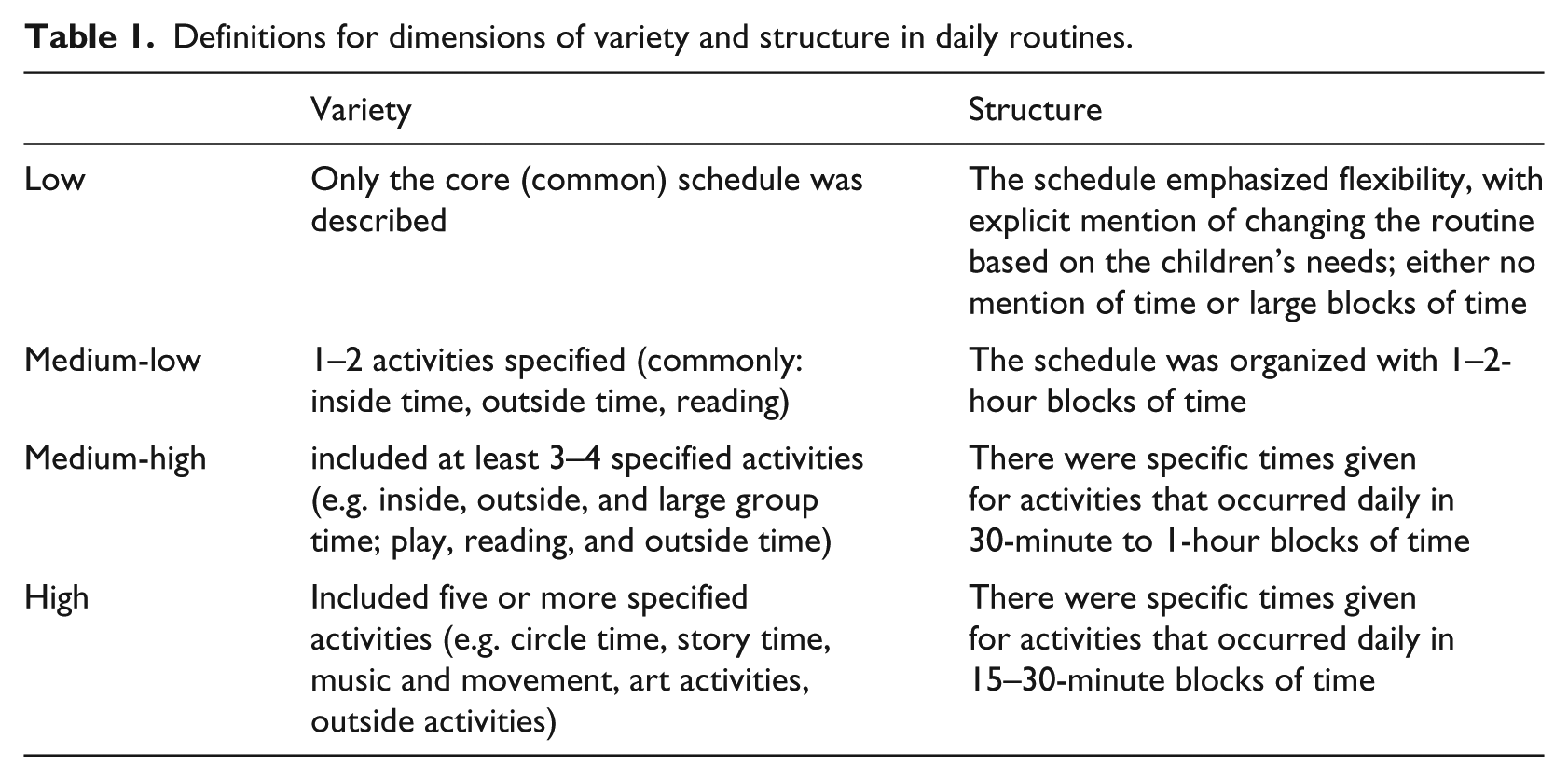
Because daily routines are central to ECT, I began by examining the providers’ descriptions of everyday activities. Overall, most providers described a general flow to the day that alternated between activities and routine care: a morning meal, an activity (e.g. outside play), a snack, another activity (e.g. inside play), lunch, nap, snack, and a final activity (e.g. outside play). However, providers varied in terms of how many different activities were described as regularly occurring, a dimension I called variety, and in terms of whether the general description emphasized flexibility and openness as opposed to structure and similarity from day to day, a dimension I called structure (e.g. one provider, Gita, wrote “For babies under 1, they have their own routine some nap twice, whereas some nap hardly at all. So I would say they are the boss of me.”). Defining features of these dimensions are summarized in Table 1.
