
Abstract
Stress of conscience seriously influence the quality of care and the wellbeing of the care providers in care for older people. It is therefore of great importance to take measures to address, and relieve but preferably prevent stress related to troubled conscience. In our participatory action research studies, we have used troubled conscience as a driving force to relieve care providers’ burden and to increase quality of care. The aim with this paper is to present our experiences of using a further developed participatory action research process in practice to deal with care providers' troubled conscience in residential care for older people. The contribution to participatory action research practice in our studies is a support to the participatory action research process through using a modified model of problem processing, an approach which we found fruitful. In the paper, we describe our experiences and discuss them in relation to relevant literature and theory. Our experiences are that in participatory action research it is crucial to build a trusting relationship and striving to create a fruitful dialogue between the researchers and the participants. In our studies, we found that participatory action research is an easy approach to adapt as a problem-solving process in clinical practice and in nursing research.
Introduction
According to Aldén (2002), conscience may be viewed as central to a human being and to have important tasks. Studies have shown that conscience can be an asset that helps healthcare personnel to provide what is perceived to be good care (Dahlqvist et al., 2007; Juthberg, 2008) but also as a burden that can generate stress of conscience, that is, stress generated from troubled conscience (Glasberg, Eriksson, & Norberg, 2007). Healthcare personnel may experience troubled conscience for not providing the quality of care they expect of themselves (e.g. Lindahl, Gilje, Norberg, & Söderberg, 2010; Söderberg, 1999; Sørlie, Kihlgren, & Kihlgren, 2005; Strandberg, 2002). In residential care for older people, troubled conscience is found to be generated when care providers perceived themselves as being caught between different demands, being torn away from residents to other “must do’s”, feeling unable to relieve suffering, and being part of providing care that is or feels wrong (Ericson-Lidman, Norberg, Persson, & Strandberg, 2013). Perceptions of not doing a good job, time pressures and difficult priorities in daily work have been described as generating troubled conscience in care providers working in residential care for older people with dementia diseases (Ericson-Lidman, Franklin-Larsson, & Norberg, 2014). High levels of stress of conscience have been found to be associated with health complaints (Orrung Wallin, Jakobsson, & Edberg, 2013), emotional exhaustion and depersonalization, i.e. the core dimensions of burnout (Åhlin, Ericson-Lidman, Eriksson, Norberg, & Strandberg, 2013; Glasberg et al., 2006), and negatively associated with care quality in care of older people (From, 2011). Stress of conscience seems to seriously affect the quality of care and the well-being of the care providers. It is therefore of great importance to take measures to address, and relieve but preferably prevent stress related to troubled conscience. In order to make an attempt to do so, we have used participatory action research (PAR) in clinical practice, supported with a modified model of problem processing inspired by problem-based learning (PBL), which is a way of self-directed learning (e.g. Silén, 2004) (see Figure 1). Our self-location as change agents is based on democracy, self-directed and lifelong learning, mutual respect and confidence. We have been professional active as registered nurses in care for older people, psychiatric care, surgical care and primary health care. As researchers we have focused on phenomenon such as troubled conscience, stress related to troubled conscience, burnout, support, inner strength, comfort and quality of care. Participants in focus of our research are care providers, residents and relatives but also managers and politicians.
