
Abstract
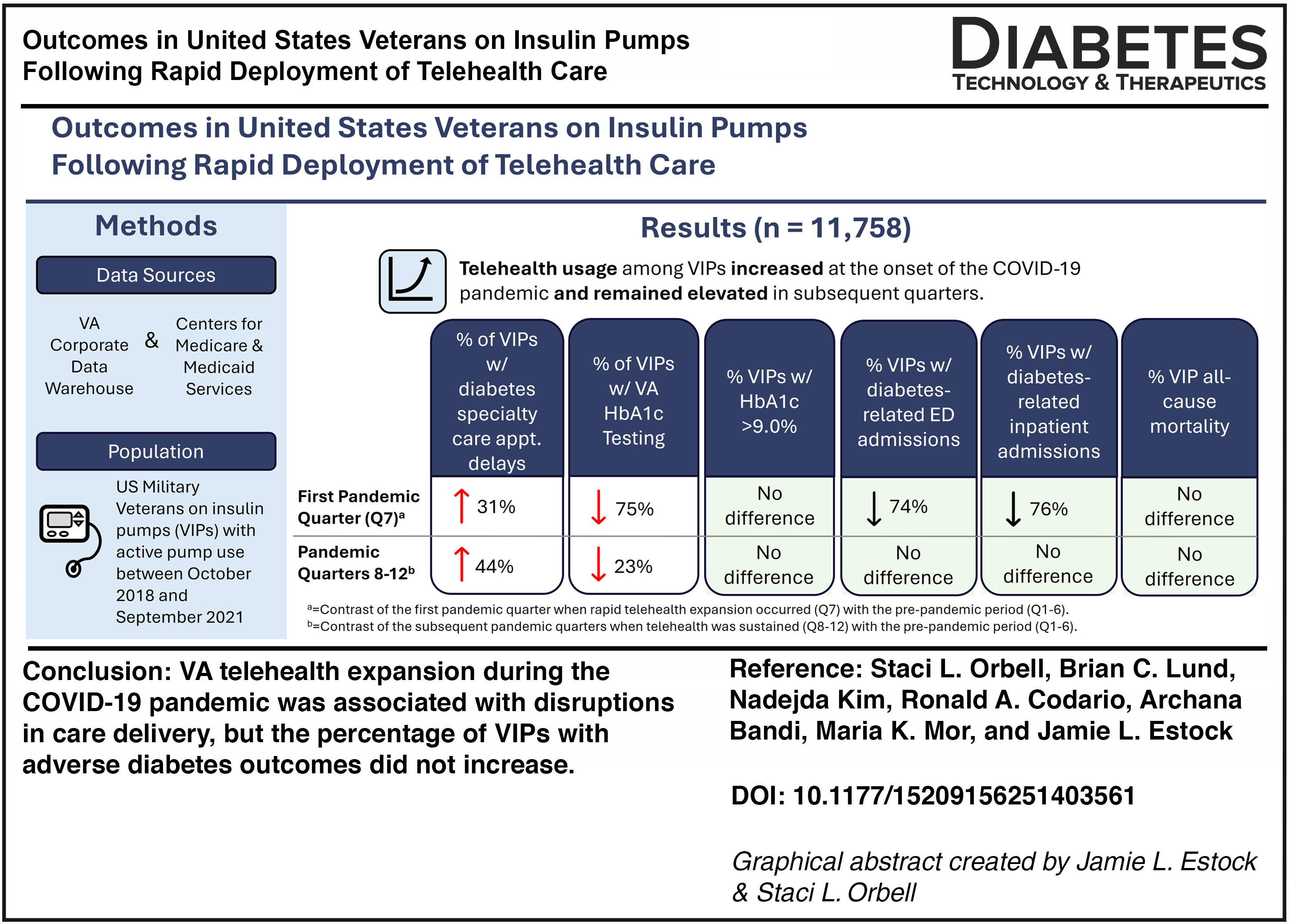
The impacts of the rapid transition to telehealth care among Veterans on insulin pumps (VIPs) at the onset of the COVID-19 pandemic have not yet been studied. We performed a longitudinal analysis of VIP outcomes from October 1, 2018 to September 30, 2021 using mixed effects logistic regression to assess changes in VA care delivery and VIP outcomes. Among 11,758 VIPs, adjusted odds of VIPs experiencing diabetes specialty care appointment delays increased by 31% in the first pandemic quarter and 44% in subsequent pandemic quarters. Adjusted odds of VIPs completing HbA1c testing decreased by 75% in the first pandemic quarter and 23% in subsequent pandemic quarters. No increases were found in the percentage of VIPs with poor diabetes control, diabetes-related emergency department or inpatient admissions, or all-cause mortality. VA telehealth expansion during the COVID-19 pandemic was associated with disruptions in care delivery, but the percentage of VIPs with adverse diabetes outcomes did not increase.
