
Abstract
Background
In the coronavirus disease 2019 era, doctors have tried to decrease hospital visits and admissions. To this end, telemedicine was implemented in a non-systematic manner according. The objective of this study was to assess the current knowledge and attitudes of physicians in Alexandria, Egypt, and Punjab, India, toward telemedicine and its ethical and medico-legal issues.
Method
A cross-sectional study was implemented using an anonymous self-administered questionnaire carried out over two months (July and August 2020). A four-point Likert scale was used to collect data about background knowledge, training in telemedicine and ethical and medico-legal issues in telemedicine practice.
Results
The questionnaire was completed by 175 Egyptian and 51 Indian physicians from different specialties. A significantly higher percentage of Indian physicians practiced telemedicine than Egyptian physicians during the coronavirus disease 2019 era. Although most physicians had no specific training or licensing to practice telemedicine, most of them practiced telemedicine through their social media accounts. Ethical violations involving waiving patient consent were detected. Significant ethical violations to doctors, for example, blackmail, defamation, hate speech, accusations in a court and violations of privacy, were observed. Indian physicians (39.2%) and Egyptian physicians (24%) thought the penalties should be lower in telemedicine than in traditional practice. Finally, most participants would like to continue using telemedicine after the coronavirus disease 2019 era but with improvements.
Conclusions
Coronavirus disease 2019 changed the acceptance of telemedicine by physicians. Many ethical and legal issues need to be addressed and clarified using formal training before implementation and standardization of telemedicine services.
Introduction
In December 2019, healthcare services were confronted with the coronavirus disease 2019 (COVID-19) outbreak. As of 30 April 2021, there were over 151,819,782 cases in all countries and 3,188,188 deaths. 1 To control the spread of the virus, hospital visits and admissions decreased to maintain social distancing, as confirmed by several publications.2–4 Telemedicine was not widely implemented or integrated into health systems in Alexandria or Punjab before COVID-19. However, physicians from these countries started using telemedicine to overcome the problem of managing patients during lockdowns. With the absence of regulatory frameworks, each physician behaved according to his judgment. Some physicians used social media groups to manage patients and considered this telemedicine. The use of social media groups resulted in some frank violations of patient privacy and confidentiality. Several malpractice cases were launched against physicians.5,6
To compare telemedicine experiences with a country of similar culture and economic status, India was selected. India is a large nation that aspires to the equitable distribution of healthcare services through telemedicine. Several successful telemedicine services, such as mammography services at Sri Ganga Ram Hospital, Delhi, 5 and surgical services at Sanjay Gandhi Postgraduate Institute of Medical Sciences, have been introduced. 6
Aim of the work
The aim of this study was to assess the current knowledge and attitudes of physicians in Alexandria, Egypt, and Punjab, India, toward telemedicine and its ethical and medico-legal issues.
Methods
Study design
This comparative cross-sectional study used an anonymous self-administered questionnaire. A four-point Likert scale was used to collect data concerning three domains: background knowledge and training in telemedicine, the practice of telemedicine and ethical and medico-legal issues of the practice of telemedicine. The Delphi technique was used to develop questionnaire items by consensus among medico-legal and ethics experts and survey design experts. A pilot study was conducted to calculate the time needed for completing the questionnaire. Professors, consultants and specialists from different clinical specialties in Egypt and India were invited to participate in the study over two months (July and August 2020).
Ethics statement
The Ethical Committee of the Faculty of Medicine approved this study (Serial Number: 0304672, IRB NO: 00012098, FWA NO: 00018699).
Statistical analysis
Data were analysed using SPSS software version 25.0. (Armonk, NY: IBM Corp). The Levine test was used to test variances then independent sample t-tests were used to compare the Egyptian and Indian physician responses. Results were considered significant at the 5% level (p < 0.05).
Results
The questionnaire was completed by 175 Egyptians and 51 Indian physicians. The Egyptian physicians were comprised of 61.1% specialists, 27.4% consultants and 11.4% general practitioners. More than one-third (36%) of the respondents were members of the Faculty of Medicine at Alexandria University. The Indian group was comprised of 39.2% specialists, 39.2% consultants and 21.6% general practitioners, and 11.8% were faculty members.
Onset of online consultations
More Egyptian physicians (57.1%) than Indian physicians (33.3%) practiced telemedicine before the COVID-19 pandemic (p = 0.003). Nearly two-thirds of Indian physicians started online consultation only during the COVID-19 (Table 1).
Difference between the Egyptians and Indian groups regarding their knowledge and practicing of telemedicine.
