
Abstract
Background:
CGM is associated with improved diabetes management. Prior studies have evaluated its effects on health care utilization and costs among individuals using insulin, particularly those prescribed rapid- and short-acting regimens. The present study compared clinical and economic outcomes between CGM users and nonusers in a large, diverse, real-world population of rapid- and short-acting insulin users.
Methods:
Using the Mariner Commercial Claims Database, adults with diabetes and at least one claim for rapid- or short-acting insulin between January 1, 2010, and October 31, 2022, were identified. Two cohorts were defined based on receipt of CGM: those with CGM (wCGM) and those without CGM (xCGM). Direct matching was applied to ensure comparability between groups. Outcomes included total medical costs, emergency room (ER) days, inpatient (IP) days, ER and IP days associated with hypoglycemia, diabetic ketoacidosis (DKA), or mixed events, and the likelihood of achieving glycated hemoglobin (HbA1c) <9%. The National Committee for Quality Assurance considers HbA1c >9% as “poor control”.
Results:
After applying exclusion criteria, 3,139,979 individuals met inclusion criteria. Of these, 536,512 received a CGM and 2,603,467 did not, meaning approximately 83% of eligible individuals had no evidence of CGM use. Total health care costs were significantly lower in the wCGM cohort ($6,245) compared with the xCGM cohort ($7,786; t(698,086) = –71.41, P < 0.001). The wCGM group also had significantly fewer ER days and IP days at 3, 6, 9, and 12 months. CGM users had 19% higher odds of achieving HbA1c <9% compared with nonusers (odds ratio [OR] = 1.19). A significantly smaller proportion of individuals in the wCGM cohort had ER/IP days associated with hypoglycemia, DKA, or both.
Conclusions:
These findings reinforce the clinical and economic value of CGM and support recent policy updates expanding access for insulin-treated populations.
Keywords
Introduction
The rising prevalence of diabetes and its associated costs continue to place a substantial burden on the U.S. health care system. An estimated 38.4 million Americans are living with diabetes 1 and approximately 9.8 million of these individuals are treated with insulin. 2 Despite the well-established relationship between poor glycemic control and both acute and chronic complications, 3 only 25.2% of people with type 1 diabetes (T1D) or insulin-treated type 2 diabetes (T2D) achieve the recommended glycated hemoglobin (HbA1c) target of <7%. 4 This persistent gap underscores the challenge of therapeutic inertia, delays in initiating or intensifying therapy despite unmet glycemic goals, which remains a major barrier to improving outcomes in insulin-treated populations.
In addition to the clinical consequences, diabetes continues to drive rising health care costs. The direct and indirect cost of diabetes in the United States now exceeds $413 billion, accounting for approximately 25% of health care expenditures, with 61% of these costs directly attributed to diabetes. 5 A significant portion of these expenses stems from the increasing number of diabetes-related inpatient (IP) hospitalizations and emergency room (ER) visits, which surged from 29.8 million in 2017–42.1 million in 2022. 5
Advances in glucose monitoring have led to the development of continuous glucose monitoring (CGM) systems, which support proactive diabetes management through continuous, real-time glucose data and trend analysis. Unlike traditional fingerstick testing, CGM devices provide around-the-clock insights and include alerts when glucose levels fall outside target thresholds. These alerts enable timely interventions such as insulin administration, correction of hypoglycemia, or adjustment of physical activity to prevent further glycemic deterioration. Through early detection and response, CGM can reduce the risk of acute complications and lower the frequency and duration of ER visits and IP stays. 6
Multiple randomized controlled trials and real-world studies have demonstrated that CGM improves glycemic control,7–22 reduces hospitalizations and diabetes-related costs,13,23–26 and significantly increases the users’ engagement in self-management.27–30 Based on this evidence, major diabetes organizations recommend CGM as standard of care for individuals treated with multiple daily injections, insulin pump therapy, or, in some cases, basal insulin.31,32
Despite the demonstrated benefits of CGM, adoption remains inconsistent. While most individuals who meet clinical criteria have some level of insurance coverage, barriers such as prior authorization requirements, provider hesitation, perceived device complexity, and out-of-pocket costs continue to limit adoption. 33 In addition, disparities in CGM use across racial, ethnic, and socioeconomic lines raise concerns about equitable access.34–38
In April 2023, the Centers for Medicare & Medicaid Services revised its coverage policy to expand access to CGM for individuals treated with insulin. 39 The updated guidance removed prior criteria, including the need for multiple daily insulin injections or pump therapy and the requirement for frequent insulin adjustments based on blood glucose monitoring (BGM) or CGM results. Although this policy change occurred after the analysis timeframe, the study population consists of individuals prescribed prandial insulin, which is a clinically relevant group given the complexity of their regimens and the need for frequent dose adjustments and close glucose monitoring.