Model of problem processing.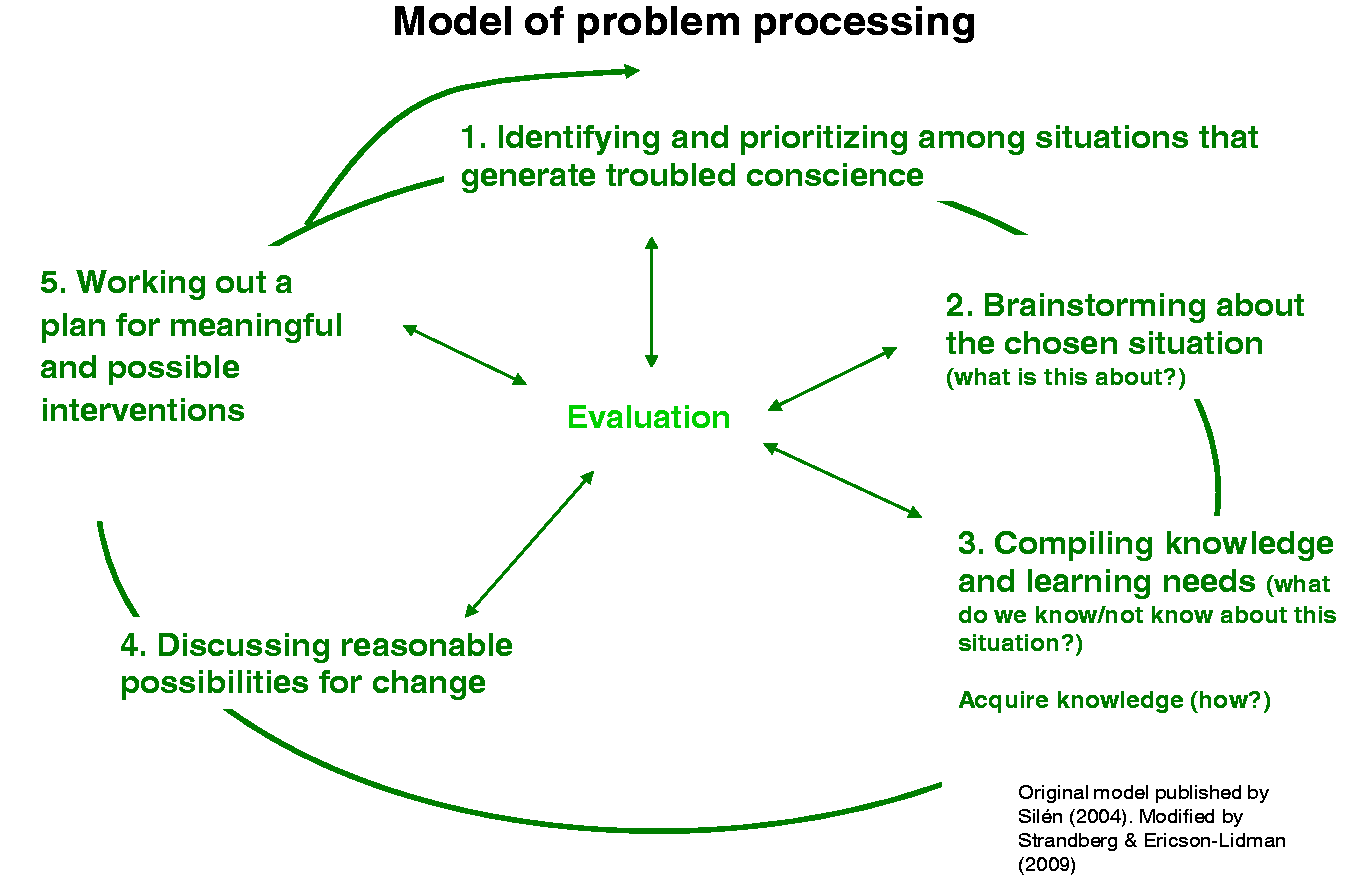
In our intervention project, we have used PAR supported by a model of problem processing to help care providers working in the residential care of older people and their managers to deal with troubled conscience and use it as a driving force to provide good care. As we have found our interventions as helpful for care providers and their managers, that is, their troubled conscience was relieved, we would like to share and discuss our experiences, both theoretical and practical. Hopefully this will inspire organizations to implement PAR as a problem-solving process in order to increase the quality of care and prevent work-related illnesses.
A description of PAR
PAR uses the knowledge and experiences of the participants (Elden, 1981). PAR puts an emphasis on collaboration and strive to engage subjects and researchers as equals in the process, wherein together the subjects have chosen the problem in focus (Stringer, 2014). The aim of PAR is to bring about change and participation among people with common interests and shared experiences. Collaboration with research participants as co-researchers is in focus. Through the process, the participants become empowered to specify their own problems and to consider solutions (Gillis & Jackson, 2002), which means that they are considered experts on their own needs and desires (Quixley, 2008). The process of PAR is often described in proper terms. However, the stages in this process overlap each other, and introductory plans are quickly becoming outdated when learning from experience (Kemmis & McTaggart, 2008).
