
Abstract
This systematic review aims to examine the use and usability of continuous glucose monitoring (CGM) among older adults with type 2 diabetes mellitus. The following databases, PubMed, Embase, and CINAHL, were searched for studies published between 2019 and 2024, and results were documented using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist. Eligibility criteria included English-language studies that researched the use and usability of CGM in adults 60 years or older with a minimum wear time of 2 weeks. We extracted usability (efficiency, effectiveness, and satisfaction) outcomes. Study quality was assessed using the Critical Appraisal Skills Program Checklist. Of the 118 identified titles, 58 articles underwent a full-text review, with seven being included in the final analysis. Studies evaluated clinical management of type 2 diabetes with CGM, assessing the following differences: CGM versus usual care, CGM across device types, and CGM across care models. Clinical effectiveness, based on glycated hemoglobin and time-in-range, and satisfaction were higher across CGM types compared with usual care. Based on descriptive measures, satisfaction was higher with real-time CGM than professional-mode CGM. Efficiency findings were not reported in the included studies. There were no findings on the effectiveness, efficiency, and satisfaction of ambulatory glucose profile (AGP) metrics. Although the clinical effectiveness of CGM among adults 60 years or older was demonstrated in the reviewed studies, our usability assessment is inconclusive. There is a gap in evidence related to the essential components that comprise the context of CGM use, which prohibits a complete usability assessment. Future studies are warranted to investigate CGM usability, emphasizing AGP metrics, to inform improvements and personalization for older adults.
Keywords
Introduction
Type 2 diabetes mellitus is a significant health burden around the world, affecting over 500 million older adults and 16.5 million only in the United States, with estimates that the prevalence of diabetes will increase from 5.9% in 2021 to 9.5% in 2050, accounting for more than 1.27 billion older adults.1,2 Older adults (defined in this study as individuals age 60 and above) diagnosed with type 2 diabetes are confronted with unique challenges related to disease progression and an elevated susceptibility to hypoglycemic events,3–5 which may increase the risk of mechanical falls, greater glycemic variability, and mortality.6,7 More so, older adults with diabetes and cognitive impairment may respond inadequately to warning symptoms of hypoglycemia due to reduced awareness.8–10
To manage type 2 diabetes, continuous glucose monitoring (CGM) has emerged as a promising intervention, 11 allowing for minimally invasive measurements of real-time glucose patterns via a subcutaneous sensor. Although glycated hemoglobin (HbA1c or A1c) has been the standard for assessing long-term glycemic management, it does not necessarily reflect glucose variability nor replace the need for self‐monitoring.12–14 For older adults, particularly those with cognitive impairment or dexterity issues, self-monitoring of blood glucose could be challenging. 15 Unlike self-monitoring of blood glucose, which provides snapshots of glucose levels at specific times, CGM continuously measures glucose levels, including fluctuations that infrequent finger pricks might miss. CGM detects a higher number of hypoglycemic events than self-monitoring of blood glucose, especially nocturnal events, which go unnoticed. 