
Abstract
The complexity of modern interdisciplinary health care practices, where different specialties work together to solve complex problems, challenges traditional approaches to organizational development and quality improvement. An example of this is surgery. This article describes and evaluates an action-oriented method to facilitate organizational development and innovation at an operating unit, centered on interprofessional aspects of health care, a method that shares some features with action learning. At its core the method had a group with members from all specialties in an operating team, who participated in regular meetings facilitated by a process leader, according to experiential learning principles. The group was evaluated using mixed methods (including interaction process analysis (IPA)), of which video recorded group meetings and interviews constituted the main sources of data. Results showed that the group achieved a successful organizational change. Indications of the success of the group process were the low level of conflicts and the high level of task focus. Interprofessional boundaries appeared to be bridged as all members participated in formulation of both problems and solutions while not being afraid to voice different opinions. Problems could be attributed to lack of awareness of the group at the operating unit at which the intervention took place.
Introduction
In this article, we describe and evaluate an action-oriented method to facilitate organizational development and innovation centered on interprofessional aspects of health care (Reeves, Lewin, Espin, & Zwarenstein, 2010). The method, which can be considered action research, is based on experiential learning principles, and it has some similarities with action learning (Kolb, 1984; Pedler & Burgoyne, 2008; Reason & Bradbury, 2008). The tested methodology puts heavy emphasis on the early stages of the action research process, i.e., on problem definition and on reflective exploration of the problem domain (Greenwood & Levin, 2007). As a consequence, it is particularly well suited in those instances where the outsiders or researchers understanding of the problem domain is limited, and it therefore is required that the insiders, i.e., the practitioners takes a very active role in both problem definition and exploration of the problem domain. Thus from the perspective of Greenwood and Levin’s (2007) cogenerative model, the method presented here, is mainly intended to ensure reflective action on the insider side of the model even though outsiders input is not discarded.
Modern health care is often described as complex (Glouberman & Mintzberg, 2001; Hughes, 2008). It is often multi-disciplinary in practice, with several medical and nursing specialties tending the same patient but focusing on different aspects of the patient’s condition. A good example is the operating team, whose team members not only are dependent on each another, but also on support structures, such as the central sterile services department for supplies and the pathology department. But also on other operating teams as the team frequently shares both equipment and personnel with other operating teams working in parallel.
Recent research addressing interprofessional collaboration in health care shows that differences in the perspectives of different professions can hinder the development of a holistic view of the patient’s condition. A contributing factor is the conflict that arise between their roles as team members versus their roles as representatives for their professions (Kvarnström, 2008). Differences in perspectives or rationales can cause unnecessary tension between professions (Rydenfält, Johansson, Larsson, Åkerman, & Odenrick, 2012), and differences in professional cultures can present barriers for interprofessional teamwork (Hall, 2005). Glouberman and Mintzberg (2001) go as far as to describe a hospital as not one, but as four different organizations, cure, care, control and community, with their own directions and priorities. It is important to consider these obstacles in projects that aim at quality improvement and organizational development in interprofessional settings, such as the operating room. One way of doing this is through methods that emphasize participation allowing different perspectives to be voiced and addressed in such way that practical issues that the different professions face are considered.
It is widely acknowledged that innovation is required in order not to increase the already sizable spending on health care in most developed countries (Berwick, 2003; Varkey, Horne, & Bennet, 2008). Innovative capacity depends on the relation between the need for exploration of the problem domain and autonomy regarding goal formulation and supervision (McGrath, 2001). In short, greater autonomy creates more exploration. In complex situations of high uncertainty, more exploration is needed to meet the unknown demands of the environment. If the problem domain is well known or simple, however, the opposite is the case. When reforming complex multi-professional health care contexts with conflicting perspectives and tension between different professions, the above mentioned need for exploration should be considered (Kvarnström, 2008; Rydenfält et al., 2012).
The following study presents a case that illustrates an example in which the need for exploration and participation has been addressed (McGrath, 2001). The case consists of an action-oriented group at a hospital operating unit, working according to a methodology built on krAft. With krAft referring to a method developed in Sweden to increase the competiveness of small- and medium-sized enterprises (Bergh, Thorgren, & Wincent, 2011; Daun et al., 2012; Norbäck, Olsson, & Odenrick, 2006; Sunding & Odenrick, 2010).
The original purpose of the action-oriented group was to (1) create collaboration between professions for shared reflection regarding the work activity, (2) develop proposals for improvements and their implementation, (3) develop their operating unit’s innovation capability and (4) feedback research findings to their work context so that they would be of practical use as well as being a basis for reflection regarding practice.
As previously stated, the method tested here was built on the krAft methodology, which puts heavy emphasis on experiential learning and on facilitating a fruitful meeting between the different group participants’ perspectives (Bergh et al., 2011; Daun et al., 2012; Norbäck et al., 2006; Sunding & Odenrick, 2010). But, it differs from the original method with regards to how different perspectives between members are provided. In the method tested here, the professions working in the operating room represents different perspectives (Rydenfält et al., 2012).
Aim
The aim of this study was to describe an action-oriented method for organizational development built around interprofessional communication, and to evaluate a case from a highly specialized health care setting in which such a method was used.
The action-oriented method
The central tenets of the krAft methodology are (1) experiential learning, (2) open dialogue between participants, (3) collaboration between practitioners and researchers and (4) acknowledgement of the importance of group processes. The participants meet in groups for a whole day on a near monthly basis for a year. It is essential that the group is action-oriented, that is strives to achieve or change something. It is also essential that the different group members feel comfortable sharing their individual perspectives on practice, as they constitute the point of departure for the groups’ collective sensemaking. In this way, the group has a second-person practice perspective as starting point for inquiry into the third-person and first-person domains (Chandler & Torbert, 2003). Besides the group participants, the group also consist of a process leader, usually a management consult, and a content leader who is an academic (Daun et al., 2012; Norbäck et al., 2006). The role of the process leader is to facilitate the group process, to ensure that the group develops into a well-functioning group or team, and to ensure that there are not too many conflicts or that the group falls apart (Wheelan, 2005a). The role of the content leader is to reflect on the content of the group’s discussions, to provide relevant content to the group and to, if needed, identify academic experts outside the group who can provide knowledge that can aid the group in its work.