Definitions for dimensions of variety and structure in daily routines.
All combinations of variety and structure are theoretically possible. Providers who were low in structure could be high in variety. For example, one provider described a very simple overall structure with just a core series of activities, but described a range of possible activities that varied from day to day. Following Strauss and Corbin (1998), I created a grid with variety and structure plotted to show the “placement” of each provider along the two dimensions (Figure 2). This revealed how each of the dimensions identified differences between providers. Most providers were in Quadrant IV: daily schedules that specifically listed a wide variety of activities at regularly scheduled times each day. Four providers were rated at the highest level for both variety (e.g. arts and crafts, story time, music/movement time inside and outside, music, and “academic” time) and structure. A fifth provider (Tina) was also placed in Quadrant IV, but had slightly less variety than the other providers in the quadrant. Three providers were placed in Quadrant III, each rated as medium-low for variety and medium-high for structure: these providers offered schedules that were quite similar from one day to the next but did not describe a wide range of activities. Two providers (Quadrant II) described a relatively low degree of structure (i.e. relatively large blocks of time set aside for activities), but included phrases in their description of their daily routine to suggest that they varied the activities that were offered during those blocks of time. One provider was in the quadrant representing low variety and structure (Quadrant I). This provider did have some activities that were relatively short (i.e. 15–30 minutes) and scheduled for regular times each day, but they were either routine care (i.e. snacks/meals) or reading time.
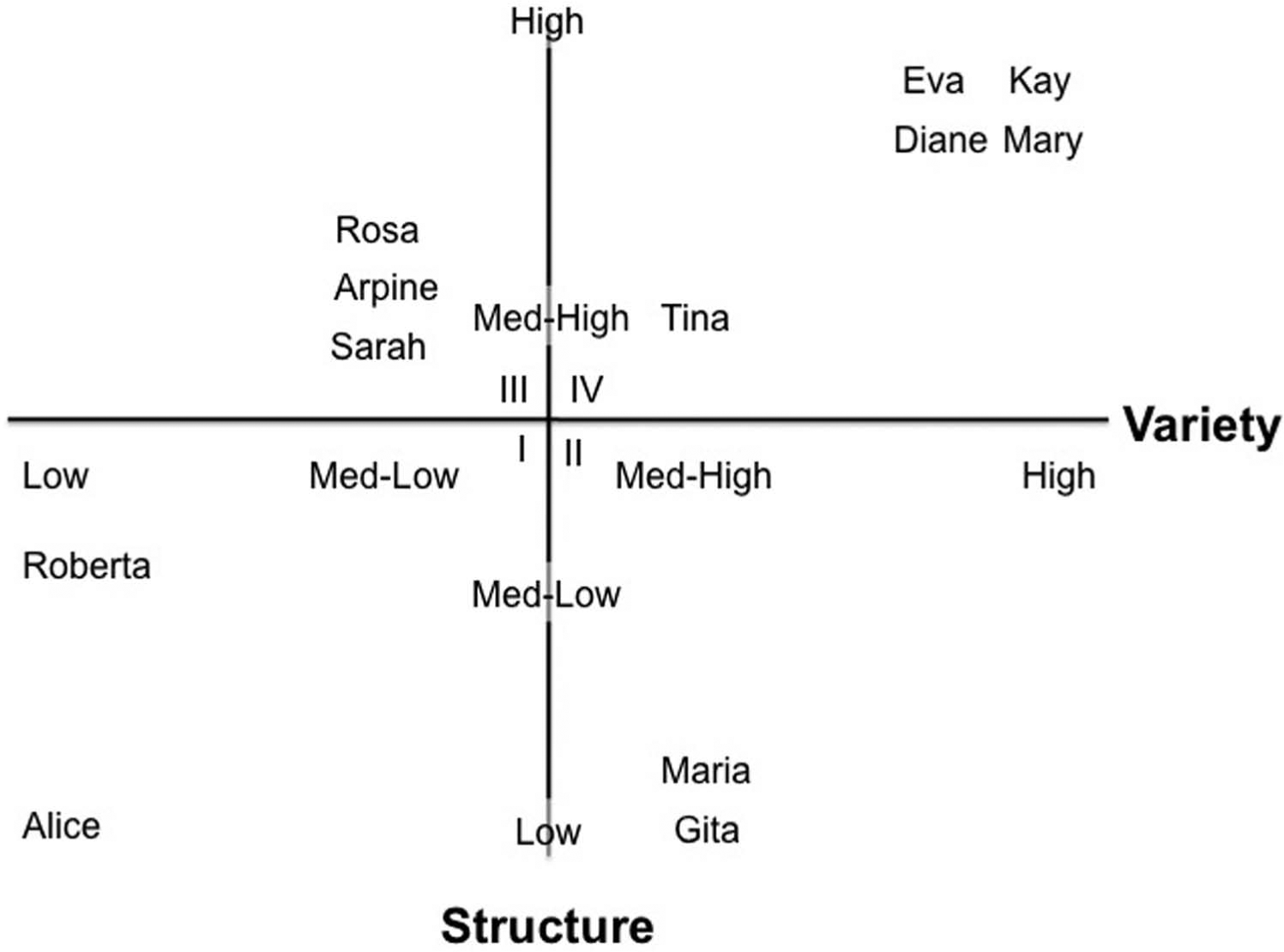
Axial grid of the variety and structure in child care providers’ daily routines. The Roman numerals represent the quadrant. I is low variety/low structure, II is high variety/low structure, III is high structure/low variety, and IV is high variety and high structure.