15 The ambulatory glucose profile (AGP) that derives from CGM enables patients, caregivers, and health care providers to make personalized interventions in diabetes management. The AGP report has 10 standard metrics, including data completeness; relevant statistics such as incidence of hypoglycemia and hyperglycemia; the depiction of glucose profiles based on a “summary day” (sometimes also called the AGP); a “glucose management indicator”; and daily glucose profiles.16,17 These CGM data can inform treatment decisions, improve medication regimens, and promote the adoption of lifestyle habits aimed at enhancing glycemic management and reducing hypoglycemic episodes.15,18,19
Published in 2019, systematic and narrative reviews provided evidence of CGM’s clinical effectiveness, efficacy, and acceptability among the general adult population with type 2 diabetes.15,20 In younger populations, CGM contributed to improved self-management behaviors, enhanced glycemic management, and effective reductions in A1c levels.21,22 Moreover, younger populations reported barriers to CGM satisfaction, including alarm fatigue, pain, cost, and technology issues, invoking future studies to identify human factors that influence CGM use. 20 Recent studies have demonstrated the importance of focusing on adults 60 years and older because type 2 diabetes management becomes more complex and individualized. 23 The burden of diabetes, multimorbidity, and age-related physiological changes increases with age, 24 as do the rates of severe hypoglycemic events.4,5 Thus, CGM expectations would adjust to aid therapeutic goals for older adults, which include management of hyperglycemia, minimizing hypoglycemia risk, preserving function, and managing polypharmacy. 15 In 2024, a systematic review of older adults with type 2 diabetes using different CGM types reported reductions in HbA1c; however, no impact on hypoglycemia and increased risk of adverse events were also reported. 25 As advancements in CGM become more accessible and available to older adults with type 2 diabetes, evaluating the use of CGM is critical for identifying barriers and facilitators for this population. 26
To extend the benefits to older adults with type 2 diabetes, the implementation of CGM must consider the unique abilities and limitations for these individuals and their caregivers. 27 Usability studies go beyond clinical effectiveness to include efficiency and satisfaction, considering the interactions of elements comprising the context of use and intended objectives (Fig. 1). The International Standard Organization defines usability as “the extent to which specified user can use a product to achieve specified goals with effectiveness, efficiency, and satisfaction in a specified context of use.” 28 As illustrated in Figure 1, CGM is the specified product (or intervention) with the specified goal of managing type 2 diabetes. The specified users are older adults with type 2 diabetes and clinicians. The context of use specifies the users, their tasks, the available tools and technology, and the environments in which CGM use occurs. The operationalization of this definition of usability enables the assessment of CGM effectiveness, efficiency, and satisfaction among older adults. Results from similar assessments in health care and other domains have informed new designs and improved health care delivery associated with better patient outcomes. 29
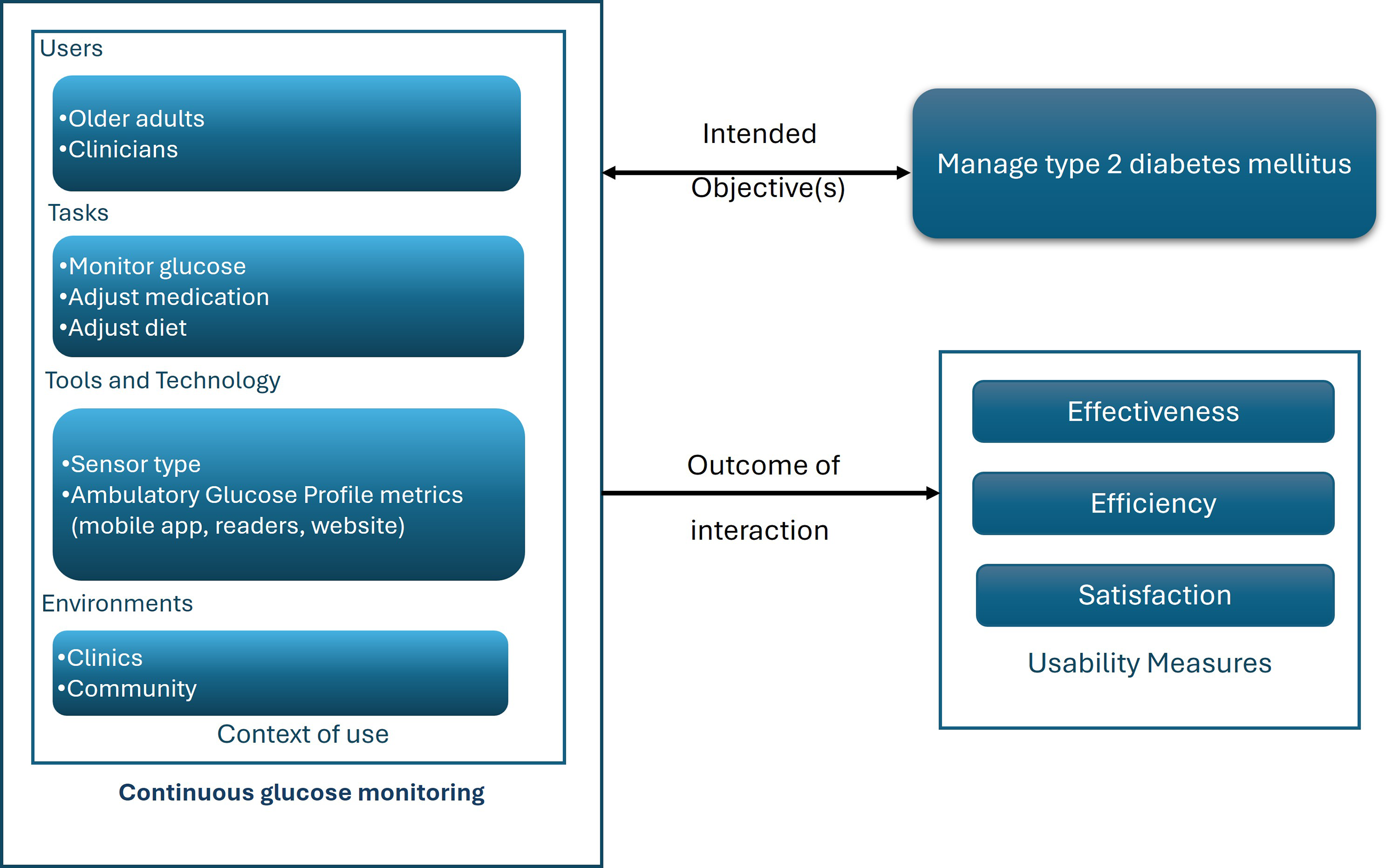
ISO/DIS 9241–11.2 usability definition adapted to CGM for older adults. 33 CGM, continuous glucose monitoring.
