
Abstract
Moral distress is a fundamental problem in the nursing profession that affects nurses. Critical care nurses are more susceptible to this problem due to the nature of their work. Moral distress may, in turn, lead to several undesirable consequences. This study aimed to determine the relationship between moral distress and intention to leave the ward among critical care nurses. This descriptive-correlational study was conducted by census method on all eligible nurses who worked in Coronary Care Unit (CCU) and Intensive Care Unit (ICU) of AhVaz hospitals, Iran. Data was collected by Corley’s moral distress questionnaire and a researcher-made questionnaire to investigate the intention to leave the ward. Questionnaires were completed through self-report and data were analyzed using a t-test and Pearson correlation coefficient. The results showed that there was a direct association between moral distress and intension to leave the ward in critical care nurses (P < 0.05). Also, the intensity of moral distress (P = 0.03) and the intention to leave the ward (P = 0.007) were significantly higher in ICU nurses. Given the high exposure of critical care nurses with moral distress and its association with leaving the ward, it seems that devising strategies to reduce or control moral distress and its negative consequences are necessary, particularly in ICU nurses.
Introduction
Moral distress is a fundamental problem in the nursing profession that affects nurses and occurs when nurses cannot do their routine activities on meeting patients’ requirements and their family in consideration of morals, due to reasons like an insufficient number of staff, lack of regulations, and deficiency in supporting organizational processes. 1 According to one definition, moral distress can be considered as a psychological imbalance, experienced when the person is prevented from the right action or is forced to do something he knows is incorrect. 2 Harmic believes that the source of moral distress for nurses in health environments is the conflict between the nurse’s tendency for doing right and moral actions and organizational rules about lawful and unlawful acts. 3
One of the risk factors for the development of moral distress is repeating and being encountered with distressing factors that affect the intensity of perceived distress. 4 Moreover, the factors leading to moral distress are different according to the career’s conditions, for example, critical care nurses may experience different types of moral distress, compared with nurses in other wards and the incidence rate of distress may be higher in them.5,6
In this regard, results of the study by Elpern et al. revealed that moral distress would increase in intensive care units, due to widespread need to moral decisions in care and treatment of patients with critical conditions. 7 Most of the moral distress in critical care units originate from the nature of work in these wards and their admitted patients. Some of these sources include aggressiveness, futile treatment of dying patients, problems related to obtaining informed consent from patients, refusing or avoiding treatment of patients with poor prognosis, the sudden death of patients, working with incompetent nurses and doctors, and being forced towards activities under organizational policies that limit moral decisions.8,9 Different studies have reported significant moral distress among critical care nurses.10,11 Studies in Iran have also shown high levels of moral distress in critical care nurses than nurses of other wards.12–14
Thus, nurses in these units are often more exposed to moral distress and decision-making challenges, due to the type of care and their activities, while moral distress has multiple negative consequences for nurses, including disorder of general health of nurses, turnover in wards, leaving their jobs, shortage of human nursing resources, decreased quality of care, nightmares, insomnia, and palpitations.12,15 Other negative consequences of moral distress in nurses include less work-engagement, loss of self-esteem, hopelessness, anger, and discomfort, caused by the feeling that they cannot fulfill the patients’ requirements or feeling of disability in performing their duties and commitments to patients. 16 Emotional exhaustion and burnout are also other consequences of moral distress, 17 which can, in turn, lead to leaving the job. According to the results of an Iranian study, 15–45% of nurses’ leaving their job is due to the effects of moral distress. 12 Fogel believes that there will be a great reduction in the number of nurses, if moral distress in nursing is not considered, 18 as it is believed that nurses’ turnover will increase and some evidence suggests 15–21% of nurses’ annual turnover, while an estimated cost of a nurse replacement is approximate to $42–64 19 Since training qualified nurses for working in critical care units need high costs, time, and energy, identification of factors that may relate to the nurses’ tendency to discontinue working in these wards is important.
As the continuation of stressful situations and the resulting mental and physical complications deplete nurses’ resistance reserves and cause dissatisfaction with the work environment, it can increase absenteeism, and intention to leave in nurses. 20 A kind of intention to leave is to leave the working unit. Since most of Iranian studies on moral distress assessed its frequency or relationship with some physical or mental consequences and showed there is a highly moral distress in critical care units,12,13,21–23 this study aimed to determine the relationship between moral distress and intention to leave the ward in critical care nurses.
Materials and methods
The present descriptive-correlational study assessed the association between moral distress and the intention to leave the unit by critical care nurses. The study was done in four educational hospitals in Ahvaz, Iran. The instruments used for data collection were two questionnaires: The first, Corley’s moral distress questionnaire that consists of 24 questions that include situations that show the intensity and frequency of moral distress by being in that position. The frequency of moral distress was measured by “never encountered” to “frequently encountered” and in the intensity was measured from “no distress” to “great distress”. The second was a researcher-made questionnaire to assess intention to leave the unit and was designed by the researchers by using similar questionnaires on leaving the job.18,21,22,24 It was included 10 questions based on a 5-point Likert scale with answers ranging from “completely disagree” to “completely agree”. The validity was confirmed using content validity and experts’ opinions who were consisted of 15 critical care nursing faculty members, and medical ethics specialists (CVI = 0.8). The reliability of the instrument was confirmed by internal consistency using Cronbach's alpha with results in α = 0.84 and α = 0.90 for the moral distress and the intention to leave questionnaires, respectively.
