
Abstract
Background
The ambulance service provides emergency care to meet the patient’s medical and nursing needs. Based on professional nursing values, this should be done within a caring relationship with a holistic approach as the opposite would risk suffering related to disengagement from the patient’s emotional and existential needs. However, knowledge is sparse on how ambulance personnel can meet caring needs and avoid suffering, particularly in conjunction with urgent and emergency situations.
Aim
The aim of the study was to explore ambulance nurses’ experiences of relationships with patients in urgent and emergency situations.
Methods
Data collection was performed using individual open-ended interviews with six ambulance nurses. The data were analyzed using a thematic analysis.
Results
Relationships with patients during urgent and emergency assignments emerged as three themes: “Ambiguous silence,” “Professional competence” and “Challenging inadequacy” comprising eight sub-themes in total. The result shows that the ambulance nurses found it difficult to prioritize between medical care and establishing a caring relationship with the patient. However, sometimes a wordless relationship was perceived sufficient and considered a first step towards a verbal relationship.
Conclusions
Ambulance nurses experience that a caring relationship cannot and does not need to be prioritized in the acute stage. This uncovers a dichotomy approach to medical care versus caring relationships that exclude a holistic approach. Thus, patients’ emotional, existential and physical needs are not considered as equally important.
Keywords
Introduction
The ambulance service, as part of the emergency medical services (EMS), provides emergency care to patients with a variety of conditions, problems and needs. In Sweden, with 10.1 million inhabitants, the medical dispatch centers handled 1.2 million ambulance assignments in 2016 and 41% of those were given the highest priority, i.e. acute life threatening conditions or accidents. 1 Hence, ambulance personnel handle emergency assignments on a daily basis, such as patients exposed to trauma or with emergency medical conditions.2,3 This requires rapid assessment, decision and transport to different hospital care units. 4
Background
The care of the patient in the EMS is often based on guidelines and protocols to secure a proper assessment of the patient’s vital functions. However, before encountering the patient, preparations are also required for the unexpected and unknown, while the initial assessment may rapidly be changed at the scene according to the patient’s condition. 5
The assessment is normally conducted using the Airway, Breathing, Circulation, Disability and Exposure (ABCDE) procedure. 6 First, life-threatening airway problems must be assessed and treated before moving to life-threatening breathing problems and so on. Second, this structured approach helps to quickly identify life-threating problems, which lead to the initiation of emergency treatment. The primary goal is to keep the patient alive and achieve clinical improvement before further treatment and diagnoses are decided at the hospital. 7
The prehospital care environment is unpredictable and the security of personnel has to be assured. The ambulance personnel have to take control of a situation guided by the specific preconditions that exist, in order to establish a safe environment for the patient and themselves, and to make complex decisions about emergency department conveyance or specialist emergency pathways.8,9 Simultaneously they have to consider the relationship with the patient as this has been found to be an important, fundamental and ethical aspect of care. Patients describe the relationship with ambulance personnel as being dependent which demands both technical knowledge and relational skills.10,11
Relationships are described as fundamental and the core in nursing care, founded in the encounter with the patient. 12 While preserving human dignity, wholeness and integrity this relationship is suggested to be labeled a caring relationship. 13 This is described as being potentially life-changing when the caregiver is someone whom the patient relies on. 14 Further, having the time to get to know patients and to meet their needs is described as a prerequisite to a nurse–patient relationship. During urgent and emergency ambulance assignments, the time to get to know the patient may be limited, but on the other hand the presence of ambulance personnel itself may be seen as a compassionate exchange of human experience in the nurse–patient relationship. 15 Uncaring encounters in emergency departments are found to affect the patient’s wellbeing while caring for trauma patients. Registered nurses (RNs) have become personally distanced and focused on medical technical equipment and thereby disengaged from the patients’ emotional needs, which may be understood as an ethical problem. 16 In addition this contrasts the understanding of patients’ suffering as simultaneously physical, psychological and existential. 17 In this the nurse–patient relationship is described as necessary in order to soothe patients’ suffering. 12 Consequently, to focus only on medical needs and treatment, thereby in the relationship not responding to all dimensions of the patient’s suffering, may increase that suffering.