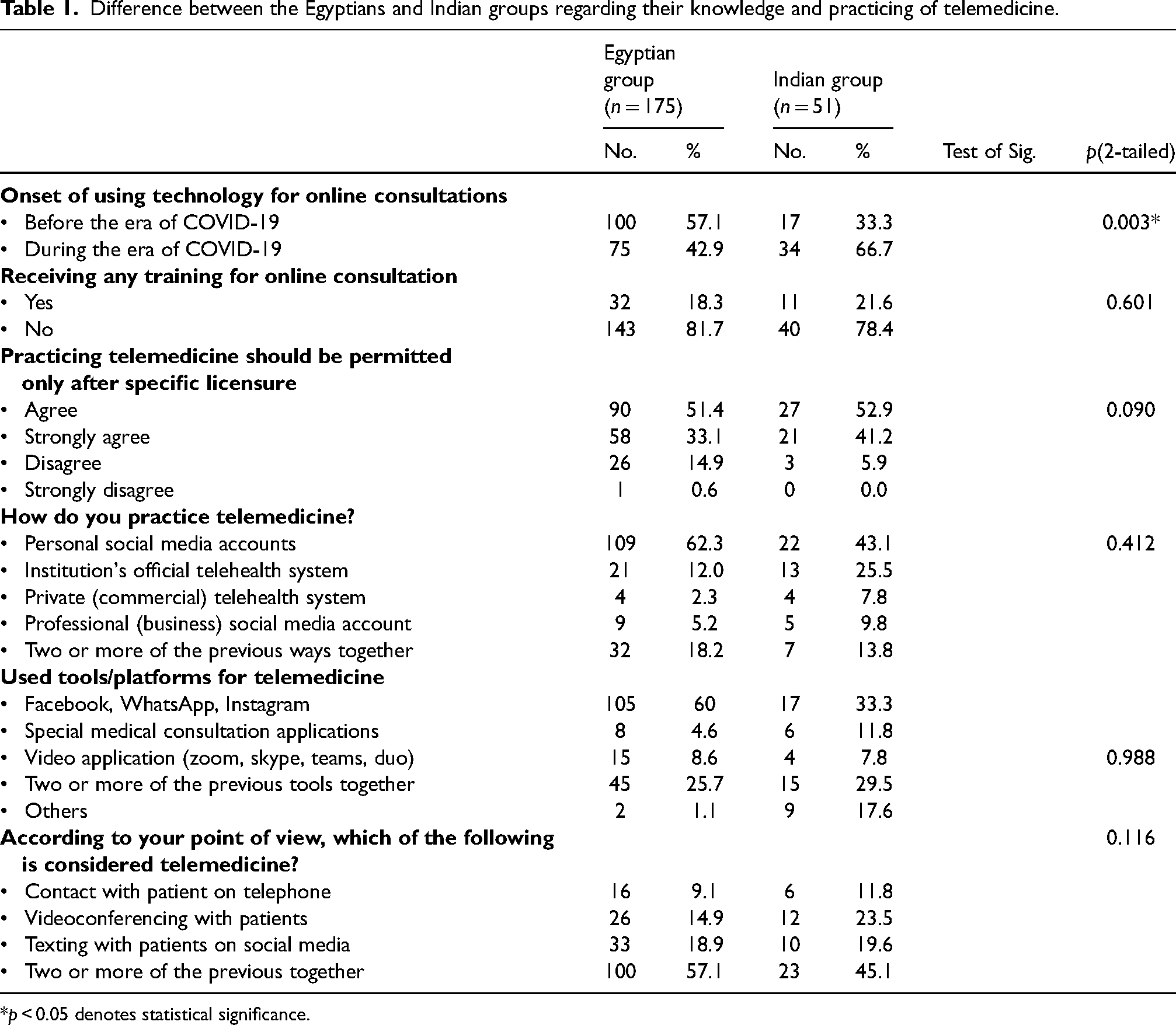
*p < 0.05 denotes statistical significance.
Receiving training for online consultation before its usage
Most Egyptians (81.1%) and Indians (78.4%) did not receive training for online consultation. Despite the lack of training, 84.5% and 94.1% of Egyptian and Indian physicians, respectively, believe that telemedicine practice should be permitted only after special licensing. These parameters were not significantly different between the two groups (p = 0.601 and 0.090, respectively) (Table 1).
Technologies for practicing telemedicine
Most Egyptians (62.3%) and Indians (43.1%) reported using their social media accounts for online consultations. On the other hand, only 25.5% of Indian physicians and 12% of Egyptian physicians used hospital/institutional official telehealth systems. The differences in usage of technologies for telemedicine were not statistically significant (p = 0.412) (Table 1). The most common applications, including Facebook, WhatsApp and Instagram, were used in 60% and 33.3% of Egyptian and Indian physicians, respectively. The use of specialized medical consultation applications or websites was reported in 4.6% of Egyptian physicians compared to 11.8% of Indian physicians.
Telemedicine from the physician point of view
Many Egyptian physicians (57.1%) considered texting with patients on social media, contact with patients by telephone and videoconferencing with patients as sound telemedicine. However, 14.9% of Egyptian physicians think only videoconferencing with patients is telemedicine. On the other hand, nearly a quarter (23.5%) of Indian physicians defined telemedicine as only videoconferencing with patients. The differences in physician point of view were not statistically significant (p = 0.116) (Table 1).
Common activities during telemedicine before and after COVID-19
Before the COVID-19 pandemic, the Egyptian physicians’ most common telemedicine activities were consultations between health care professionals (48%) and obtaining laboratory and radiological results (42.9%). Marketing for their private clinics was the most common activity (31.4%) done by the Indian physicians before the COVID-19 pandemic.
