
Abstract

Most continuous glucose monitoring (CGM) systems derive the displayed readings from glucose level measurements in the interstitial fluid (ISF). These CGM readings can be delayed with respect to blood glucose (BG) levels, which is caused by the time it takes for glucose to diffuse from the blood to the ISF, as well as the sensor response time and signal processing algorithms. The resulting time delay between CGM readings and BG levels is an often-reported metric of CGM performance and is partially responsible for the discrepancies of CGM readings when compared with BG concentrations, especially during phases of fast-changing BG levels. 1
In studies evaluating the accuracy of CGM systems, especially for market approval, a well-established practice is to “arterialize” the venous blood before sampling and subsequent comparator BG concentration measurement. 2 This means that the arms of the participants from which venous blood is sampled are heated with a heating blanket or pad throughout the comparator measurement period. The purpose of this arterialization is to reduce the difference between venous and capillary BG concentrations through heat-triggered physiological processes. 3 However, these effects may also lead to an increased diffusion of glucose from the blood to the ISF, which could reduce the physiological component of CGM system time lag, especially when sensors are worn on the heated arm.
Methods and Results
To examine this hypothesis, this article used data from a study with 20 participants with type 1 diabetes. Data from two in-clinic sessions were included in this analysis, where either the dominant or nondominant arm was heated for at least 6 h. This was accomplished by wrapping an electric heating blanket set to 50°C (122°F) around the hand, lower arm, and elbow. Additionally, each participant wore two CGM sensors (FreeStyle Libre 3, Abbott Diabetes Care Inc., Alameda, CA, USA) simultaneously, one on each upper arm (not covered by the heating blanket). Every session thus yielded CGM data from a heated and a non-heated arm. During sessions, moderate to fast BG concentration changes were induced, and BG level measurements were obtained every 15 min from venous samples collected from both the heated and non-heated arms simultaneously using a YSI 2300 STAT PLUS laboratory analyzer (YSI). 3
The 40 in-clinic sessions yielded a total of 156 datasets containing simultaneously collected CGM and BG level data (one session yielded an insufficient number of YSI measurements on both arms). For each of these datasets, time lag, bias, mean absolute relative difference (MARD), and 20% agreement rate (AR20) between CGM readings and comparator measurements were calculated. Datasets were then separated according to the four possible combinations of CGM data and comparator BG levels (sensor from heated arm vs. YSI from non-heated arm, sensor from non-heated arm vs. YSI from non-heated arm, sensor from heated arm vs. YSI from heated arm, sensor from non-heated arm vs. YSI from heated arm). The mathematical approach to estimate the time lag was based on the method proposed by Kovatchev et al. and involved maximizing the agreement between BG measurements and time-shifted CGM data. 4
