
Abstract
Objective
Gather information from physicians about factors contributing to unnecessary noninvasive imaging and impact of possible solutions.
Methods
Qualitative study of 14 physicians using a phenomenological approach and the Theoretical Domains Framework.
Results
Most participants (n = 9) self-reported that >10% of the imaging tests they order are unnecessary. External sources of pressure included: peer-review, patient demands, nursing expectations, specialist requests (social demands), as well as prior experience with patient advocates, and the compensation and pension system (environmental context). Internal sources of pressure included reliance on anecdote (emotion), self-doubt about diagnoses (beliefs about capabilities), and fear of missing a diagnosis and of professional liability (beliefs about consequences). Participants expressed both optimism and concern about potential solutions, such as adopting decision support software.
Conclusion
Physicians are under pressure from multiple sources to order unnecessary imaging. Peer review, nursing expectations, and perceptions about Veteran compensation and pension are newly reported contributing factors.
Introduction
The United States (US) spends twice as much on health care as other industrialized countries with the majority of costs driven by medical technology and higher prices. 1 In 2013, Americans had the highest per capita rates of imaging exams (magnetic resonance imaging, computed tomography (CT), and positron emission tomography) as compared to similar countries with available data. 1 This has led both the lay press and biomedical literature to consistently express concerns about the overuse of noninvasive imaging for clinical situations, where such testing is not likely necessary resulting in the movement toward high value, cost-conscious care. 2 These issues have led to the development of appropriate use criteria (AUC) for testing by specialty societies and a mandate from Congress to use these criteria for reimbursement by Medicare.3–5 The public group Consumer Reports partnered with the American Board of Internal Medicine and numerous other organizations to promote the Choosing Wisely campaign and encourage patients to take a more active role in questioning low-value care. 6 Myriad solutions have been promoted on how to reduce low value imaging including educational curricula, audit and feedback, decision support software (DSS), and more.
While some small-scale interventions have proven effective, on a national level, trends in unnecessary cardiac imaging appear to have not shifted. Within cardiology, the rate of unnecessary echocardiograms, cardiac CT, and nuclear stress tests has not changed despite decades of history of AUC. 7 Modest evidence suggests that poor awareness of AUC may partially explain the lack of practice change, although other drivers may contribute to unnecessary care. One proposed solution is the adoption of DSS that would provide AUC recommendations at the point of care. DSS systems appear to modestly reduce unnecessary care; however, potential pitfalls have not been well described.8,9
We conducted this qualitative study among physicians who order noninvasive tests to explore attitudes and opinions about low value care. Specific domains included self-reflection on patterns of noninvasive imaging use, inquiry to factors that contribute to ordering of unnecessary tests, and opinions about potential benefits and risks with adoption of DSS.
Methods
We performed a qualitative study using a phenomenological approach to broadly address several domains related to the unnecessary use of noninvasive imaging. A rapid assessment process approach was used for data analysis. 10 The research team included physician and non-physician members with a wide range of experience using qualitative methods. Non-physician team members provided unbiased perspectives regarding study design, recruitment, thematic saturation, and interpretation of data. No members of the study team had any supervisory roles over study participants. The study conformed to all Veterans Health Administration (VHA) 11 regulations for human subject research, and regulatory oversight was provided by our Institutional Review Board.
Study participants were physicians actively practicing at our VHA facility and recruited through email. Purposeful sampling was employed to include participation from a wide variety of specialties including hospital medicine, internal medicine and subspecialties, primary care, emergency medicine, and radiology. All participants provided written informed consent. The interview guide was developed based on the Theoretical Domains Framework with the intent of exploring knowledge, skills, beliefs, motivations, environmental contexts, social influences, emotions, and decision processes related to noninvasive imaging and DSS12,13 (supplemental material). The interview guide was pilot-tested on two trusted informants and adjusted based on their interviews. Individual interviews were conducted with participants in a private office with the principal investigator and lasted approximately 30–60 min. Recordings were performed anonymously and transcribed by the study team with each transcription being double-checked by a second team member. Each team member independently assigned a neutral domain name to every question and sub-question from the interview guide, which was reviewed and discussed by the team for consensus. A total of 27 domains were initially assigned that were used in the analysis of the transcripts (supplemental material). Two domains were merged resulting in 26 pre-specified domains mapped to each question or sub-question from the interview guide. The 26 domains were combined into nine for the purposes of succinctly presenting the results.