Experiential learning, as outlined by Kolb (1984), is a central aspect of a krAft group’s activity. The problems the group members work with should be based on their own experience and needs, thus constituting the concrete experience stage in Kolb’s (1984) four-stage experiential learning cycle (see Figure 1). The role of the process leader is to promote an open dialogue between group members and to first encourage reflective observation, which is the second stage, and then abstract conceptualization, the third stage of the experiential learning cycle. By means of reflective observation, the perspective on the observed topic is altered or widened; it is explored from more angles due to reflection. The phase consisting of concrete experience and reflective observation is called the divergent phase as it is about exploration and widening one’s understanding. Abstract conceptualization means that the aspects of the altered view of the observed topic are integrated or grasped through the formulation of new meaning structures and ideas or the reformulation of old ones. This stage is followed by the fourth and last stage of the cycle, active experimentation, where the testing of ideas and new ways of doing things is carried out. The phase consisting of abstract conceptualization and active experimentation is called the convergent phase, as it is concerned with narrowing the focus so that decisions on actions can be made, and those actions can be tested (Kolb, 1984). Being a model that integrates previous work by Lewin, Dewey and Piaget (Kolb, 1984), the experiential learning cycle shares many features with Lewin’s classic description of action research as an iterative process where each iteration “is composed of a circle of planning, action and fact finding.” (Lewin, 1946, p. 38) The krAft methods heavy focus on facilitation of action, on developing workable solutions to practitioners’ problems, positions it closer to the pragmatic tradition within action research than to the critical (Johansson & Lindhult, 2008).
An illustration of the group’s learning process in relation to Kolb’s (1984) experiential learning cycle. The Roman numerals represent phases in the group’s development and learning process. The numbers in parentheses represent group meetings.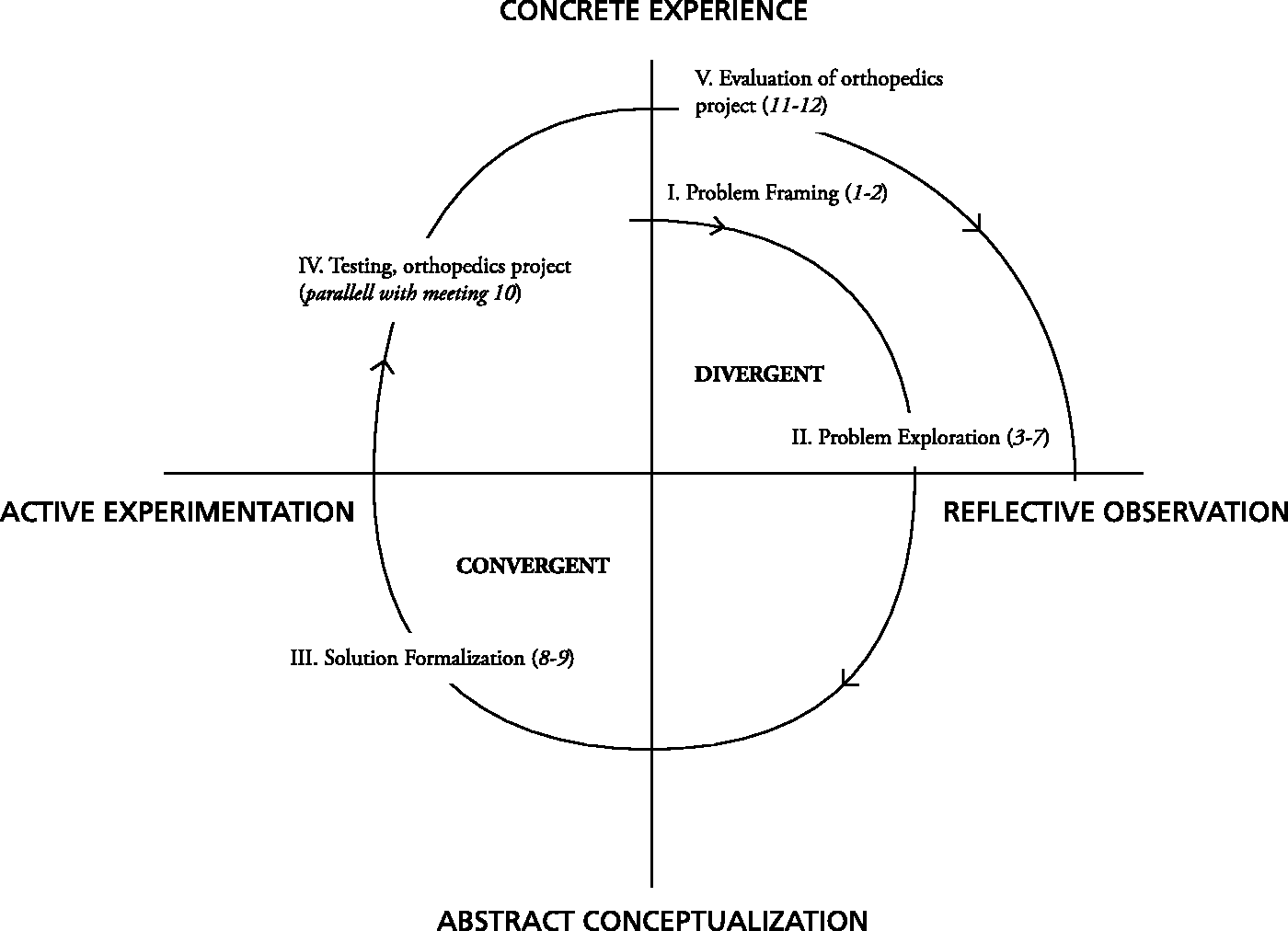
The idea with the krAft group is to ensure that the group members go through the entire experiential learning cycle and thus achieve an altered understanding of their practice and the problems addressed. The group should thus formulate both problems and solutions themselves. This may appear to be straight forward, but it is generally easy to get stuck in a smaller cycle composed of the first and the fourth stage, going directly from concrete experience to active experimentation; in practice this means that a trial and error approach is pursued. When this happens the learner cannot reach a deeper level of understanding or reframe or reformulate the problem at hand, i.e., it thwarts double loop learning (Argyris & Schön, 1996). Getting the group to converge is generally not a major problem for the process leader; the problem, in most cases, is to make the group more divergent. It must be emphasized the group should work with problems rooted in the group members own experiences (i.e., on the first stage in the experiential learning cycle) and needs as well as develop the solutions to those problems themselves. These principles has some resemblance with action learning. However, the methodology differs in that it lacks the dislike of experts associated with action learning (Bergh, 2010; Kemmis & McTaggert, 2000; Pedler & Burgoyne, 2008). In fact, inviting experts to the group is an important part of the method. Another difference is that the method presented here puts larger emphasis on the research or reflective stage in the experiential learning cycle than what is sometimes associated with action learning. In action learning research sometimes is just seen as a way to get on to the next, albeit developed, action (Pedler & Burgoyne, 2008). Forcing the group to stay a little longer in the divergent phase helps the group to question their current practice at a deeper level, that is, it creates conditions that facilitate questioning insight (Rigg, 2014).