Recent systematic reviews of the literature have illustrated advancements in CGM technology for the general adult population with type 2 diabetes,24,25,29 specifically the evolution of real-time sensors, applications, and the availability of CGM data, and have highlighted shifts in health practice and policy. However, existing reviews have focused on clinical effectiveness, with a limited focus on usability and even less on older adults.15,26,30,31 This systematic review aims to characterize published findings of CGM usability among older adults with type 2 diabetes.
Materials and Methods
This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist (see Supplementary Data). A protocol is publicly registered on Open Science Framework. 32
Search strategy
In February 2024, we searched the PubMed, Embase, and CINAHL databases for studies published since January 1, 2019. A lower “limit” of 2019 was selected to identify articles published during a recent period of significant changes in CGM health policy and technology, and to build on existing literature already identified in prior reviews.24,26,29 Bibliographies from four published reviews were used to find additional eligible studies.24–26,29 We also searched these databases in May 2024 and December 2024 using two updated search terms, “AGP” and “ambulatory glucose profile.” The final search phrase is the following: (((CGM) OR (FGM) OR (Flash glucose monitoring) OR (Continuous glucose monitoring)) AND ((elderly) OR (older) OR (aged)) AND ((feasibility) OR (acceptability) OR (usability) OR (user engagement) OR (effectiveness)) AND ((ambulatory glucose profile) OR (AGP))). For this review, “older” participants are defined as individuals aged 60 years or older.
Study selection
Two authors independently screened titles and abstracts using Covidence following a systematic search. If the age range or mean age of the study population was not available in the abstract, the full text of the article was reviewed to determine the age. Studies were excluded at the full-text screening stage if at least two reviewers agreed that the eligibility criteria below were not met. A third reviewer resolved any discrepancies, which were discussed in weekly meetings. The reviewers’ interrater reliability was assessed using Cohen’s Kappa, resulting in a value of 0.367, indicating fair agreement. The iteration of multiple consensus meetings may have contributed to stronger agreements. The small sample size of articles served as a limiting factor for Cohen’s Kappa, where a few disagreements disproportionately reduced the value.
Inclusion and exclusion criteria
The following criteria were used to determine the eligibility of studies for the review: available in English in full text; most participants were at least 60 years of age, or the study population had a mean age of at least 60 years; most of the study population had type 2 diabetes; study evaluated the use of CGM in the study population for at least 2 weeks; and study evaluated aspects of usability, such as effectiveness, efficiency, and satisfaction.
Exclusion criteria were the following: systematic reviews, abstracts, conference presentations, and case studies; interventions whose primary outcome was not related to the CGM sensor; and studies of CGM in a nondiabetes-related context (e.g., diet- or exercise-focused interventions with CGM performed as secondary outcomes, assessed in acute care or hospital settings).
Data extraction
An independent reviewer extracted relevant data from eligible articles using the method used in a previously published review of human factors of CGM. 24 The following information was included: study population, study design, and reporting features related to CGM usability, CGM type, and quality appraisal. Following initial data extraction, one of the two remaining reviewers independently cross-checked the extracted data, which were tabulated, to ensure accuracy and consistency. Inconsistencies were discussed in weekly meetings until consensus was reached. Extracted data were stored on a secure online shared network accessible only to the three reviewers.
Study quality assessment
The quality and risk of bias in included articles were assessed using the Critical Appraisal Skills Program (CASP) checklist for randomized controlled trials (RCT), cohort studies, and cross-sectional studies, as appropriate. 34 A single independent reviewer initially marked relevant areas of the checklist for each included article. Following individual assessment, a more senior researcher reviewed the initial quality appraisal. Over several weeks, consensus meetings were held between the two reviewers to discuss study elements and reach an agreement on the methodological soundness of each article.
Usability metrics
In this review, the three primary measures of usability—effectiveness, efficiency, and satisfaction—were used, with their definitions tailored to specifically apply to type 2 diabetes management. 35 Effectiveness was defined as the extent to which individuals with type 2 diabetes or clinicians achieve care goals for diabetes management. Efficiency was defined as the ease with which older adults or clinicians achieved care goals for type 2 diabetes management. Satisfaction was defined as the level of comfort or acceptability older adults and clinicians had with CGM.