We hypothesized that CGM use among individuals with insulin-treated diabetes would be associated with reduced health care resource utilization (HCRU), fewer ER and IP days related to glycemic excursions, a higher likelihood of achieving an HbA1c < 9%, and lower total health care costs. This study evaluated these outcomes using a large, nationally representative administrative claims dataset.
Methods
Study design
This retrospective matched cohort study evaluated the impact of CGM use on clinical and economic outcomes among adults with diabetes treated with rapid- or short-acting (prandial) insulin. Short-acting insulin refers to regular insulin; basal insulin type (e.g., NPH, glargine) was not differentiated in this analysis. Eligible individuals were identified from administrative claims based on documented use of rapid- or short-acting insulin and clinical indicators consistent with CGM initiation. Individuals were directly matched on age, gender, insurance type, and diabetes type, and then assigned to one of two cohorts based on the presence or absence of a documented claim for CGM during the study period: the CGM cohort (wCGM) and the non-CGM cohort (xCGM).
Total health care costs were defined as the sum of all paid amounts for IP, outpatient, ER, and pharmacy claims. Costs were evaluated over a 12-month follow-up period to provide a comprehensive and stable measure of overall health care spending.
Health care utilization, including ER days and IP days, was assessed quarterly to capture temporal patterns and potential shifts in service use following CGM initiation. This approach allowed for the evaluation of trends over time while preserving an annualized perspective on cost impact.
Acute glycemic events were identified using ER or IP claims associated with a primary or secondary diagnosis code for hypoglycemia or diabetic ketoacidosis (DKA). Hypoglycemia was defined using International Classification of Diseases (ICD)-10 codes E16.0–E16.2. DKA was defined using ICD-10 codes E08.1, E09.1, E10.1, E11.1, and E13.1. Individuals with claims for both events during the follow-up period were categorized under “both.” Each ER visit was counted as 1 day, consistent with established claims-based methods.
Glycemic control was evaluated by identifying individuals with evidence of achieving an HbA1c level <9%. Because laboratory values are not available in the Mariner dataset, researchers used CPT code 3046 F, which denotes HbA1c > 9%, and classified patients as having sustained elevated HbA1c > 9% if they had two such codes more than 90 days apart during the 12-month follow-up. All others were assumed to have achieved HbA1c < 9%, effectively using the inverse of the >9% designation. A 9% threshold was selected because it is more reliably captured in the claims data; CPT codes for lower HbA1c thresholds were not as consistently reported.
Comparisons between cohorts were conducted using t-tests for continuous outcomes and chi-square tests for categorical variables. A P value of < 0.05 was considered statistically significant.
Data source
Administrative claims data were obtained from the Mariner Commercial Claims Database, a national dataset containing more than 75.7 billion de-identified claims from approximately 161 million individuals across all payer types. While the full dataset spans from January 1, 2010, to October 31, 2024, this analysis was limited to data beginning in the first quarter of 2021 to reflect more recent patterns in CGM use. The database includes fully adjudicated claims, providing comprehensive information on health care encounters, diagnoses, procedures, and pharmacy use. All data complied with the Health Insurance Portability and Accountability Act standards for de-identification. Institutional Review Board approval was not required, as the analysis did not involve identifiable patient information.