The PAR process has been described in three phases; look, think and act (Koch & Kralik, 2006; Stringer, 2014), a systematic and cyclical process. In short, during the look phase, the participants describe a situation. In the think phase, they reflect on the situation, and in the act phase they consider available options of change (Koch & Kralik, 2006). PAR has been shown to be successful in dealing with problematic issues in practice, in both social- and healthcare (Day, Higgins, & Koch, 2009; Ochocka, Janzen, & Nelson, 2002; Robichaux & Parsons, 2009). Studies with PAR design have been found to be the optimal designs for decreasing occupational stress on both a group and organizational level (Svensson Dalgren & Gard, 2009). PAR is often depicted as a process of learning (e.g. Koch & Kralik, 2006), and to have a learner-centered approach (Millwood et al., 2013) Our PAR studies are based on an intention to “understand the world as it is, to understand the fundamental nature of the social world at the level of subjective experience” (Burrell & Morgan, 1979, p. 28). To achieve change, we agree with the opinion that it is of vital importance for the PAR researcher to focus on the participants' perspective and to interact with them to understand their world and thoughts (cf. Pajalic & Westergren, 2013). Action research has during the years been framed to fit the study situation instead of following a template (Dick, 2009). In this study, the “model of problem processing” described below was considered to support the PAR process, thus be helpful in order to concretize situations wherein dealing with troubled conscience were in focus. Except from our own intervention studies presented in this study, research on learning to deal with troubled conscience through PAR has not been found in database searches. The aim with this paper is to present our experiences of using a further developed PAR process in practice to deal with care providers' troubled conscience in residential care for older people.
A description of our interventions in residential care
Our studies were performed at a municipal residential care facility for older people which was randomly chosen (from a total of 21 comparable residences, that is, with same mode of operation and same care level) to participate in the intervention. The facility was located in a medium-sized town in a municipal in northern Sweden and was divided into four units; all were included in the intervention. The 50 residents who lived in the units were between 80 and 95 years old, had extensive disabilities and multi-morbidities, and suffered from dementia disease with different levels of functioning. The facility provided 24-hour care and enrolled nurses (ENs) and nurse assistants (NAs) were the principal staff. Registered nurses (available during daytime on weekdays) were employed on a consultative basis, together with occupational therapists and physiotherapists. The intervention was carried out during two consecutive years with two units each year (finished 2012). We (the researchers) met the care providers monthly for one year and each meeting lasted 90 minutes. In total, 44 care providers (ENs and NAs) and two managers participated in the intervention sessions. From this point, we will refer to care providers and their managers as “participants”. The studies were carried out in collaboration with the municipal department of the care for older people. We have structured and compiled our experiences from all our studies. After every session, we systematically summarized the session together with the participants: the group process, the work process and the learning process. These dialogues were regularly written down as field notes and used in this manuscript to compile our experiences and to draw conclusions. Our experiences are reflected on in the light of relevant literature and theory.
An overall aim of our four PAR studies (Ericson-Lidman & Strandberg, 2013a, 2013b, 2015a, 2015b) was to assist care providers in residential municipal care of older people to constructively deal with their troubled conscience generated from various challenging situations. As a start, we interviewed all participants in the facility, which was divided into four units, individually about what they perceived generated troubled conscience in their daily work. The result was then presented for the participants at each unit and together they prioritized what situation they wanted to process. In one unit they decided to work with their shortcomings and troubled conscience for not providing sufficient activities for residents. Through sharing experiences with each other, care providers raised their awareness of what types of activities that were meaningful for the residents. They also could confirm one another about meaningful activities and, actions were taken to implement such activities, which was found to be satisfying to the residents and at the same time eased the care providers’ troubled conscience (Ericson-Lidman & Strandberg, 2013b). At another unit, a challenging situation was chosen by care providers as they perceived shortcomings in providing an individualized meal schedule and a lack of opportunities for meaningful interventions. We, the researchers in PAR, became the bridge between the care providers and the management that was needed to improve individualized mealtime schedule and thus ease their troubled conscience (Ericson-Lidman & Strandberg, 2015b). A third unit chose a challenging situation in how to deal with a resident with spitting behavior as they felt insufficient and had troubled conscience when caring for him. Through the PAR process the care providers found strategies for dealing with the behavior, it was for example easier to cope with the behavioral symptom if it was perceived unintentional (Ericson-Lidman & Strandberg, 2013a). A fourth challenging situation chosen was deficient teamwork. During the PAR-process, participants raised their awareness of the need to view the team in a wider sense than they had done before to improve team outcome (Ericson-Lidman & Strandberg, 2015a). In all the four studies described above, care providers used their troubled conscience as a driving force in order to find meaningful actions throughout the PAR process. A quantitative follow-up study to evaluate our four PAR studies was performed 6 months after the intervention was ended, see section “Reflections” (Ericson-Lidman & Åhlin, 2015).