During the COVID-19 era, follow-up of patients at home and assessment of symptoms during the first interview were the most common telemedicine activities reported by the Egyptian group. In India, making outpatient appointments using the Internet was the most common telemedicine activity (33.3%), followed by obtaining laboratory and radiological results and consultations between health care professionals. Moreover, marketing for private clinics (77.7%) and patient referrals (56.9%) were the highest percentages of activities never used through telemedicine by the Egyptian and Indian physicians, respectively (Table 2).
Difference between the Egyptians and Indian groups regarding the activities done by telemedicine.
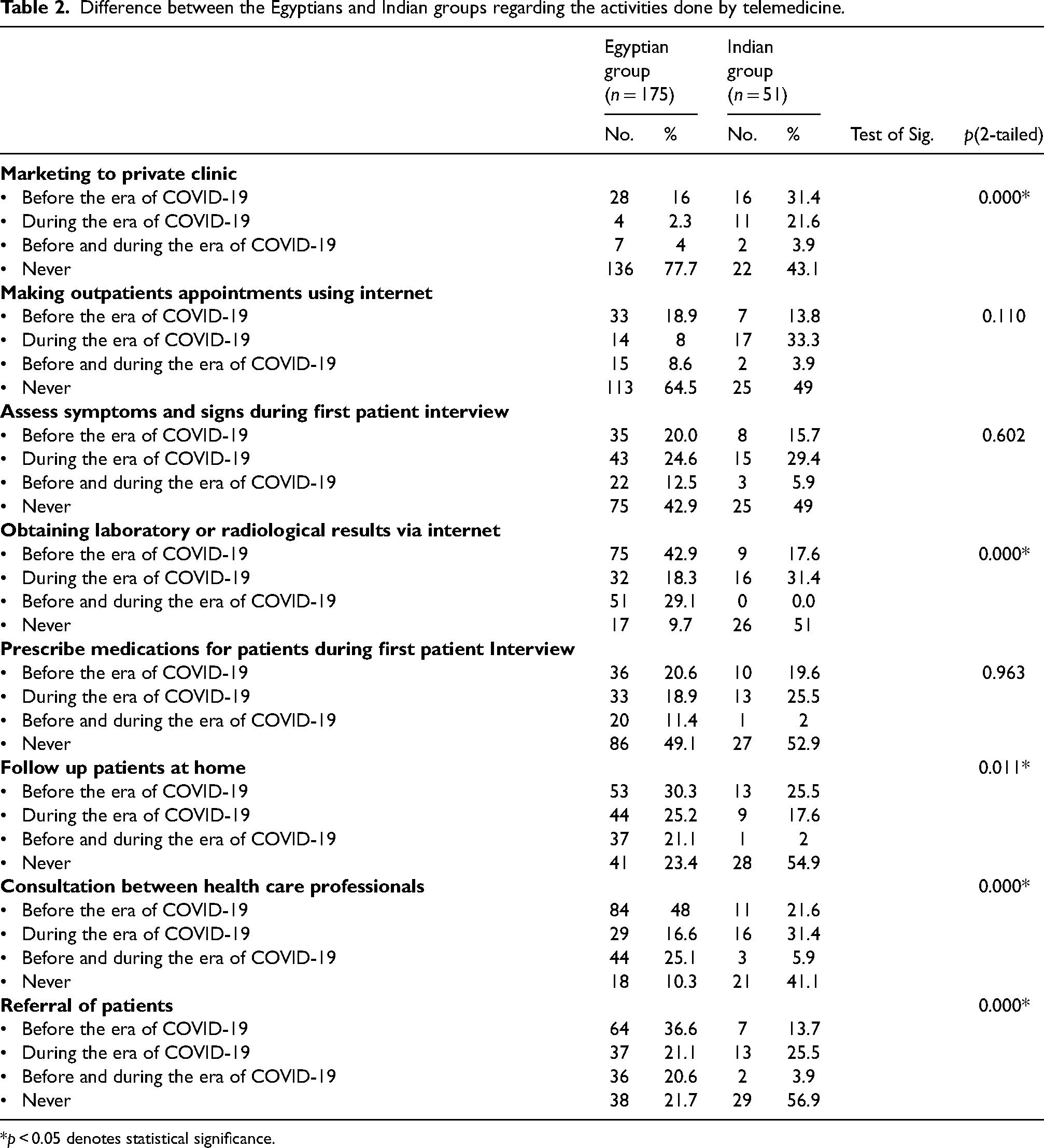
*p < 0.05 denotes statistical significance.
There was a statistically significant difference between the two groups regarding telemedicine use for marketing private clinics and obtaining laboratory and radiological results before and after the COVID-19 era (p = 0.000). There was also a significant difference regarding follow-up of patients at home (p = 0.011), consultation between health care professionals (p = 0.000) and referral of patients (p = 0.000) (Table 2).
