
Abstract
South Africa currently lacks HIV counselling interventions that are youth-specific and that meet the psychosocial needs of young people living with HIV/AIDS. Indigenous strategies and interventions need to be developed that cater for the psychosocial needs of South African youth living with HIV/AIDS. By using Participatory Action Research (PAR) a Cognitive-behavioural-based Counselling Intervention Programme (CBCIP) was developed for use in a rural South African town. This article discusses the participatory action process involved in the development of the CBCIP. It shows how PAR theory relates to practice by highlighting the benefits, challenges and caveats in applying PAR within a rural setting. The lessons that were learned in the development of the CBCIP may provide future researchers with useful insight and foresight in the development of HIV counselling interventions for young people living with HIV/AIDS in South Africa.
Keywords
Introduction
There are numerous young people living with HIV/AIDS in South Africa who have increased levels of psychological distress (Batohi, 2004; MacPhail, Pettifor, & Coates, 2008). However, there is a currently a shortage of indigenous interventions aimed at meeting their psychosocial needs. Specifically, there is a lack of HIV counselling interventions that are youth-specific and that alleviate the psychosocial distress associated with living with HIV/AIDS.
Several evidenced-based models that focus on young people living with HIV/AIDS from a care/treatment perspective, have been developed in America (Bettencourt, Hodgins, Huba, & Pickett, 1998; Hymen & Greenberg, 1998; Remafedi, 1998; Schneir, Kipke, Melchior, & Huba, 1998; Sturdevant, Kohler, Williams, & Johnson, 1998; Tenner, Trevithick, Wagner, & Burch, 1998; Woods et al., 1998; Wright, Gonzalez, Werner, Laughner, & Wallace, 1998). Although these models have been shown to be effective in meeting the psychosocial needs of adolescents and youth living with HIV/AIDS in America they may not be applicable to young people living with HIV/AIDS in South Africa. This is because the traditions, beliefs and practices that contribute to the experience of health and illness may be different in South Africa and within the African culture from that of the American culture (Swartz, 2002). Western models and interventions therefore should not be imported to the South African context without taking into consideration the local realities and cultural aspects of the target group (Nsamenang & Dawes, 1998). This is why the need for indigenous interventions is crucial within the South African context. Indigenous interventions, therefore, need to be developed that cater for the psychosocial needs of South African youth living with HIV/AIDS.
One method to tap into indigenous knowledge is by means of Participatory Action Research (PAR) as it actively involves participants in the research process by drawing on their knowledge and experiences to bring about change and improvement (Rogers & Palmer-Erbs, 1994). According to Fals Borda (1998) one of the premises of PAR is the recognition of the people's beliefs and wishes as important contributors to community transformation. This type of research ‘allows aid and community development initiatives to be generated in a manner that respects local communities and their value systems’ (Cohen, 1991, as cited in Nsamenang & Dawes, 1998, p. 83). Contrary to the asymmetrical Subject/Object or empowered/disempowered relationship adopted by traditional research, PAR is an approach that employs horizontal participation or symmetrical reciprocity between the researcher and participants. In other words, both parties learn from each other through a dialogical relationship and in so doing the division between subject and object becomes significantly reduced (Fals Borba, 1998). According to Freire (1993) dialogue must serve the needs of each individual and not of one individual dominating another. PAR recognizes the value of dialogue and encourages true dialogue. True dialogue exists when critical thinking emerges and when people begin to look at their social reality critically and are subsequently able to immerse themselves in transformation and action (Freire, 1993). Interventions that are based on research methods such as PAR that recognize the need for true dialogue in intervention development, are not imposed but have instead been negotiated dialogically between the researcher and the community (Nsamenang & Dawes, 1998).
The need for PAR within the South African context is based on the uniqueness of South African youth especially with regard to cultural beliefs and practices and the implications for mental health thereof. For instance, the emotional expression of distress is not universal but rather varies from culture to culture. Research has shown that many South Africans are inclined to think of illness as caused by witchcraft (Kalichman & Simbayi, 2004; Shisana & Simbayi, 2002), spirits and supernatural forces (Kalichman & Simbayi, 2004). According to Van Dyk (2005), people believe in witchcraft because it helps them attribute meaning to the illness which science fails to provide. This is because Western medicine does not understand the diversity of emotional experience and the cultural beliefs that go with it (Swartz, 2002). The benefit of using PAR within local contexts is that PAR combines everyday knowledge with scientific knowledge to produce a new type of knowledge that is both social and scientific and has strong application potential (Montero, 2000). PAR has been used successfully for health interventions with youth (Boutilier, Mason, & Rootman, 1997; Cheatam & Shen, 2003; Flicker et al., 2008). Similarly, research conducted in South Africa has also found the use of PAR to be successful for health interventions with children (Govender & Reddy, 2010; Hrenko, 2005) and for health interventions with youth (Wallace-DiGarbo, 2006).