Thus, guided by ECT, this research identified both a common cultural form and two dimensions along with daily routines varied across providers. All providers had a common core of activities in their daily routine: from arrival, breakfast, activity, snack, activity, lunch, nap, activity, to departure. However, they could all also be described by variations in the variety of activities offered and the structure or extent to which the daily routine included blocks of time scheduled for specific activities that were the same from day to day.
Findings—cultural models
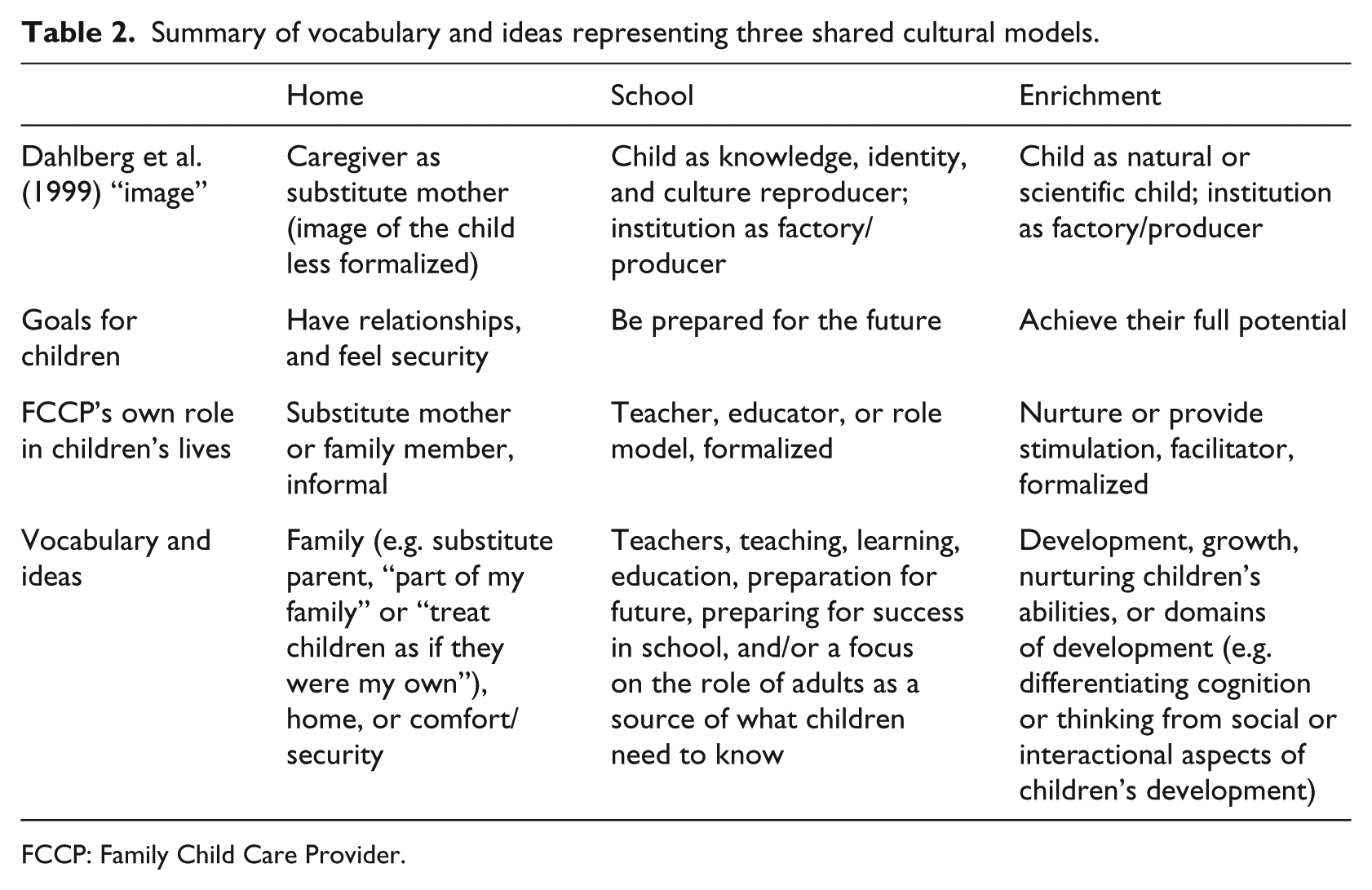
In order to examine providers’ cultural models or ideas about their work, I next examined their descriptions of their approach to their work. I identified three main dimensions, which I labeled school, enrichment, and home (Table 2). Two of these reflect more bureaucratic (Bromer 2001) models of care, in which providers described more formalized practices and roles (as opposed to multifaceted, individualized relationships). The two more bureaucratic approaches (school and enrichment) differed in the ideas or images about children and education reflected (Dahlberg et al., 1999). The most common, enrichment, reflected an image of the Natural or Scientific Child with an emphasis on domains of development and the adult as facilitator of the natural course of development. The school dimension, by contrast, reflected a future/preparation-oriented image of the child as Knowledge, Identity, and Culture Reproducer with the adult as the active guide or provider of what is to be reproduced. A third dimension, home, emphasized flexibility, intimacy, and relationships in a way similar to child care as a substitute home and contrasted with a bureaucratic model of care (Dahlberg et al., 1999).
Summary of vocabulary and ideas representing three shared cultural models.
FCCP: Family Child Care Provider.
Because these dimensions were not considered to be mutually exclusive, each provider was rated for each dimension (as low, medium-low, medium-high, or high) based on responses to questions about “overall approach to or beliefs about early child care,” the providers’ own role in children’s lives, the role of other children, adult–child relationships, aspirations for type of care they would like to provide, professional story, and long-term goals/plans. As expected, providers differed in their emphasis on the different shared cultural models. The most common (n = 6) profile was called enrichment, based on classification as high on enrichment and low or medium-low for school and home. The second most common (n = 4) profile was called home based on classification as high for home and low or medium-low for school and enrichment. Two other cultural models reflected mixtures of ideas. Bureaucratic was a name given for three providers scored as medium-high for both school and enrichment dimensions and low or medium-low for home because school and enrichment both reflect more formalized, structured, less individualized care than is central to the home dimension. The final group, called undifferentiated, included three providers who were not well described by these dimensions: two (Audre, Arpine) were considered medium-low for all of the three rated orientations, and one (Roberta) was considered medium-high for enrichment and medium-low for each of the others.