Data and resource availability statement
All data generated or analyzed during this study are included in the published article (and its Supplementary Data).
Results
Of the 118 titles and abstracts screened for eligibility criteria, 58 articles were selected for full-text review. After the full-text review, 51 articles were excluded; seven articles were included in this systematic review (Fig. 2).
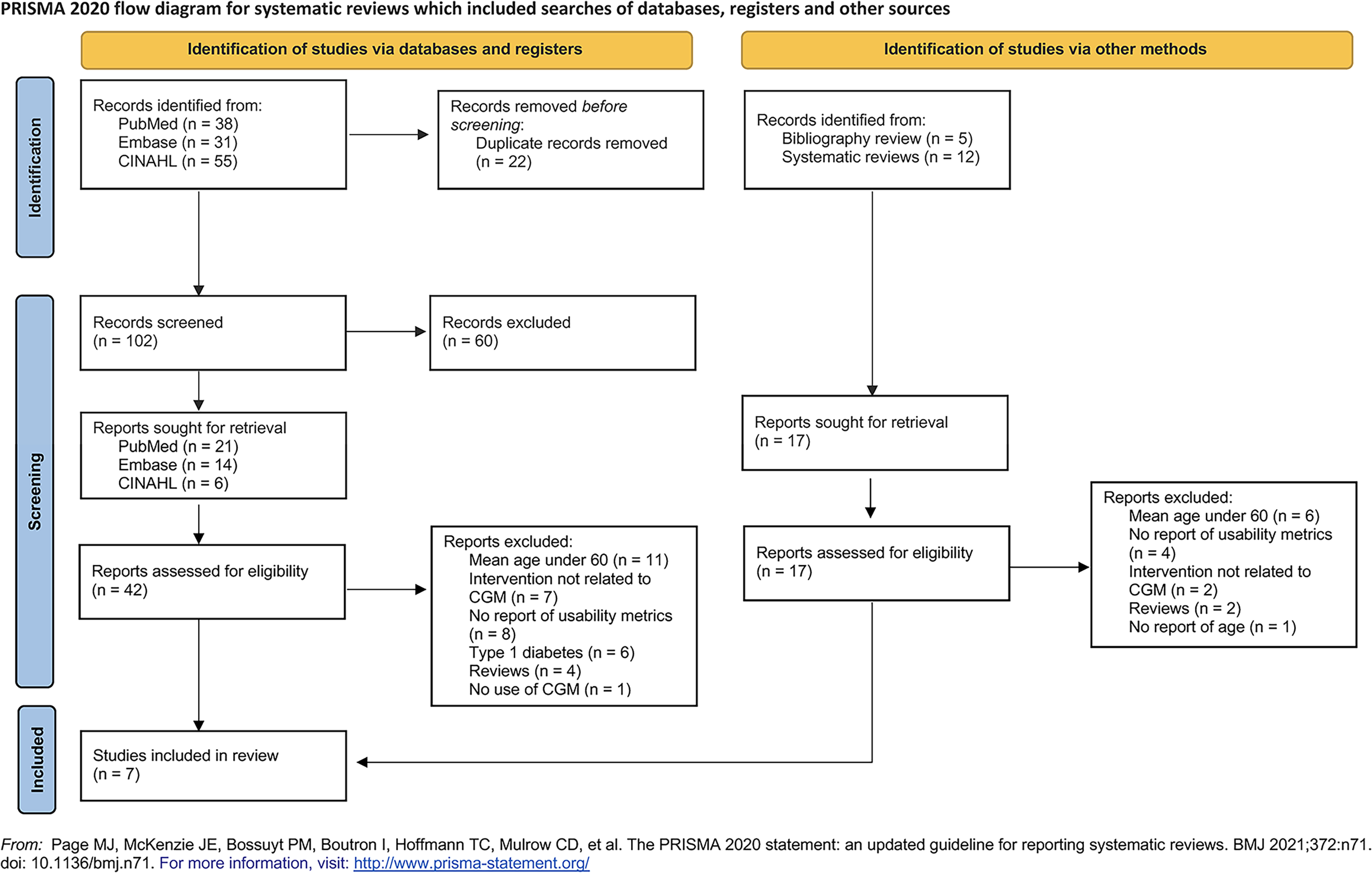
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Population and study characteristics
Among the seven included studies, the mean age of the older adults was reported as participants ranged from 60 to 69 years (Table 1).36–42 Conducted across five countries, the study objectives focused on the effectiveness and satisfaction with CGM. Among the reviewed studies, three main comparisons were made: CGM versus usual care,36,39,42 CGM across device types (professional mode vs. real time),40,41 and CGM across care models (peer support model, nurse or diabetes educator-led model, and physician-led model).37,38 Of the seven articles, 86% (six of seven) of studies blinded all or some of the participants from AGP metrics for a portion or full duration of the study period.36–41 RCTs were reported for 57% (four of seven) of the included studies. Based on the CASP checklist, the included articles were considered methodologically sound (Supplementary Table S1).