Study population
The study population included adults aged ≥18 years with a documented diagnosis of T1D or T2D and a claim for rapid- or short-acting (prandial) insulin in the first quarter of 2021. This inclusion criteria was selected to focus on individuals using intensive insulin regimens, for whom CGM is often clinically indicated due to the heightened risk of glycemic variability. This timeframe was selected to reflect contemporary patterns in CGM use and prescribing behavior. The date of the first qualifying insulin claim was designated as the index date.
To reduce confounding, individuals prescribed a sodium-glucose cotransporter 2 (SGLT2) inhibitor or glucagon-like peptide-1 (GLP-1) receptor agonist were excluded, as these agents can independently improve glycemic control and cardiovascular outcomes, which could bias cost and utilization comparisons between CGM users and nonusers. Individuals who met the inclusion criteria and had a CGM claim during the index quarter were assigned to the wCGM group. All individuals were required to have continuous health plan enrollment for at least 6 months prior to and 12 months following the index date, with no evidence of CGM use during the baseline period. Individuals with diabetes were identified using ICD codes: 9th Revision (249.00–250.99, 790.2, 790.21, 790.22, 790.29, 791.5, 791.6) and 10th Revision (E08.0 through E13.9). After applying all inclusion and exclusion criteria, 3,139,979 individuals met eligibility requirements. Of these, 536,512 (17%) had evidence of CGM use during the study period and 2,603,467 (83%) did not, indicating low uptake among eligible individuals. The disposition of individuals included in the analysis is shown in Figure 1.
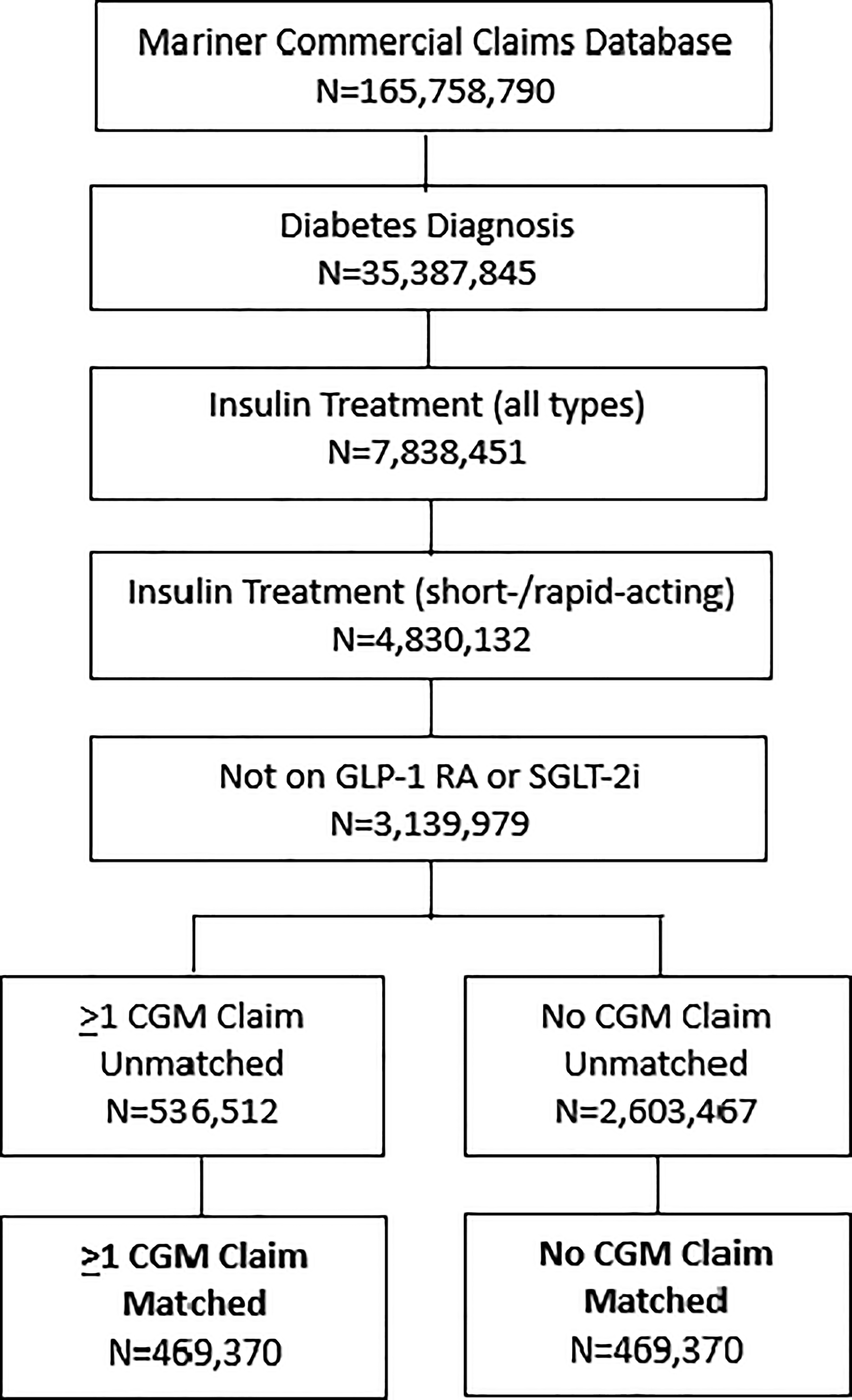
Consort diagram. GLP-1 RA, glucagon-like peptide-1 receptor agonist; SGLT-2i, sodium-glucose cotransporter-2 inhibitor.
Outcomes
Primary outcomes were changes in glycemic status, HCRU, and total medical costs. Glycemic status was inferred using CPT code 3046F, which indicates HbA1c >9%. Individuals were classified as having poor glycemic control if they had two claims for 3046F more than 90 days apart during the 12-month follow-up period.
HCRU was assessed based on the number of IP and ER days at 3-, 6-, 9-, and 12-months post-index. Each ER visit was counted as 1 day. The number of individuals with at least one ER or IP claim for hypoglycemia, DKA, or both was also evaluated. Total medical costs included all allowable charges under medical and pharmacy benefits for individuals with