
Abstract
Background:
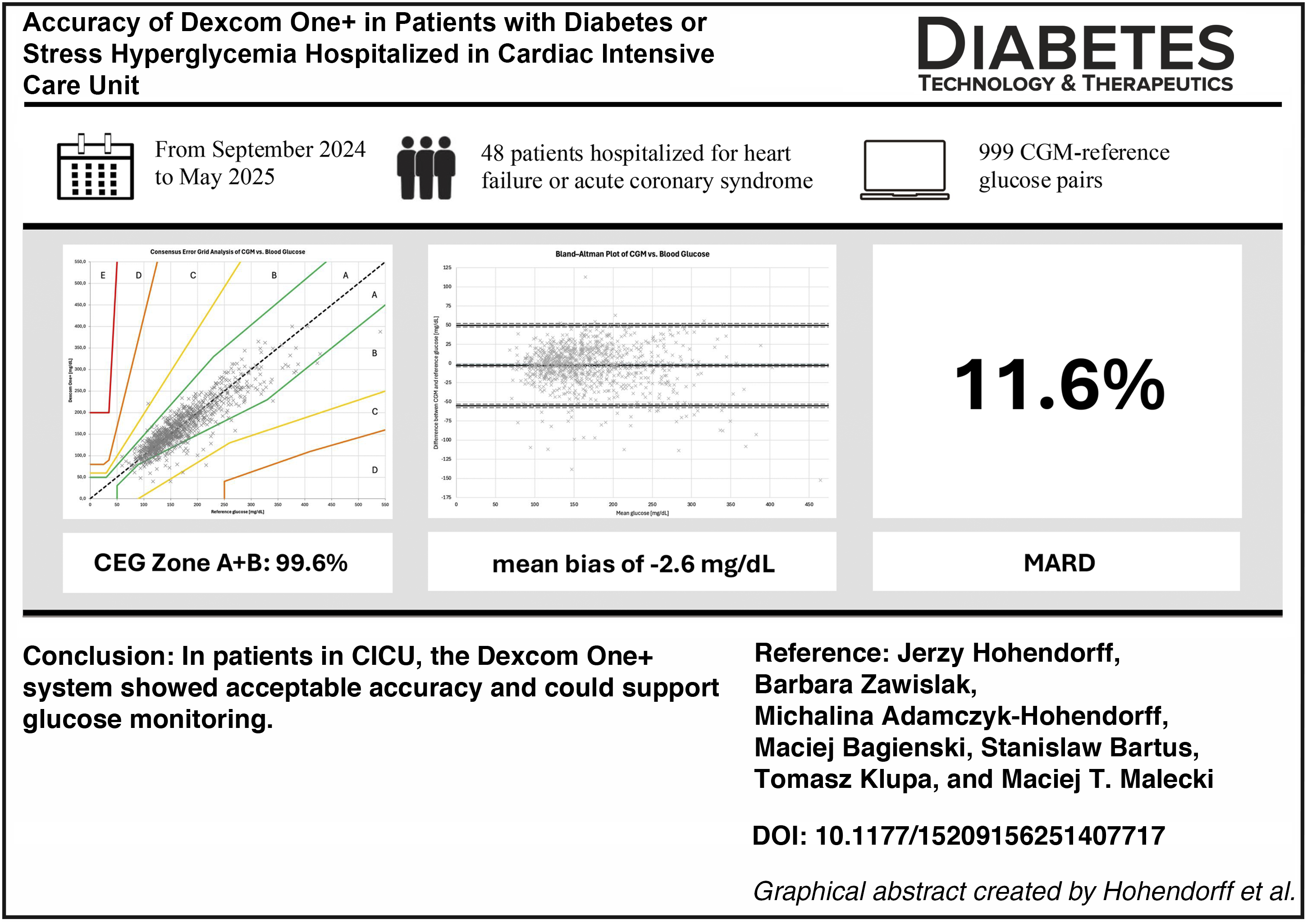
Continuous glucose monitoring (CGM) systems may assist in glucose management for patients in the cardiac intensive care unit (CICU). We aimed to assess the accuracy, feasibility, and tolerability of Dexcom One+ in comparison with standard blood glucose measurements.
Materials and Methods:
From September 2024 to May 2025, we included patients with known diabetes or hyperglycemia on admission >140 mg/dL who were hospitalized in the CICU for acute coronary syndrome and/or heart failure. Sensors were inserted into the upper arms, and glucose readings were obtained using a dedicated receiver. Glucose levels were measured with the Cobas Pulse glucometer (Roche Diagnostics) at the routine frequency in the CICU as part of standard care. Accuracy was evaluated by the mean absolute relative difference (MARD). Clinical performance was assessed through Consensus Error Grid analysis. The feasibility outcome included the number of early sensor detachments and sensor failures. Safety outcomes encompassed skin reactions.
Results:
We obtained 999 CGM-reference glucose paired samples from 48 patients (39 with previously diagnosed type 2 diabetes aged 73.5 ± 9.6 years. The mean HbA1c was 7.1 ± 1.3%. Overall, 725 paired samples were obtained during oxygen therapy, 362 during vasopressor infusion, and 280 during combined oxygen therapy and vasopressor infusion. CGM use duration was 4.0 ± 3.2 days. There were 3 reference readings below 70 mg/dL, 658 within the 70–180 mg/dL range, and 338 above 180 mg/dL. Overall, MARD was 11.6% (95% CI: 10.9–12.2). 93.5% of readings were in Zone A, 6.1% in Zone B, and 0.4% in Zone C. No readings were found in Zone D + E. We observed one mild hematoma at the insertion site, three sensor failures, and three early detachments.