Population and Study Characteristics of Included Articles for Older Adults with Type 2 Diabetes
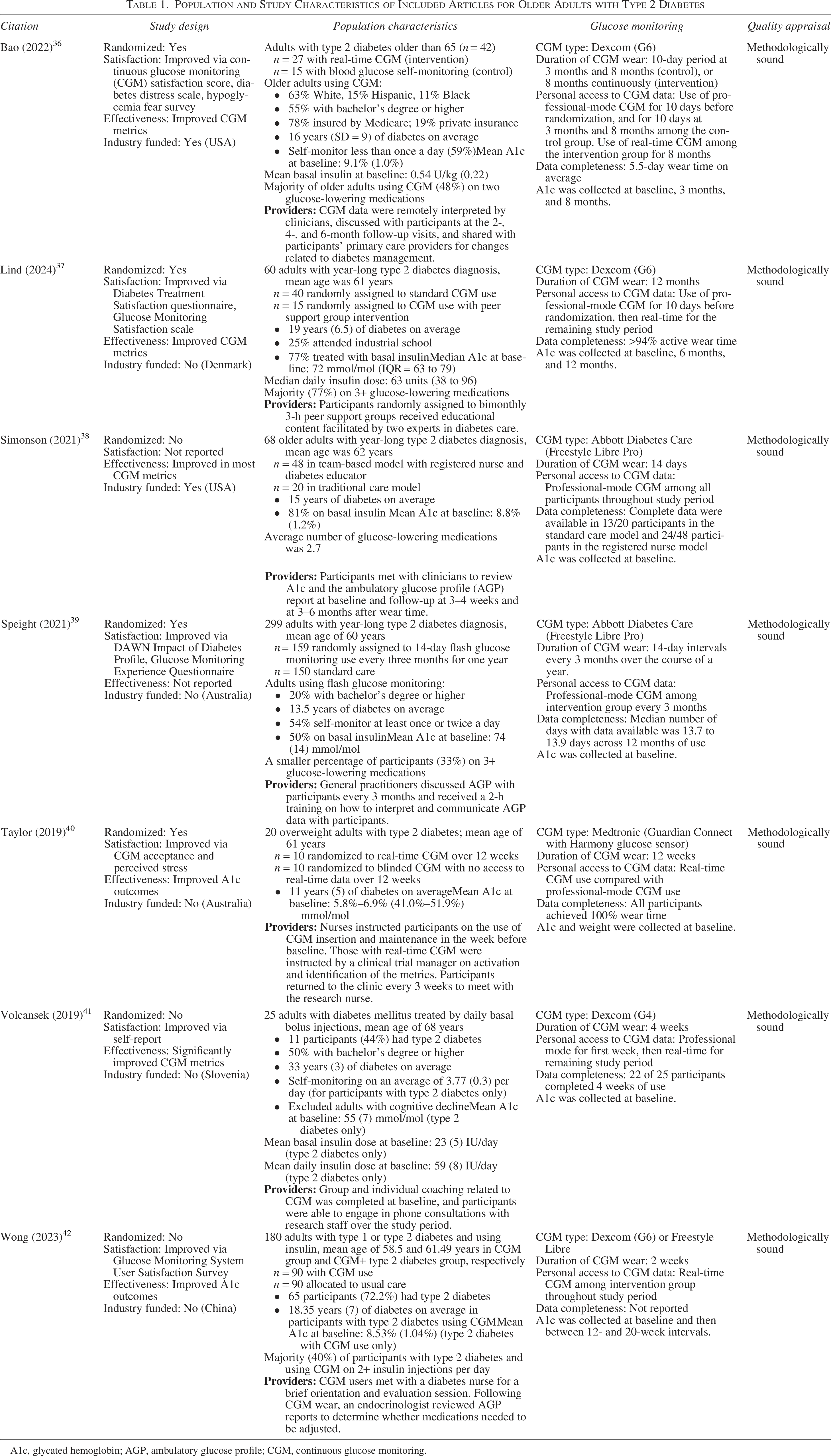
A1c, glycated hemoglobin; AGP, ambulatory glucose profile; CGM, continuous glucose monitoring.