In an attempt to meet the psychosocial needs of young people living with HIV/AIDS in a rural South African town, the Cognitive-behavioural-based Counselling Intervention Programme (CBCIP) was developed in 2003 (L’Etang, 2011). The CBCIP followed a PAR design in which participants (including service providers, community members and young people living with HIV/AIDS themselves) played an extensive role in the developmental process. In so doing, the CBCIP was developed by tapping into the indigenous knowledge of young people living with HIV/AIDS in a rural South African town.
The purpose of this article is to critically reflect on the participatory action process that led to the development of a CBCIP for young people living with HIV/AIDS. This article uses the process of the CBCIP as a case study and describes how PAR worked in practice in a rural setting by detailing the benefits, challenges and caveats. It is hoped that this would provide future researchers with useful insight and foresight into the development of indigenous interventions designed for African young people living with HIV/AIDS using PAR methods.
Synopsis of participatory action research
The origins of PAR stem from the ideas and social movements of many (Montero, 2000). Among them is the influential work of Paulo Freire (1970) who included the participation of people who were usually voiceless and anonymous in the research process (Montero, 2000). Through the process of participation, dialogue and the expression of opinions individuals become aware of their personal abilities to bring about change and improvement in their own lives which contributes to their empowerment at the individual level (Bhana, 2006).
The PAR approach is characterized by six major criteria: (i) it is participatory, (ii) it is cooperative, (iii) it is a co-learning process, (iv) it involves systems development and local capacity building, (v) it is an empowering process for participants, and (vi) it achieves a balance between research and action. (Israel, Schultz, Parker, & Becker, 1998, as cited in Morisky, Ang, Coly, & Tiglao, 2004, p. 70)
Research following a PAR approach can therefore have many different variations of the approach. PAR has emerged as a popular methodology by offering an advantage over traditional research as it aims to empower people to confront the dominant power-holding and control elements of society by constructing and using their own knowledge (Huizer, 1989). It allows for the voices of ordinary people to be heard which creates opportunities for new ideas to be generated (Mertens, 2005).
In South Africa, PAR has been utilized successfully within the HIV/AIDS context (Campbell & MacPhail, 2002; Mantell et al., 2006). For example, The Mpondombili Project (Mantell et al., 2006) aimed to promote risk reduction (the use of condoms) and risk avoidance (delay of the commencement of sexual activity) amongst rural school-going youth. The development of the project employed a participatory process in which youth were trained through an interactive process as peer educators. The purpose of the peer educators was to make the programme more youth friendly, to empower the youth as well as build self-confidence and instil in them leadership skills. The draft programme which was developed by project staff was presented to the peer educators for their critique. The peer educators played the role of auditors which gave insight into the needs of youth themselves. In this way, the main intervention issues became apparent.
Although there is evidence to suggest the value of using PAR within the South African context, it must be noted that there are both advantages and disadvantages to this method. Many of the advantages of PAR lie in the criticisms of traditional research relative to its assumptions and practice. For example, one of the major advantages of PAR is that the researcher is allowed to develop an egalitarian relationship with participants in which open communication is valued thereby creating an environment in which an ‘in-touch’ perspective can be gained (Uzzell, 1995). PAR is also one of the few methods in which an attempt is made to combine academic and grassroots knowledge (Bryceson, Manicom, & Kassam, 1982). The opportunity for participants to choose the research issues and areas of focus for the research gives power to participants and breaks down the distinctions between the researcher and the participants.
One of the criticisms of PAR is that PAR lacks methodological rigor and technical validity (Tewey, 1997, as cited in Balcazar, Keys, Kaplan, & Suarez-Balcazar, 2006). Another criticism of the method is that there is no clear indication of what constitutes ‘participation’ or ‘active involvement’ of participants. Montero (2000) points out that what is needed on the part of the researcher is an appreciation or understanding of the varying levels of interest and involvement of participants in the research based on their own needs, motivations, fears and stake. One other disadvantage of PAR is that because of the committed nature of the participatory action researcher, participants may become suspicious of the researchers’ (political) agenda and he/she may be perceived as biased and overly passionate (Montero, 2000).