After receiving ethical approve from the Ethics Committee of Tehran University of Medical Sciences and coordinated with the head nurses to enter the wards. The researchers identified the eligible nurses that were 142 nurses, totally. Inclusion criteria consisted of having a bachelor's or master’s degree in nursing and at least one year of work experience in coronary/intensive care units (CCU/ICU). Due to limited sample size, the census sampling was used. The tools and written informed consent were distributed to the qualified participants. They were asked to answer the questionnaires in self-report manner whenever it was possible and they were comfortable. Totally, 119 questionnaires were returned (response rate of 83.8%). After removing incompeleted questionnires, 113 remained and analyzed. After completing data gathering, the data were analyzed using SPSS software (version 16; SPSS Inc., Chicago, IL, USA). Descriptive analysis, independent t test, and Pearson correlation coefficient were used for analyzing the data. A P value of <0.5 was considered statistically significant.
Results
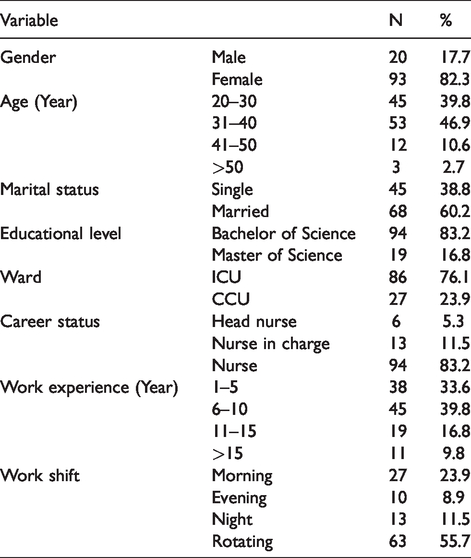
Most of the nurses participating in the study were female (82.3%), married (60.2%), and had a bachelor's degree (83.2%). The mean age of nurses was 33.6 ± 5.5 years with the range of 23–51 years. The most of the participants (39.8%) had 6–10 year-work experience in critical care with average of 10.8 ± 0.8 years. Most of the nurses worked in ICU (76.1%) and the rest in CCU. With regard to the career status, head nurses were at least (5.3%) and the nurses were the most (83.2%). The mahority of the participants (55.7%) had rotating shifts (Table 1).
Characteristics of Nurses (N = 113).
The results showed that majority of the participants had a moderate moral distress with reference to frequency (63.8%) and intensity (51.3%). Similarly, most of the nurses (61%) had a moderate intention to leave the ward. There was no significant difference between frequency of moral distress in CCU and ICU, but mean of intensity of moral distress in ICU was higher than CCU (56.4 ± 18.1 vs. 47.7 ± 20.3) and it was statistically significantly (t = 4.8; P < 0.05). According to the findings, the mean of intention to leave the ward between ICU and CCU nurses was 28.8 ± 8.7 and 23.9 ± 8.8, respectively. A significant difference was found between intention to leave ICU in comparision with leaving CCU (t = 5.1; P < 0.05) (Table 2). It must be mentioned there was not any significan relationship between demographic variables and research variables, except female nurses experienced more moral distress (P = 0.04).
Frequency and intensity of moral distress and intention to leave intensive care units by nurses.
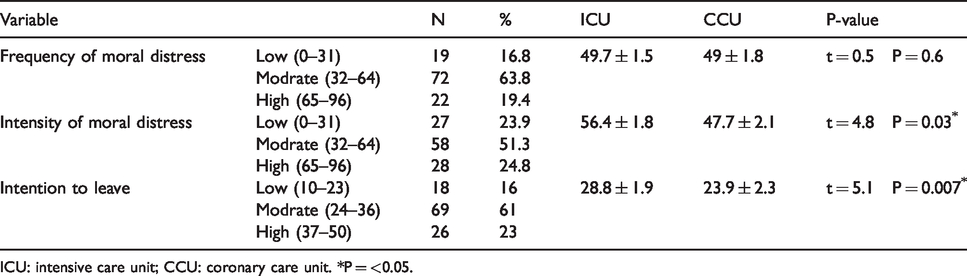
ICU: intensive care unit; CCU: coronary care unit. *P = <0.05.
According to the results, the total mean score of intention to leave the ward among critical care nurses was 26.3 ± 2.1. The Pearson correlation coefficient showed there was a significant correlation between intention to leave the ward with both frequency of moral distress (r = 0.141; P < 0.05) and intensity of moral distress (r = 0.118; P < 0.05) (Table 3).