Our contribution to further develop the PAR process in practice
Our contribution to PAR practice is that we, as mentioned above, supported the PAR process with a modified model of problem processing inspired by PBL. The model of problem processing was used to clarify the PAR process, which we sometimes found difficult to visualize together with the participants. We have found that using the model of problem processing to support the PAR-process with its theoretical underpinnings, is a fruitful way of visualizing, clarifying and structuring the process to the participants. In both PAR and PBL, reflection and extending one's understanding are central. With its systematic and investigative approach to process problems, PBL is supporting the PAR process. PBL builds on prior knowledge, critical thinking, integration and reflective learning (Maudsley, 1999), concepts that also may be related to the look-, think-, and act-phases in PAR. Prior knowledge is used in PBL to strive for understanding of the problematic situation (Silén, 2004). In the same way, the participants in the look-phase in PAR are striving to offer their different perspectives of the situation (Koch & Kralik, 2006). Critical thinking in PBL means to review and analyze the problematic situation (Silén, 2004), which may also be found in the think phase in PAR wherein the participants are asking questions like; what is happening in this situation and why? (Koch & Kralik, 2006). Integration in PBL is for example about striving to co-understand the problematic situation on different levels (cf. e.g. Maudsley, 1999), which also may be found in the think phase in PAR (Koch & Kralik, 2006). Reflective learning in PBL is built-in in all stages, which is comparable to phases in PAR. In PBL, the outlook on learning and knowledge is associated with a humanity that regards people as actively creative, willing and capable to acquire knowledge and skills (Silén, 2004). PBL is, as mentioned above, a fruitful way of visualizing, clarifying, and structuring the process to the participants. The model of problem processing, with its five steps (see Figure 1), thus contributed to facilitate the problem-solving journey and helped to concretize the challenging situations that generate troubled conscience in daily praxis.
As mentioned above, the stages in the PAR process overlap each other and there is often a need to alternate between steps in the process. To follow the process in a trustworthy way, we audio taped all the intervention sessions, transcribed them and then used domain analysis to sort the text according to stages in PAR, steps in the model of problem processing and in order to present the results clearly and appropriate. A domain analysis is focusing on content areas of importance in a text (cf. Graneheim & Lundman, 2004). We found that this approach is seldom used in PAR and, together with the use of the model of problem processing this might be considered innovative in PAR. Below we elaborate the steps of our model of processing and the use of the model.
Practical description on how we worked to further develop PAR process in practice
The way we used the PAR, with support from the model of problem processing, can be described in following steps (see Figure 1, steps in the figure are marked as italics in the text below):
Step 1. Identifying and prioritizing among situations that the participants in individual interviews (Ericson-Lidman et al., 2013) had described generated troubled conscience in them. The situations were often characterized by the participants’ feelings of inadequacy to uphold quality of care and consisted of different problematic situations. Among these difficult situations, the participants prioritized one situation to start reflecting on. Participants in the various units chose different situations to process; perceived shortcomings about not providing sufficient activities for the residents (Ericson-Lidman & Strandberg, 2013b), deficient teamwork (Ericson-Lidman & Strandberg, 2015a), behavioral symptoms (Ericson-Lidman & Strandberg, 2013a), and deficient mealtime schedule (Ericson-Lidman & Strandberg, 2015b). In our qualitative follow-up study performed 2–4 months after the intervention was ended, one participant described step 1 as follows: “We never have time to sit all together and talk. Yes, you run into someone every now and then and you exchange a few words. Now the entire team has been able to sit and talk about things [that troubled their conscience].” (Juthberg & Ericson-Lidman, 2015, p. 8).