Background sketch of the development of the CBCIP
The CBCIP (L’Etang, 2011) aimed at young people living with HIV/AIDS (between the ages of 18 to 24 years) in a rural South African town (Lusikisiki, Eastern Cape province) in an effort to meet their psychosocial needs. The reason why Lusikisiki was chosen for this research, is that very few studies have been conducted in Lusikisiki on the provision of adequate care and support services to address the mental health and social needs of people living with HIV/AIDS (including young people living with HIV/AIDS) (Dickson-Tetteh & Ladha, 2000). Among the limited research available, a study conducted by Mango (2004) found that, although there were various psychological services for people living with HIV/AIDS and their communities in existence in Lusikisiki, no mention was made of any specific counselling services to address the needs of young people living with HIV/AIDS, in particular. By means of PAR the development of the CBCIP sought to draw on the indigenous knowledge of the target group. This was achieved through a variety of steps. Figure 1 below and the following paragraphs briefly describe the PAR process involved in the development of the CBCIP.
Actual stages undertaken in the development of the CBCIP.
Data were collected from three primary health care clinics, two non-governmental organizations (NGOs) (the Treatment Action Campaign [TAC] and Medecins Sans Frontieres [MSF]), one college and one hospital in Lusikisiki (which has an HIV/AIDS unit) (refer to Figure 1). These three clinics were chosen because it was anticipated that a sample of young people living with HIV/AIDS who met the selection criteria could be recruited more easily from these clinics.
The needs assessment (Potter, 2006) served as the first step to the development of the CBCIP (refer to Figure 1). The main aim of the needs assessment was to identify and assess the counselling needs of young people living with HIV/AIDS from the perspective of service providers (n = 10), community members who were present at the data collection sites at the time of the interviews (n = 10) and young people living with HIV/AIDS (n = 10) themselves. The interview questions were aimed at identifying the counselling needs and so it is acknowledged that the questions asked may have coloured the interview process and the resulting data. The open-ended interview method (Rosentahal & Rosnow, 1991) was the main method of data collection in this first step. With the help of a fieldworker who spoke isiXhosa, interviews were carried in out over a period of five days in December 2003. The data generated by this process were then analysed using thematic content analysis (Creswell, 2009).
The CBCIP was then compiled according to what emerged from the needs analysis (refer to Figure 1). The next step of the PAR process involved two focus groups (Kelly, 2006) in which the CBCIP contents and methods was presented to service providers by the first author (refer to Figure 1). Only two clinics were chosen to be part of this stage of the research because they were seen as more accessible areas to young people living with HIV/AIDS and because they had higher patient-loads compared to the third clinic. A separate focus group was conducted at each clinic (n = 8 at each clinic). The main aim of the focus groups was to elicit critical comments on the content and process of the draft CBCIP. In other words, service providers were invited to do member checking (Mertens, 2009). The duration of each focus group was approximately one hour. Hard copies of the draft CBCIP together with the counselling manual that accompanies the CBCIP were made available for the service providers so that they would find it easier to follow the discussion and also for their scrutiny of the CBCIP. For example, service providers raised concerns relating to the applicability of the homework exercise (included in the CBCIP) to clients who might be illiterate; concerns relating to the language of instruction on the homework exercise (for those who were literate) as well as concerns relating to time constraints in relation to the amount of information in Session 2 to be covered. The majority of service providers demonstrated an overwhelming enthusiasm and commitment to the concept of the intervention programme, especially since it was developed specifically for young people living with HIV in Lusikisiki. Only one service provider chose not to participate in the focus groups. The inclusion of service providers in the research was important. This is because service providers were seen as having a relationship with young people for whom the intervention programme was created. Service providers could therefore advocate for the intervention and approach the young people to participate in the study.