Cultural models—an enrichment profile
The responses of one provider, Tina, exemplify the enrichment profile that was common among these providers in which children learn through natural processes that are often described in terms of domains of development: I want kids to HAVE FUN! And learn to be nice to each other, take turns, sharing, helping their friends up if they fall etc. ABC’s, 123’s are important to (sic), but I believe playing should be the priority and finding a way to make learning fun … I want them to be happy and able to express themselves freely.
Tina’s description of dispositions and skills (“be nice to each other, take turns, sharing”), her juxtaposition of play and learning, and her reference to letting children “express themselves” freely all reflect an image of a child as having potential inside rather than a blank slate. Furthermore, Tina’s reasons for becoming a provider also reflect a common pathway reported for women, perhaps particularly White/European-heritage women who become providers (Armenia, 2008; Tuominen, 2003): I used to do accounting. But I wanted something different, so I took the classes at [institution]. Shortly thereafter, I became pregnant and I refused to put my baby in day care—so I quit my job and started my own day care. The training sure came in handy!
Cultural models—a home profile
Another provider exemplifies a home profile. Maria, a Latina with a 2-year degree and training in ECE (completed in Costa Rica), was licensed for a home-based service for no more than seven children. When asked about her approach, she wrote, Children should be able to have a quality day care and made to feel like this is a second home for them. I try to be a “secondary” parent to them and feel love and care from my day care … [own role] I want them to see that I care for them and here to make them to feel safe and loved while in my care. I discipline with love.
Two other providers’ articulations of a home model illustrate both the central aspects of a home model and variations in how they appropriated the shared ideas central to this dimension. A home cultural model was defined as emphasizing security, intimacy, and continuity in relationships as the “products” of early childhood institutions and potentially as attempting to imitate a particular construction of motherhood as that of a mother with devoted attention to a small number of children. Diane was an “owner” who articulated the core ideas of security and home as an ideal place for early childhood development: I believe that a child should spend their Early Childhood years in a home environment. It has been my experience with children, that a child, by the time they reach school age, is tired of spending all day in a four wall classroom. I believe that a home environment, is an advantage to the child … As a provider, I see myself as a person, a child can trust, feel safe, loved, and comfortable with. Every day is a teachable experience, children learn from our daily routines and being a role model.