Step 2. During brainstorming, the participants discussed and analyzed the chosen situation from different perspectives. It was important that every participant was given the opportunity to speak as freely about their views of the situation. Our experience is that it is of great importance to dare to remain in the steps of analysis, especially the second step. We also found it necessary to go back to step 2 when there was an incongruence with interpreting and tackling the present problem. For example, when dealing with perceived shortcomings about not providing sufficient activities for the residents, the participants brainstormed about what kind of activities they did/did not provide, and wished to provide from the residents’ needs. It took a while before the picture became clear, therefore they needed to go back and discuss what the situation was about (Ericson-Lidman & Strandberg, 2013b). One participant described step 2 as follows; “We thought we acted wrong when we created activities out of our resident’s condition and personally wishes and not according to rules and recommendations, after talking it through we now know that we acted right”.
Step 3. Then they compiled their knowledge and their learning needs about the challenging situation; together they described what they knew and what they did not knew about the situation. Together they decided if gathering knowledge was important and how to do this. In our studies, the most common way to gain further knowledge was provided by the involved researchers, but also from outside sources. For instance, when the challenging situation had to do with perceived shortcomings in managing behavioral symptoms, the participants decided to involve a “dementia-team” (Ericson-Lidman & Strandberg, 2013a). One participant described their needs as follows; "We don't know much about this kind of challenging situations, what we know is that we are feeling inadequate to deal with it”.
Step 4. When knowledge was provided, a discussion about the reasonable possibilities for change started. These possibilities for change were grounded in the participants’ prior knowledge and their gained knowledge about the problematic situation. With newly gained knowledge, a need to go back to step 2 occurred occasionally. For example, when they processed about their troubled conscience generated from perceived shortcoming of managing behavioral symptoms, the participants discovered a need to observe the situations which one of the researchers did. With help from these observational notes the participants discovered that the problem “per se” was unsolvable but possible to relate to (Ericson-Lidman & Strandberg, 2013a). One participant described this new insight as follows; “It feels horrible to read this observational notes, it become so obvious that we can't do anything else but relate to the situation”.
Step 5. A plan for meaningful and possible interventions was worked out and managed. The participants worked according to the plan, that is, they stage-managed the changes, until the next intervention meeting when the plan was evaluated and occasionally revised or a new plan was worked out. In this step, there was also a need to revisit step 2 on occasion. Every PAR session began with feedback and reflection on the previous session in order to uphold congruence in participants’ and researchers’ interpretations. Evaluation took place throughout the whole intervention process. For example, when dealing with perceived shortcomings about not providing sufficient activities for the residents, they started to perform activities and evaluate the results from the residents’ perspective; they observed the residents’ reactions and asked them about their feelings (Ericson-Lidman & Strandberg, 2013b). One participant described the situation as follows; “It is important to closely observe the reaction of the resident, does he or she seem content with the activity?”
Reflections
We will reflect on our experiences of using a further developed PAR process in practice in relation to conscience as a driving force to deal with care providers' troubled conscience, working with PAR together with “model of problem processing”, own thoughts about challenges and important issues when working with PAR, and finally our own role as PAR researchers.
As mentioned above, we have in our PAR studies used troubled conscience as a driving force to relieve care providers’ burden and to increase quality of care (Ericson-Lidman & Strandberg, 2013a, 2013b, 2015a, 2015b). Findings from all of our four published studies reveal the necessity for care providers to listen to their conscience, to express and interpret its message both personally and as part of a team, to make conscience a driving force and an asset possible to follow in their daily work (Ericson-Lidman & Strandberg, 2013a, 2013b, 2015a, 2015b). Conscience refers to something fundamentally social and sharable (Brown, 1996), and can be regarded as central to a person (Aldén, 2002). Our conscience is too important to ignore (Birchley, 2011) and therefore needs to be respected (Broeckaert, 2011), enlightened, informed, and educated together with others (cf. Ratzinger, 2007). Care providers often lack a voice in healthcare research (Northway, 2010a), and through PAR their voices are being heard. They have very important things to teach researchers about their daily working life. This knowledge may be used to increase quality of care and prevent work related ill-health, just as our studies intended.