Following the modifications that were made to the CBCIP based on the critical focus group process, the subsequent step in the PAR process was the service provider (nurse in this case study)–youth participant collaboration to trial the CBCIP (refer to Figure 1). The purpose of the trial was to determine the shortcomings of the CBCIP as revealed through the process of collaboration between the service provider and youth participant and feedback between the service provider and the first author. One youth participant (a young female living with HIV/AIDS) received three counselling sessions that were based on the CBCIP. There were two reasons that only one participant was invited to participate in the trialling of the CBCIP. The first relates to a desire to work ethically and not to place multiple participants in a trial situation before the suitability of the CBCIP was clearer. Second, the focus group process had provided such detailed input on the contents and structure of the CBCIP, that the researcher was comfortable trialling the intervention with one young person only. The counselling sessions were conducted by the Professional Nurse in Charge at the clinic who invited the participant to participate in the trial as she had met the selection criteria for inclusion in the trial (i.e. she had been diagnosed within less than a month and was between the ages of 18 to 24 years). The aim of participation was explained to the participant as a trial process in which three counselling sessions based on a new intervention programme were to be conducted. Feedback of her experience of the intervention was to be used to tweak the intervention further. Feedback from the service provider on the collaborative process showed for example, that in Session 1 of the CBCIP, the participant was concerned as to why so many questions were being asked of her and was hesitant to answer. In Session 2, it was found that the participant did not fill in the homework exercise correctly because the service provider was unable to explain it adequately to the participant because he himself did not completely understand it. Lastly, in Session 3, no concerns were reported. Based on the findings of the service provider–youth participant collaboration trial the CBCIP was further refined (refer to Figure 1).
The resultant CBCIP consists of three sessions, each approximately 45 minutes in duration. Each session takes place on a weekly basis. The aspects of living with HIV/AIDS that the CBCIP is to impact include: somatic symptoms, anxiety and insomnia, social dysfunction and severe depression.
Lessons learned in the PAR process that led to the development of the CBCIP
In reflecting critically on the PAR process followed in the CBCIP research, it was possible to identify benefits, challenges and caveats. These are shared below.
Benefits of the PAR process
The importance of youth voices
Although the service providers and community members made valuable contributions to the needs assessment there were instances in which the young people living with HIV/AIDS raised needs and concerns that were unique. Service providers, for example, failed to recognize some of the needs and concerns of young people living with HIV/AIDS like relationship specific issues and depression management. If youth had not participated, the intervention contents would not have catered well enough for their needs. Thus, the benefit for future researchers is that the PAR process allows for youth voices to be heard and for researchers to tap not only into professional/adult knowledge but also into youth knowledge to create relevant and meaningful interventions for young people. Without youth voices, interventions are at risk of being either not meaningful enough or being perceived as an outsider's agenda.
Knowledgeable stakeholder input
PAR proved to be very beneficial to the development of the CBCIP in terms of the valuable information that was gained from the input of the knowledgeable stakeholders (service providers in this case). This was achieved through focus groups in which several important issues were raised by service providers. Were service providers not part of this stage of the development of the CBCIP, essential modifications such as the language of instruction of the homework exercise that could have contributed toward the intervention programme would not have been made. The benefit for future researchers, who recognize service providers as key informants, is that this information will provide them with necessary and local insight in the development of intervention programmes.
By drawing on the knowledge of service providers regarding the time constraints commonly involved in the counselling process within the rural setting (due to the lack of personnel), the PAR process helped to identify a possible deterrent to the success of the CBCIP. Future researchers should take heed of the restrictions involved in the application of intervention programmes, as voiced by service providers, as they may be more knowledgeable in this regard given their insider status and typically intimidate knowledge of the local.
Caveats and emerging lessons learned from the PAR process
Involving youth in the intervention design and implementation
One caveat in the development of the CBCIP was that the CBCIP was drafted by the first author and then presented to service providers in the form of focus groups. However, the indigenous forming of the CBCIP content and process should have commenced sooner (Mertens, 2009). What emerged from the service provider–youth participant collaboration to trial the CBCIP was that youth should have been included in the focus groups and should not have been ignored as experts. Were youth included, it would have been understood up front that youth feel threatened by many questions and the format of the first session could have been changed to a youth-friendly approach (e.g. inviting them to dramatize) (refer to Figure 2).
