
Abstract
Background
In the general population without COPD, indoor air pollution from biomass is a causal factor of cognitive impairment (CI). CI is also common in patients with tobacco smoke COPD and has been associated with hypoxemia and cardiovascular comorbidities. CI and its risk factors have not been evaluated in COPD patients living at high altitude, who experience greater hypoxemia and frequent exposure to wood smoke.
Methods
Patients with COPD residing at high altitude with FEV1/FVC <0,70 and COPD risk factors (wood smoke, Tobacco smoke or combined exposure). Measurement of the Mini-Mental State Examination to assess CI, educational level, comorbidities, exacerbations, arterial blood gases, diffusion (DLCO), and 6-min walk test (6MWT). Comparisons between groups with and without CI using the X2 test and unpaired t-test. Logistic regression with odds ratio (OR) calculation was used to evaluate the association of CI with the variables of interest.
Results
In the 199 patients included, 16.1% had CI, the majority with mild involvement (68.8%). Those with CI had more frequent exposure to wood smoke (p<0.001), older age (p=0.017), lower educational level, PaO2 (p=0.032), DLCO (p=0.036), and fewer meters in the 6MWT (p=0.007), with no differences in sex, severity of obstruction or comorbidities. Adjusting for the other variables, exposure to wood smoke was associated with CI [OR and 95% CI: 4.82 (1.62-14.33).
Conclusions
In patients with mild to moderate COPD living at high altitude, regardless of hypoxemia, age, educational level, comorbidities, and lung function, exposure to wood smoke was associated with CI.
Introduction
According to the World Bank and World Health Organization (WHO), 2.1 billion people worldwide, one-third of the world’s population, use coal, kerosene, or biomass (wood, animal dung, and crop waste) as fuel for cooking. In 2020, the WHO estimated that 3.2 million people die annually from diseases attributable to indoor air pollution caused by the household use of these solid fuels. 1 It is known that children and women who are inside the home bear the greatest health burden from indoor air pollution, which causes chronic diseases in adults, such as chronic obstructive pulmonary disease (COPD), lung cancer, coronary heart disease, and cerebrovascular disease. For this reason, the WHO promotes the use of clean technologies such as solar energy, electricity, petroleum gas, natural gas, alcohol fuels, and improved cookstoves to reduce household air pollution and protect health. 2 In Latin America, although renewable energy sources are on the rise, electricity generation from coal-fired increased by 2.6% between 2000 and 2020, and only 46.3% of the rural population in Central America and 23.3% in South America had access to clean cooking fuels by 2022. 3
Cognitive impairment (CI) involves deficits across cognitive domains, including memory, language, attention, executive function, and visuospatial ability. The risk of CI increases with multimorbidity, particularly when mental health and cardiometabolic disorders are present. More recently, CI has been associated with COPD and exposure to indoor air pollution.4,5 In large cohorts from the general population without COPD, after adjusting for several factors, greater indoor air pollution from particulate matter and a higher risk of CI have been demonstrated with the use of biomass fuels for cooking compared with clean fuels.6–10 On the other hand, several studies have described the association between smoking-related COPD and CI. Although various instruments have been used to assess CI in these patients, the MMSE is the most widely used, allowing for comparison between studies. 4 A recent meta-analysis reported a CI prevalence of 20% to 30%, with age, education level, severity of obstruction, arterial oxygen pressure (PaO2), and comorbidities identified as risk factors. 4
CI has a major negative impact on the life of a patient with COPD and has been linked to an increased risk of disability, limitations in activities of daily living, and a greater need for assistance, decreased adherence to treatment and rehabilitation, poor inhalation technique, and, from a motor perspective, alterations in hand function and in the performance of dual tasks.11–14 Although clinical, functional, and tomographic differences have been demonstrated between patients with COPD due to smoking and biomass exposure, 15 CI in COPD patients exposed to wood smoke and its association with the severity of obstruction or the level of hypoxemia have not been previously evaluated.