Our experience is that the problems that were processed during the PAR sessions belonged to different levels in the participants’ daily work. We processed problems from the first person perspective, such as “what can I do in this situation?” We also processed problems from the second person perspective, that is, “what can we do together as a team in this situation”? Finally, we also processed problems from a third person perspective, that is, “what can the organization contribute with”? We found it fruitful to raise participants' awareness about these levels to create realistic expectations of their problem-solving and direct issues related to the organization level to deal with these. This awareness, about that some issues were beyond their power to change, could relieve the participants' troubled conscience in some situations.
The model of problem processing (see Figure 1) made it possible to give structure to the PAR process by helping us to keep track of where in the process we found ourselves. We felt that the participants needed time to understand their role as co-researchers and to understand the cycles of PAR. During the first group sessions, we carefully described and explained the cycles of PAR with help of the figure, to increase the participants' feelings of involvement and safety. Therefore, during our first session and continuously afterwards, we explored the participants’ expectations of the process (cf. Bevan, 2013), and later on, when discussions had been lively and had went on for quite some time this was particularly helpful. The figure could easily be shown and it visualized where we were and where we were heading. Every session also started with feedback on the previous session and the participants were given the opportunity to comment on or clarify any issues and if needed the figure was shown. The participants often started the session with statements like; “We, both individually and together, have been pondering a lot since the last session”. It was then natural for us to reflect on the last session together with the participants, reflections that made an important starting point to the session for the day. We also found it important to help the participants in recognizing PAR as an approach that could be used in their day-to-day work when they are facing challenging situations that generate troubled conscience. The figure gave structure to the process and it was easy to understand.
An ethical issue in action research is that the participants are giving their consent for participation to unknown challenges (cf. Meyer, 1993, 2000). A safe and supportive meeting environment could be jeopardized as it is difficult to predict what issues that will be raised during the PAR sessions (Koch & Kralik, 2006). Our project started, as mentioned above, with individual interviews wherein the participants narrated about challenging situations that generated troubled conscience in them, and during the first session they were given the opportunity, as a group, to prioritize one of these situations. Reasonably, some of the participants would have chosen another situation if they had the opportunity to choose themselves. It was also sometimes a challenge to “get everybody on the train”, that is, to get everybody interested in the area of discussion. To increase the interest of the area we inspired and motivated the group to discuss the importance of processing the challenging situation and the risk of not doing so. In our qualitative follow-up study, some participants described that the topics discussed not always were of their concern (Juthberg & Ericson-Lidman, 2015). However, we consider it to be a crucial first step for the PAR group to agree on what area to process. It may be tempting to process many challenging situations at the same time in order to relieve the participants’ troubled conscience. However, our experience is that in order to keep focus and not to lose sight, you must not process more than two situations at the same time. This was also confirmed by participants who described that the researchers structured the sessions and kept the discussion to the area chosen by the group (Juthberg & Ericson-Lidman, 2015). Structuring the sessions was possible through using the model of problem processing. The model also made it possible to keep the discussion to the area chosen.
In PAR, the participants are regarded as co-researchers (e.g. Gillis & Jackson, 2002). We found it therefore important to clarify from the start that all participants had an equal say in the process. Our experience is that the manager should be a “front person” to create equality in a safe and open climate when working with PAR. The sessions were sanctioned by the manager who also participated in the process, a collaboration that in fact meant success (cf. Ericson-Lidman & Strandberg, 2015a). In our quantitative follow-up study, care providers scored significantly higher on the question “Are your work achievements appreciated by your immediate superior?” 6 months after our intervention (Ericson-Lidman & Åhlin, 2015).