Introduction
Although telehealth is recognized as a safe and effective modality of care for people living with diabetes,1–4 historically, Veterans on insulin pumps (VIPs) were excluded from telehealth programs in the U.S. Department of Veterans Affairs (VA) due to concern that their complex care needs would place considerable strain on telehealth workflows.5,6 At the onset of the COVID-19 pandemic, VA rapidly increased telehealth appointments for all Veterans to maintain access to care while preventing COVID-19 exposure.7,8 This rapid telehealth transition may have been especially challenging for VIPs due to a lack of established best practices for remote insulin pump management. The impacts of this telehealth transition on VIPs have not yet been studied. Thus, the purpose of this study was to explore associations between VA’s rapid telehealth transition during the COVID-19 pandemic and VA care delivery and VIP outcomes.
Materials and Methods
This study was approved by the VA Central Institutional Review Board (1727818). Administrative data from the VA Corporate Data Warehouse (CDW) was the primary source of data for this study. Medicare claims data from the Centers for Medicare and Medicaid Services (CMS) was a secondary source. We used reservoir/cartridge/pod dispensing data found in the outpatient pharmacy database of the VA CDW to identify VIPs and track their longitudinal use of insulin pumps. We determined the manufacturer and model of insulin pump used by each VIP through purchase order data found in the VA prosthetics database. We used VA outpatient encounters to identify diabetes specialty care visits and VA laboratory data to determine completion and results of hemoglobin A1c (HbA1c) testing at a VA facility. Medical comorbidity and diabetes-related emergency department (ED) and inpatient admissions were assessed using VA encounters and supplemented with Medicare claims data and claims for care in the community paid for by VA.
Our 3-year observation period included 12 quarters. The first 6 quarters (Q1–Q6; October 1, 2018 through March 31, 2020), herein referred to as the prepandemic period, occurred prior to the onset of the pandemic. The next 6 quarters occurred after the pandemic onset (Q7–Q12; April 1, 2020 through September 30, 2021). We divided the pandemic period into two phases, the first pandemic quarter (Q7) to examine immediate changes following the rapid telehealth transition and subsequent pandemic quarters (Q8-12) to examine prolonged changes as telehealth practices were sustained.
VIPs were included for a given quarter if they had evidence of recent pump use prior to the first day of that quarter (index date) and prior VA service use. We determined recent pump use (within 45 days prior to index) through longitudinal dispensing records of pump reservoirs/cartridges/pods over the year prior to index, using a cabinet supply approach. 9 We defined prior VA service use as either two VA outpatient encounters, or at least one VA outpatient encounter and at least one VA inpatient admission, in the year prior to index for any condition, including diabetes-related care and nondiabetes care. We applied these criteria independently for each of the 12 quarters of the observation period, where new pump starters were allowed to enter the analysis during the first full quarter following their insulin pump initiation, and those discontinuing pump use excluded in the quarter following discontinuation.
Sociodemographic measures included age, sex, race, ethnicity, rurality, diabetes type, priority group rating, and comorbidity. Priority group ratings range from 1 to 8, based on a Veteran’s income, disability rating, military service, Medicaid eligibility, and other VA benefits, with those in groups 1–3 receiving the highest financial coverage for VA health care. 10 We calculated comorbidity using the Gagne index, a composite measure based on the presence of 20 disease states. 11 Scores range from −2 to 26, with higher values indicating higher risk of mortality. VIP’s diabetes specialty care appointments, which were outpatient encounters to endocrinology or diabetes as coded with VA clinic stop codes 305 or 306, and delivery modality (i.e., face to face [F2F] or telehealth), 7 were captured on a quarterly basis over the observation period.