at least one claim during the 12-month follow-up period. After exclusions, 3,139,979 individuals met inclusion criteria. Of these, 536,512 (17%) had evidence of CGM use and 2,603,467 (83%) did not, indicating low uptake in this eligible population. CGM uptake was calculated as a descriptive measure to contextualize adoption in the study population and was not analyzed as an outcome.
Statistical analysis
Descriptive statistics, including mean HbA1c, standard deviations, and interquartile ranges, were used to summarize glycemic control trends. Differences between cohorts were examined using t-tests for continuous variables and chi-square for categorical variables, with statistical significance set at P < 0.05.
Results
Study cohorts
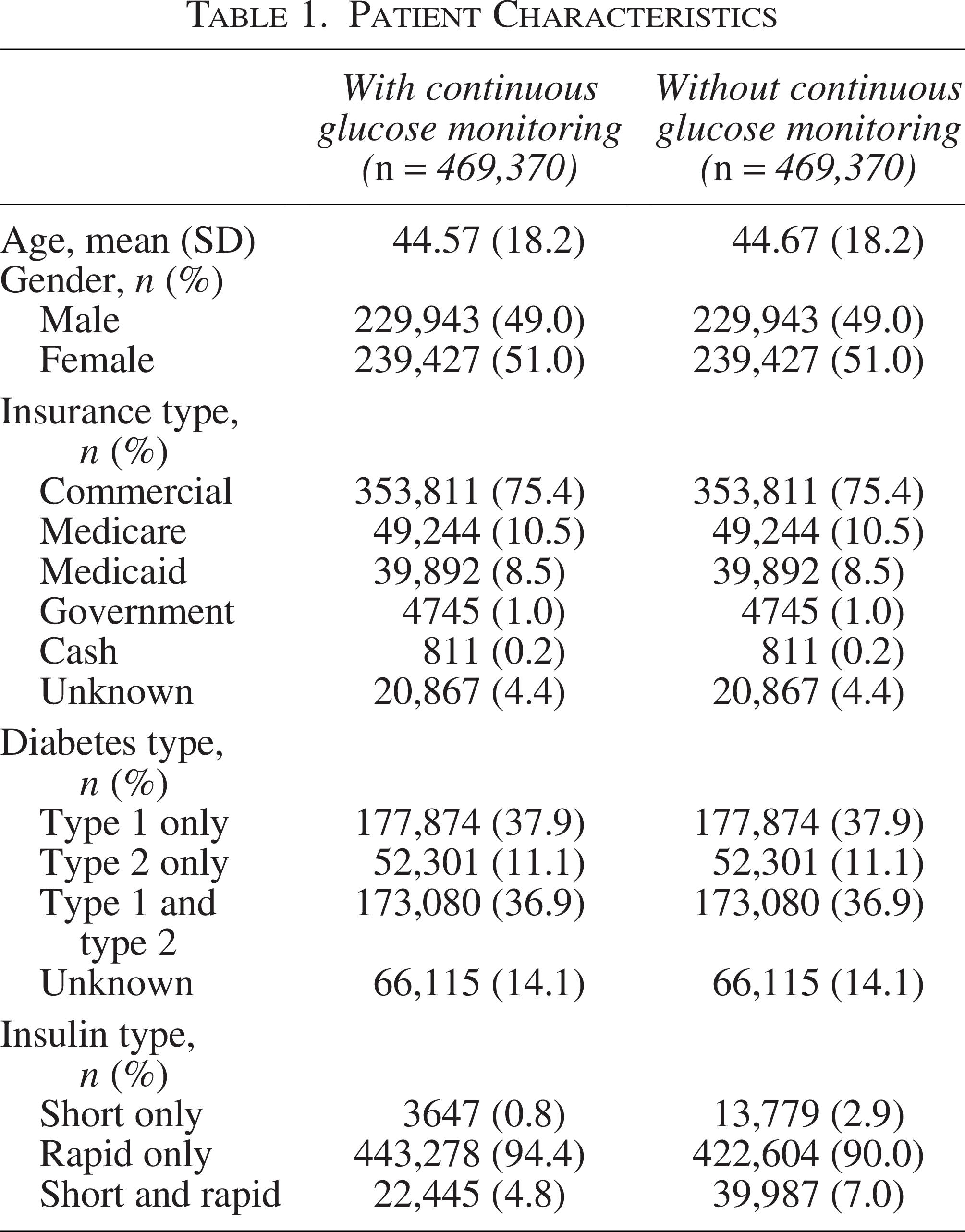
The analysis was conducted on a matched sample of 938,740 individuals, with 469,370 assigned to the wCGM cohort and 469,370 to the xCGM cohort. Participant demographics are presented in Table 1.
Patient Characteristics
Health care costs and utilization
Over the 12-month follow-up period, total health care costs within the CGM cohort were significantly lower than observed in individuals with xCGM use ($6,245 ± $7,457 vs. $7,786 ± $11,627, respectively, t(698086) = −71.41, P < 0.001). (Fig. 2).