Due to the methodologies reliance on the sharing of the different group members perspectives with each another, trust is an important component that has to be considered in this kind of groups (Bergh et al., 2011). Newell and Swan (2000), distinguish between commitment, companion and competence trust. Bergh et al. (2011) state that trust building starts with commitment trust, such as committing to being part of a group or doing a job. Companion trust and competence trust are built as the trustees get to know each other. While commitment and competence trust are quite fragile, companion trust appears to be more resilient (Bergh et al., 2011).
In this study, we worked with one hospital unit instead of several organizations with a common line of business. The common line of business in krAft resulted in a common objective and a sense of shared meaning to the group, hence motivating the participants, while their backgrounds in different enterprises ensured variation in perspectives. This was important in order for them to challenge one another’s perspectives and to start thinking in a divergent manner. A larger variation in the ways is in which a phenomenon can be experienced is associated with more successful learning (Marton & Booth, 1997). In applying the methodology to the hospital operating team, the approach was the opposite in the sense that: the participants were recruited from the same organization, but they constituted different parts of the interprofessional group that provides care to the patients in their organization. Thus, their profession backgrounds provided variation in perspectives, and their common organization provided them with a common focus and motivation to participate.
Method
Design
The overall design of the study can be considered as action research, since the practitioners worked alongside and interacted with and had input from researchers according to a method with emphasis on reflection and action (Reason & Bradbury, 2008). As previously mentioned, the tested action-oriented method has some resemblance with action learning, but its emphasis on reflective observation in every action cycle and the usage of experts as input to the group places it closer to the action research tradition. The study was designed as a single case study, a design suitable when the purpose is to test a previously formulated theory (Yin, 2014). The main unit of analysis was threefold in the sense that the operating unit constituted the overall unit of analysis, as we were interested in effects on the operating unit level. However, as the hands on intervention work took place in the group, the group constituted another, embedded unit of analysis. A project, initiated and inspired by the group, the orthopedics project was also evaluated by the research team, as it was considered as a result of the group’s work, and hence, also constituted an embedded unit of analysis.
The group was followed by an observer (the first author) who was present during all, but two meetings. As the observer was there and occasionally interacted with the group during meetings, the observations should be regarded as participatory, even though the observer distanced his approach to the group and was not regarded as a group member (Gobo, 2011). In addition to the observations, all meetings except the first were video recorded, and individual interviews were conducted. The methodology used to evaluate the case can be considered a mixed methods design as both qualitative and quantitative data was used. More specifically, it has much in common with what Creswell, Plano Clark, Gutmann, and Hanson (2003) calls a concurrent triangulation strategy. Even though all data were not collected concurrently, it was considered concurrently in the analysis.
Sample and data collection
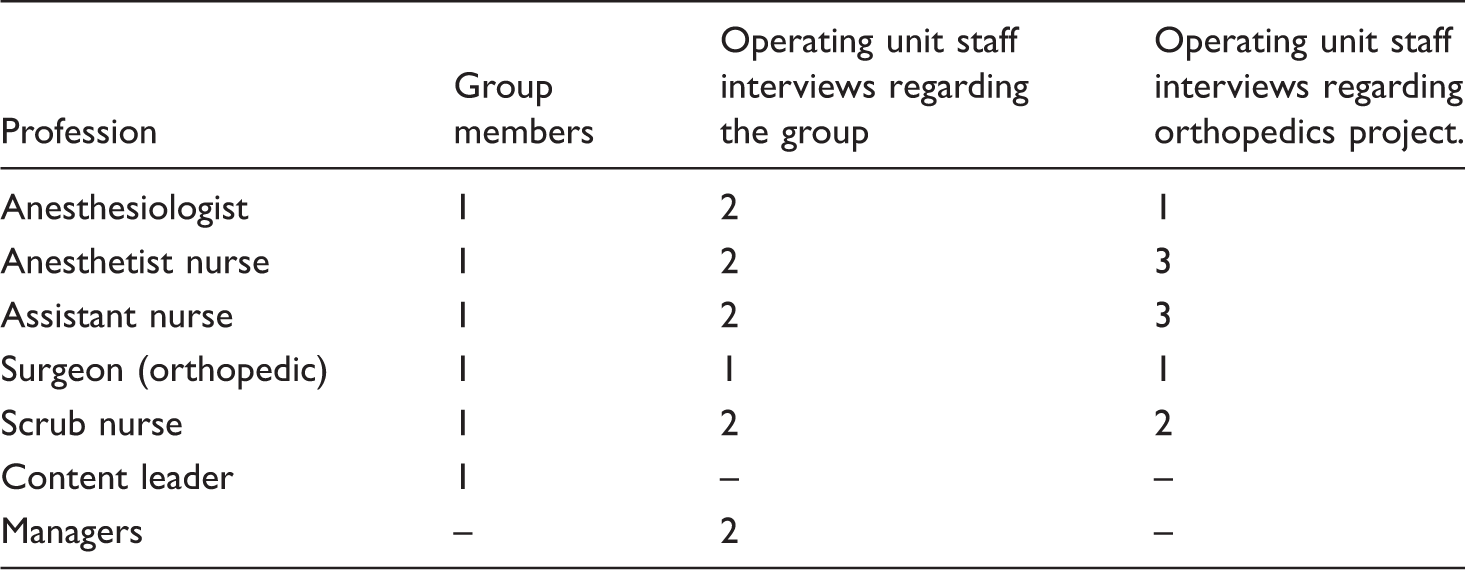
The group had a total of seven members, of which one was the process leader. The other members were a surgeon specialized in orthopedics, an anesthesiologist, an anesthetist nurse, a scrub nurse, an assistant nurse (in Sweden the assistant nurse has a role similar to that of the circulating nurse) and a surgeon acting as a content leader. All group members, except the process leader, worked at an operating unit of a Swedish county hospital, and they were in various ways involved in surgery. All group members except the content and process leaders were selected by management on the merits of being perceived as creative and positive. The content leader was recruited by the research team, and the process leader was part of the research team. The content leader was a field expert rather than an academic, and the process leader also provided some of the content. Thus, the content leader became more of a bridge to the field working with the process leader. As the process leader and the observer in various ways worked with and interacted with the practitioners directly they also were the primary “action researchers” of the project. However, the research group also consisted of a third member that was active in the planning and evaluation of the project. In the research process, the researchers together with the practitioners strived to develop actionable knowledge useful for the practitioners and their unit, a task in which the practitioners themselves were the largest contributors, while the researchers at the same time conducted research on the process.