Primary outcome measures included two VA care delivery outcomes (diabetes specialty care appointment delays and HbA1c testing), and four adverse diabetes outcomes (poor diabetes control, ED and inpatient admissions, and all-cause mortality). For a given quarter, we defined a diabetes specialty care appointment delay as ≥210 days since a VIP’s last prior appointment. HbA1c testing was assessed by the percentage of VIPs completing HbA1c testing at a VA facility during a given quarter. Since strict monitoring every 3 months is not necessarily indicated for all VIPs, we did not expect 100% of VIPs to be tested in each quarter. However, we expected the observed frequency to be consistent across quarters and any meaningful decline would allow us to detect disruptions. We defined poor diabetes control as an HbA1c test value >9.0% observed during a given quarter to align with VA’s internal Electronic Quality Measures and the CMS reporting. 12 We defined diabetes-related ED and inpatient admissions as an ED or hospital admission with an ICD-10 code indicating diabetes short- or long-term complications, as defined by Agency for Healthcare Research and Quality Prevention Quality Indicators (AHRQ PQI), 13 as a principal/primary diagnosis. We determined all-cause mortality through the VA Vital Status file.
We calculated descriptive statistics on sociodemographic measures and diabetes specialty care delivery modality using means for continuous and discrete measures and frequencies for categorical measures. We used mixed effects logistic regression models, with random effects for VA facility and VIP, to examine the associations between the rapid deployment of telehealth care due to the pandemic on VIP outcomes while accounting for the nonindependence of observations from the same VIP and the same VA facility. We created separate models for each primary outcome comparing outcomes from the first pandemic quarter (Q7) with the prepandemic period (Q1–6) to examine immediate changes following the rapid telehealth transition and comparing the subsequent pandemic quarters (Q8–12) against the prepandemic period to examine prolonged changes as telehealth practices were sustained.
We adjusted all models for patient demographics (age, sex, race, ethnicity, and rurality), diabetes type, comorbidity, and VA priority group. Diabetes specialty care appointment delays, poor diabetes control, diabetes-related ED admissions, diabetes-related inpatient admissions, and all-cause mortality models also included the VIPs’ prepandemic telehealth experience (Q1–6) as covariates. We conducted all statistical tests using SAS Enterprise Guide 8.3 9 (Cary, NC) and Stata MP 18 (College Station, TX) and used two-tailed tests with α = 0.05.