Considering that at high altitude there is greater hypoxemia both at rest and during exercise in patients with COPD, 16 that hypoxemia has been suggested as an important factor related to CI and that there are no studies on the association of CI in COPD with exposure to wood smoke, we designed this study in patients with stable COPD living at high altitude to establish the prevalence of CI and its associated factors, particularly the exposure to wood smoke as one of the most widely used types of biomass worldwide.
Materials and methods
A cross-sectional analytical study was conducted in patients with stable COPD residing at high altitude (Bogotá, Colombia, 2,640 m above sea level) who attended a respiratory reference center (Fundación Neumológica Colombiana). The study was approved by the Institutional Research Ethics Committee (Approval Document No. 201508-21201), and participants signed informed consent forms.
Population and groups by exposure
We included consecutive patients residing at high altitude with COPD, defined by a post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio < 0.70 and clinical stability over the previous 8 weeks. We used a respiratory questionnaire with questions about WS exposure and smoking history: “Have you ever used wood for cooking habitually?” and “If yes, for how many years? To establish WS exposure as a risk factor for COPD, we followed the methodology of previous epidemiological studies, which used a cutoff of ≥10 years of WS exposure as a reasonable threshold for distinguishing COPD risk.17,18 Smoking amount was calculated in pack-years based on self-reported information on tobacco duration and amount consumed. Patients were classified according to COPD exposure risk factors as: 1) Wood smoke COPD group (W-COPD): exposed to wood smoke for ≥ 10 years and with a smoking history of < 10 pack-years; 2) Tobacco COPD group (T-COPD): smoking history of ≥ 10 pack-years and exposure to wood smoke for < 10 years; 3) Combined group (T&W COPD): exposed to both factors: wood smoke for ≥ 10 years and smoking history of ≥ 10 pack-years.
Measurements
Clinical variables: Age, anthropometric variables, educational level, Charlson comorbidity score, 19 degree of dyspnea according to the Medical Research Council scale, inhaled treatment, and number of exacerbations in the previous year were recorded for all patients.
Pulmonary function tests: Spirometry and carbon monoxide diffusion (DLCO) were performed on a V-MAX 229d (Sensormedics Inc., Yorba Linda, CA, USA) according to American Thoracic Society and European Respiratory Society standards,20,21 and GLI reference equations were used.22,23 The 6-min walk test (6MWT) was performed following the recommendations of the European Respiratory Society (ERS) and the American Thoracic Society (ATS), 24 and the reference equation derived from healthy subjects at high altitude was used. 25
Cognitive impairment: It was assessed using the validated Spanish version of the Mini-Mental State Examination (MMSE), a screening test that evaluates orientation, registration, attention, calculation, memory, and language. CI was defined as a score of 27 or less.26,27
Statistical analysis
The normality of variables was assessed using the Kolmogorov-Smirnov test. Continuous variables were expressed as mean ± standard deviation (SD) or median and interquartile ranges, and qualitative variables as proportions. For all analyses, CI was treated as a dichotomous variable using the recommended cutoff. To assess differences in continuous variables between groups with and without CI, the unpaired t-test or the Mann-Whitney test was used; for qualitative variables, the chi-square test was used.
The association between CI and the variables of interest was examined using a multivariate logistic regression model. Variables were selected using a purposive approach. Variables considered a priori clinically and biologically relevant, as well as potential confounders identified in the previous literature, were included. In addition, candidate variables showing an association with CI at p < 0.20 in the univariable analysis were considered for inclusion, following the approach described by Hosmer and Lemeshow. Crude and adjusted odds ratios (ORs) with their corresponding 95% CIs were calculated. SPSS 25.0 statistical software was used for analysis. There was no missing data for the variables included in the analysis. This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Results
Clinical and functional characteristics of COPD patients with and without cognitive impairment.

CI: Cognitive impairment; (-): Without CI; (+): With CI; BMI: Body Mass Index; SABA: short-acting bronchodilator; SAMA: short-acting anticholinergic; LABA: long-acting bronchodilator; LAMA: long-acting anticholinergic; ICS: Inhaled corticosteroid; FVC: Forced Vital Capacity; FEV1: Forced expiratory volume in the first second; DLCO: Carbon Monoxide Diffusion; 6MWT: 6-minute walk test; PaO2: Arterial oxygen pressure; PaCO2: Arterial carbon dioxide pressure, SpO2: Pulse oximetry oxygen saturation.