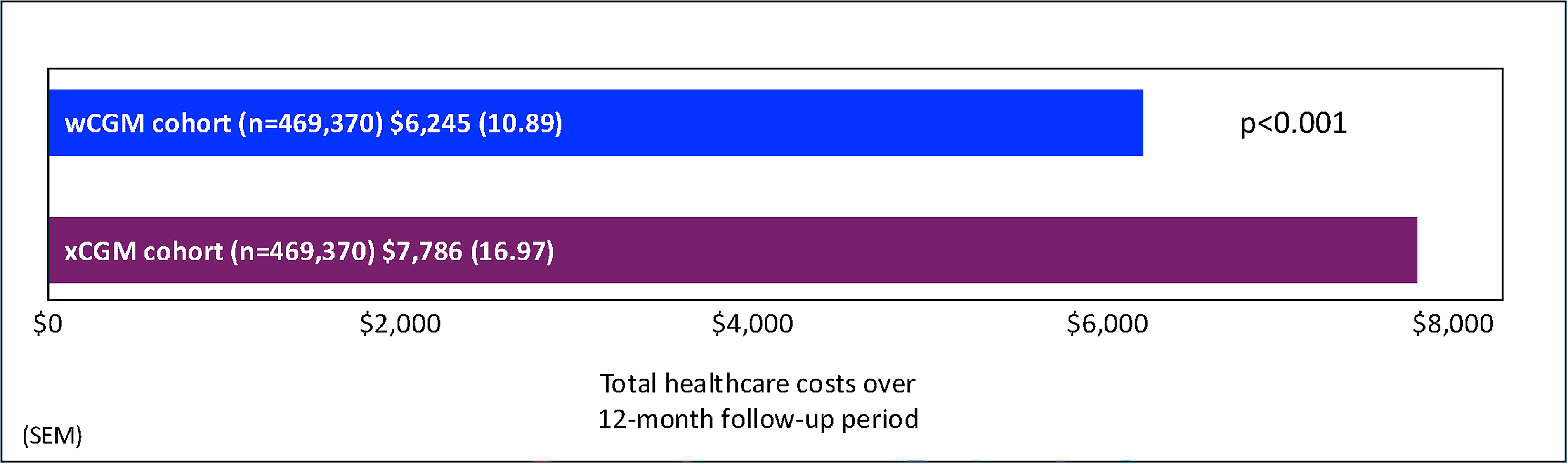
Total health care costs (wCGM vs. xCGM). CGM, continuous glucose monitoring.
HCRU and costs
Mean ER visits (1 day each) and IP days for individuals in the wCGM cohort was significantly lower than the xCGM cohort across the time windows. (Fig. 3).
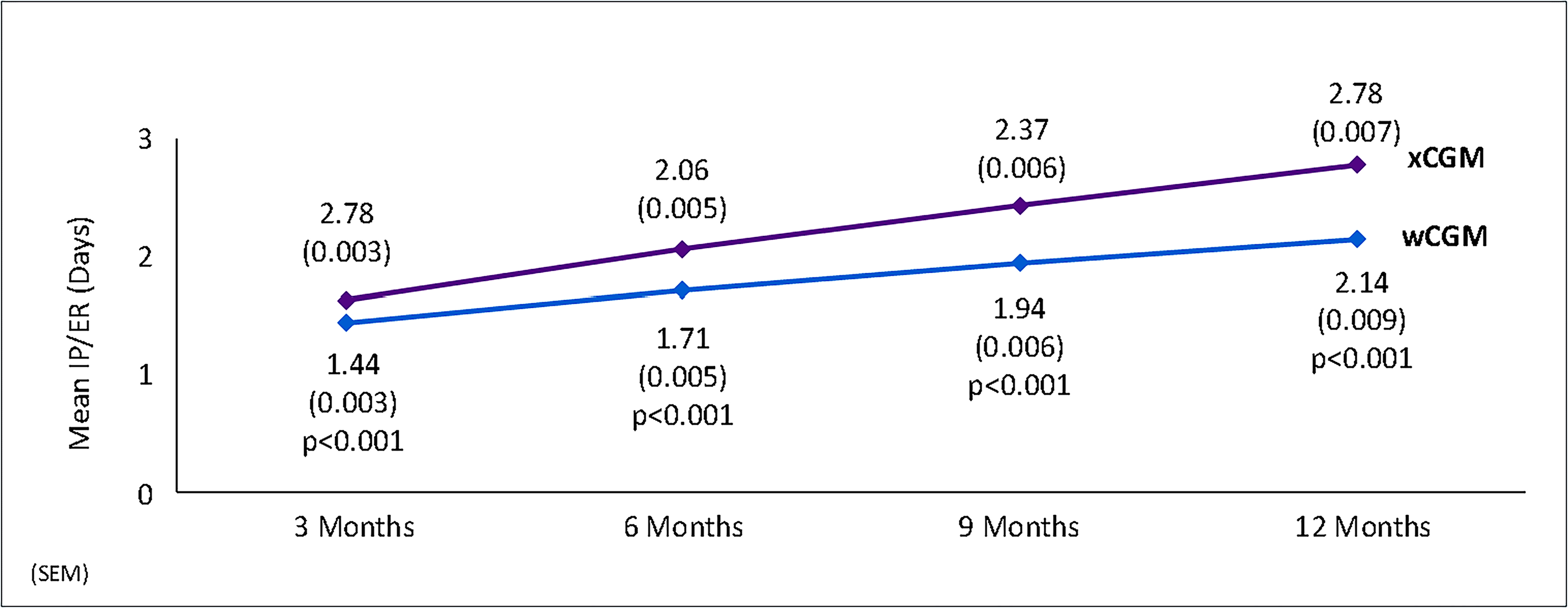
ER and IP days (wCGM vs. xCGM). ER, emergency room; IP, inpatient.