Results
We identified 11,758 VIPs for this analysis, the characteristics of whom are described in Table 1. VIPs had a mean age of 58.2 (SD = 14.2) years, with more than half of them being 55 years of age or older (63.1%). The majority of VIPs were white (83.4%) men (91.1%) of non-Hispanic or Latino ethnicity (94.0%). Most VIPs resided in urban areas (64.1%) and were part of VA priority groups 1–3 (75.7%). Almost half of VIPs had a type 2 diabetes diagnosis (46.7%). Overall mortality risk among VIPs was low (median = 1.0). As of the final quarter of our observation period starting on July 1, 2021, 54.4% of VIPs used Medtronic brand insulin pumps.
Characteristics of Veterans on Insulin Pumps Active During Any Quarter, October 1, 2018 and September 30, 2021
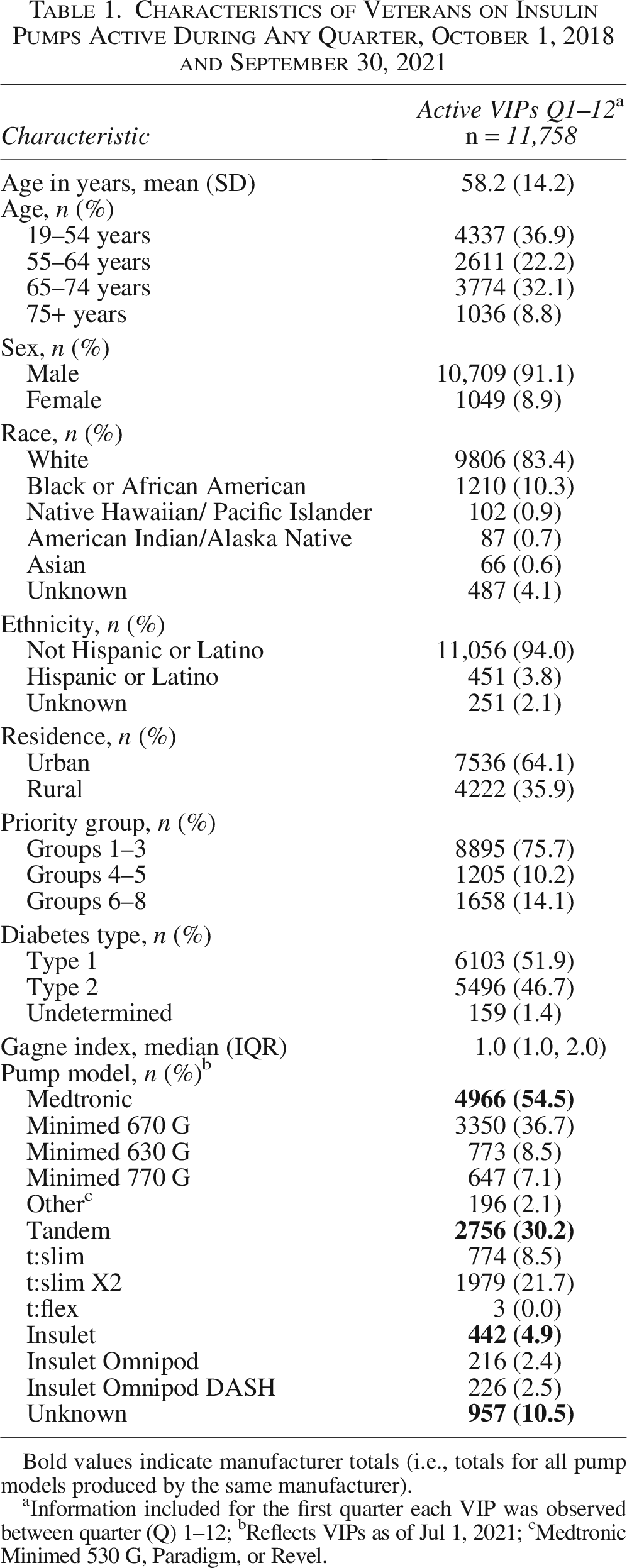
Bold values indicate manufacturer totals (i.e., totals for all pump models produced by the same manufacturer).
Information included for the first quarter each VIP was observed between quarter (Q) 1–12; bReflects VIPs as of Jul 1, 2021; cMedtronic Minimed 530 G, Paradigm, or Revel.
Throughout the observation period, VIPs’ mean HbA1c ranged from 7.7% to 7.8% (Supplementary Data). Table 2 details our study outcomes by quarter and their respective adjusted odds ratios of immediate and prolonged changes. Compared with prepandemic quarters (Q1-6), the adjusted odds of VIPs experiencing diabetes specialty care appointment delays increased by 31% during the first pandemic quarter (Q7; 95% CI: [1.16, 1.47]) and remained 44% higher during the subsequent pandemic quarters (Q8–12; 95% CI: [1.27, 1.64]). Compared with prepandemic quarters (Q1–6), the adjusted odds of a VIP completing HbA1c testing at a VA facility decreased by 75% during the first pandemic quarter (Q7; 95% CI: [0.23, 0.27], and remained 23% lower during the subsequent pandemic quarters (Q8–12; 95% CI: [0.72, 0.82]). Diabetes-related ED and inpatient admissions significantly decreased by 74% and 76%, respectively, during the first pandemic quarter (Q7; 95% CI: [0.21, 0.31] and [0.20, 0.29], respectively). No significant differences were found in the percentage of VIPs with poor diabetes control (OR: 0.88, 95% CI: [0.70, 1.10]) or all-cause mortality (OR: 0.75, 95% CI: [0.51, 1.10]) between the prepandemic quarters (Q1–6) and the first pandemic quarter (Q7). Finally, no significant differences were found in percentages of VIPs with poor diabetes control (OR: 0.84, 95% CI: [0.69, 1.01]), diabetes-related ED or inpatient admissions (OR: 0.89, 95% CI: [0.77, 1.03] and OR: 0.88, 95% CI: [0.76, 1.01], respectively), or all-cause mortality (OR: 1.23, 95% CI: [0.84, 1.80]) between the prepandemic quarters (Q1–6) and the subsequent pandemic quarters (Q8–12).