Ethical issues during telemedicine practice
Most Egyptian physicians (88%) did not obtain written consent from patients before using telemedicine. On the other hand, 43.1% of Indian doctors obtained written patient consent before using telemedicine. More Indian physicians obtained patient consent compared with Egyptian physicians (p = 0.000) (Table 3). Most Egyptian (82.9%) and Indian physicians (76.5%) thought that voluntary contact from patients implied consent before starting therapy. In addition, more than half (53.7%) of Egyptian physicians thought that patient consent was not assessable through telemedicine. In contrast, significantly more Indian physicians (62.8%) than Egyptian physicians thought they could assess patient consent via telemedicine (p = 0.100). Moreover, more than two-thirds of physicians from both groups thought that data or photos of patients received via telemedicine could not be used for educational purposes without obtaining patient consent; differences between the two groups were not significant (p = 0.160) (Table 3).
Difference between the Egyptians and Indian groups regarding some ethical issues during practicing telemedicine.
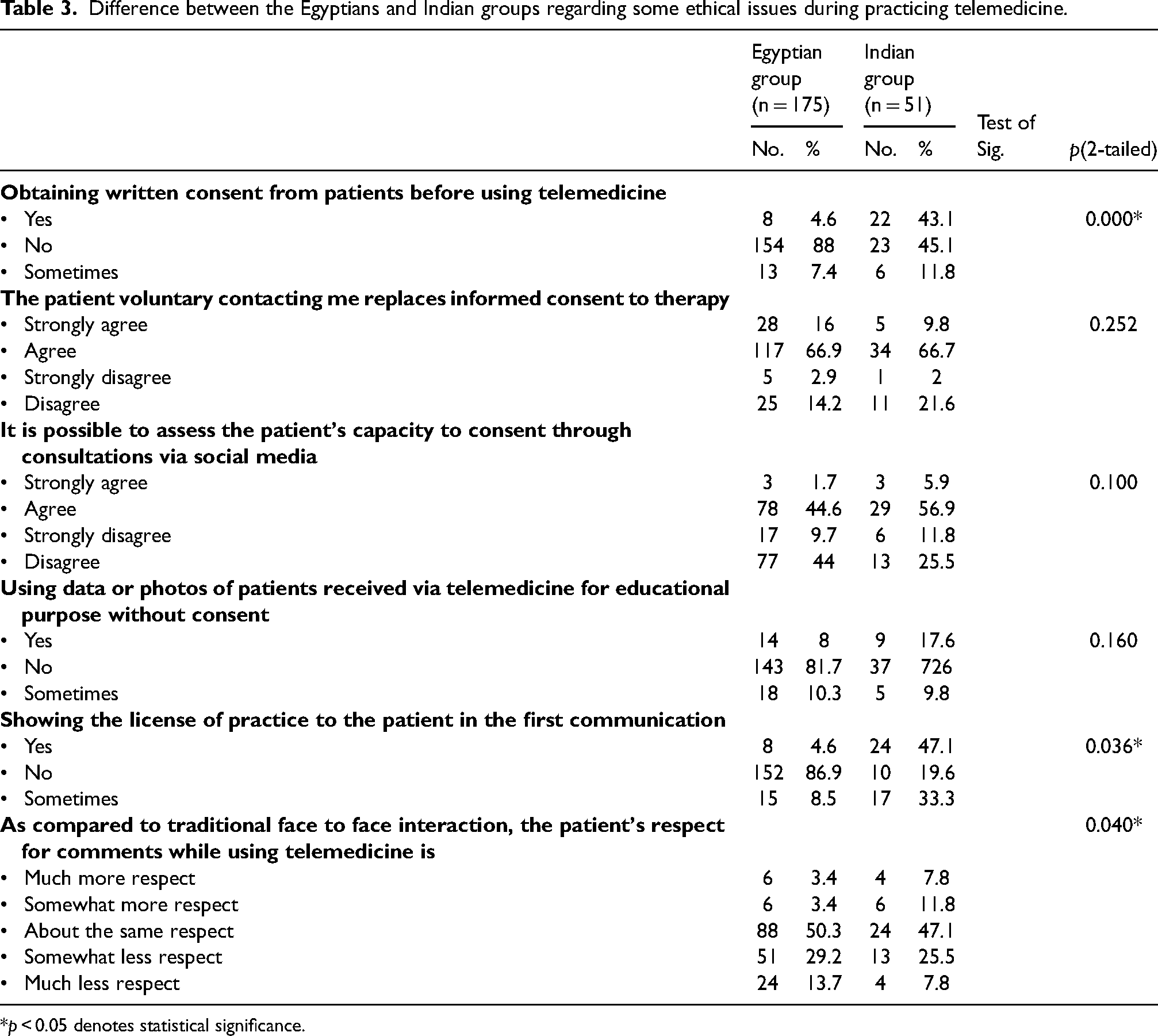
*p < 0.05 denotes statistical significance.
Most Egyptian physicians (86.9%) did not show their practice licenses to patients during the first communication. In contrast, significantly more Indian physicians (47.1%) than Egyptian physicians showed their practice license to patients during telemedicine consultations (p = 0.036) (Table 3). About half of Egyptian (50.3%) and Indian (47.1%) physicians felt less respect for their comments through telemedicine than traditional face-to-face interactions. Significantly fewer Egyptian physicians (6.8%) felt more respect during telemedicine consultations versus face-to-face consultation compared with Indian physicians (19.6%) (p = 0.040) (Table 3).