Compared to patients without CI, the most frequent risk factor for COPD in patients with CI was exposure to wood smoke (p<0.001). These patients with CI were also older (p=0.017), had a lower level of education (p=0.007), lower PaO2 (p=0.032) and DLCO (p=0.036), and walked fewer meters in the 6MWT (p=0.007). No differences were observed between these groups in sex, comorbidities, dyspnea, exacerbations in the previous year, inhaled treatment, or severity of obstruction on spirometry (Table 1).
Univariate analysis for cognitive impairment.
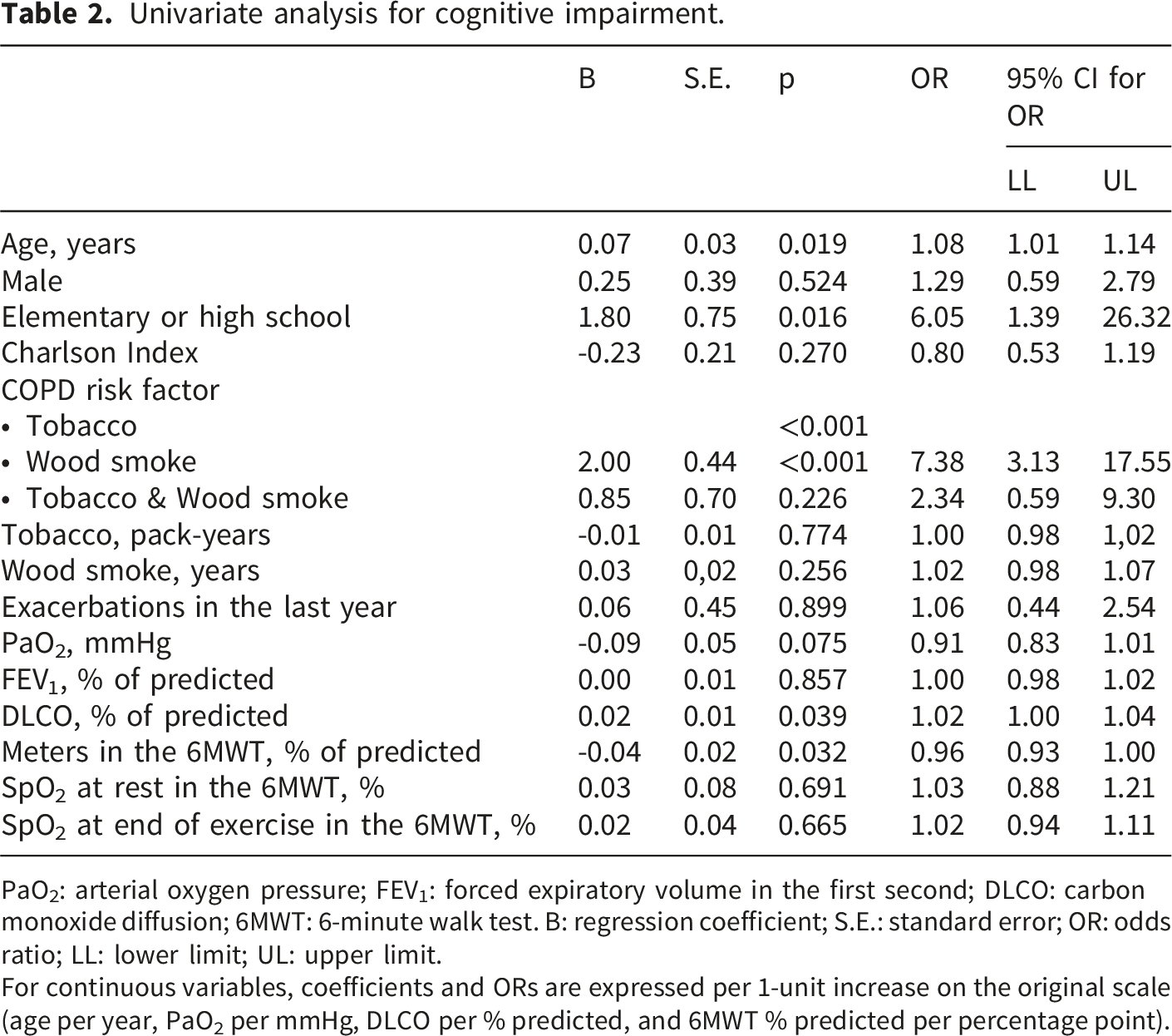
PaO2: arterial oxygen pressure; FEV1: forced expiratory volume in the first second; DLCO: carbon monoxide diffusion; 6MWT: 6-minute walk test. B: regression coefficient; S.E.: standard error; OR: odds ratio; LL: lower limit; UL: upper limit.