An ideal representation of a PAR process for intervention development aimed at young people living with HIV/AIDS.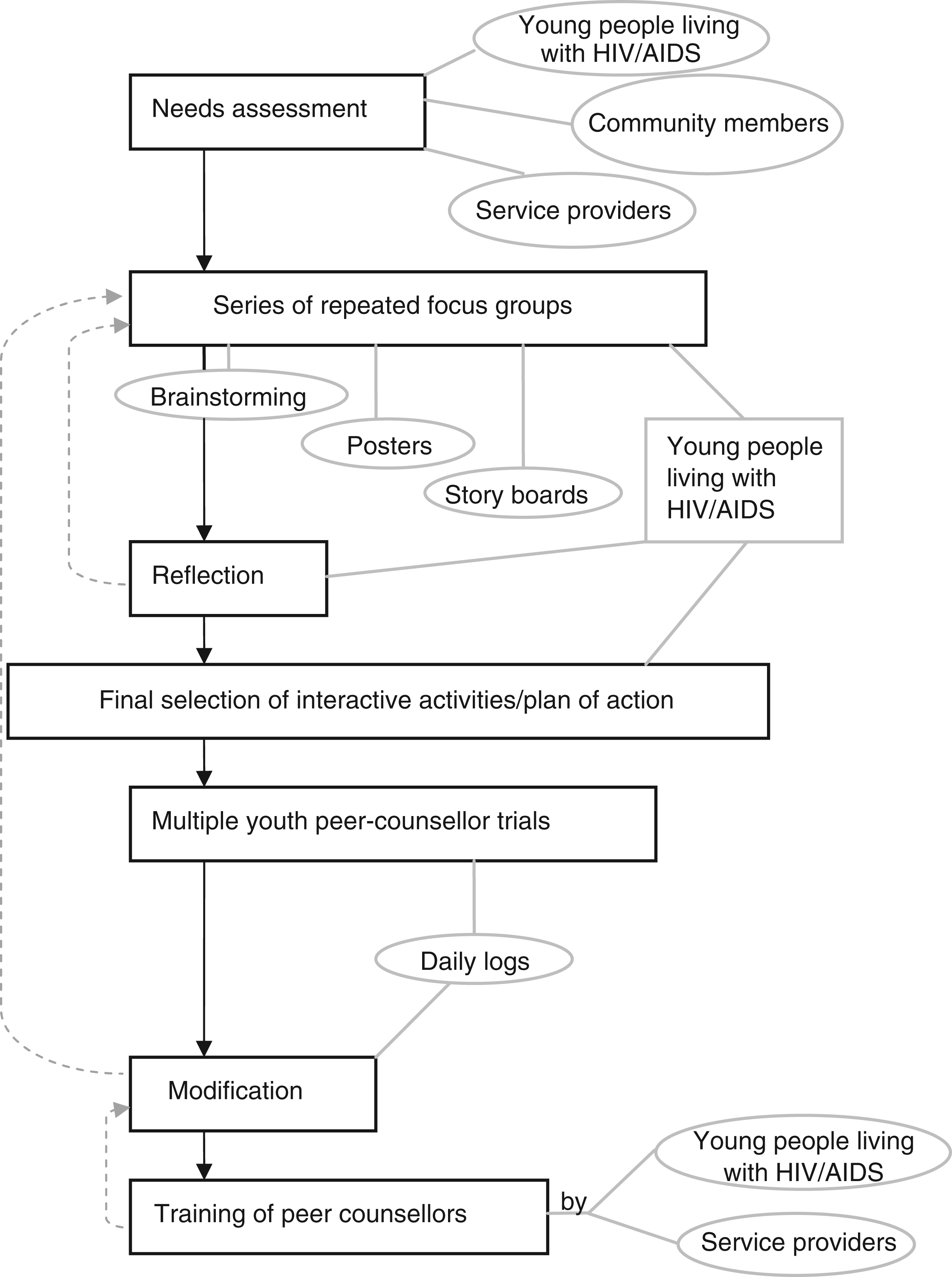
In retrospect, youth should have been afforded the opportunity to construct a plan for action. A higher level of participation should have been employed as described in The Ladder of Pretty (Pretty, Guijt, Thompson, & Scoones, 1995). Pretty et al. (1995) describe seven stages of participation using a ladder as a metaphor to differentiate a truly participatory approach. The lower levels of participation (levels 1 to 3) signify the participation of community members but only as sources of information. The higher levels, on the other hand, represent participation in which researchers and participants work as equal members (level 6) or where the participants construct their own plan for action (level 7). Concepts such as dialogue (Freire, 1993) and reciprocity (Fals Borda, 1998) are essential to the participatory approach of Pretty et al. (1995). Hence the role of the researcher in the current research should have been less prominent and should have been more that of a facilitator or dialogical coach. In this way, the PAR process would have been more closely aligned with the equitable essences of Freire (1993) and Fals Borda's (1998) participatory philosophy.