In conclusion, ambulance nurses face unpredictable situations and multi-dimensional suffering when caring for critically ill/injured patients, requiring the ability to assess and provide advanced medical care, and at the same time establish a caring relationship, taking the patient’s dignity, integrity and wholeness into account. In contrast, distance and disengagement from the patient’s emotional and existential needs in emergency situations may result in extended suffering, as a result of a fragmentary perspective on the patient. 18 Ambulance nurses’ experiences of care relationships during urgent and emergency assignments may contribute with important knowledge as to how inflicted suffering can be mitigated, serving as a foundation for further research in this field. Hence, the aim of the study was to explore ambulance nurses’ experiences of relationships with patients in urgent and emergency situations.
Methods
Design
In line with the aim, an explorative qualitative design, using open-ended individual qualitative interviews, was chosen. 19 The data were analyzed using inductive thematic analysis. 20
Setting
In Sweden, the ambulance service comprises a system of advanced life support (ALS) units with at least one RN in each ALS ambulance. The proportion of paramedics varies between 15% and 35% of the total Swedish EMS staff. The rest of the EMS staff consists of RNs. The proportion of RNs who are specialist trained in ambulance care varies considerably between EMS organizations and represents 20–80% of the total Swedish EMS nursing staff. Ambulance nurses and other specialist nurses (e.g. in anesthetic or intensive care) have four years of university training, with three years to qualify as an RN and one year for specialization. Paramedics usually have two years of high school training as assistant nurses and about one year of EMS education. The RNs have the overall responsibility for assessing and caring for the patient, unlike the paramedics. This study was conducted in one EMS organization in western Sweden, a region of 23,797 square kilometers with 1.65 million inhabitants (69 inhabitants/km2). The regional EMS has 123 ambulance units located at 47 stations. 1
Data collection
Data collection from open-ended individual interviews was conducted during spring 2016. In total six ambulance nurses were included using a purposive sampling. 21 The EMS manager approved the study. The inclusion criteria were: (1) at least two years of experience of EMS prehospital care and (2) one-year specialist-education in ambulance care. Firstly, the inclusions criteria were judged to cover a sufficient amount of clinical experiences of urgent and emergency care assignments. Secondly, specialist trained ambulance nurses were judged to have deepened theoretical knowledge covering ethical aspects of patient relationships. The ambulance nurses received a letter informing them of the study’s aim and procedures. Personal contact was established with six potential participants after one week, asking them if they would be willing to participate in the study. All agreed to participate. Five of the participants were women, and their age varied between 36 and 44 years. The ambulance nurses’ experiences of working in the EMS varied between 2 and 20 years. All open-ended interviews were conducted one-to-one away from the workplace by the first author. The interviewer initially encouraged the participants to reflect upon and define their experiences of good relationships with patients in urgent and emergency situations. 19 The interviews were held in Swedish and introduced with the question; “Can you tell me about a good relationship with a patient?” Follow-up questions were posed where necessary to probe and thereby deepen understanding; “Can you describe how you establish a good relationship with a critically ill patient during emergency assignments?” or “Can you tell me about challenges occurring during urgent and emergency assignments?” Each interview was digitally recorded and lasted between 30 and 60 minutes.
Analysis
The interviews were carefully transcribed verbatim, in order not to alter the original data, and read through several times by the authors in order to get a sense of the whole. Meaning-units were extracted from the text, condensed, abstracted into codes and merged thematically. 20 The relationships between themes were then identified through constant circular comparison of the transcripts, meaning-units and codes (Figure 1) until the formulated themes were judged to comprise internal homogeneity and external heterogeneity. The codes and their applications were reviewed along with the suggested alternative interpretations until consensus was reached among all authors about the interpretation that best fit the data. Quotations were used in order to clarify the described sub-themes. The analysis was undertaken in Swedish and subsequently translated to English. The reliability of the translation of the themes was constantly validated in an ongoing critical discussion between all authors about different possible translations in relation to data and formulated themes. Finally, a professional language review was performed and followed by the same critical authors’ discussion.