Outcomes Among Veterans on Insulin Pumps, by Quarter, Between October 1, 2018 and September 30, 2021
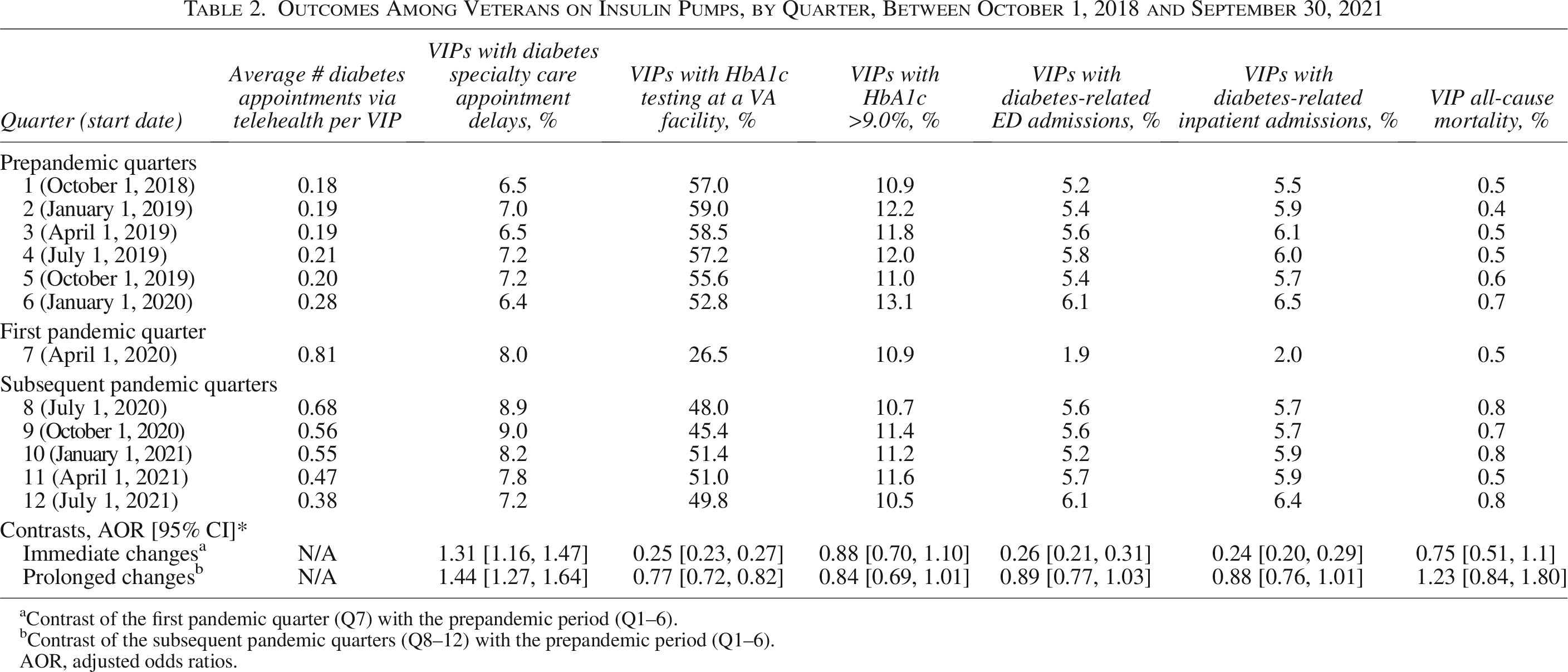
Contrast of the first pandemic quarter (Q7) with the prepandemic period (Q1–6).
bContrast of the subsequent pandemic quarters (Q8–12) with the prepandemic period (Q1–6).
AOR, adjusted odds ratios.
Discussion
We observed immediate changes in VA care delivery outcomes, including increased delays in diabetes specialty care appointments and decreased HbA1c testing, at the onset of the pandemic when VA rapidly expanded telehealth care to VIPs. As the pandemic continued and telehealth care for VIPs was sustained, diabetes specialty care appointment delays decreased and HbA1c testing increased but neither returned to prepandemic levels. However, the percentage of VIPs with poor diabetes control, diabetes-related ED admissions, diabetes-related inpatient admissions, and all-cause mortality did not increase from the prepandemic period to the onset of the pandemic or subsequent pandemic quarters.
Despite rapid expansion of telehealth care for VIPs during the COVID-19 pandemic, 7 delays in diabetes specialty care appointments occurred. The immediate increase in diabetes specialty care appointment delays observed at the onset of the pandemic are likely explained by stay-at-home orders that advised high risk individuals, including people with diabetes, to avoid social interactions. Multiple studies examining the pandemic period have also noted these appointment delays among people with diabetes.14–17 Both the immediate and prolonged increase in diabetes specialty care appointment delays among VIPs may also be attributed to delays associated with implementing new care processes as VA facilities had to create new protocols for how to schedule and conduct VIP follow-up appointments in the telehealth environment with limited best practice examples available.