The correlation between frequency and intensity of moral distress with intention to leave intensive care units.

*P = <0.05.
Discussion
This study aimed to determine the relationship between moral distress and the intention to leave the unit in critical care nurses. The results showed that the frequency and intensity of moral distress are higher than average in critical care nurses and moral distress was higher in ICU than CCU nurses. In most Iranian studies, moral distress of critical care nurses was reported moderate to high.12,14,25,26 The results of other countries consistently show moderate to a high level of moral distress experienced by critical care nurses.2,27,28
The results of this study showed that most of the nurses (69%) moderately intend to leave their current working unit. Although no Iranian study has addressed the issue of leaving the ward/unit, the results of this study can be justified based on the experiences and observations of authors as critical care nurses. Based on our long and real experiences, some nurses intend to work in other wards except critical care units due to various reasons, like instability of ICU environment, working with critically ill patients, futile treatment of dying patients, high workload, high work stress, physical burnout, occupational depression, low salary in comparision with difficult tasks, some unbecoming procedures (e.g. suctioning) and so on. While some others tend more to work in these units, due to some other reasons such as plyaing a role in saving the lives of critically ill patients, occupational independency, direct involvement in patients’ care, working with complex medical devices, and necessity of being knowledgeable and skilled. Thus, a combination of these motivational and preventive factors creates moderate intention to leave critical care units by the study population. As a whole, diverse factors are associated with nurses’ intention to leave the profession/ward however the quantitative findings of similar studies may present different results in this issue. For example, Cortese conducted a study on critical care nurses in two large public hospitals and a private hospital in the north of Italy and reported 41.8% of nurses intended to leave their current working place 29 but various reasons have been found about intention to leave differents wards including occupational independence, participation in decisions related to patients’ care, organizational environment, leadership, teamwork, etc. 19
In general, the results of this study showed a direct and negative association between intensity and frequency of moral distress with the intention to leave critical care units and ICU nurses are more vulnerable to this issue, compared to CCU nurses. As it has been shown, 25–45% of nurses’ turnovers between different units are due to the effects of moral distress. 12 The results of other studies that addressed the issue of turnover have also confirmed the significant direct relationship between moral distress and leaving the job.18,30,31 For example, it has been identified that 43% of critical care nurses in the United States have left their jobs due to moral distress, 32 and 15% of them have left their nursing profession for this reason. 1 Laurs et al. (2020) found nurses who had a high moral distress level were three times more likely to consider leaving their position compared with respondents who had a medium or low moral distress level (8.7% and 2.9%, respectively; P< .05). 11 In addition, it has been found that intention to leave is different among nurses in different wards and many factors are associated with this issue.29,33
Based on the evidences, critical care nurses experience different moral distress than other nurses.6,7,14,26 Moral distress in intensive care units usually referes to critical conditions of patients with poor prognosis, high work tension, lack of professional and specialized personnel, 14 invasive procedures, caring for dying patients, working with unsafe personnel and need to make decisions quickly, 12 carrying out physician’s orders that seem to be unnecessary tests and treatments, following the family’s wishes to continue life support even though it is not in the best interest of the patient. 11 Despite these findings, no study was found on the issue of comparison moral distress and leaving the ward or job between different wards and the associated factors. Thus, the current study is invaluable and innovative, as it has provided baseline information in this regard, but considering that it was performed in a small level with limited sample size, further studies are required to confirm the results and increase its generalization. Also, it is essential to assess the predictive factors of intention to leave in critical care nurses.
Conclusion
As the results of this study indicated high moral distress in critical care nurses and the association between moral distress and intention to leave the working unit, identifying factors involved in moral distress, and implementing appropriate methods to control or remove them is essential. Strategies such as implementing continuous professional development courses on ethical issues and dilemmas, ethical decision making, coping and relaxation techniques for nurses are suggested. In addition, make some policies to enhance a better team work and to define specific protocols for some challenging situations like no resuscitation or futile care of critically ill patients can result in stress and worries reduction about ethical and legal outcomes for critical care nurses. Hence, these can cause preventing undesirable consequences of moral distress, including the intention to leave the ward or even nursing profession, and saving extreme expenditures and resources that needed to train nurses to work in critical care units. However, there is a need for further investigation about strategies and approaches for reducing critical care nurses’ moral distress.
Supplemental Material
sj-pdf-1-cet-10.1177_1477750920977094 - Supplemental material for Moral distress and intention to leave intensive care units: A correlational study
Supplemental material, sj-pdf-1-cet-10.1177_1477750920977094 for Moral distress and intention to leave intensive care units: A correlational study by Abbas Naboureh, Masoomeh Imanipour and Tahmine Salehi in Clinical Ethics
Footnotes
Acknowledgements
This research was approved by its Ethics Committee of Tehran University of Medical Sciences. The authors would like to express their gratitude to participating nurses, who cooperated in conducting this study, despite their busy workload in intensive care units.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was part of MSc. thesis that has been supported by Tehran University of Medical Sciences (grant no. 9111449019).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.