Time spent performing telemedicine and its drawbacks
Less than a quarter (23.4%) of Egyptian physicians and 35.3% of Indian physicians spent five or more hours performing online consultations. However, only 3.4% and 9.8% of Egyptian and Indian physicians, respectively, received fees for their online consultations. Violations in the form of blackmail, defamation, hate speech and accusations in court were another drawback of telemedicine; significantly less Egyptian physicians (18.3%) than Indian physicians (31.4%) felt violated (p = 0.008). In contrast, a majority of Egyptian (81.8%) and Indian (53%) physicians felt that their privacy was violated by patients who contacted them at any time (p = 0.000) (Table 4).
Difference between the Egyptian and Indian groups regarding the drawbacks of telemedicine on the physicians and the legal issues.
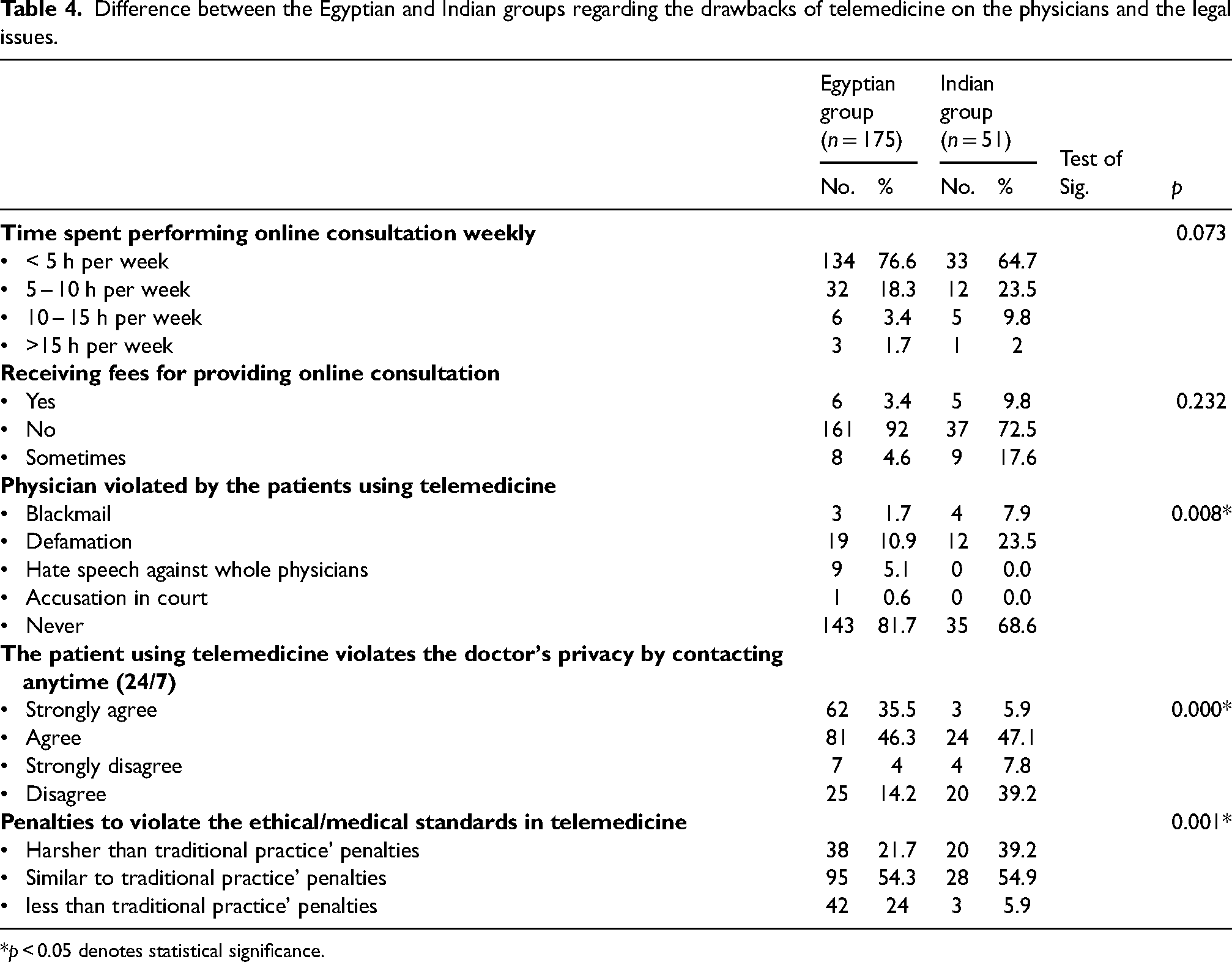
*p < 0.05 denotes statistical significance.
Legal issues of practicing telemedicine
None of the Egyptian physicians were aware of specific laws that guide telemedicine practice. In contrast, more than half of Egyptian physicians (54.3%) thought that the penalties should be similar to traditional face-to-face practice, and 24% of Egyptian physicians thought the penalties should be less than penalties in traditional practice. On the other hand, more than half (54.9%) and more than one-third (39.2%) of Indian physicians thought penalties should be similar to traditional practice or even harsher; the difference between the groups was statistically significant (p = 0.001) (Table 4).