To enhance the validity of the data, each transcription was analyzed by a minimum of three study team members in two stages. First, reviews were done individually, where relevant responses were identified as themes and assigned to the pre-specified domains. Second, the reviewers shared their results, discussing and resolving any discrepancies. Consensus on relevant themes for each domain and each with representative quotes for each theme for every study participant was captured in an electronic database. Enrollment continued until (1) all desired medical specialties were represented in the sample and (2) the study team agreed that the thematic saturation had been achieved for the pre-specified domains. At the conclusions of individual transcript analyses, the study team collectively reviewed the data and agreed on final themes for each domain. We applied the Standards for Reporting Qualitative Research in drafting this manuscript. 14
Results
A total of 14 physicians participated, the median number of years in practice was 15, ranging from 3 to 40. Most participants (n = 9) reported that they order noninvasive imaging tests at least daily; the most common tests ordered were CT of the abdomen (n = 7), CT of the head (n = 5), and CT screening for lung cancer (n = 3).
Domain 1: Definition of unnecessary testing
Participants were asked to volunteer their own definitions of what constituted an unnecessary noninvasive test. Responses fell into three basic themes: the test is low value, the test is primarily being done to satisfy the demands of an individual (patient or healthcare provider), or the test will not result in a change to diagnosis or management. One participant said: “When clinical findings are benign and I’m not going to gain any more from doing that imaging study than what I know as a clinician.” The majority (n = 9) self-reported that 10% or more of the noninvasive tests they order are unnecessary.
Domain 2: Pressure to order unnecessary tests
All but one participant reported that they felt pressured to order noninvasive tests; sources of pressure are listed in Table 1. One participant described how nurses and other care team members sometimes pressure physicians to order unnecessary tests: “I may stand up to the nurses or to the ERT [emergency response team]…and say ‘hey we don’t need to do this’, but folks pressure you into it.” Nearly, all respondents indicated that their response to these pressures is to first communicate with the patient or clinician, and if that fails to resolve differences, they will order the requested test.
Themes for qualitative domains.
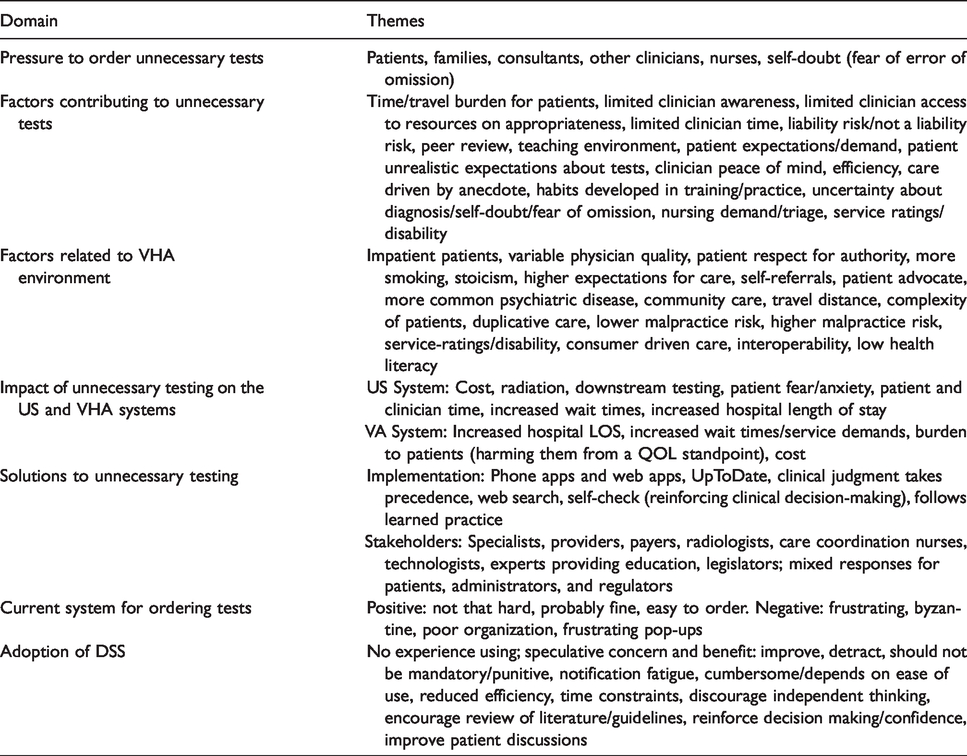
Domain 3: Factors contributing to unnecessary noninvasive testing
Themes for this domain were myriad, including: patient demands, clinician uncertainty/self-doubt, care driven by anecdote, and reliance on imaging over other data (Table 1). In addition to clinical demands from patients, some participants reported that patients demanded that tests be done in order to increase the remuneration they receive from the Veterans Administration Compensation and Pension System. Overreliance on imaging was described as such: “We have people who want imaging on every patient they see; one does not do well interpreting plain films, so everything is a CT scan.”; “[doing an unnecessary test] is easier than doing a physical exam; you can always order a CT scan, you can always talk yourself into one.” Opinions on the impact of professional liability concern on unnecessary testing were mixed. One participant was concerned that unnecessary tests increase liability risk due to minor abnormalities not receiving adequate follow-up. Two respondents mentioned peer review as a contributor. “Sometimes it enters your mind, based on your experience with a previous peer review, that if you don’t do something … people are going to be looking over your shoulder.” Anecdotes were mentioned as a contributing factor. “Everybody has that story of this one time and you can tell them about the other thousand times it wasn’t, but that one time seems to loom larger.”