Usability outcomes
CGM effectiveness, efficiency, and satisfaction assessments varied across studies (Table 2). Overall, CGM was reported to be more effective than usual care (77%, 10 of 13 evaluations). Findings also demonstrated higher satisfaction measures for CGM than usual care (86%, 6 of 7 evaluations). Among the reviewed studies, there were no findings related to the efficiency of CGM.
Measures of Effectiveness, Efficiency, and Satisfaction Across Included Articles
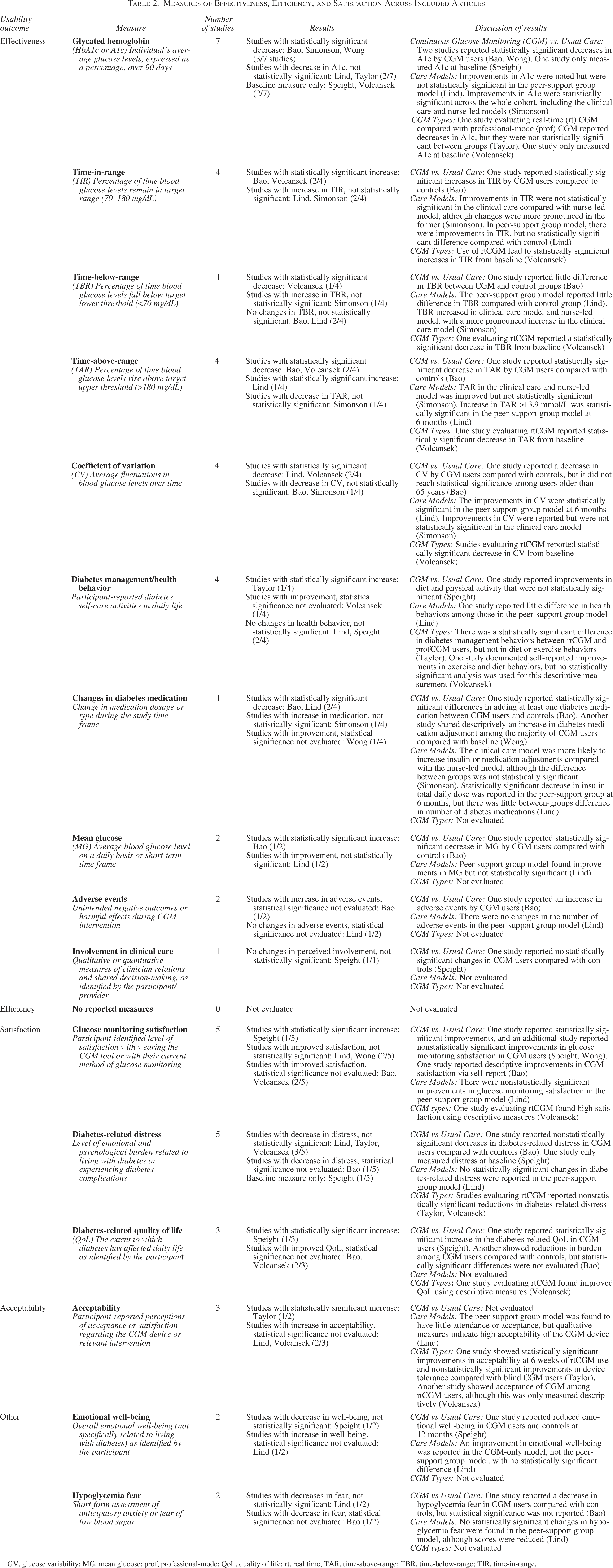
GV, glucose variability; MG, mean glucose; prof, professional-mode; QoL, quality of life; rt, real time; TAR, time-above-range; TBR, time-below-range; TIR, time-in-range.
Within the included studies, there were 36 evaluations of effectiveness measures, of which 42% (15 of 36) showed statistically significant results. Although three of 20 evaluations demonstrated statistically significant results for satisfaction, 80% (16 of 20) also described improved satisfaction with CGM use. There were no evaluations of efficiency measures. For a complete description of the effectiveness and satisfaction per included article, see Supplementary Table S2.