However, Diane, a former teacher, describes home in opposition to the “four wall classroom” organization and, by implication, schools. By contrast, another provider, Gita, who became a provider after immigrating to the United States with small children and who had a bachelor’s degree in her home country of Kenya, but no formal training in early childhood, describes similar core components from a different perspective: I really don’t know what to write, but all I have to say is that if children have to be at a daycare is not such a bad idea, they do good in attention (sic). Children grow up together in a small group, they make friends and look forward to playing together … I do play important role. Some children are with me for 8–9 hours. I do get attached to them and they do get attached to me. I can’t replace a mother, but I can give them affection, bit of discipline, and routine in their lives.
Gita’s description seems to be in response to views of day care as possibly harmful for children (“have to be at daycare is not such a bad idea”). Although both providers’ responses emphasize intimacy and relationships, the core components of a home profile, Diane contrasts her role and program with an institutional setting whereas Gita contrasts her role with a mother she can only approximate and cannot replace.
Cultural models—a school or bureaucratic profile
One provider was higher than all others on the school dimension. Mary was a Latina with an associate’s (2-year) degree in child development who became a provider to be at home with her daughter. Although she was very articulate at describing the scripts involved in her daily routines, her responses to questions about her overall approach were relatively short and she was rated high on the school dimension because each of her responses to the section on approach included some reference to teaching, learning, or school: [Approach] Provider and parent work together for best experience for child. Childcare/
The most pervasive vocabulary in her responses relates to school and education. Nonetheless, when responding to the closed-ended questions about the reasons her work is important, she wrote in the space for comments, “[t]o provide a place for a child to express themselves (sic) (artistically, creatively)” which refers to children’s “natural” capabilities central to enrichment. Thus, her responses reflect a mixture of ideas in which adults provide structure and models for development characteristic of a Bureaucratic profile.
Thus, as predicted from ECT, some shared cultural models could be identified from the individual belief systems noted in these providers’ descriptions of their work. In particular, cultural models of enrichment, home, and school were noted in many providers’ responses. However, individuals’ belief systems often included a mix of these ideas.
Associations between daily schedule (structure) and cultural model
ECT suggests that daily routines will be related to individuals’ belief systems, and so I examined associations between the two sets of codes described above. Because of the important role of the environments adults provide for children in both enrichment and school dimensions, providers with high scores on these dimensions were expected to have a more highly structured daily routine and offer a wider variety of activities on a daily basis than providers who fit a home profile. This expectation was only partially upheld (Table 3). Of the five providers classified as having an enrichment profile, all four who provided a daily schedule were high on structure, but not all were high in variety.