Domain 4: Good and bad outcomes of unnecessary testing
To further explore the impact of clinical anecdotes on unnecessary imaging, participants were asked to describe any stories they could recall, where an unnecessary test resulted in a good or bad outcome for the patient. Several provided anecdotes about unnecessary tests that uncovered an occult renal cell carcinoma, a pulmonary abscess associated with a malignancy, a pulmonary embolus, severe obstructive multivessel coronary artery disease, liver nodules, and others. One participant noted that even if a test is clinically unnecessary, it may have substantial value for the patient by providing reassurance and confirmation of the physician assessment. Physicians noted several ways that unnecessary tests result in bad outcomes for patients including contrast nephropathy, radiation exposure, and increased length of hospitalization. Participants noted how “incidentalomas” found on unnecessary tests contribute to further unnecessary tests. One participant explained: It’s very common for people to have one test done that shows an abnormality and then that leads to further testing and anxiety that leads down this rabbit hole of serial testing and with each additional test, there’s a possibility that there could be another abnormal finding of borderline significance.
Domain 5: Factors related to VHA environment
Participants were asked to describe factors contributing to unnecessary noninvasive testing that might be unique to the VHA environment; results are shown in Table 1. Themes included Veteran stoicism and respect for authority. Some participants felt that the VHA environment had a higher risk of professional liability compared to other environments, while others felt that liability risk was lower in the VHA. Some factors that physicians outside the VHA may not be aware of include the compensation and pension system, the patient advocate, community care, and travel burden for Veterans. As one participant put it: You can’t argue with Veterans, we’ve been told the patient is right and this is consumer driven … if you don’t give Veterans what they want they’ll go to the Chief of Staff’s office, they go to the patient advocate, and they call their Senators.
Domain 6: Impact of unnecessary testing on the US and VHA systems
Participants provided thoughts on the impact of unnecessary testing on the US healthcare system and then, specifically, the VHA system. Increased costs and lost clinician productivity were common themes; many also reported on how unnecessary tests burden patients with cost, time, travel, and how unnecessary tests create delays in care through length of stay and wait times. As one participant explained: “It makes our health care unnecessarily more expensive than it already is. It has this compounding effect where one test leads to another test leads to another test, so not only unnecessary cost the first time, it’s the unnecessary cost of these incidental tests.”
Domain 7: Solutions to unnecessary testing
Participants had mixed opinions on whether clinical guidelines are useful for reducing unnecessary testing. Adjectives to describe guidelines included: vague, accessible, helpful, clear, and not always clear. “Guidelines are only as good as the degree of their dissemination and whether the person reading it incorporates it into their practice.” Guidelines were adopted in clinical practice through a variety of methods (Table 1). Most participants (n = 9) were aware of the Choosing Wisely campaign. Most indicated agreement with Choosing Wisely recommendations from their specialty society; however, they expressed concern about effectiveness at reducing low value care. When asked “which stakeholder should participate in reducing unnecessary imaging,” most agreed that general and specialty clinicians should collaborate. There were mixed feelings about the potential roles for patient, administrators, and regulators. (Table 1)
Domain 8: Current system for ordering tests
The current VHA system for ordering noninvasive testing received mixed reviews with some participants feeling that the system was “not that hard” or easy to use. One participant described the VHA system as “byzantine.” None of the participants could recall that their ordering habits for noninvasive testing were used as a measure of quality. When asked how this might affect care, those who thought that tracking test ordering might improve care were concerned about how such a system would be implemented.
Domain 9: Adoption of DSS
When specifically asked to address the adoption of DSS, none of the participants had any prior experience with such tools. They expressed concern over how the DSS is implemented into workflows and potential negative effects on efficiency (Table 1). One expressed concern about DSS discouraging independent thought, while others thought DSS might encourage a clinician to review literature about testing or reinforce decision making. Some reported that using DSS might facilitate discussions with patients about when tests are unnecessary. One participant said: It depends on how quick and easy it [DSS] is to use. If this is something that is inserting itself with every test that I order, that is going to be a frustration because there is a lot of stuff that I order routinely that I know as indicated, that I want to get and I just want to get a quickly.