Risks versus benefits of telemedicine
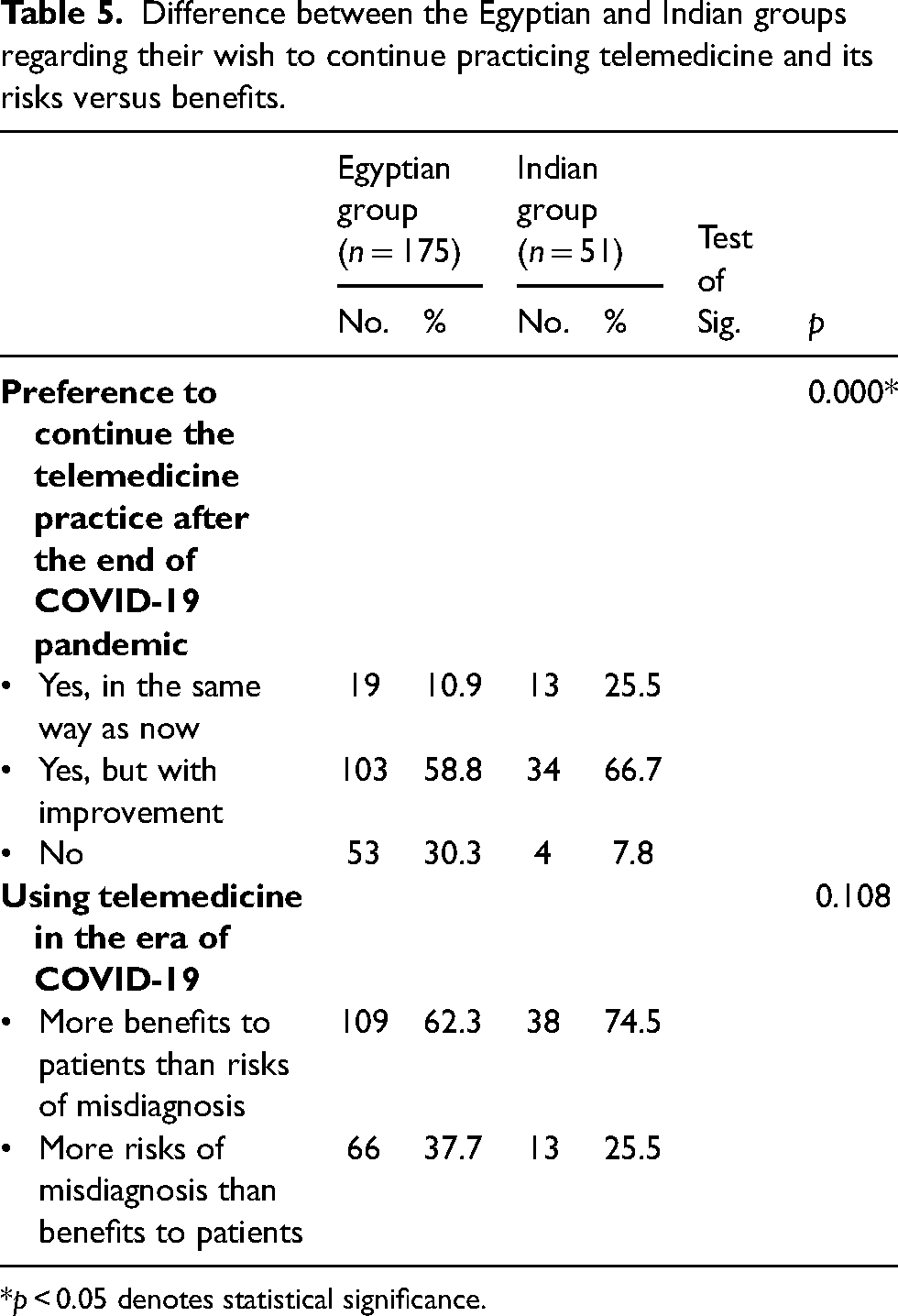
Most Egyptians (62.3%) and Indian (74.5%) physicians thought practicing telemedicine was beneficial to patients in the COVID-19 era. However, 37.7% of Egyptian physicians and 25.5% of Indian physicians thought there was a higher risk of misdiagnosis in telemedicine than face-to-face patient/physician interactions (Table 5). More than half (58.8% and 66.7%, respectively) of Egyptian and Indian physicians want to continue telemedicine after the COVID-19 era but with improvements. On the other hand, significantly more Egyptian physicians (30.3%) did not want to practice telemedicine after the COVID-19 pandemic compared to only 7.8% of Indian physicians (p = 0.000) (Table 5).
Difference between the Egyptian and Indian groups regarding their wish to continue practicing telemedicine and its risks versus benefits.
*p < 0.05 denotes statistical significance.