Orientation ratings and classification as related to placement on the axial grid of variety and structure in daily routines.
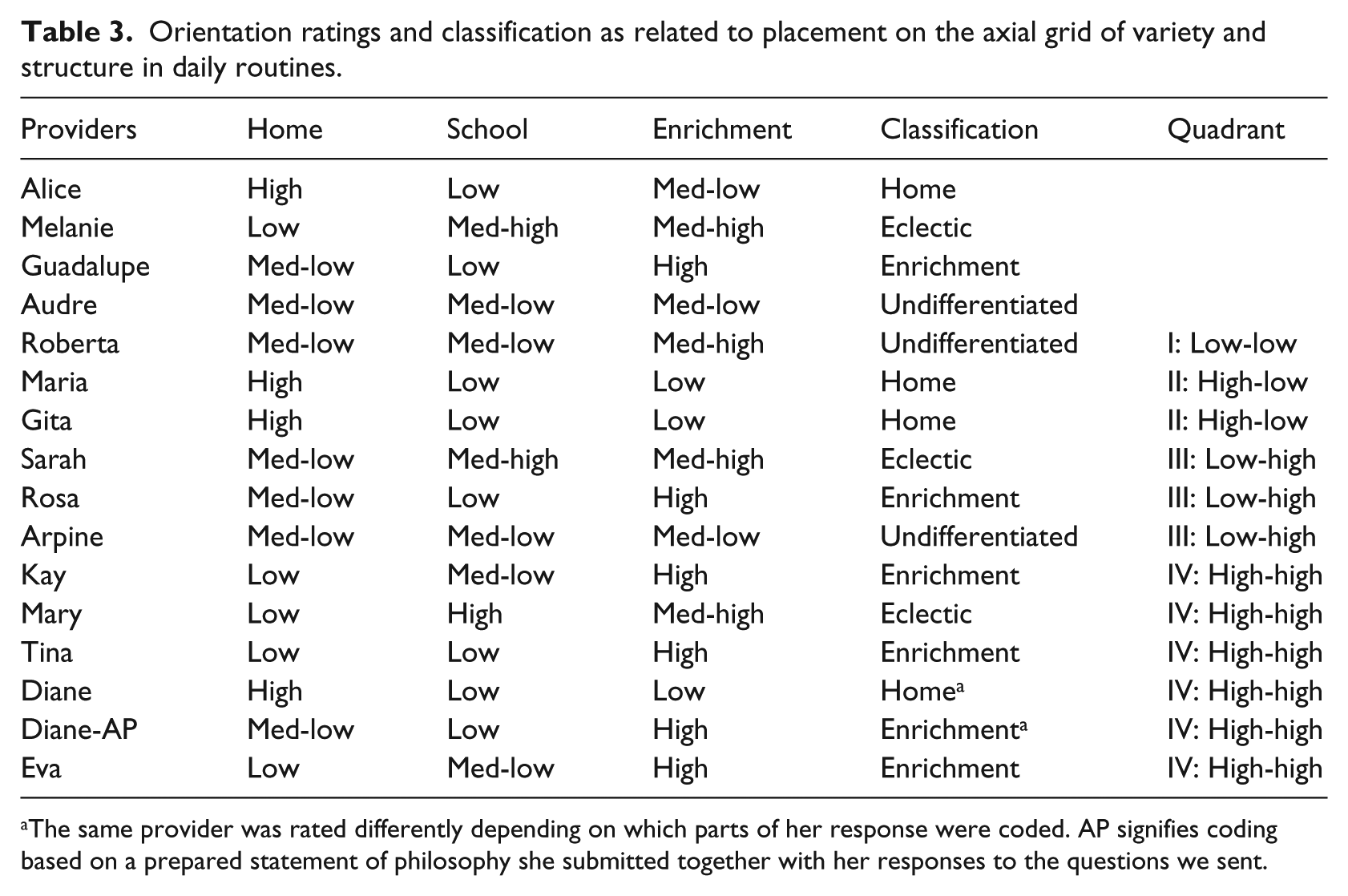
The same provider was rated differently depending on which parts of her response were coded. AP signifies coding based on a prepared statement of philosophy she submitted together with her responses to the questions we sent.
Providers who fit a home profile were expected to have less structured daily routines. This expectation was upheld, but with a limited number of cases. Of the three providers who were classified as having predominantly a home model, two provided their daily schedules and were grouped into Quadrant II (med-high variety, low structure). A third (Alice) did not provide an overall schedule, but in response to the questions about how she organized arrival/departure, snacks/meals, and naps, she listed only the times for those routine activities. Based on the limited information she provided, it is not clear whether she only scheduled routine activities or what she did in between those routine care activities.
Five providers were rated “low” for home (Kay, Mary, Melanie, Tina, and Eva), and all but one were considered to have highly structured daily schedules. Of these, three were classed as enrichment (Kay, Tina, and Eva) and two as Bureaucratic (Mary and Melanie).
One provider, Diane, mentioned above for her description of a home profile in opposition to a “four walls classroom,” was hard to classify. Diane was one of only two respondents who also mailed us a prepared Philosophy Statement, as they were all invited to do, together with her survey and that, when coded by itself, resulted in an enrichment classification. For example, her Philosophy states, [program name] provides a stimulating environment designed to promote social, cognitive, and physical development … a variety of learning experiences that encourage a positive self-image, self-esteem, and respect for the rights of others … [in] an environment that is clean, fun, and creative.
Thus, she is using the language of enrichment, and claiming that a “home environment is an advantage to the child” while emphasizing her role as someone a child feel secure around, but still organizing her activities in a highly structured way. Furthermore, when asked about her aspirations, she wrote, “I enjoy what I am doing, and I am in the process of returning to school and get my degree in teaching.” Her prepared philosophy includes specific mention of domains of development. Her daily routine looks more like those of the enrichment-oriented providers.
Thus, as expected based on ECT, providers’ descriptions of their daily routines were associated with the cultural models noted in their descriptions of their work. However, the patterns of association among cultural models and daily routines were messy. A holistic approach that could examine idiosyncrasies was necessary, partly because providers’ responses did not always fit neatly into anticipated analytic categories (e.g. Diane).