Interviews conducted in the different units of analysis of the case.
The group meetings varied in length, to investigate the group process development and functioning, the first hour of the videos from seven of the group meetings was selected for deeper analysis. The inclusion criteria were (1) that the process leader was present and (2) that the group did not have any visitors during that hour, as this would have affected the group dynamics. The last meeting, which was used to evaluate the group, was also excluded.
Consent was obtained from the study participants about the use of the video recorded meetings and interviews for research purposes. As participation was voluntary and no patients or other persons in a dependent situation were involved, permission from the Research Ethics Committee was not required.
Analysis
All interviews were semi-structured and were transcribed and analyzed with qualitative content analysis with the help of QSR International Nvivo 10© (Kvale & Brinkmann, 2009; Patton, 2002).
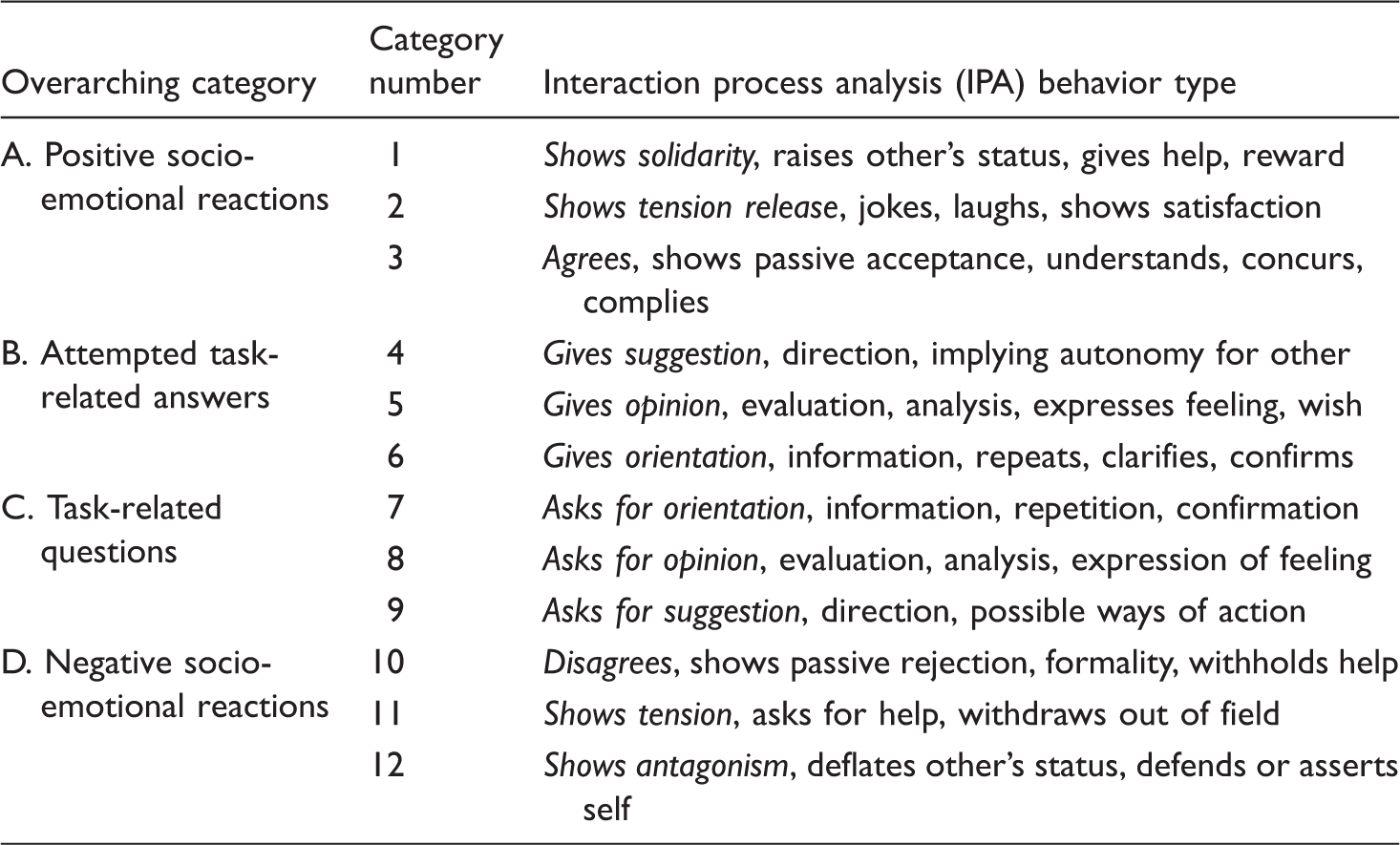
The IPA categories after Bales (1950). In the analysis, a Swedish translation by Einarsson and Hammar Chiriac was used (2002).
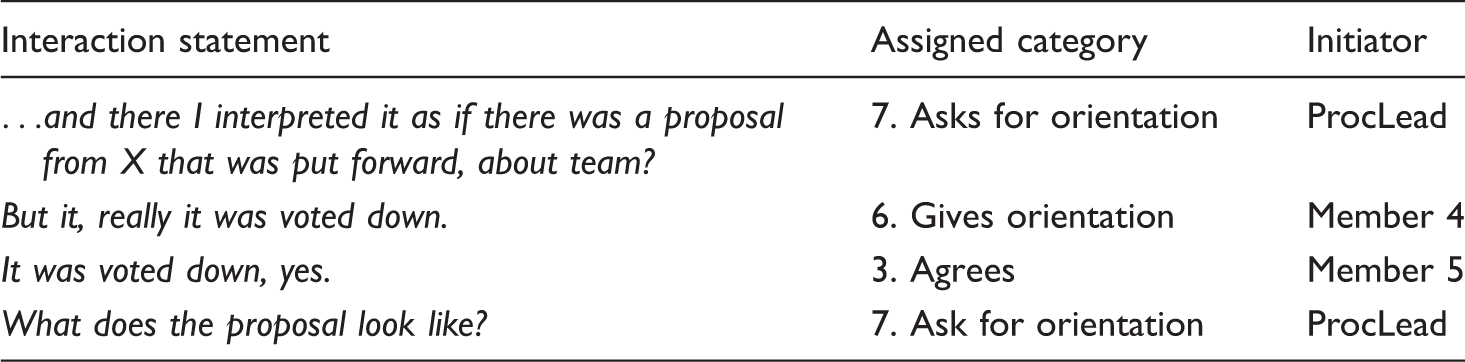
An illustrative example of the IPA with the analyzed statements to the left.