The analysis process.
Ethical considerations
The study was carried out in accordance with the Declaration of Helsinki. 22 According to Swedish law ethical approval is not required for this type of study. 23 However, the study underwent a peer ethical review in advance. The participants received both written and verbal information prior to the study. They had the opportunity to ask questions and signed an informed consent before the interviews started. The interviews were coded to protect the participants’ identities, and only the first author had access to the code-key. Quotations have been labelled with the interview number in order to protect the participants’ anonymity.
Results
Relationships with patients during urgent and emergency assignments in the EMS are described in three themes; “Ambiguous silence,” “Professional competence” and “Challenging inadequacy” and comprise seven sub-themes in total (Figure 2).
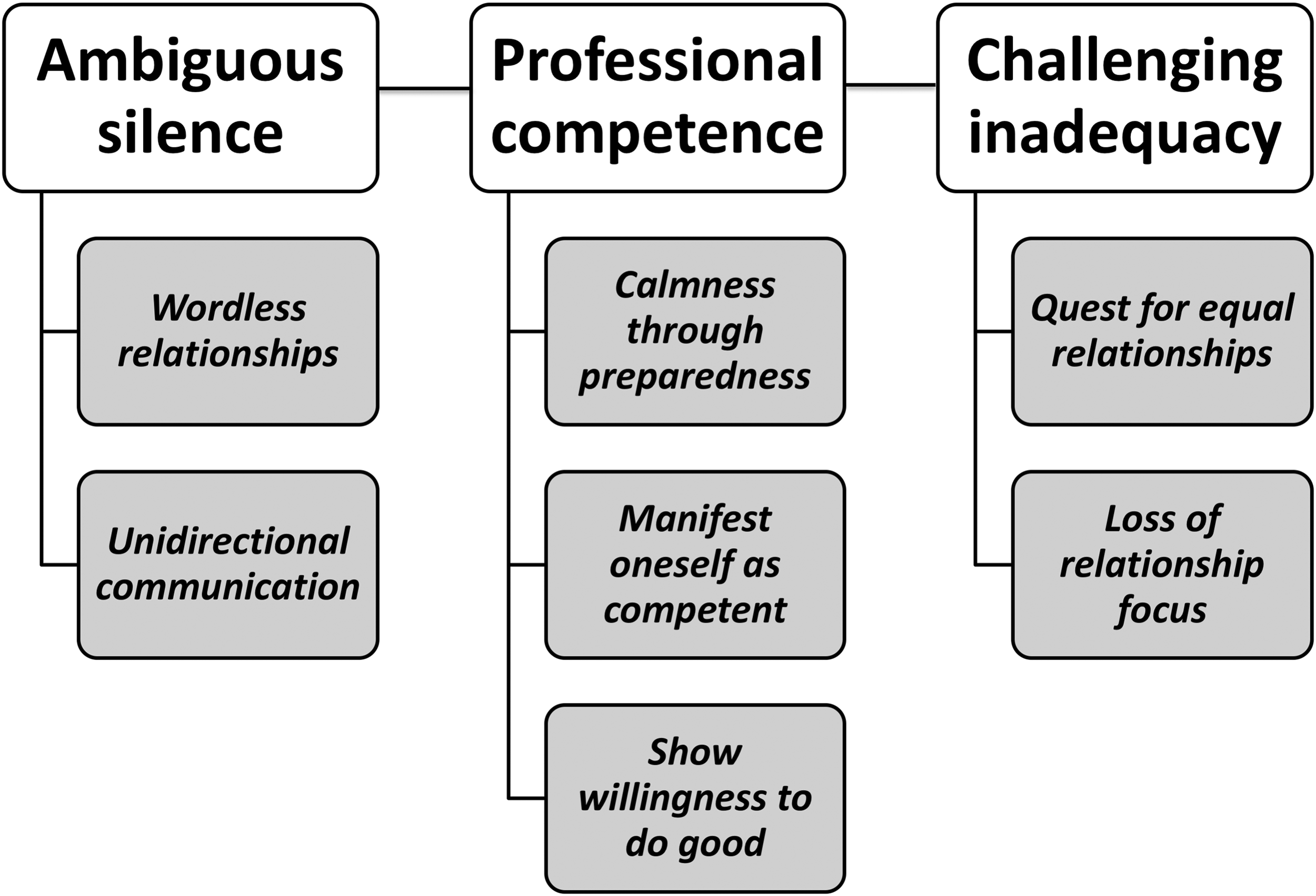
Themes and sub-themes.