For continuous variables, coefficients and ORs are expressed per 1-unit increase on the original scale (age per year, PaO2 per mmHg, DLCO per % predicted, and 6MWT % predicted per percentage point).
Multivariate analysis for cognitive impairment.

Hosmer and Lemeshow Test Chi-square = 9,652 (p=0.290).
PaO2: arterial oxygen pressure; B: regression coefficient; S.E.: standard error; OR: odds ratio; LL: lower limit; UL: upper limit. For continuous variables, coefficients and ORs are reported per 1-unit increase on the original scale (age per year, PaO2 per mmHg, DLCO per % predicted, and 6MWT % predicted per percentage point).

Odds ratios and confidence intervals of the multivariate model for cognitive impairment. In the multivariate analysis, indoor exposure to wood smoke was significantly associated with CI, with an OR (95% CI) of 4.82 (1.62 - 14.33). PaO2: Arterial oxygen pressure; FEV1: Forced expiratory volume in the first second; DLCO: carbon monoxide diffusion.
Discussion
The main result of this study in patients with mild to moderate COPD living at high altitude was that indoor exposure to wood smoke was strongly associated with CI, independently of age, smoking, educational level, comorbidities, hypoxemia, and lung function. This is a novel finding that, to the best of our knowledge, has not been described.
The relationship between smoking-related COPD and cognitive impairment (CI) has been extensively studied. In studies that primarily used the MMSE to assess CI, several risk factors, including chronic hypoxemia, age, low educational attainment, lung function, and comorbidities, were associated with CI.4,28,29 Hypoxemia has been considered a significant contributing factor associated with CI in these patients.13,30 Low oxygen saturation has been associated with a higher risk of CI when measured with the MMSE, and conversely, regular use of supplemental oxygen therapy has been associated with a lower risk of CI. 31 Furthermore, a meta-analysis demonstrated a negative correlation between cognitive function and PaO2 in patients with COPD. 32 Despite these results, CI can occur without chronic hypoxemia, so its presence does not fully explain CI in patients with COPD. 33 This is consistent with our study, in which PaO2 or SpO2 at rest and during exercise were not associated with CI, even though these patients living at high altitude are exposed to more severe chronic hypoxemia than at sea level. In addition, it is known that CI is significantly associated with small vessel disease of the brain, and in COPD there are several mechanisms, beyond hypoxemia, that relate to vascular disease, including oxidative stress and systemic inflammation,33,34 which implies a multifactorial etiology of CI in COPD.