Results
In the following section, we will first describe the groups’ process. We will then describe the orthopedics project, followed by the perceptions of the group held by the group members as well as by the department staff members, respectively. Finally, we will present the IPA results.
Task process development
The first two group meetings were predominately used for problem formulation with the first meeting being more tightly organized by the process leader to help the group get started. Already at the second meeting, the group decided to focus on the topic of orthopedic surgery. We interpret the activities during the two first meetings as the problem framing phase providing direction for the group, even though the problem is by far not fully investigated at this stage.
In the following five meetings, the group members predominantly discussed their practice in relation to orthopedics and by doing so created an expanded common understanding of how orthopedic surgery was related to other parts of the practice, such as the needs of other specialties and the operating unit’s work methods in general. Previously conducted time studies were discussed and their quality questioned. Dependent requirements on post-operative care and outpatient surgical units were also discussed. Prioritization and scheduling were discussed because orthopedic patients often are emergency patients, but are not considered sick enough to be given high priority; their surgery thus risks being postponed in favor of patients that are more critical. A desire to start orthopedic surgery early in the morning as well as to ensure that it was not removed from the list in the afternoon was expressed in order to decrease the number of postponed orthopedic surgical procedures as well as the number of orthopedic surgical procedures conducted at night. The group learned that a parallel discussion regarding patient flows was being held at the managerial level. A flowchart over the operating procedure was developed iteratively to visualize how different steps in the process are dependent on each other with the help of the researchers, i.e., the researchers provided visualizations based on discussions in the group that the practitioners reflected on which led to modifications. In turn, the researchers got a deeper understanding of the procedure and its dependencies. Routines for bringing the patient to the operating room were investigated and discussed with those who were perceived as being responsible for this task. New ideas for routines for calling down patients to surgery were investigated and tested by group members. Limited personnel resources and limited space in the operating unit’s waiting room (it takes only five beds) were identified as bottlenecks that made it hard to start more surgical procedures in the morning. One group member also conducted observations for a day in two different operating rooms, which showed that there was a huge difference in efficiency between them. During these meetings, the possibility of having one operating room open longer in the evening for orthopedics was also brought up with the operating unit’s manager. At the sixth meeting, the group really started to consider the role of the team during surgery and in what way teamwork was conducted. During the seventh meeting, the possibility of making the operating rooms committed to orthopedic surgery, their own team was brought up. The phase consisting of the third to seventh meeting can be said to constitute the problem exploration phase of the group’s process since many of the activities during this phase, the assembling of data on how it really worked by asking and observing, and long reflective discussions regarding the problem domain could be seen as divergent activities (Kolb, 1984). Some of the activities in this phase could also be seen as small learning cycles of their own. For instance, the formulation and testing ideas for new routines for how patients should be called to surgery, mentioned above, contains both planning, execution and fact finding for the purpose of both evaluation and to gain a better understanding of the current conditions (Lewin, 1946).
In the following two meetings, 8 and 9, the group became more convergent. One of the group members, member 3, was part of another group put together by management to improve the efficiency of orthopedic surgery. Member 3 thus fed experience from the problem exploration in the action-oriented group to the orthopedics group and the orthopedics group initiated the orthopedics project. But the outline of the orthopedics project was based on the ideas developed in the action-oriented group. We call this the solution formalization phase in the action-oriented group’s activity. At the eighth meeting, Wheelan’s (2005a) definition of an effective team was discussed on the researcher’s initiative. Members expressed that the people working together in the operating room are far from an effective team, as described by Wheelan. One member stated reflectively that “we are not even a group,” according to Wheelan’s definition. The subject of the teams at the operating unit being organized around professions rather than around operating rooms or patients had already been discussed at the second meeting. Another member concluded that the best days at work were those days when she worked with the same assistant and anesthetist nurse the whole day, with no outside interference. This type of insights played an important role in the design of the orthopedics project. The insight that operating team was not even a group can be interpreted as an instance of double loop learning as the traditional (in health care) idea that the people working together in the operating room is a team, is being questioned (Argyris & Schön, 1996). Making room for questions in the spirit of, if it is not a team, then what? How do we make it a team?
It took a while to anchor the orthopedics project sufficiently at the management level and to find a good time period for it, but after meeting 9 the project was started and between meetings 9 and 11, the orthopedics project was tested. We label this phase the testing phase.
During meetings 11 and 12, the results from the orthopedics project were assembled and evaluated by one of the group members. This was reflected upon, and a second evaluation to be conducted by the academic observer was discussed. The last and 13th meeting was dedicated to evaluating the whole group process.
The group process relation to Kolb’s (1984) experiential learning cycle can be seen in Figure 1.
The orthopedics project
The orthopedics project took place for six weeks between meetings 9 and 11. The purpose of the project was to increase the effectiveness of orthopedic surgery by concentrating surgery to office hours and avoiding surgery postponements. These goals were largely met by
organizing the three operating rooms in the unit committed to orthopedic surgery in their own large team; previously, different personnel categories had worked in their own professional teams organized around two or three operating rooms, rather than around a surgical specialty; assigning one of the operating rooms committed to emergency surgery to orthopedic emergency surgery during the late afternoon; provision of a whiteboard with all personnel and their assigned operating rooms clearly marked to get a better overview of who was doing what in the team; dedicating one anesthesiologist to all orthopedic surgery and conducting a morning team assembly at the whiteboard.
It should be noted that, in Sweden, anesthetist nurses handle most of the anesthesia on delegation from the anesthesiologist. Though the anesthesiologist has planned the anesthesia, he/she is only directly involved if the case is deemed extra difficult.