Theme: Ambiguous silence
The relationship between the nurse and the patient is often characterized by an ambiguous silence. A good initial encounter is perceived as dependent on the patient feeling secure and cared for, which is established in dialogue, through unidirectional communication or without words or conversation.
Sub-theme: Wordless relationships
Sometimes a relationship with the patient is created without any verbal communication. It is not always necessary to use verbal communication to establish a relationship. The patient could also be perceived not to want any verbal relationship. In these situations, eye contact with the patient is a way of establishing a relationship. Physical touch is one important aspect of the relationship with the patient. I had one patient who actually said it when we drove him: “Thank you for touching me” … I thought that was all he needed, and nothing more … We talked no more at all the rest of the way. (Interview 5)
Sub-theme: Unidirectional communication
Communication is considered important for creating relationships. In some situations it is impossible to communicate verbally, for example when the patient is unconscious. In these situations, verbal information is given to comfort the patient regardless of whether the patient is unconscious or awake. Providing information about medical treatment and assessments is perceived as to create a good relationship and to promote a sense of security. However, during these assignments the time for this is short. Hence, creating a sense of security in a short time frame is essential. My experience of creating a relationship is to communicate with the patient all the time. For example, telling the patient “I’m sitting right here next to you, I’m about to do this now” or “We are going to the hospital.” To provide continuous information, even though the patient might be critically ill, so that the patient feels that you are there for them all the time. (Interview 1)
Theme: Professional competence
Being professional is described as using medical knowledge and experienced as an essential aspect of patient relationships. Being prepared and being secure in the professional role helped the nurses to remain calm and in control. This is also a prerequisite for being able to manifest oneself as competent and to provide security for the patient.
Sub-theme: Calmness through preparedness
Experience gained in the EMS helps to make it easier to create a relationship with the patient. Stress is reduced when confidence in one’s professional role is combined with experience in the EMS. There is a need to show professionalism by using medical knowledge and to appear professional in the eyes of the patient. It is perceived that the main reason for calling an ambulance is the nurses’ ability to provide medical care. Well, that’s why they called for us; to be able to help out. I’ve worked in the ambulance service for a long time and I’m always very calm. I rarely get stressed. When you’ve worked for as long as I have, you establish an inner structure that you follow so the work runs smoothly, the ABCDE structure you know. If you remain calm and do not get stressed, I think that the patient notices that. I think it makes them feel safe. (Interview 2)
Sub-theme: Manifest oneself as competent
To manifest oneself as competent by generating a professional impression is described as working in a structured manner and following formal guidelines to provide proper medical care. If the patient’s condition worsens, there is a need to discuss with a colleague how to adapt medical treatment to the changed situation. In such situations, it is important to do this in a way that ensures that, for the patient, the nurse’s own professional knowledge is never in doubt. It is obviously about the medical care in the first place, we get them to hospital. I feel that it's important to be professional and use our skills instead of sitting there rambling on. That doesn’t improve the patient’s situation (laughs). (Interview 2) Of course, it would have provided a completely different opportunity. Sometimes purely medical assistance is important because of how much more quickly you get the work done./…/But also in a patient relationship, it obviously helps. When it’s a bit calmer then maybe one of you can sit and talk in a little more detail with the patient about what we are doing. (Interview 3)
Sub-theme: Show willingness to do good
It was perceived as possible to show a willingness to do good and create a relationship, if an open attitude was maintained towards the patient. By trying to create an open initial encounter with the patient helped to form a foundation for developing a good relationship. This was described as essential in order to make the patient feel cared for, and at the same time it was subordinate to efforts to save life. I think a patient in a vulnerable position just wants to be rescued. Of course, they don’t want to be unpleasantly treated. But I think it is enough that the staff, the professionals are caring. That you as a patient know that you will be cared for. Also that there is kindness, plain simple love. Knowing that people wish you well. (Interview 3)
Theme: Challenging inadequacy
There are feelings of inadequacy in the relationship with patients. The focus on providing medical treatment means less focus on the relationship, which is challenging as it means to simultaneously meeting both the patient’s medical and emotional needs. However, when there is time for dialogue it gives nurses the opportunity to explain what medical treatment is necessary and thereby creating a sense of security for the patient.