Remarkably, the risk factor identified for CI in COPD patients in our study was exposure to indoor wood smoke, which has previously been linked to cognitive decline in several studies conducted in the general population without COPD. In large cohorts and after adjusting for several factors such as comorbidities, educational level, alcohol consumption and age, a higher risk of CI has been demonstrated with the use of biomass fuels for cooking compared with the use of clean fuels,6–10,35 risk that decreases when switching from biomass to clean fuels 9 and in households with a separate kitchen. 36 This association has also been found in children with prenatal exposure to air pollutants37,38 and children exposed to biomass fuels, in whom alterations in neuropsychological development have been described.39,40
Household air pollution is a mixture of several pollutants, including particulate matter (PM), carbon monoxide (CO), nitrogen dioxide, and volatile organic compounds; among these, the most studied are PM 2.5 (PM2.5) and CO. 41 PM2.5 exposure has been linked to cataract, COPD, ischemic heart disease, lower respiratory infections, stroke, lung cancer, and type 2 diabetes. 41 CI associated with indoor air pollution from biomass fuel use may be primarily associated with exposure to particulate matter (PM). A significant increase in PM levels has been observed in homes that use biomass fuel for cooking, especially when stoves are located indoors, compared with homes that use clean fuels. 42 Similarly, in homes that use firewood as fuel, significantly high levels of CO and PM2.5 have been described. 40 In addition to epidemiological studies linking cognitive impairment to high PM levels from indoor air pollution due to biomass fuel use, anatomical changes in the brain have also been demonstrated. Magnetic resonance imaging studies have shown that the prevalence of ischemic gliotic foci is almost 8 times higher in subjects with a history of exposure to biomass smoke than in subjects without exposure (81.2% vs 11.5%), suggesting that indoor air pollution could influence some clinical outcomes, such as the risk of headache and brain injury. 43 Additionally, in vivo studies have implicated the biomass smoke in the induction of oxidative stress, brain inflammation, disruption of the blood-brain barrier, and disruption of key proteins associated with neurodegenerative diseases. PM containing polycyclic aromatic hydrocarbons is also known to alter neurotransmitter signaling, enhance proinflammatory responses, and disrupt neurodifferentiation processes in neuronal cells. 44
The prevalence of CI in our patients (16.1%) was lower than that reported in several studies in smoking-related COPD, despite their significant hypoxemia, which supports the conclusion that chronic hypoxemia in these patients residing at high altitude did not influence CI. It should also be noted that prevalence estimates across studies and meta-analyses vary widely, attributable to population heterogeneity in COPD diagnostic criteria and disease severity, age, lifestyle, and comorbidities, as well as to methods for identifying cognitive impairment that varied across studies.4,5 We did not find age or sex to be risk factors for CI, consistent with a previous meta-analysis. 28 Although we found no relationship between comorbidities and CI, our patients had few comorbidities and a low Charlson index, which may explain this finding.
We emphasize that this is the first clinical study to associate CI with COPD patients exposed to biomass, using a multivariate model that adjusts for variables related to CI, such as comorbidities, age, and educational level, and that examines chronic hypoxemia, which has previously been implicated as a risk factor for this condition. Additionally, we highlight the significant sample size, the fact that it was conducted at high altitude in patients chronically exposed to hypoxemia, and the comprehensive functional assessment using arterial blood gases, DLCO, and 6MWT. This study contributes to the epidemiology of wood smoke COPD and aligns with the WHO guidelines to promote the use of clean technologies to reduce domestic air pollution and protect health.
Our study has several limitations. The MMSE is a screening test that does not thoroughly assess all cognitive domains, is influenced by respondents’ age and educational level, performs less well in cases of mild cognitive impairment, and its translations are not always interchangeable across cultures. Despite these limitations, the MMSE has become a widely used standard tool for cognitive assessment in elderly patients in clinical practice and is frequently used in patients with COPD. 4
The lack of association between years of WS exposure, treated as a continuous variable, and CI could be explained by the imprecise quantification of the exposure. 5 While previous studies show that years of exposure to wood smoke are a useful measure for estimating the risk of developing COPD, this assessment of solid fuel exposure may not accurately reflect the magnitude of the risk associated with other health impacts, such as CI, which could limit the interpretation of results and comparisons across studies. 5 Because biomass is used as a cooking fuel, exposure to smoke in homes often begins at a young age, which could have a greater impact on health. However, we lack detailed information on the age at which this exposure begins and ends. Another limitation was the inclusion of a small number of patients with more severe obstruction, which limits the generalizability of our results to this group.
Conclusions
In patients with COPD, regardless of hypoxemia, age, smoking status, educational level, comorbidities, or lung function, exposure to wood smoke was associated with CI, suggesting an association between CI and indoor particulate matter or gases.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministerio de Ciencia, Tecnología e Innovación.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.