During the project, there was a significantly smaller amount of orthopedic surgery performed during evenings and at night. In this sense, the project was successful as surgery during nights is associated with diminished patient safety (Etchells, O’Neill, & Bernstein, 2003). However, the staff’s perception of the change was not unambiguously positively expressed in the interviews. On one hand, it was reported that the staffing situation was more predictable, that it was calmer in the operating room, that the responsible anesthesiologist had a better overview and that the patient flow was better. On the other hand, some anesthetist nurses who had previously worked in professional teams in two operating rooms felt uncomfortable working in teams organized around three operating rooms because it was perceived as harder to get an overview of the patient flow.
Directly after the orthopedics project was finished, it was discontinued with the exception of the whiteboard that is still in use. However, a year after project completion, scrub nurses and assistant nurses had started to work together in teams organized around surgical specialties and operating rooms rather than around their profession. Thus, the project resulted in some organizational change in the intended direction, even though the change was not as big as initially intended.
The group members’ experiences
During the interviews with the group members, all of them stated that there were no conflicts in the group during its course of existence.
Regarding the group’s functioning and dynamics, the members seemed to agree that everybody in the group was not afraid to speak freely. They also expressed that the discussions were enjoyable. Here is what three of the members had to say on the matter: Yes, first because it’s nice to go there. I’ve looked forward to it and I think the discussions have been very good. There have been a lot of good suggestions and the atmosphere has been very open minded, and you knew you could say what you thought and what you felt. I learned a lot! Well, I think the people have been good at seeing all the professions, actually, and that we have been comprehensive . . .we haven’t come up with any answers but you know what I mean, that everyone has had their say. … at the beginning we were quite cautious and continued to be so until we got to know each other and then the dialogue was more open. I think it ended up being a really fun group with good ideas and it worked out. Nobody was, like, embarrassed about anything they said, but it was just a matter of saying anything you wanted, like speaking from your heart in a way.
Regarding the way the group formulated problems and selected tasks, group members had different opinions: Some felt that a clear goal would have been desirable; others felt that because the group defined its tasks itself, this ensured that the tasks felt relevant. One member stated that the main problem was that they were not used to defining problems themselves but rather that the problems were presented to them by someone else. They felt less constrained, though, when defining their problems themselves and that everything fell into place as they went along.
The operating unit
At the operating unit level, the action-oriented group’s purpose and its activities were not well known. Those interviewed reported that the group’s purpose was related to rebuilding of the unit’s facilities, better work environment and improvements in orthopedic surgery. Several participants, though, reported that they did not know anything. When asked what their colleagues thought about the group, a couple of participants answered that they had not even heard anyone talk about it. However, the two orthopedic surgeons interviewed, of whom one was a head and chairperson of the clinic, answered that the group worked with things that had to do with the orthopedic specialty. Hence, the group’s activities were poorly anchored with other staff at the operating unit, expect for those working in the orthopedics clinic.
Interaction process analysis
In total, 5611 behaviors were scored for all the action-oriented group members from the selected videos. When excluding the process leader and observer, 3894 scores remained.
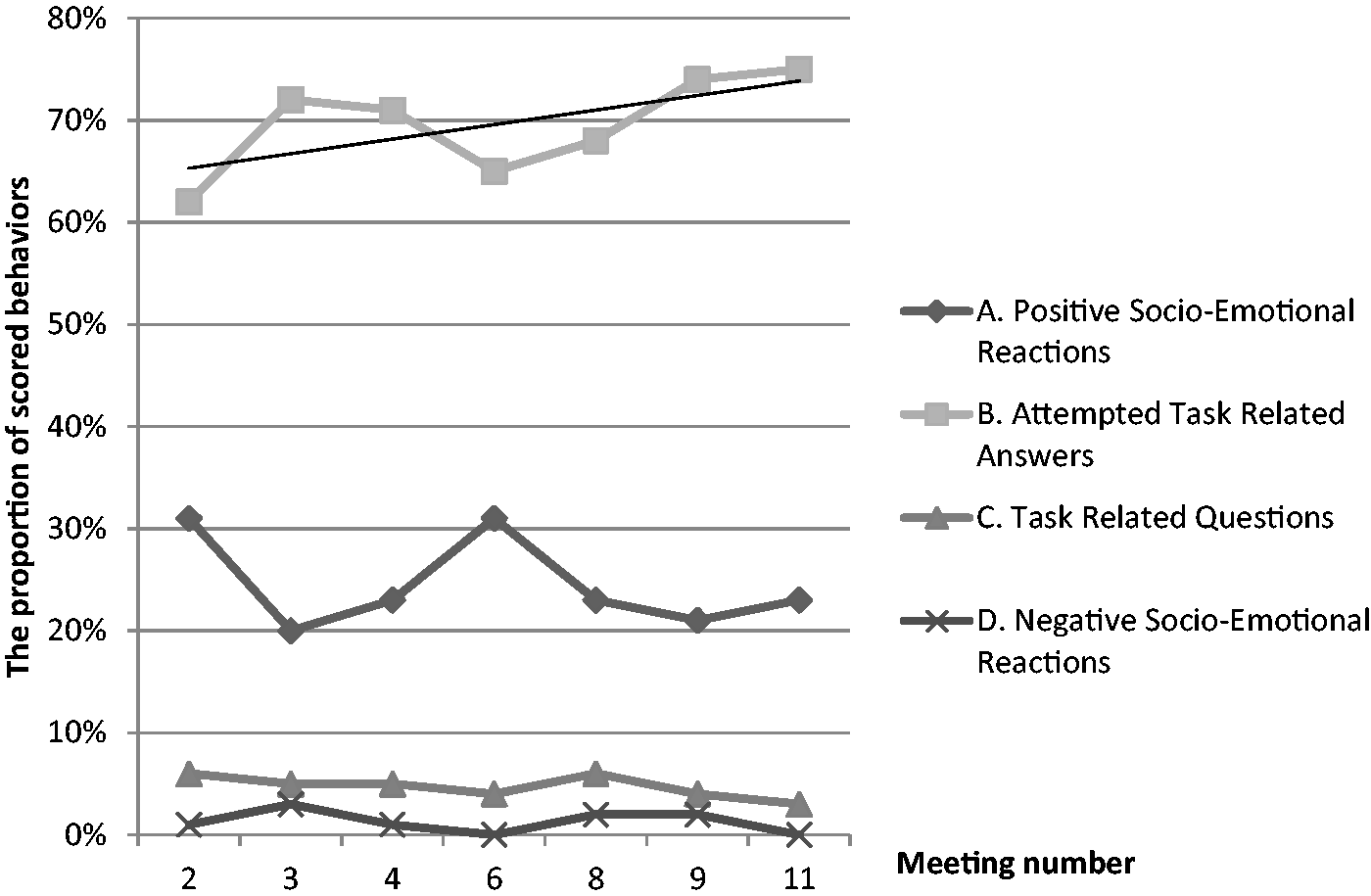
When the orthopedics project was decided upon, the group member responsible for it, member 3 took an increasingly larger role (see Figure 2). The increase in activity had a non-significant Pearson correlation coefficient (r = 0.745, α = 0.054), even though the correlation coefficient could be considered strong. Over time, a tendency towards an increase in category B was shown, and the correlation between meeting and score is strong (see Figure 3). But again, the correlation was non-significant (r = 0.599, α = 0.156). Between 68% and 78% of the scores at the different meetings were task related, that is, they belonged to the overarching categories B and C, with a mean of 74%.