Effectiveness
Ten measures of effectiveness were reported across the studies, including A1c, time-in-range, time-below-range, time-above-range, and glycemic variability.36–38,41 In three studies, type 2 diabetes management with CGM resulted in statistically significant reductions in A1c.36,38,42 Comparing CGM types, eight effectiveness measures were reported.40,41 A1c and time-in-range were the most commonly measured parameters. No significant differences in A1c values were reported between real-time and professional-mode CGM use (only clinicians could see the data).40,41 However, one study found significant increases in time-in-range with real-time CGM (users could see the data). 41 Comparing CGM effectiveness across care models, there were improvements in A1c and time-in-range; however, the differences were not significant between clinician-supported models or peer-supported models.37,38 In addition, six studies reported changes in diabetes management behaviors and adjustments in insulin or diabetes medication among their study population.36–40,42
Efficiency
The impact of CGM on efficiency in type 2 diabetes management is not consistently addressed in the studies reviewed. Although efficiency measures were not explicitly described, the lack of integration of AGP metrics into the electronic health record was reported as a clinical workflow barrier. 38 In the included studies, clinicians mainly uploaded the sensor output sent by older adults in person or via mail,38,39 or received CGM data via wireless Bluetooth transmission. 36 In these cases, clinicians reviewed and discussed the sensor data and AGP report with participants at follow-up visits, occurring at variable time intervals after sensor placement. Researchers suggested that therapeutic inertia and degradation of glycemic impact over time could be prevented with workflow optimization. 38 Furthermore, Speight et al. noted a reduced uptake of AGP training by clinicians who were unfamiliar with AGP or lacked experience in interpretation. 39
Satisfaction
Six of seven articles reported older adults’ satisfaction with using CGM.36,37,39–42 Satisfaction measures were predominantly descriptive. None of the reviewed studies evaluated clinicians’ satisfaction with the CGM. Only differences in satisfaction and quality-of-life scores among flash-CGM intervention participants in an RCT, 39 and acceptability scores after 6 weeks of real-time CGM use, 40 were significant compared with control groups. Studies reported trends of reduced diabetes-related distress,36,37,40,41 reduced CGM-related general chronic stress for older adults, 40 and increased diabetes-related quality of life. 39 There were few differences in quality of life or perceived stress scores between comparison groups.39,40 Older adults randomized to a peer support intervention in addition to CGM (n = 15) were more likely to desire additional education from clinicians on the use of CGM data; all desired to continue using CGM, despite no interest in continuing with a peer support group. 37 Nine of 11 participants with type 2 diabetes using real-time CGM for 3 weeks indicated their desire to continue to use the device after the study. 41
Discussion
This is one of the first systematic reviews of research evaluating the use of CGM and its usability for managing type 2 diabetes in older adults. Similar to existing reviews, our findings support the use of CGM for people 60 years and older based on the overall clinical effectiveness and satisfaction. Yet, this review expounds findings by identifying a critical gap in the literature: measures of efficiency, effectiveness, and satisfaction were not reported for essential elements of the CGM context of use, including the AGP.36,39,42 Early studies compared CGM with usual care.36,39,42 In later studies, we noted a shift in the primary objectives to comparisons of different types of CGM and care models.37,38,40,41 Among later comparisons, few significant differences in outcomes were reported. Based on our review, critical aspects of AGP metrics were understudied.
More than time-in-range: AGP metrics for effectiveness
Although A1c is the established measurement of glycemic management, publications have denoted its limited ability to convey glucose variability. Through CGM, time-in-range and other measures provide additional insight. Various AGP metrics contribute to a comprehensive and useful understanding of type 2 diabetes. Similar to other studies, in this review, the most reported clinical effectiveness measures were changes in A1c and time-in-range.31,43 Time-above-range and time-below-range were evaluated inconsistently. Although AGP metrics vary across manufacturers’ reporting formats, 10 standard metrics are consistently reported in the AGP. 16 For example, the coefficient of variation describes how much glucose levels vary daily. 44 The glucose management indicator estimates an individual’s A1c. 45 Previous studies have demonstrated the value of these AGP metrics, 46 but were rarely reported in the articles included. Three CGM studies did not report any AGP metrics other than the A1c.37,39,42 Future studies are warranted to assess clinicians’ knowledge, interpretation, and use of AGP metrics beyond time-in-range. Although clinician satisfaction with CGM in the management of type 2 diabetes was not reported in the included articles, CGM-integrated workflows could affect clinician-reported CGM satisfaction, efficiency, and effectiveness. A better understanding of the clinicians’ decision-making process may guide advancements in AGP data and improve its ability to support type 2 diabetes management.
Considering CGM’s ability to detect hypoglycemia, few of the included articles examined this feature among adults aged 60 years and older.36,38,41 While time-below-range was mentioned, the AGP reports and other CGM data provide more information on hypoglycemic events, including the number of events, the average duration of these events, and the days or times of events. With this information, clinicians’ awareness of the individual’s hypoglycemic risk can increase, which is important with an older population prone to hypoglycemic unawareness. 47 Future research should investigate the usability of time-below-range metrics for hypoglycemia detection in this target population and clinician response.