Sub-theme: Quest for equal relationships
Striving to have a positive attitude towards the patient is considered important, despite any preconceptions there might be about the patient. However, not all patients are approached in the same way. For example, apprehensions about persons who drink and drive negatively influence the nurse’s attitude, causing a lack of willingness to create any relationship at all. Sometimes you’ve spent time at scenes where someone is stood by the side of the car and is drunk and said that someone else was driving. Then the police come over and says that the car is registered to you, but they keep insisting that it was not them who was driving. The same attitude is not adopted to these patients if there is a chance that someone may die. (Interview 5)
Sub-theme: Loss of relationship focus
In challenging situations focus is often lost in striving for a good patient relationship. The challenges are sometimes related to external factors outside one’s control. You have to make phone calls to various hospitals and perhaps get feedback on ECG [electrocardiography] changes and so on, everything takes much longer than you think. It can be difficult to care during high-priority assignments when sometimes the roads are winding and not that smooth, even if you do not drive fast. (Interview 1)
Discussion
In the present study, the ambulance nurses perceived patients in emergency and medically critical situations as having less need of a verbal relationship. In this regard, the results show that a relationship with the patient sometimes may involve just eye contact, physical proximity and touch, i.e. a wordless relationship through human presence. Such presence can be seen as an interpersonal process that includes sensitivity, intimacy and vulnerability.24,25 This presence also has an ethical bearing. It corresponds to Levinas who suggest that within the encounter with the other’s face lies an ethical dimension calling for responsibility that arises before we begin to think about it; it is already there. 26 Presence is thought to involve being close to another person in an intimate way, being empathic, respectful and willing to make efforts in order to adapt to every unique situation. 25 This corresponds to a patient study describing the relationship as “to surrender” when the ambulance personnel arrive, and where their presence represents the ambulance nurses’ knowledge and skills. 10 Patients may experience a promise of help when the ambulance arrives, which is interpreted as a sign of trust for the ambulance personnel’s knowledge and skills, and feeling safe within the relationship when the caregiver understands, supports and trusts them.27,28 These previous research findings correspond to findings in the present study, understanding that a wordless relationship may be of importance in urgent and emergency situations. The wordless relationship might then be experienced as engendering a sense of trust and security through the ambulance nurse’s ability to care both for medical and emotional needs. Overall, our results show that the ambulance nurse has important caring, medical and ethical responsibilities that ought to be combined to shape a holistic care process. However, the ambulance nurses seem to perceive the combination and interweaving as impossible and even unnecessary and that there is a strong dichotomy between medical care and caring relationships, understanding that only one aspect can be prioritized at a time.