The proportion of scored behaviors per meeting for each action-oriented group member and the observer. The total number of underlying scores was n = 5611. The proportion of the four overarching IPA categories over the seven categorized meetings, excluding the behaviors of the process leader and observer. Total number of underlying scores n = 3894.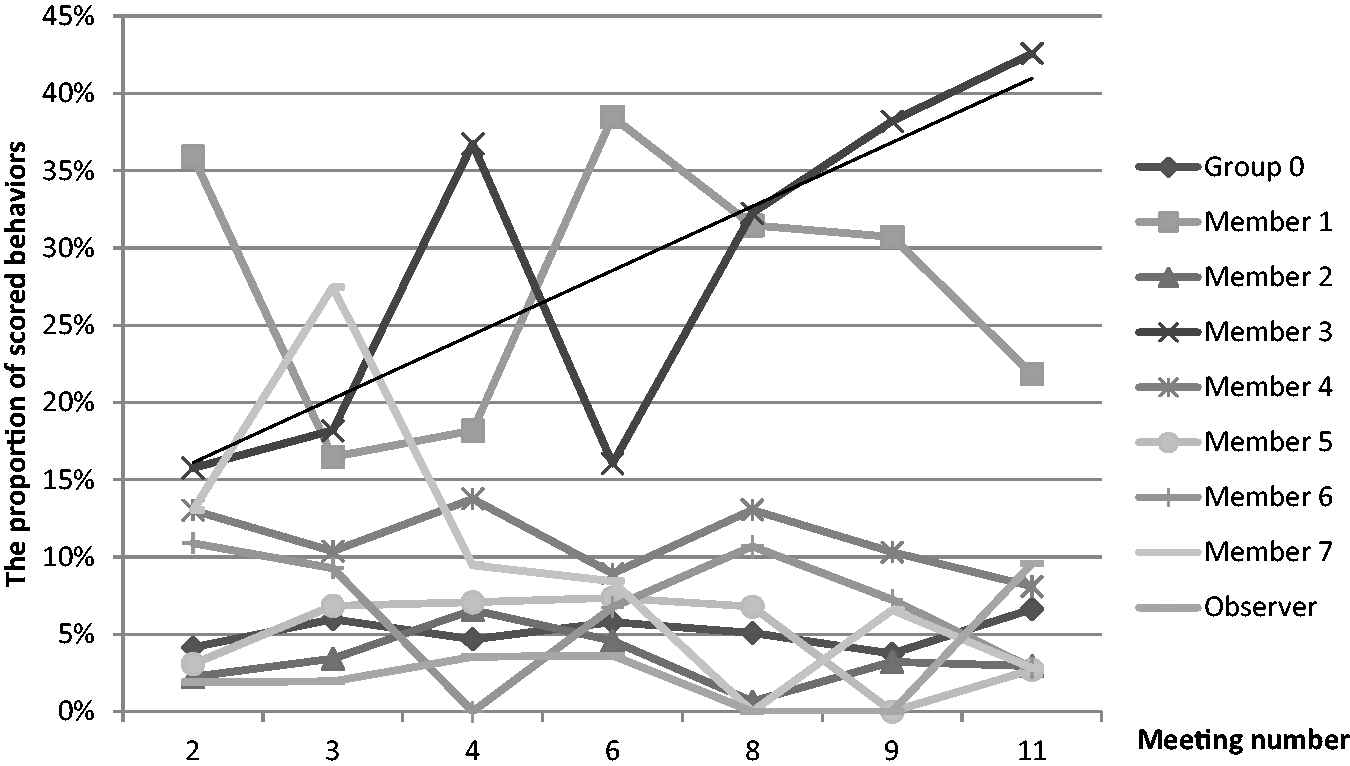
Discussion
The group managed to go through the experiential learning cycle (Figure 1), the interviews described a free and open dialogue in the group and a group process without any serious conflicts. The group put a substantial amount of effort into problem exploration during meetings 3–7, indicating that the autonomy given the group resulted in increased exploration (McGrath, 2001). Thus, in relation to the central tenets of the krAft concept, the action-oriented group process has to be regarded as a success.
Group process
The open dialogue, and that the members of the group were not afraid to show their vulnerability also indicates that trust was established. As stated in the interviews, the climate in the group was initially expectant or wait and see, but once people grew more familiar with one another, it became a group with an open dialogue. This indicates that the level of companion trust did increase during the course of the group meetings (Newell & Swan, 2000). The very low level of negative socio-emotional reactions shown by the IPA and the high level of attempted task-related answers, whom also appeared to increase over time, supports the assumption that the group members had sufficient trust for each other to stay focused on their task, rather than to have to attend to efforts to sustain a sufficient level of trust in the group.
We identified three possible explanations of the remarkable lack of conflict: (1) that group members were chosen among personnel perceived as positive and cooperative, (2) that they only had meetings every third week for one year and (3) that they in a sense already were a group as they all worked at the same unit and knew each other to a varying degree before accepting to participate in the group. We regard the last explanation to be the most plausible and that the group, as a consequence, already had gone through the earlier steps of group development to some degree and thus already passed those phases normally associated with conflicts (Wheelan, 2005b).