To further characterize the impact of CGM use on acute diabetes-related events, the proportion of individuals with at least one ER or IP encounter associated with a glycemic excursion was assessed over the 12-month follow-up period. Glycemic excursions were classified as hypoglycemia, DKA, or both. As shown in Table 2, individuals in the CGM cohort had significantly lower proportions of ER/IP utilization across all categories compared with those without CGM. Specifically, the CGM group had lower rates of utilization for hypoglycemia (0.89% vs 0.93%; χ2 = 7.16, P < 0.001), DKA (3.52% vs. 4.44%; χ2 = 467.86, P < 0.001), and both events combined (4.44% vs. 5.42%; χ2 = 423.46, P < 0.001).
Proportion of Individuals with ≥1 Emergency Room or Inpatient Encounters Attributed to a Glycemic Excursion, by Event Type

Differences HbA1c
Results from the chi-square analysis (χ2(1) = 58.24, P < 0.001) indicated that individuals in the wCGM group had 19% higher odds of achieving HbA1c <9% compared with those in the xCGM group (OR = 1.19).
Discussion
In this real-world retrospective analysis of administrative claims data, initiation of CGM compared with no CGM use was associated with significantly lower IP days and ER visits (−23.0%) and total medical costs of care (−19.8%) within a large cohort of people with insulin-treated diabetes. Importantly, the high percentage of CGM users who achieved HbA1c levels <9% is relevant to payers. In its Healthcare Effectiveness Data and Information Set (HEDIS) performance measures, the National Committee for Quality Assurance (NCQA) considers HbA1c < 8.0% as “in control” and HbA1c >9% as “poor control.” 40 Our findings can help inform payer strategies aimed at improving CGM adoption among individuals who meet clinical criteria for use. After applying all inclusion and exclusion criteria, 3,139,979 individuals in our study population were eligible for CGM; however, 83% had no evidence of use, indicating low uptake despite eligibility. Although, many plans have expanded access to CGM through both the pharmacy and medical channels, our findings suggest that coverage alone may not be sufficient to drive adoption. Even within existing coverage policies, there is an opportunity to strengthen implementation through provider engagement, prescribing support, and patient-centered onboarding. Ensuring that eligible individuals are not only prescribed CGM but are supported in sustained use may also contribute to improved performance on quality measures such as STAR Ratings and NCQA Health Plan Ratings, which influence reimbursement and plan growth, particularly within Medicare Advantage populations.
The results from our analysis relative to HCRU and costs are similar to those reported in previous studies.13,24,41 For example, Miller et al. analyzed data from the MarketScan™ administrative claims database to assess the effects of CGM on rates of acute diabetes-related events and all-cause hospitalization in a large cohort of adults with T2D treated with nonintensive or noninsulin medications during the 6-month observation period following acquisition of a CGM device. 24 Investigators showed a significant reduction in the rate of acute diabetes-related events, from 0.076 to 0.052 events/patient/year (P < 0.001). Significant reductions in all-cause hospitalization were also observed, from 0.177 to 0.151 events/patient/year, P = 0.002).
A similar analysis of a large claims database that assessed the effects of CGM use after 6 months reported significant reductions in acute diabetes-related events, from 0.180 to 0.072 events/patient-year, P < 0.001). 41 Rates of all-cause hospitalizations decreased from 0.420–0.283 events/patient-year; P < 0.001.