The results highlight that ambulance nurses prioritize medical tasks before trying to establish a caring relationship, something that is seen as difficult when focus is on saving the patient’s life. This confirms previous research indicating that emergency care personnel can be emotionally distanced in acute situations.16,29 EMS professionals sometimes choose to make a conscious choice to focus on medical technology when the situation requires a series of complex tasks, and choose not to prioritize establishing a caring relationship. 30 The ambulance nurses in the present study also made a conscious choice not to prioritize a caring relationship but, paradoxically, also experienced a sense of inadequacy when they were unable to do so. Research shows that focusing on medical care increases patient safety and survival at the same time as the medical assessment could benefit from the patient’s subjective experiences.7,31 Getting to know the patient and trying to understand his/her subjective suffering, may change the course of the medical treatment as the patient’s own experience provides important information to supplement objective medical data. Hence, in urgent and emergency situations, it also seems important to find out quickly how the patient experiences the symptoms, condition and situation, as this can help to differentiate non-serious conditions from serious ones. However, the present result is noteworthy from a relation-based ethical perspective as it may exclude the uniqueness of the other resulting in a unidirectional relationship in which the nurse and not the patient is at the center. Buber suggests that this may be the case in teleological based relationships, as a relationship in which the medical treatment and its effect are paramount. 32 In addition it can be understood as an utterance of a context that shapes relationships in a negative way. 33
Thus, a strong focus on medical care only, increases the risk of not paying enough attention to the patient’s existential and emotional needs. This may cause additional suffering to be inflicted by ambulance nurses. This “unnecessary” suffering corresponds to Eriksson’s theory of suffering related to care, meaning that the patient does not experience the care as neither caring nor ethical. 17 This suffering related to care occurs, for example, when the caregiver neither assesses nor acknowledges the emotional needs of the patient. Suffering also appears to be caused by the ambulance nurses’ unawareness of possible consequences of the asymmetric care relationship. This could lead to a loss of focus on the relationship and endanger core ethical values, stated by the Swedish Society of Nursing as respect for patient vulnerability, dignity, integrity and autonomy. 34 This loss of focus in turn risks the patient’s sense of trust, meaning and hope and thereby causing additional suffering. The ambulance nurses’ focus on task-aspects rather than relational aspects, may indicate an ethical paradox between what is good and right and the choice to abstain from what is good and right. On the one hand the ambulance nurse understands the importance of a caring relationship with the patient. On the other hand, in severe and difficult life-threatening situations the relationship is given a low priority where nurses appear to ignore the relational importance, focusing solely on task-aspects. This raises a number of concerns from a nursing and caring perspective, based on the fundamental condition of human existence and core ethical values. Firstly, as the patient’s vulnerability is especially challenged in urgent and emergency situations it is understandable that helping the patient to survive must be prioritized. However, as vulnerability also means fragility, delicacy and exposure to suffering beyond the biological sphere, these situations also require that the relational aspects are handled concurrently. Secondly, in addition to showing concern for the patient, dignity includes respect for the patient’s right to his/her own experiences. However, in the wordless relationships described by the nurses, it seems impossible to understand the patient’s experience and thus make it difficult to meet the patient’s concerns. Thirdly, as integrity means whole and inviolable it can be problematic when the ambulance nurses dichotomize their duties as a matter of either performing emergency medical measures or promoting a caring relationship. Fourth, autonomy includes the patients’ basic rights to receive information to give informed consent to care and treatment. However, in urgent and emergency situations the patient’s ability to be autonomous is often reduced for various reasons. This should not justify ambulance nurses to ignore their responsibility to facilitate patients’ self-determination as much as possible. Acknowledging those core ethical values might contribute to the patient’s experience of trust, meaning and hope and can contribute to relief of suffering and taking responsibility for the patient’s emotional well-being. Thus, from an ethical standpoint the acknowledgement of the other’s uniqueness is paramount in the relationship. However in a medically orientated care, based on an objective perspective on the patient, this may not be the case. 32 Ambulance nurses in the present study stated that the patient’s life was not saved by conversation and, hence, this was not prioritized. This indicates that ambulance nurses may feel compelled to choose between medical care and caring relationships, having to prioritize one of these areas that comprise ethically good care. In addition, this limits the understanding of patient relationships being related only to verbal communication. Hence, emotional distance seems important to provide care in acute assignments. This shows a dichotomy between medical care and caring, which counteracts a holistic approach. Nurse–patient relationships in the EMS setting are described as medically focused and must be understood as a dynamic process and not as something fixed. 35 Hence, the nurse–patient relationship and the medical care must not be understood as two separate responsibilities, but parallel and integrated.