Likewise, the immediate decrease in the frequency of HbA1c testing at VA facilities observed at the onset of the pandemic may be explained, in part, by stay-at-home orders and the risks of VIPs attending in-person appointments. Other studies involving patients with diabetes have also noted this decrease in HbA1c monitoring.14,17 The prolonged decrease in the frequency of HbA1c testing found in our study may reflect advances in continuous glucose monitoring (CGM) and insulin pump technologies that occurred around the same time as our observation period. Automatic data sharing via smart phone technologies 18 and the emergence of the glucose management indicator 19 metric may have allowed providers to more readily access and analyze CGM data to determine VIP glucose control in lieu of traditional HbA1c testing.
Despite increased specialty care appointment delays and decreased HbA1c testing, the percentage of VIPs with negative diabetes outcomes did not increase during the observation period. This finding aligns with other studies finding no differences in diabetes control compared with prepandemic levels,14,15 as well as studies reporting adequate or improved glucose control for patients receiving telehealth care for diabetes management.2–4 While VIPs adept at their own self-management as well as effective telehealth care may explain stable diabetes outcomes across the observation period, it is important to note that advances in hybrid closed loop algorithms integrated into many insulin pump models coincided with the observation period and thus may have also contributed to the stability and/or improvements in VIPs’ glycemic control. 20
Limitations
There are several limitations to this study. While we supplemented VA health care data with CMS and VA purchased community care data to assess medical comorbidity, care paid for by Veterans out-of-pocket or through employer-based insurance plans and non-VA laboratory testing was not captured. Furthermore, appointment interruptions for VIPs who received diabetes care exclusively through VA primary care were not captured in this study. In addition, the VIP population observed in our study was not identical over time, as such, unmeasured confounders that differed between quarters may also be present. Specific to poor diabetes control, which reflects only those VIPs who completed HbA1c testing at a VA facility in a given quarter, limitations may exist given the precipitous decline in HbA1c testing at the pandemic onset and lower rates in subsequent quarters. This may have introduced selection bias in terms of which patients completed testing over time. The examination of all-cause mortality as an outcome was potentially limited by the impact of COVID-related deaths, but the data source did allow for isolation of diabetes-related mortality. Finally, the COVID-19 pandemic led to operational changes within the VA and broader societal impacts, making it difficult to disentangle telehealth as a discrete factor contributing to study outcomes.
Conclusions
Our findings suggest that even with disruptions in VA care delivery, adverse diabetes outcomes among VIPs did not increase with a switch to telehealth care, a concern that previously limited their access to this care delivery modality. Our findings suggest that care for VIPs via telehealth care is, at minimum, comparable with F2F care in terms of diabetes control, diabetes-related admissions, and all-cause mortality. Further research is warranted to examine VIP outcomes over a longer observation period, particularly as telehealth technologies and processes have rapidly advanced since the study observation period.
Authors’ Contributions
S.L.O.: Formal analysis, Writing—Original Draft, Writing—Review and Editing, Visualization; B.C.L.: Methodology, Formal analysis, Investigation, Data Curation, Writing—Original Draft, Writing—Review and Editing, Visualization; N.K.: Methodology, Formal analysis, Investigation, Data Curation, Writing—Review and Editing, Visualization; R.A.C.: Conceptualization, Validation, Investigation, Writing—Review and Editing; A.B.: Conceptualization, Validation, Investigation, Writing—Review and Editing; M.K.M.: Methodology, Formal analysis, Investigation, Data Curation, Writing—Original Draft, Writing—Review and Editing; J.L.E.: Conceptualization, Methodology, Investigation, Writing—Original Draft, Writing—Review and Editing, Supervision, Funding acquisition.
Footnotes
Acknowledgments
The authors would like to thank Anne Marie Shields for her assistance in managing CMS data and Terrence Litam for his early work in coordinating this study.
Author Disclosure Statement
The authors have no disclosures or conflicts of interest.
Funding Information
This work was supported by Merit Award # I01 5I01HX003581-03 from the United States Department of Veterans Affairs Health Services Research and Development Service. Support for VA/CMS data provided by the Department of Veterans Affairs, Office of Research and Development, VA Information Resource Center.
Disclaimer
The contents of this article do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.