Conclusion
The primary purpose of this article was to articulate and illustrate an ecocultural approach to understanding everyday activity as organized by cultural models and to demonstrate the utility of that approach with some initial data. These results show that even a limited sample and a simple survey including open-ended questions provided a foundation for articulating three cultural models related to providers’ descriptions of their daily routine activity. Thus, these results provide a suggestive “proof of concept” that asking providers to describe their daily activities provides insight into their cultural models as well as their daily routines. The models reflected in their responses show both shared (e.g. ideas about child development and how to organize daily activity) and idiosyncratic components, as predicted by ECT (Gallimore and Lopez, 2002), with many individuals’ responses reflecting mixed themes in their cultural models (See also, Tonyan and the AERA paper, Tonyan et al 2013.). Overall, the results point to the usefulness of conceptualizing family child care as an ecocultural niche: providers’ cultural models varied and were related to descriptions of daily routines.
This study’s first research question addressed the organization of daily routines in family child care. ECT suggests that understanding daily routine activity is central to understanding human development. All providers’ descriptions shared a common core, alternating between routine care and other activities. Thus, it may be possible to identify common features of daily routines in family child care settings. However, providers differed in the variety of activities and degree of structure in the daily routine, indicating that measuring that variability and the conditions that predict that variability may prove fruitful for future research. Some providers’ descriptions emphasized variety from one day to the next whereas others emphasized similarity from day to day with a variety of activities offered each day. This framework and these initial results pose important questions for early childhood research. First, to what extent are these specific dimensions common or context-specific? Although some influential studies have taken a comparative approach to examining similarities and differences in daily routines within and across cultural contexts (Tobin et al., 1989, 2011), little (if any) research has done so for home-based or family child care settings. Most research continues to focus on the component activities of daily routines (i.e. literacy activities and play; for example, Fleer et al., 2008) or moments of time (Kryzer et al., 2007) rather than the structure of the whole day. Second, what are the conditions that impact whether and how providers organize daily routines as they do? Our ongoing interviews with these providers suggest that many struggle with the limitations of space in their homes to store the many materials that their training leads them to believe that they need. For example, they frequently describe struggling to store materials they can rotate to provide a variety of activities across days and to arrange multipurpose spaces to provide a variety of activities within a particular day. Such struggles may be specific to the United States where common interpretations of Developmentally Appropriate Practice (Copple and Bredekamp, 2009) suggest that many specialized materials are needed to provide “quality” care (Harms et al., 2007). Without more research using common methods and points of reference, it will be difficult to theorize when and how such conditions impact daily routines.
The second question of this study examined individual belief systems and shared cultural models theorized as important from an ECT perspective. Among these providers, three cultural models of enrichment, home, and school captured some commonly held cultural ideals, but profiles of individual providers suggested that individuals varied widely in how they constructed their own meaning. Enrichment reflected the extent to which providers appropriated ideas similar to Dahlberg et al.’s (1999) image of a Natural or Scientific Child and was the most commonly appropriated of the dimensions articulated here. However, a home model emphasizing continuity in relationships, security, and intimacy was also commonly expressed by these providers. Among these providers, the vocabulary and ideas of school and education were often used, but seldom separately from enrichment. Although certain discourses about early childhood seem to have relatively widespread impact on a global level (Dahlberg et al., 1999; Fleer, Tudge, and Hedegaard, 2009), they are still resisted and individually negotiated (Blaise, 2005), and much more research about the discourses relevant in a variety of local contexts is needed. Talking with providers about their everyday activity and daily routines represents an important methodological “tool” for accessing cultural models.
Finally, as expected based on ECT, addressing the third question of this article suggested that the organization of daily routines was related in patterned ways to individuals’ cultural models. Providers who described highly varied and structured daily schedules tended to emphasize enrichment, whereas providers who described flexibility in their daily routines (e.g. “the babies are the boss of me”) tended to emphasize a home model. The variability found in even this pilot work suggests that a methodological approach based on ECT is warranted: conversations about daily routine activities provide a useful window for understanding the cultural organization of family child care. Responses to these surveys and preliminary interviews based on this work suggest that providers love to describe their daily activities and such descriptions provide a window into their cultural ideals. This may provide an important methodological move forward from the inconsistent and conflicting results that have been found by examining only providers’ responses to paper and pencil surveys of their beliefs (e.g. Huijbregts et al., 2008; Tonyan et al., 2013) because beliefs are abstract, often implicit, and difficult to describe.