Discussion
Telemedicine is a subset of eHealth and can be defined as the practice and delivery of healthcare over a distance using information and communication technology. 7 Telemedicine is required for delivering health services to patients during pandemics. Telemedicine has several advantages for the patients, including reduced time, travel costs and infection rates. For physicians, telemedicine provides extra income, reduces exposure to infectious agents and sometimes provides more satisfaction from more relaxed patients. Telemedicine involves patients, doctors, technology and a regulating framework. Regardless of its value and widespread use in many countries, several ethical and legal aspects of professional telemedicine practice are of concern, including obtaining informed consent, confidentiality, patient privacy and malpractice rates. Telemedicine cannot replace regular doctor-patient relationships but is advisable in certain situations like the COVID-19 pandemic, emergencies, distant patients and war.8,9
The object of the current study was to explore the knowledge and attitudes of physicians in both countries about the use of telemedicine, patient management and compliance with normative ethics. The study also investigated the drawbacks and legal ramifications of practicing telemedicine compared to well-established telemedicine systems in developed countries. In the current work, 175 Egyptians and 51 Indian physicians from different specialties completed the designed questionnaire. Most of the respondents were specialists and consultants (88.5% and 78.4% for Egyptians and Indians, respectively). Thus, these physicians have experience and can compare regular methods to implementing telemedicine in the management of patients.
There was a statistically significant difference between Egyptian and Indian physicians regarding the onset of practicing telemedicine; almost half of participating Egyptian physicians used telemedicine before the era of COVID-19, while 66.7% of the Indian physicians used telemedicine for the first time during the COVID-19 era. In these developing nations, the COVID-19 pandemic sped up the implementation of telemedicine but without a regulatory framework. In Egypt, significant advances in the information technology infrastructure have been made, providing and enabling legal and regulatory frameworks. Despite these advances, telemedicine was confined to educational processes, such as transferring videos from the operating theater, before the pandemic. 10 India faced a similar situation. However, the current study showed that most physicians before the COVID-19 era started implementing and practicing telemedicine on their own. Thus, few publications describe the application of telemedicine before COVID-19. Telemedicine was used side-by-side with conventional health care services or as an alternative to conventional services.
Several physicians used social media to manage the diagnosis and treatment of patients during the COVID-19 pandemic, and a few physicians implemented telemedicine in their research. For example, Ashry and Alsawy 11 from Cairo University implemented telemedicine as part of a research trial. The study included 30 patients from the neurosurgery department who consented to telemedicine during a 30-day follow-up period after being discharged from the hospital. All patients were well-educated and had smartphones, high-speed Internet, and a smooth postoperative period. Residents recorded all recent clinical data concerning patient progress. Live communication with the patients or recorded videos enabled the doctors to assess the patient's mental status and speech. Patient satisfaction with the use of telemedicine ranged from 80% to 100%. Physician satisfaction rates ranged from 80% to 95%. Of course, the inclusion criteria were ideal, and this type of telemedicine is not appropriate for all patients.
Agarwal et al. 12 described the increased need for telemedicine by healthcare providers in the Medical Council practice guidelines released in March 2020. This indicates that some physicians responded faster to the situation, even though online consultations began only during the era of COVID-19. The guidelines state that telemedicine is a paid service and insists on identifying both sides of the telemedicine device. Consent is implied by the patient contacting the doctor, and texting, audio and video communication for telemedicine are allowed. Explicit in the physician/patient relationship is restricted management in certain situations, necessitating applying all known ethics with patients. Practitioners are not considered responsible for breaches of confidentiality if there is a technology problem. Areas of misconduct are identified and penalties predetermined in the guidelines as with regular methods of management. 13
In the current research, most physicians from both countries did not receive training or licensing for telemedicine. However, the physicians believe that telemedicine practice should be permitted only after special licensing. This agrees with the World Health Organization (WHO) report; the WHO reported that less than 50% of survey respondents said that specific national telehealth policies were implemented in their country or that telehealth was referenced in their national eHealth policy. 14
Several countries, including the USA and the UK, require special training and permit licenses for physicians to conduct telemedicine; these requirements were already implemented before COVID-19. 15 Moreover, the Health Professions Council of South Africa stated that only practitioners who have been deemed competent and are registered in their respective professions are authorized to participate in telemedicine practice. 16 All countries should encourage health professionals to receive training about the laws, rules and regulations for providing telemedicine health services in their respective countries.
Regarding the technologies for practicing telemedicine, most Egyptians (62.3%) and Indians (43.1%) reported using their social media accounts, for example, Facebook, WhatsApp and Instagram, for making online consultations. Unfortunately, this highlights the lack of specific telemedicine applications in developing countries. Usually, both physicians and patients use audiovisual communication for telemedicine in developed countries and consider privacy issues. In a meta-analysis, Giordano et al. 17 examined 30 articles utilizing WhatsApp Messenger in medical research. The study PICO (P-problem, I-intervention, C-comparison, and O-outcome) did not match the question PICO in many of the examined trials. Ethics and data security were not discussed in any of the research studies included in the analysis. Mann et al. 18 clarified the feasibility and impact of video-enabled telemedicine use among patients and providers in the USA.