Summary statistics of datasets for the four possible combinations of CGM data and comparator BG levels are shown in Table 1. The results indicate that, compared to both heated and non-heated YSI measurements, CGM data from sensors worn on a heated arm show a considerably lower time lag than sensors worn on non-heated arms. This finding suggests the presence of an effect of heating on the CGM system time lag, in addition to the known arterialization effect on venous BG concentrations. Data from sensors on the heated arms, when compared to the same YSI measurements, also demonstrated improved MARD and AR20 but similar bias, which could also be explained by the reduced time lag. However, CGM accuracy was generally higher against YSI measurements from the heated arms due to a lower bias, as already described previously. 3
Summary Statistics of Time Lag and Various Accuracy Metrics
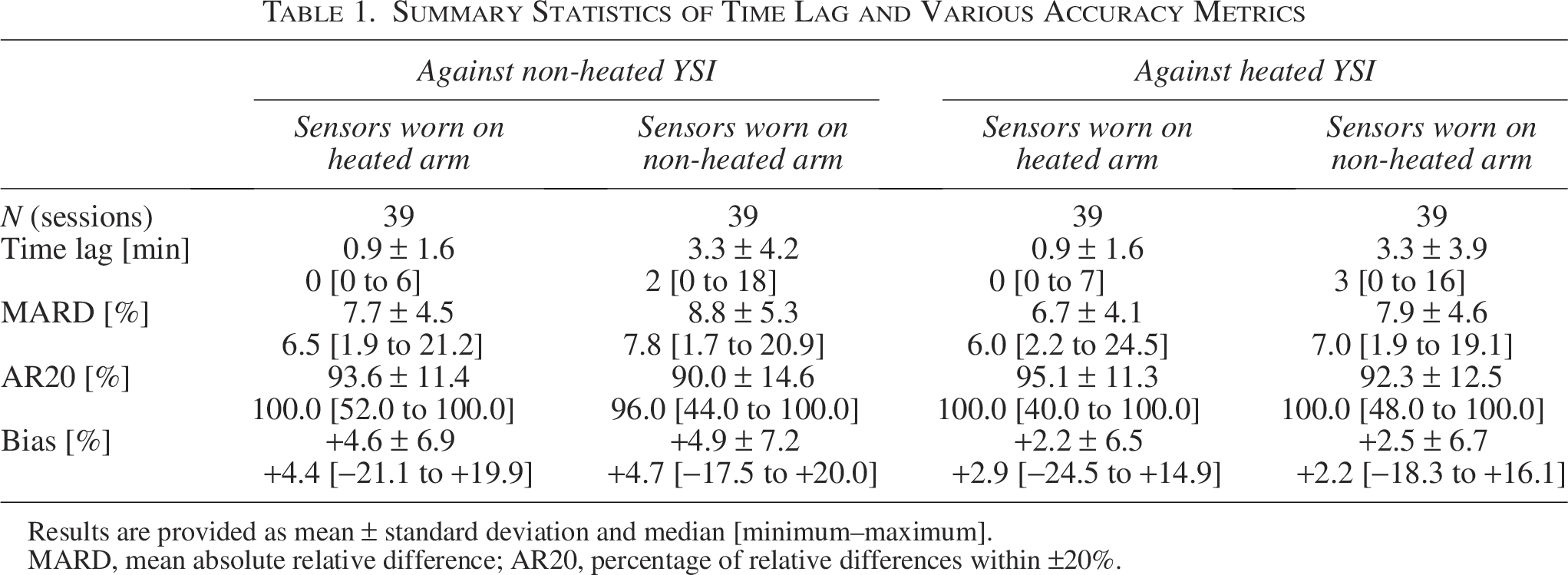
Results are provided as mean ± standard deviation and median [minimum–maximum].
MARD, mean absolute relative difference; AR20, percentage of relative differences within ±20%.
Conclusions
The results of this article have no direct implications for the use of CGM systems in clinical practice. However, we assert that the observed effect of arterialization on CGM system time lag affects the design and interpretation of CGM performance studies. In the context of standardizing these CGM performance evaluations, it was previously argued that arterialization is not a suitable approach because the arterialization effect likely depends on aspects of the specific heating procedure. Furthermore, it creates unrealistic testing conditions compared to everyday CGM use due to the immobilization of study participants. 5 The results of the present analysis further strengthen this argument, as the heating, and thus possibly the reduction in time lag in CGM performance studies, does not represent real-life CGM use.
Authors’ Contributions
M.E.: Data curation, formal analysis, and writing—original draft. S.P.: Writing—review and editing. D.W.: Writing—review and editing. G.F.: Writing—review and editing.
Footnotes
Author Disclosure Statement
G.F. is the general manager and medical director of the Institute for Diabetes Technology (Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany), which carries out clinical studies, e.g., with medical devices for diabetes therapy on its own initiative and on behalf of various companies. GF/IfDT received research support and/or speaker fees and/or consultancyhonoraria from Abbott, Ascensia, Bionime, Boydsense, Dexcom, Insulet, i-SENS, Lilly, Menarini, Novo Nordisk, Perfood, Pharmasens, Roche, Sinocare, Terumo, Vertex, Ypsomed. M.E., S.P., and D.W. are employees of IfDT.
Funding Information
The data used in this work originated from a study funded by Roche Diabetes Care GmbH.