Discussion
Prior literature investigating the factors that contribute to unnecessary or low-value imaging has primarily focused on testing individual hypotheses one at a time. By applying qualitative methods to this issue, we have uncovered some factors which may have been unknown and warrant further investigation. A key observation is that myriad factors contribute to unnecessary noninvasive imaging, many of which are external pressures that cannot be solved with more physician knowledge. In trying to understand readiness for adopting DSS, we noted that physicians without any exposure to DSS accurately speculated on potential positive and negative effects of these systems.
Within the domain of factors contributing to unnecessary testing, we observed many themes including peer pressure, following intuition or anecdote, and fear of missed diagnoses. Many themes are similar to those observed in a study of attitudes about guideline-discordant imaging for prostate cancer. 15 Makarov et al. 15 found, as we did, factors specific to the VHA environment including patient characteristics and that guideline-discordant imaging saps resources from other areas in the hospital. Prior work has shown that some clinicians are driven by concerns about professional liability; so, it was interesting to note that some participants, in this investigation, specifically reported that liability was not a concern.
In addition to informal peer pressure driving low-value care, participants in our study indicated that formal peer review was a factor. While some peer review programs have demonstrated improvement in care quality metrics, the success appears to be linked to physician engagement and perceptions of how the peer review is administered. Parallels may be drawn from data on audit and feedback programs, which have shown mixed effectiveness. 16 It is not difficult to imagine how having an anonymous peer criticize you for not ordering a test could potentially shift your practice pattern toward more test ordering. Further study would be necessary to determine if the participants at our facility have specific concerns about our local peer review program or if this is a more widespread problem across other facilities. 17
The Compensation & Pension system in the VA evaluates Veterans’ service-related disabilities and makes determinations about appropriate remuneration. This system is separated from the clinical care provided by VHA on purpose to avoid the conflict of interest that would arise if clinicians also had to make decisions or have input to the compensation system. Many patients and clinicians are unaware of the firewall separating the two and may feel pressure to order tests thinking it will contribute to an increase in compensation from service-related disabilities. The potential impact of this phenomenon has not been studied in the biomedical literature and would be worthy of future investigation.
While patient advocates may be clinical staff, in our healthcare system, the title refers to a non-clinical staff member, whose occupation is to help the patient navigate the health care system and to help bridge gaps between patients and clinicians. The effect that advocates have on care has not been well studied, although they have been noted to improve patient satisfaction scores. 18 Within the VHA system, patient advocates are responsible for ensuring that the rights of patients are met (VHA). The themes voiced by our participants suggest that, in some cases, these well-intended advocates may exert lasting influence on the ordering of noninvasive imaging tests.
One goal of our investigation was to gauge the opinions of physicians on adopting DSS to help encourage more judicious use of imaging tests. Conceptually, DSS operate on the presumption that ordering clinicians are poorly informed about appropriate indications for tests. That presumption is based on literature such as Kline et al., 19 where over one-third of clinicians had not heard of AUC.
Themes from this domain suggested that physicians had some optimism about the capacity for DSS to help in this regard, similar to findings from the qualitative study done by Gyftopolous et al. 20 on CT angiography for pulmonary embolus. Building on this optimism, however, participants in our study identified some potentially serious issues with DSS adoption, specifically that reinforcement of best practices could come at the cost of lost productivity and efficiency. These issues have been documented quantitatively in other studies, including the VHA’s Systematic Review on DSS. 8 As healthcare facilities make plans to adopt DSS systems, serious attention should be paid to how implementation affects workflow to minimize these risks.
Our study was conducted in an academically affiliated VHA facility, and the findings may not be applicable in other settings. As a qualitative study, we cannot confidently comment on the prevalence of these factors among practicing physicians. We did not use a grounded theory approach to this study topic, because so many factors related to unnecessary imaging have already been documented; we did allow for new domains to be included as data collection proceeded.
Conclusions
Unnecessary imaging is a substantial problem in health care contributing to wasteful spending and limitations in access for patients. While some unnecessary imaging is ordered because clinicians are unaware of when a test is appropriate, substantial external pressures from a multitude of sources are important factors as well. Solutions, such as DSS, may address part of the problem but are not likely to be a panacea.
Footnotes
Authors contributions
David E Winchester provided the concept and design, obtain funding. All authors did Data collection, analysis and interpretation, manuscript drafting, critical revision, final approval.
Acknowledgements
Contents do not represent the views of the Department of Veterans Affairs or the U.S. Government.
Data integrity
The authors declare that they had full access to all of the data in this study and the authors take complete responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Career Development Award #13-023 from the United States Department of Veterans Affairs Health Services Research and Development (HSR&D) Program.
Supplemental Material
Supplemental material for this article is available online.