Personal access to AGP data: Benefit or burden?
For adults 60 years and older, the introduction of CGM raised concerns of increased stress or burden, such as data overload and alarm fatigue. 48 Consistent with existing studies among younger populations, evidence from the reviewed studies demonstrated that the use of CGM either improved or had no detrimental impact on participants’ general or diabetes-related levels of stress, thus reinforcing the positive value that CGM has on self-reported well-being and quality of life.32,49 While comparisons among care models were similar, 37 comparisons between CGM types demonstrated differences in satisfaction and long-term adoption. 41 In reviewed studies, the number of participants who completed the full intervention protocol with professional-mode CGM, which does not allow personal access to AGP data, reduced progressively after 9 months of use. 39 Access to AGP data is perceived as having value, and the visual display of real-time blood glucose data provides positive reinforcement for participants’ behavior. 14 Future research should investigate whether engagement in self-management induces or leads to CGM satisfaction.
CGM-integrated workflows: Efficient clinician access to data
Although efficiency was not reported as an outcome in the included articles, efficient access to AGP data related to the implementation of CGM in clinical workflows was discussed. 38 The efficiency of AGP interpretation depends on data access, quality, and reliability of collected information, and implementation of a standardized process. 50 One study described barriers to data access and an intervention to overcome them; 38 no study addressed data standardization. Efficient CGM-driven type 2 diabetes management relies on the integration of AGP into clinical workflows; a lack of integration can be challenging due to data overload, increased clinic staff time, and delayed interventions. 51 Efficient CGM-based management of type 2 diabetes relies on clinicians’ adoption of technology education about data access and interpretation and the use of standardized AGP report-based interventions. Evaluating workflows associated with AGP-based self-management in adults 60 years and older could be valuable in enhancing the efficiency of care. Future research is needed to investigate approaches to integrating AGP metrics with electronic health record systems.
Limitations
There are limitations to consider regarding this review. The search strategy may have missed relevant articles. The 2-week minimum CGM requirement may have omitted studies relevant to the study’s topic. Articles selected for review might not reflect all the important findings. Variability in study quality challenges our ability to compare findings meaningfully and limits the validity of our conclusions. Some included studies had small sample sizes or lacked consistent measurement of key outcomes such as AGP and usability, highlighting a gap in CGM usability research for older adults.
Conclusions
Although CGM is effective among adults 60 years of age or older with type 2 diabetes, the determination of CGM’s usability is inconclusive. Little evidence was reported regarding the effectiveness, efficiency, and satisfaction of CGM tools and technology, including those required to use AGP metrics. From both clinician and older adults’ perspectives, these gaps in evidence prohibit assessment of AGP metrics and insights on its use, interpretation, and communication. AGP metrics inform type 2 diabetes management and decision-making. Therefore, a lack of emphasis on AGP metrics beyond time-in-range limits knowledge of how to improve CGM for older adults across various settings, CGM types, and care models. Existing studies do not provide insights into specific data metrics (beyond time-in-range) or visualizations that are helpful for clinicians or older adults. Future research is warranted to investigate the usability of AGP metrics for clinicians and older adults and to assess the potential benefits of enhanced awareness, shared decision-making, and self-management with CGM.
Authors’ Contributions
A.S., C.B., and M.W. were involved in the conception and design of the systematic review. A.S., C.B., and M.R.T. were involved in the conduct of the review and analysis and interpretation of the results. A.S., C.B., and M.R.T. wrote the first draft of the article, and all authors edited, reviewed, and approved the final version of the article.
Footnotes
Author Disclosure Statement
M.W. reports stock holdings in 3M, AbbVie, Amgen, Bristol Myers Squibb, Centene, CONMED, Crispr Therapeutics, Dexcom, DXC Technology, Embecta, GE Healthcare Technologies, Globus Med, GSK, Haemonetics, Integer, Integra Lifesciences, Johnson & Johnson, Medtronic, Novo Nordisk, Orthofix, Pfizer, Revvity, Roche, Stryker, Teva Pharmaceutical Industries, Veradigm, and Zimmer Biomet. The other authors have no competing interests to declare.
Funding Information
A.S. is supported by a Career Development Award from the National Institute on Aging (Award Number K01AG076971).
Disclaimer
The views expressed in this article are those of the authors and do not necessarily represent the views of the U.S. Department of Veterans Affairs or the U.S. government.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.