In Egypt, the most common telemedicine activities before the COVID-19 era were consultations between health care professionals and obtaining laboratory and radiological results. In India, marketing for private clinics was the most common telemedicine activity before COVID-19. During the COVID-19 era, follow-up of patients at home and assessing signs and symptoms during the first interview were the most common telemedicine activities in Egypt. In India, the most common activities during the COVID-19 era were making outpatient appointments, obtaining laboratory and radiological results and consultation between health care professionals. The most common shared activities between both groups during the era of COVID-19 were the marketing of private clinics and patient referrals.
According to the WHO and the Pan American Health Organization (PAHO), the principal telemedicine services were teleconsultations for follow-up, diagnosis and treatment of patients, telemonitoring services for chronic patients, electronic communication between professionals and administrative management of patients (e.g. laboratory test, billing for service delivery, distance learning for professionals and evaluation and collaborative research networks). 19 As shown in our study, telemedicine services and activities practiced in both Egypt and India are congruent with the activities recommended by WHO and PAHO, except for the marketing of private clinics and patient referrals.
The American Medical Association (AMA) believes that a valid patient-physician relationship must be established before the provision of telemedicine services through face-to-face examination. The AMA also describes telemedicine services as “Unprofessional conduct” if patient management occurs without previous examination. 20 Moreover, the AMA, the World Medical Association (WMA) and the telehealth segment of the Health Professions committee of South Africa describe the ethical guidelines for conducting telemedicine, including descriptions of doctor/patient relationships, assessment of patient capacity, fidelity, privacy and confidentiality. 21
In the present study, 88% and 56.9% of Egyptian and Indian doctors committed ethical violations regarding waiving patient consent. Voluntary contact from the patients was considered consent (as with telemedicine practice in India). Assessment of a patient's capacity to consent through telemedicine is not an easy task for both sides. Still, physicians agree to not use data or photos of patients for educational purposes without patient consent. Furthermore, 86.9% and 19.6% of Egyptian and Indian physicians did not show their license to practice before conducting telemedicine. Thus, there is a gap between ethics guidelines and practitioner perspectives. This gap was described by Kuziemsky et al., 22 who stated that ethics guidelines on telehealth have a distant focus compared to the needs of practitioners. Telehealth practitioners and ethics guideline developers should comprehend medical care frameworks and initiate suitable frameworks that medical practitioners can easily apply. In addition, Kaplan 23 suggested that clinicians and guideline developers need refreshed rules for moral utilization of telemedicine and telehealthcare.
The drawbacks of telemedicine for doctors include violations of doctors’ privacy (81.8% for Egyptians and 53% for Indians), time-consuming methods, no fees for physicians, blackmail, defamation, hate speech and accusations in court. These drawbacks were experienced by 18.3% and 31.4% of Egyptian and Indian physicians, respectively. In addition, 50.3% of Egyptian and 47.1% of Indian physicians felt disrespect when practicing telemedicine. Violent episodes against doctors are not confined to telemedicine and are multifactorial. Kumari et al. 24 and Sharma et al. 25 classify these factors into professional, patient-related, organizational and violent societal episodes. From our experience, the main factors are negative media images for doctors, which provoke negative feelings from patients toward healthcare services, miscommunication between health care services and aggression from patients or their relatives. There are no penalties or support from the government.
While telemedicine's drawbacks are confined to the quality of care, the possibility of misdiagnosis, the security of personal health data transmitted electronically, the cost coverage by insurance companies and infrastructure malfunctioning may result in patient harm during tele-educational sessions or telesurgery consultations. Patient outcomes using telemedicine have not been clarified. 26
Many physicians were not aware of specific laws guiding telemedicine practice and thought that the penalties might be similar or less than penalties in face-to-face doctor/patient interactions. Developed countries have developed guidelines, laws and regulations. The Medical Council of India released practice guidelines in March 2020, but laws have not yet been implemented.
Finally, most participants wish to continue telemedicine after the COVID-19 era but with improvements. Still, ethical issues with telemedicine should be the same as in-person medicine. Maintaining trust and limiting violence toward doctors requires developing a strong patient-doctor relationship, protecting patient privacy, promoting treatment equity and targeting the same outcomes. 27 The necessity for telemedicine increased due to cost-effectiveness. Telemedicine systems should be monitored in all countries, protocols and safeguards to protect patients and doctors should be implemented, and all persons should be treated with dignity and respect. 28 All stakeholders are encouraged to address the challenges and collaborate to promote telemedicine's safe and evidence-based use during the current pandemic and future outbreaks. 29
Conclusions
In conclusion, COVID-19 changed the acceptance of telemedicine practice by Egyptian and Indian physicians. However, many ethical and legal issues need to be addressed and clarified. The optimal telemedicine services include teleconsultations, telemonitoring, communication between professionals and educational and collaborative research. Thus, telemedicine services should not replace but aid the regular medical practice. Registration, competency and training are prerequisites to licensing doctors for the practice of telemedicine.
Recommendations
Implementation and standardization of telemedicine services are needed, especially during the COVID-19 era.
In developing countries, telemedicine regulations need to be designed and evaluated, considering different cultural, environmental and economic factors.
Registration, competency and training are prerequisites to licensing telemedicine practices.
The gap between the ethics guidelines and practitioner perspectives should be removed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.