There were differences in activity levels between group members as can be seen in Figure 2. One possible explanation for member 3’s high activity level, especially towards the end, could be because of this person’s important role in the orthopedics project.
Figure 3 shows that the group scored extremely high on overarching category group B (attempted task-related answers). According to Bales as referred by Wheelan, the optimal proportion between task related (B and C) and group maintenance or socio-emotional (A and D) is 60/40%. But according to Wheelan’s more recent measurements, the optimal ratio is rather 80/20% (Wheelan, 2005b). In our study, task-related behaviors had a mean of 74%, which is closer to Wheelan’s optimal value than to Bales’, albeit in between the two. We take this as an indication that the group indeed was very task focused. Related to this is that the group scored very low on overarching category group D (negative socio-emotional reactions). These low scores are supported by statements from the interviews that the group had no conflicts. In light of this, together with group members’ reports of a very good group process with good dialogue and good discussions, the high task focus reported in the IPA analysis does not seem out of place. Thus, through triangulation with IPA results and interviews with group members, we conclude that the group was very task focused (Miles & Huberman, 1994). This is interesting considering that the group defined its goals by itself, since unclear goals have been pointed out as something that affects performance negatively (O’Leary-Kelly, Martocchio, & Frink, 1994). A hypothesis we have is that the group, as it was put together in order to provide the participants with a common frame of reference (their common workplace), while at the same time providing different perspectives (their respective professions), had easier to develop common and relevant goals.
Reflection and learning
Compared to the defined original purpose of the group, the interviews with group members showed that collaboration and shared reflection regarding the work activity between professions certainly did occur. The group also managed to develop proposals for improvements that were implemented specifically in the form of the orthopedics project. On the group level, it is likely that the members learned about approaches to innovation and organizational development that they could use in the future. In fact, the interviews showed that the way the group operated was new to the members. For instance, one member stated that “Well, I haven’t worked in a group like this under such conditions before. It’s a new way for me….” As the groups ideas about the orthopedics project at least to some degree had effect on practice a year after the orthopedics project ended, and that the design of the orthopedics project was influenced by research on teamwork as well as the groups own inquiry into their own practice, research findings was fed back to practice in ways that made them come to use.
Problems in the group’s work and with the method did not much appear on the group level but rather in the group’s interaction with its surroundings. Our interpretation is that it, even though the group succeeded to convince management to support its ideas, was extremely difficult for management to mobilize resources around the group’s initiative for reasons beyond the group and even beyond management. For one thing, when implementing projects such as the orthopedics project in a large operating unit serving many specialties, a substantial number of operating specialties will be affected. Some could suspect that the project, though favorable for orthopedics, would be a disadvantage for them and the same holds for the different professions working in the operating room. In this sense, this could be a manifestation of the differences in perspectives and priorities between different parts of the organization as well as between different professions associated with healthcare. This in turn is something that makes a hospital extremely difficult to manage (Glouberman & Mintzberg, 2001; Rydenfält et al., 2012). While Hughes (2008) points out that management support is a key facilitator when conducting action research in health care, management’s ability to commit in practice can be hampered by the conflicting strong interests mentioned, even if management has formally committed to the project.
Methodological discussion
In relation to Chandler and Torbert’s (2003) typology of action research, the voice of the work presented here, is mainly second-person, through its concern with inter-subjectivity (and the lack there of) between group members and informants as expressed in interviews and at group meetings. But, it can also be considered to express a third-person voice in the form of the IPA methodology which is more detached from the research subjects and thus also can be considered more objective by some. When it comes to practice (Chandler & Torbert, 2003), we have mainly focused on second-person practice, that is on the interaction between the group members in the group. However, in the work conducted by the group, a third-person practice perspective was also applied in the sense that group members inquired into the other parts of the organization far outside the group itself. For instance, into how orthopedic surgery currently is organized and into how the hospital wards that send patients to surgery prepare patients as well as through mobilizing other forces at the operating unit (i.e., management) around the orthopedics project. The case also illustrates how learning in the first-person domain, i.e., how single group members becomes aware of that “we are not even a group” in the operating room, are shared in the second-person domain resulting in a reframing of what teamwork looks like in the operating room which in turn results in a new vision about how good teamwork should be achieved affecting the third-person domain in the form of the orthopedics project.
Limitations
Despite that the project described above was successful; we identify two factors that could have hindered the project from reaching even better results. The first limitation is the above mentioned size of the operating unit as compared to the size of the group. The second limitation is concerned with whom we decided to involve and invite to the group. As can be seen above, the group is constituted entirely of healthcare professionals. It could be argued that also patients should be involved in a project like this, as it is for them the care provided is intended. However, for two reasons, we decided not to involve any patients. First, it would be much harder, not at least for ethical reasons, to assemble such group. Second, inviting only healthcare professionals to the group puts less pressure on the group members which in turn provides a better foundation for dialogue and openness between the group members. In one sense the format allows for the patients to be involved. As it is the group members that ultimately decide what direction their project should go in, they could also decide to involve patients, even if this was not the case in the project described here.
Conclusion
In this article, we report on an action-oriented method, inspired by action learning, intended to facilitate organizational development and innovation capability, while at the same time considering the interprofessional aspects of complex health care settings.
The method studied worked very well on the group level, the group was very task focused and sufficient levels of trust, in order to allow an open dialogue, appeared to be established in the group. The group also delivered results in the form of new ways of working. However, the method as implemented here, had limited effects at the operating unit level, apart from the implications of the group’s work on the units’ ways of working. Despite this, we found that the action-oriented group method was promising and managed to bridge interprofessional borders within the group. This resulted in problem formulations and solutions that all members in the group could agree on. However, we acknowledge that it would be desirable to involve the wider community at the operating unit even more in the group’s inquiry. Though this would probably require a different strategy as the sheer size of the unit was identified as an inhibitor of wider involvement. We conclude that this, for instance, could be achieved through the establishment of more groups working in parallel at the department with organizational structures being established that facilitates exchange and dialogue not only in those groups, but also between them.
Footnotes
Acknowledgements
The authors would like to thank editor in chief Hilary Bradbury and associate editor Svante Lifvergren as well as the anonymous reviewers for valuable feedback on previous versions of this manuscript that we sincerely thank who had helped us to make the manuscript much better. We welcome and invite your comments and reactions at our action research community's interactive ARJ blog housed at AR+ ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Gorthon foundation, which is a private foundation residing in Helsingborg, Sweden.