Walakira (2010) provides an example of the use of community dialogue approaches in which the role of the researcher was successfully maintained as supportive/supervisory. Through the use of Community Dialogue approaches, Walakira (2010) underscored the possibility of drawing on the knowledge of youth and other stakeholders in developing their own agenda and organizing a plan for HIV prevention in Uganda. Future researchers should consider the importance of a collaborative decision-making process in which youth voices are heard in the development of the intervention programme. Interactive activities such as brain-storming sessions and visual methods such as posters drawn or created by the youth can be used to help the youth to conceptualize the intervention programme contents (refer to Figure 2). In this way, the resultant intervention programmes may be more reflective of youth needs and of youth opinions.
In a study on the demands of community-based PAR, Jacobs (2010) commented that PAR can be used for the purposes of the empowerment of a community or it can be used as a means to improve the academic quality of research. Jacobs (2010) found that although empowerment was one of the goals of the ‘Aspiring to Healthy Living in The Netherlands’ project amongst elderly people, it was one that was not attained. This is because although community members had the opportunity to voice their concerns, they felt that it was irrelevant because they were not made part of the decision-making process to design the intervention for health promotion. Additionally, Jacobs (2010) found that members of the academic team had hidden meanings of participation (i.e. for either empowerment purposes or academic purposes) which caused clashes amongst the team and made them in some ways revert to the more traditional ways of conducting research as opposed to executing the empowerment goals of the project. Similarly, in the current study, more emphasis should have been placed on employing an empowerment approach that sought foremost to empower young people living with HIV/AIDS as opposed to improving the quality of the intervention programme. It is possible that were youth invited to participate in the decision-making process of the development of the CBCIP, they could have been empowered to realize their own capabilities to bring about change in their own lives and within their community. The lesson learned is that future PAR designs should try to aim to empower youth at every phase of the research and that empowerment should not be an unintentional consequence of intervention development. Once we as researchers had reflected critically on our hidden meanings to participation we realized that in the African context an academic agenda is not enough which is why researchers need to examine themselves and their research agendas if their research is to reflect the true essence of PAR (Ray, 2007 as cited in Jacobs, 2010).
The need for PAR researchers to be flexible and to let the PAR framework direct the research has become apparent both in previous research (Smith, Bratini, Chambers, Jensen, & Romero, 2010) and in the current research. Researchers need to decipher what is needed by the target group as opposed to just ‘pushing their own ideas’ of the sequence of events that should follow in the PAR design. This is in contrast to traditional research that follows a pre-defined research design that dictates the direction of the stages of research. Smith et al. (2010) for example, in a reflective study on the challenges faced by university-based researchers in America, found that there was a need to take action sooner than was anticipated as participants found the initial stages of the research as laborious from the point of view that it involved too much discussion and no activities. Consequently, they would have preferred if the action component of the research commenced sooner. Perhaps young people and even service providers of the current research would have benefited from this type of flexibility. They should have been asked to decide and direct the way forward (refer to Figure 2). In this way, it is likely that the power structures would have changed as the first author would have been able to relinquish her power and reassign it to the community thereby reflecting a more symmetrical relationship between the researcher and the participants (Fals Borda, 1998).
It may also be useful for future researchers to consider recruiting peer-counsellors to make the implementation of the intervention programme more youth-friendly (refer to Figure 2). A lesson that emerged from the service provider–youth participant trial of the CBCIP was that the participant did not fill in the homework exercise correctly because the service provider was unable to adequately explain the instructions of the homework exercise to the participant as he himself failed to understand it fully. Future researchers should consider that the training of peer-counsellors be conducted by other youth and/or that service providers be thoroughly workshopped using youth-friendly techniques such as role-playing activities which may be a more effective way to learn new concepts and skills. Peer-counsellors can also be paired with service providers for supervision. Previous research by Morisky et al. (2004) in an HIV/AIDS risk reduction intervention in the Philippines supports the use of these interactive activities with youth as favourable results were indicated. However, the rural setting may need to be taken into consideration in the PAR design. For example, the existence of power imbalances between the youth and adult staff (service providers) especially within the clinic setting is not uncommon in rural areas (Wood, Maepa, & Jewkes, 1998). Youth are often frowned upon, for being sexually active, for acquiring condoms from the clinic and are counselled and educated with an authoritarian style as opposed to a youth-friendly approach. The use of PAR within this setting, therefore, needs to be implemented with caution especially if peer-counsellors are to be paired with adult service providers and if the method is to truly empower young people as opposed to having the contradictory effect.