Our results indicate that the ambulance nurses’ understanding of professional competence is not fully in line with core nursing and caring ethical values as stated by the Swedish Society of Nursing. 34 The ambulance nurses in this study state that it is important to act professionally towards both patient and significant others in acute situations, but the meaning of professionalism appears to be limited to being medically competent even in situations where the patient’s life is not threatened. However, professionalism in ambulance care has earlier been found to be more complex than being related to just medical care, also involving for example ethical deliberation and interpersonal communication.30,36 In the present study, the emotional, caring and existential needs of patients may not have been considered as important by the nurses and therefore were not prioritized in urgent and emergency situations. This is of great interest since professional nursing ethical values should be applied in all nursing fields and contexts. Instead, the ambulance nurses experienced that patients in need of emergency medical assistance only wanted to be rescued, i.e. they wanted only medical care. Thus, the relationship is not considered as alleviating the patients’ suffering, which is contradictory to nursing care theories and earlier studies.13,17,37 The results show that professionalism is experienced as the performance, appearance and presentation of medical knowledge and skills exclusively, this being the main reason for the ambulance nurse’s presence at the scene. Thim et al. argue that, by working with systematic medical assessment, patient safety and survival increases. 7 However, providing ethically good care also requires the courage to be affected, having the ability to respond to the patient’s existential needs, reducing his/her suffering.17,38 From this perspective, assessment and care could benefit from the adoption of a non-dualistic holistic approach, being responsive to the patient’s subjective experiences performed in a caring process together with medical treatment.
Methodological discussion
In order to ensure trustworthiness, this study involved all authors in an ongoing discussion until consensus was reached and sub-themes and themes emerged. The authors’ own experience from the prehospital emergency care may have affected both the questions and follow-up questions. However, the aim was to describe the ambulance nurses’ experiences reducing the impact of the authors’ pre-understandings by constantly discussing and questioning each other’s perceptions in the data analysis and other parts of the research process. In addition, the analysis has been the subject of seminars, with the aim of establishing trustworthiness. One limitation in this study may be the low number of participants. However, in line with the aim the number of interviews was judged to contribute with sufficient data in order to thematically explore the ambulance nurses’ experiences. In this regard, six interviews are earlier described as sufficient. 39 In addition, the length of the open-ended interviews is earlier reported as sufficient for in-depth data. 40 The results might be transferrable to other prehospital care settings, accepting the small sample size, through the authors’ efforts to describe the participants, context, data collection and analysis as thoroughly as possible.
Conclusion
The findings suggest that ambulance nurses experience that a caring relationship cannot, and does not need to, be prioritized in the acute stage, taking a dichotomy approach to medical care and caring relationships that exclude a holistic approach. The ambulance nurses’ narratives indicate that being professional is not always in line with the core nursing ethical values. It seems that the meaning of professionalism is limited to being medically competent, while patients’ emotional and existential needs might not be considered as important and therefore not prioritized in urgent and emergency situations.
Taken together this study highlights the question of what contribution specialized ambulance nurses make in the EMS if the interpersonal and medical aspects are not seen as equally important. This is especially interesting as ambulance nurses are educated with a focus on both medical science and caring science, the two being seen as equally important.
Relevance to clinical practice
The result indicates a need for increased knowledge of the importance of the caring relationship, irrespective of context and the acute nature of the situation. In order to promote practice of this knowledge, training and simulation exercises can be carried out in specialist training for ambulance nurses and among clinically active ambulance personnel. Moreover, it is important to stimulate reflection on core ethical nursing and caring values, both in specialist education in general and in clinical education in the ambulance services in particular.
Further research into this topic is important. Firstly, studies are needed to understand a caring presence as a wordless relationship from the patient’s perspective. Secondly, studies are needed to further understand how ethical values are interpreted, applied and discussed amongst ambulance nurses, specialist nurses and other ambulance personnel in the prehospital setting.
Footnotes
Authors’ contribution
All authors were involved in the study’s concept and design. Cecilia Svensson collected the data. Cecilia Svensson, Anders Bremer and Mats Holmberg together analyzed the data, drafted the manuscript and approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study was carried out in accordance with the Declaration of Helsinki. According to Swedish law (SFS 2003:460), ethical approval is not required for this type of study. However the study underwent an ethical review in advance.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.