It is important to apply strategies to ensure that the participants feel supported and respected (Guba & Lincoln, 1989), e.g. by ensuring them of their competencies (Wimpenny, 2010). We were careful with clarifying and emphasizing their role as co-researchers and the need of their competence in order to be able to perform the intervention and that everybody's competence and knowledge is of equal importance. In some occasions, it was a challenge to make everybody talk—or to create an atmosphere that stimulates and motivates everyone to talk, and wait for the participants who needed time to express themselves. In our follow-up study, participants described the sessions as a time for ventilation, an opportunity to speak freely about anything and they perceived that others also felt free to do so, even workmates who usually did not talk (Juthberg & Ericson-Lidman, 2015).
The participants in our studies had known each other for several years, but they did not know us. According to Savage et al. (2006), building a trustful relationship between the researchers and the participants is very important in the PAR process. Montero (2000) wrote that PAR assumes “the capacity to accept the Other in its full distinctiveness, in its full difference”. By accepting the Otherness, the full possibility of a dialogue is created, an essential condition for PAR (p. 135). Also essential to PAR is creating an environment that promotes learning, therefore it is of great importance to strive for a safe and inclusive atmosphere in the group sessions—a responsibility for the researchers. In order to build trust and to uphold the power balance, it is also important for the researchers to carefully consider their use of language (cf. Savage et al., 2006), and therefore avoid academic language and arcane technical terms.
PAR researchers may have to relate to participants who have louder voices than others (Koch & Kralik, 2006), but we discovered that relating to participants who keep quiet also can be a challenge. Therefore as a PAR researcher it is important to be aware of the power balance in the group (Löfman, Pelkonen, & Pietilä, 2004), and to uphold democracy (Kidd & Kral, 2005). In our follow-up study, the participants in one unit described that conflicts in the team made them sometimes to keep quiet about their viewpoints during the sessions (Juthberg & Ericson-Lidman, 2015), a fact that reveals that group processes, imperceptible to the researchers, may be ongoing. As a PAR researcher, it is of great importance to always be aware of the group processes. In order to observe the group process, we were listening actively and carefully to what was said, but also to the unsaid.
As researchers in PAR, we also found that it was important to continuously reflect, not only on the process, but also on our own role (cf. Northway, 2010b). Experiences of being a PAR researcher is described as balancing on a slack rope in a world of compromises. The role of the researcher means to be a guest in the activity, striving to cope with the lack of control and challenges when various perspectives come together (Edberg, 2013). After the PAR sessions, we often talked about that we were “walking on thin ice”, and that we did not always have control over what was happening in the group and what we “were going into” or face in the next sessions. This uncertainty is often a part of the PAR process and can surely be perceived as worrying as a researcher. However, working with PAR is a discovery journey, and striving for control could certainly end the journey, and make it pointless.
During our PAR project, we discovered that being a PAR researcher means to be ready to put aside many of one’s presumptions and beliefs of how research is going to be conducted. According to Northway (2010b), researchers have traditionally taken an objective and detached role in the research process, which is clearly different in PAR. Changing the balance of power is central to a PAR researcher. Traditional research often views the researchers as experts while viewing participants as passive subjects with no regard for their experience and knowledge, a starting point which has been changed through PAR. As we have experienced it in practice, it is crucial to have trust in each other, respect for each other’s knowledge, and last but not least, have a willingness to learn from each other in order to obtain well-functioning PAR.
Validity and reliability in PAR
PAR is criticized for lacking scientific rigor (Kemmis & McTaggart, 2000), which suggest that some of the existing definitions are not clear enough, which may contribute to an unclear understanding of the concept (Cronholm & Goldkuhl, 2004). Critics also argue that the statement about PAR as empowering, liberating and emancipatory are false promises (McTaggart, 1994). In order to uphold PAR as quality research, it is crucial to carefully describe the process and to discuss validity and reliability. As PAR may be regarded as a qualitative approach (Dick, 1999), almost the same demands for validity are current (Waterman, 1998). In PAR, the participants are part of the validation process through validating the findings in the cycles of reflection and action, a fact that it is important to clarify and overall visualize for a reader (Koch & Kralik, 2006), and a fact that we found to be unique in the research approaches, but also questionable. To achieve an objective description of the validation process, and to evaluate the work-, learning-, and group processes, individual follow-up interviews with the participants were performed by an outside researcher 2–4 months after the intervention was ended (Juthberg & Ericson-Lidman, 2015). To strive toward credibility, it is important to show that participants’ voices are represented adequately, e.g. by quotations (Koch & Kralik, 2006). In order to judge transferability, the context and participants’ profile must be described adequately. Dependability may be judged through enabling the research process to be audited by a reader (Koch & Kralik, 2006; Stringer, 2014). It is therefore important to carefully describe the process of analysis to enable a reader to judge if the interpretations are grounded in the data.