Involving youth in the service provider–youth participant trial
Future researchers may want to consider allowing peer-counsellors to conduct the intervention programme trial (refer to Figure 2). This may be a less threatening approach for young people living with HIV/AIDS and may create a more comfortable and open space for them to share their thoughts and feelings with a person of similar age. This is because young people may feel intimidated by adult service providers. This is often the case within the African culture where young people are reluctant to speak freely to their elders about certain issues (such as sex) because it is seen as culturally taboo (Campbell, Foulis, Maimane, & Sibiya, 2005). In this case, peer-counsellors may be in a better position to provide counselling to young people living with HIV/AIDS. Peer-counsellors can keep daily logs of the counselling process which may help in the modifications and refinement of the intervention model (refer to Figure 2). For example, in a study conducted by Feudo, Vining-Bethea, Shulman, Shedlin, and Burleson (1998) in an HIV/AIDS outreach model for at-risk youth in America, daily logs were used by project staff to document all peer educator activity. The method was found to be particularly useful in the training of peer educators and in the modification of the intervention programme.
The need for a cyclical PAR design
In terms of the shortcomings of the CBCIP research design, no additional time was given to service providers to think of other comments and suggestions regarding the content and process of the CBCIP. In other words, the researcher did not conduct subsequent focus groups with the same group and therefore did not make allowances for reflection time which may have been beneficial to the development of the CBCIP. Future researchers should consider employing a cyclical PAR design in which there is a continual recycling or spiral set of activities in the modification of the intervention programme (refer to Figure 2). The benefit of allowing participants time to reflect was shown by Walakira (2010) as it gave participants the opportunity to ponder on all the options available to them and contributed toward them making an informed choice of action plans. Similarly, Mantell et al. (2006) found that repeated focus groups amongst the youth led to critical consciousness which thereby brought to the fore the main elements for intervention. In addition to the need for reflection time, input from service providers and participating youth should be regular and not just at the design stage and the contents of the intervention programme should be continuously revisited, analysed and revised in accordance with the elements of the intervention programme that are working and that which are not, hence the need for formative evaluation (refer to Figure 2).
Contextual challenges of using PAR in a rural setting
One of the contextual challenges of using PAR within the rural setting pertains to the issue of language and translation. For example, the samples of community members and young people living with HIV/AIDS were made up of many individuals who were not fluent in English. Communication therefore took place by means of a translator (fieldworker) who explained the question in isiXhosa to the participant and then related the answer in English back to the researcher. It is therefore possible that the meaning/or some essence of the question/answer was not relayed in its correct form to either the participant or the researcher. As pointed out by Swartz (2002, p. 41), what is needed under these circumstances is to take into account ‘the impossibility of finding a perfect translation’. Having said this, it must be stated that situations such as these may have implications for the PAR process within the rural setting. The emerging lesson for future research relates to the possibility of including an external auditor (Creswell, 2009) in the research process who is familiar with the rural setting and translation difficulties to conduct an independent quality assurance of the information received before it is used in the development of the intervention programme. This will add to the overall validity of the research (Creswell, 2009).
Conclusions
The value of PAR lay in the importance of the voices of the ‘end users’ (the youth in this case) being heard and the need for the end users to be included in the intervention design and implementation as well as the evaluation stages. If future researchers recognize service providers as key informants in intervention design, this information can provide them with useful insight in the development of intervention programmes. But this value of PAR must be circumspectly used. The caveats are that the indigenous forming of the intervention programme's content and process should commence from the beginning that is, from the research design stage. Future researchers should consider the benefits and potential value of a collaborative decision-making process for both the participants and the researcher. Youth-friendly techniques such as the recruitment of peer-counsellors may prove to be useful in the implementation stage of future interventions. However, caution is drawn to need to consider the contextual challenges of applying PAR within rural settings. Nevertheless, when viewed holistically, PAR facilitated outsider–insider collaboration to potentially make a difference in the lives of young people living with HIV/AIDS in rural Lusikisiki.
Footnotes
Acknowledgment
We thank Hilary Bradbury-Huang for leading the review process for the author of this paper. Should you have comments/reactions you wish to share, please bring them to the interactive portion of our website: arj.sagepub.com.