A number of limitations impact the conclusions to be drawn from this research, because this research could only partially test an ECT approach. First, providers were only surveyed at one point in time and their activity was not directly observed. Thus, this research cannot disentangle the direction of causal effects nor triangulate the providers’ perceptions with any external understanding of their reality. Second, an open-ended survey such as this can only capture that which the respondent can explain and make explicit and not tacit or implicit knowledge. Nonetheless, the most powerful cultural models may well be taken for granted (Rogoff et al., 2007). As such, participants would never think to write them on a form. For example, it seems likely that some providers may be serving young children well even though they may not be able to articulate what it is that they do or how they do it. Some research suggests that variations in levels of training and involvement in the field of early childhood may also relate to providers’ ease in talking about their practices (Fleer et al., 2008). By contrast, a skillful interviewer can surface taken-for-granted ways of thinking and acting (e.g. “do you know any providers who do that differently?” followed by “how do you think children in those programs would be different?” or “have you always done it that way?” followed by “how were things different before?”). Despite the limitations of this research, providers’ idiosyncratic belief systems could be understood to also reflect shared cultural models. One question arises: Why have some early childhood discourses been widely taken up by these providers (e.g. enrichment) whereas others are not used as much (e.g. family and close relationships)? If we in the field of early childhood research are to consider cultural models as actively constructed and as drawn from ideas shared during the course of activities of communities, we will require open-ended, qualitative, or ethnographic style research that examines associations between ideas and action in the context of local meaning. “Local” can sometimes be an individual, as in the pilot survey presented here, but will also, ultimately, need to include patterns among individuals and across different communities of providers to understand which cultural models providers appropriate and under what conditions. Conversations about how and why daily activity is organized in particular ways can be fruitful for professional development efforts precisely because such descriptions offer windows into meaning and cultural models as well as concrete examples of practices that can be a focus for change. Such an approach has already proved useful for impacting early interventions for families of children with special needs (Bernheimer and Weisner, 2007; Weisner et al., 2005), medical practice (Hay et al., 2008), and more (Daley and Weisner, 2003; Goldenberg et al., 2005; Huston et al., 2003, 2005; Lieber et al., 2005). Indeed, the method used here, of a simple, open-ended survey asking providers about their daily schedule as well as their approach, could be a useful exercise for starting such conversations.
Future research will need to examine whether the cultural models and profiles found here are relevant to other local contexts and how actual practices relate to providers’ descriptions of their daily routines. Under what conditions are practices aligned with cultural models? What professional development activities help providers articulate (i.e. externalize) and critically examine their beliefs, practices, and the associations between them in ways that can support more reflective practice? ECT suggests that asking providers discuss their daily life provides a rich method for documenting beliefs, activities, and the associations between them. Members of my research team and I are currently conducting pilot interviews based on the Ecocultural Family Interview created for use with families (The Ecocultural Scale Project, 1997; Weisner, 2011; Weisner et al., 2005). We find that quite a number of providers are hesitant to talk about their approach to care, but provide rich descriptions of a typical day, particularly when describing photographs of their daily activities. Scholars from multiple perspectives have called for more research that can identify patterns and variations in the conditions of specific local contexts that can help to understand both local and global more effectively rather than trying to identify universal or context-free results (Fleer, Tonyan, et al., 2009; Kemmis and McTaggart, 2005). For example, Rogoff (2003) calls for identifying “regularities” in the kinds of conditions that are associated with patterns of childrearing and human development. Similarly, James et al. (1998) called for scholars to study childhood at the local level and then identify links and trends among localities. If scholars across a range of local settings use compatible methods—like talking with providers about daily activity as a window into cultural ideals—and anchoring concepts—like the core components of ECT, including activity, ecology, scripts, and cultural models—early childhood researchers can begin to better understand the complexities of how child care providers as active agents appropriate and enact diverse and pluralistic cultural models in their work with children.
Thus, this research provides initial evidence to support an ECT-based approach to family child care as illustrated in Figure 1. In particular, this article illustrated an approach based on asking providers to report on their daily activity and documented a number of cultural models relevant for family child care providers. Measuring and examining the associations among two of the three components identified as essential in ECT—daily routines and belief systems—provided insight into both individual variation and common potential cultural forms (i.e. shared across particular ecocultural niches). Further research is needed to examine the variety of belief systems and cultural models that are likely relevant to ECE in many different local contexts with varying physical and material conditions. Nonetheless, these findings suggest that this framework, in general, and the specific approach of asking providers to describe their daily routines represent a promising means to document the cultural organization of family child care.
Footnotes
Acknowledgements
This research would not have been possible without the participation of the family child care providers who participated or the students who volunteered to assist in conducting the research. Special thanks to Joce Nuttall for her assistance in preparing this manuscript. Thanks to Thomas Weisner for his guidance in moving this research forward, making sense of its findings, and preparing the manuscript for publication. Thanks to Carrie Saetermoe and Jennifer Romack for their thoughtful feedback.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute On Minority Health And Health Disparities of the National Institutes of Health under Award Number P20MD003938. Support was also provided by the Department of Psychology, Dean Theodoulou (College of Social and Behavioral Sciences), and Provost Harold Hellenbrand at California State University, Northridge.