In a retrospective analysis of administrative claims data, Norman et al. assessed changes in IP hospitalization rates and costs in 571 adults with T2D after initiating CGM. 13 Approximately 80% of individuals were treated with prandial insulin therapy. Investigators reported slight reductions in IP hospital admissions (−0.006 PPPM, P = 0.057) and total hospital days (−0.042 per patient per month [PPPM], P = 0.139). However, significant reductions in the average cost PPPM for diabetes-related medical costs were observed (−$424, P = 0.035). These reductions were driven, in part, by reductions in the costs associated with diabetes-related IP admissions (−$358 PPPM, P = 0.044).
Strengths and limitations
A key strength of this analysis is the use of a large sample size and real-world, longitudinal data with a matched control cohort. Moreover, the claims dataset provided accurate information about HCRU and total health care costs, and the 12-month observation period allowed for the assessment of the sustainability of glycemic improvement associated with CGM use. However, the analysis has notable limitations. As with most large claims dataset analyses, we were unable to capture more granular beneficiary information beyond household income and race/ethnicity. Laboratory results were not available, and HbA1c values were identified through diagnosis and procedure codes rather than direct laboratory measures, which precluded evaluation of HbA1c as a continuous variable or assessment of changes before and after CGM initiation. Additionally, we were unable to stratify outcomes by factors such as comorbidity burden, complication type, or duration of CGM use, which could provide a more longitudinal view of cost and clinical benefit. Although direct matching was applied to balance observed characteristics between groups, important dimensions of socioeconomic status such as education level, employment, or housing stability were not available in the dataset. These unmeasured factors are well documented to influence health outcomes and technology adoption and may be necessary to further normalize comparisons using standardized approaches. As previously noted, disparities in CGM use due to implicit racial bias and socioeconomic status are well documented.34–38 Nor was it possible to determine whether individuals were prescribed a CGM but chose not to fill it, or how those who initiated CGM used the data in their daily self-management. We also note that differences in basal insulin type could influence hypoglycemia rates and health care costs, and future research could examine whether CGM mitigates risks associated with NPH use. Additionally, the large number of participants with a “dual” diabetes diagnosis of T1D and T2D (n = 346,160) likely impacted our ability to accurately match the cohorts. Excluding patients on SGLT2 inhibitors or GLP-1 receptor agonists reduced confounding but may limit generalizability, as these agents are increasingly used alongside CGM in real-world practice. Finally, because only individuals treated with prandial insulin were included in the analysis, our findings cannot be generalized to the larger diabetes population.
Conclusions
CGM adoption among individuals with diabetes treated with prandial insulin therapy is associated with reduced health care utilization, lower costs, and improved glycemic control, reinforcing its role as a cost-effective intervention in diabetes management. Despite clear clinical guidance and well-documented benefits, CGM remains underutilized. In this study, 83% of individuals who met criteria for CGM prior to matching (Fig. 1) were not using the technology, reflecting a substantial gap in adoption. This untreated segment represents an opportunity to improve outcomes and reduce avoidable health care costs. Expanding access, educating providers to increase comfort with prescribing, and supporting individuals in CGM use may help align real-world practice with current standards of care and improve health outcomes across populations. Future research should further evaluate longitudinal outcomes and the impact of CGM duration, adherence, and integration with emerging therapies to better understand how sustained use influences clinical and economic outcomes across diverse populations.
Authors’ Contributions
J.C.A. and C.D.: Conceptualization, original draft; review and editing. V.E.B. and I.B.H.: Original draft; review and editing.
Footnotes
Acknowledgments
The authors wishes to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for his editorial support in developing this article.
Author Disclosure Statement
C.D. is an employee of CCS Medical. J.C.A. has received consulting fees from CCS Medical. V.E.B. is an employee of OneHome, receives consulting fees from the American Diabetes Association, speaking fees supported by sponsorship from Sanofi (via DiabetesSisters), and program contract support from Mecklenburg County, NC. I.B.H. serves as an advisory board member for Abbott Diabetes Care, Roche Diagnostics, and receives research grant support from Tandem Diabetes Care and Sequel Med Tech.
Funding Information
This study was funded by CCS Medical.