As a researcher in PAR, it is important to be aware of one's worldview, as it drives the PAR processes (Koch & Kralik, 2006). Therefore, it is both usual but also important to present one’s worldview so a reader can make judgments of the trustworthiness. Our worldview is based on the values of democracy, learning for personal development, and equality, which are values consistent with Koch and Kralik (2006). In order to increase rigor and trustworthiness, developing mutually trusting relationships and being open to communication is crucial to achieve high-quality outcomes (Lennie, 2006). We strived to sustain an open way of communicating in the group and that everyone’s voice should be heard.
Concluding comment
The ultimate goal with participatory research is to create permanent change in the activities involved (Edberg, 2013). Our viewpoint is that PAR together with PBL is an easy approach to adapt as a problem-solving process in residential care for older people. In our project, troubled conscience was the focus, but PAR may also be used to process other problematic areas. However, it must be underlined that there are no PAR-cookbook approaches to follow as PAR can take on various forms (Hall, 1992). In order to manage sustainable change, participants crucially need “to maintain approaches to development that engage the participatory processes and foster a sense of community among all participants”. This change takes time, resources and planning is needed in both scheduling and budgeting (Stringer, 2014, p. 189). We have found PAR to be a rewarding approach which reveals knowledge and understanding which is impossible to reach with other research approaches (cf. Bevan, 2013).
Implications for practice
This paper provides a description of a PAR process combined with a model of problem processing that should be considered to be useful as an approach in clinical practice, in nursing research, and transferred into other areas that is benefitted by bringing together action and reflection, theory and practice in order to develop organizations as well as prevent work-related illnesses. We have found that PAR together with a model of problem processing is successful in relieving troubled conscience among care providers and in upholding quality of care in residential care for older people. However, based on our experiences we consider PAR also to be useful in other contexts wherein troubled conscience may be experienced. One challenge with PAR, according to our experiences and the experiences of others, is that building trust and safety in the PAR group is essential for creating a learning environment during the process. Therefore, it seems reasonable that, especially in the beginning of the process, to put an emphasis on building relationships in the PAR group. As PAR has been questioned as a research approach (see Kemmis & Taggart, 2000), it is important to emphasize that the participants are constantly participating in the validation process, a fact that we find as a valuable and unique research approach. As mentioned above, questions have been raised whether PAR is research or if it is organizational development. Rather than distinguish research from development of organizations, PAR may be considered as research that may develop an organization. For a researcher in PAR, it is important to constantly reflect on one's role as an equal in the process and consider how to uphold equality. It is also important to be aware that being in control of the research process in PAR is neither possible, nor desirable.
In our studies, a number of 44 care providers and 2 managers participated. The transferability of the studies is up to a reader to judge, however, it is reasonable to assume that the findings in our studies may be valid in other similar contexts of residential care for older people, also in other countries. In order to strive for validity and reliability, the model of problem processing needs to be further tested and refined in future PAR studies. Aside from the description of our PAR project, this paper highlights challenges, important issues, validity and reliability when using PAR together with our reflections on the role of the researchers, which PAR researchers should find beneficial.
Footnotes
Acknowledgements
The authors would like to thank their research colleagues in the “Stress of Conscience Study”, especially Professor Emerita Astrid Norberg who contributed with valuable suggestions.
Author contributions
Both authors have contributed to the study design, writings, and drafting of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Swedish Council for Working Life and Social Research (FAS, Forte) 2010-0296. The Swedish Research Council (VR) K2011-70X-21823-01-3 AFA Insurance 090136