Conclusions:
In patients in CICU, the Dexcom One+ system showed acceptable accuracy and could support glucose monitoring.
Keywords
Introduction
Cardiovascular events are the leading cause of death in patients with type 2 diabetes (T2DM) worldwide.1,2 Among patients hospitalized in cardiac intensive care units (CICU) due to acute cardiac syndrome or heart failure (HF), a large number are those with T2DM.3,4 High glucose variability and hypoglycemic events are thought to increase death risk in such patients.5–7 However, very intensive glucose control (80–108 mg/dL) could increase hypoglycemia risk and mortality among adults in the ICU, as shown in the NICE-SUGAR Study. 8 In a recently published patient-level meta-analysis of intensive glucose control in critically ill adults, intensive glucose control (blood glucose target of 120 mg/dL or less) was not associated with a reduced risk of mortality but increased the risk of severe hypoglycemia, and no specific subgroup of patients was found in whom intensive glucose control was beneficial. 9 International guidelines recommend that in patients receiving insulin infusion, frequent, i.e., hourly, blood glucose measurements be taken and glucose level be maintained in the range of 100–180 mg/dL.10,11 This approach, involving frequent blood glucose measurements, adds a significant extra workload for medical staff, particularly in departments caring for patients with acute conditions.12,13
Continuous glucose monitoring (CGM) is a standard of care for most patients receiving insulin in outpatient settings.14,15 There are numerous studies on CGM use in patients with type 1 diabetes (T1DM) and T2DM on intensive insulin therapy that show improvement in glucose control, time spent in range, time spent in hypoglycemia (time below range), and glucose variability.16–19 Subsequent generations of CGM have demonstrated progressively improved accuracy, as assessed by mean absolute relative difference (MARD).20–23 MARD of less than 10% is acknowledged as a safe and useful threshold for decision-making without the need for blood glucose confirmatory measurements using a glucometer. 24 With MARD of less than 14%, CGM is considered accurate in inpatient settings with the need for additional blood glucose measurements. 25 The 2025 American Diabetes Association Standards of Care recommend continuation of in-hospital CGM use if clinically appropriate; however, insulin decisions should be confirmed by capillary blood glucose measurements. 10
Considering this, we aimed to assess the accuracy, feasibility, and tolerability of CGM Dexcom One+ compared with standard blood glucose measurements in patients with diabetes or stress hyperglycemia hospitalized in the cardiac intensive care unit for acute coronary syndrome or HF.
Material and Methods
Study design
The study was an investigator-initiated, observational study conducted in the Cardiac Intensive Care Unit, University Hospital in Krakow, Poland, between September 2024 and May 2025. Adult patients were eligible for the study if they had known diabetes or hyperglycemia at admission (>140 mg/dL), were admitted to CICU for acute coronary syndrome or HF, and were expected to stay in the CICU for at least 2 days. Patients were excluded from the study if they required renal replacement therapy or if written informed consent could not be obtained.
Sensors from the Dexcom One+ were inserted into the upper arms, and glucose readings were obtained using the dedicated Dexcom One+ receiver. Capillary glucose measurements were performed using the Cobas Pulse glucometer (Roche Diagnostics), which meets the CLSI POCT12-A3 criteria (more stringent than ISO 15197:2013) for hospital glucometers, including those used in intensive care units, at the frequency routinely applied in the CICU as part of standard care.26,27 No optional sensor calibrations were performed during the study. Glycemic data were collected for up to 10 days or until patients were discharged, transferred to another department, or died, whichever occurred first.
Outcomes
The primary end point was the accuracy of the Dexcom One+, assessed as MARD between glucose measurements obtained by the CGM and the glucometer. In addition, the accuracy was evaluated based on the proportion of CGM values within 15% of reference blood glucose values ≥100 mg/dL or within 15 mg/dL of reference blood glucose values <100 mg/dL (%15/15), along with the %20/20, %30/30, and %40/40 agreement rates. Bland–Altman analysis and clinical accuracy assessment using the Parkes Consensus Error Grid (CEG) were performed.28,29 The CEG is divided into zones representing the degree of risk arising from incorrect measurement (zone A—no effect on clinical action; zone B—altered clinical action, little or no effect on clinical outcome; zone C—altered clinical action, likely to affect clinical outcome; zone D—altered clinical action, could have significant medical risk; and zone E—altered clinical action, could have dangerous consequences). Feasibility outcomes included sensor failure or early sensor detachments. Tolerability outcomes included skin reactions to sensor application or sensor adhesives.
Data analyses
Statistical analyses were performed using IBM SPSS Statistics, version 29 (Armonk, NY, USA).
Bioethics
The study was approved by the Jagiellonian University Bioethics Committee, Krakow, Poland (1072.6120.49.2024, 1072.6120.21.2025), and conducted in accordance with the Helsinki Declaration. All patients gave written informed consent prior to inclusion in the study.
Results
Patients
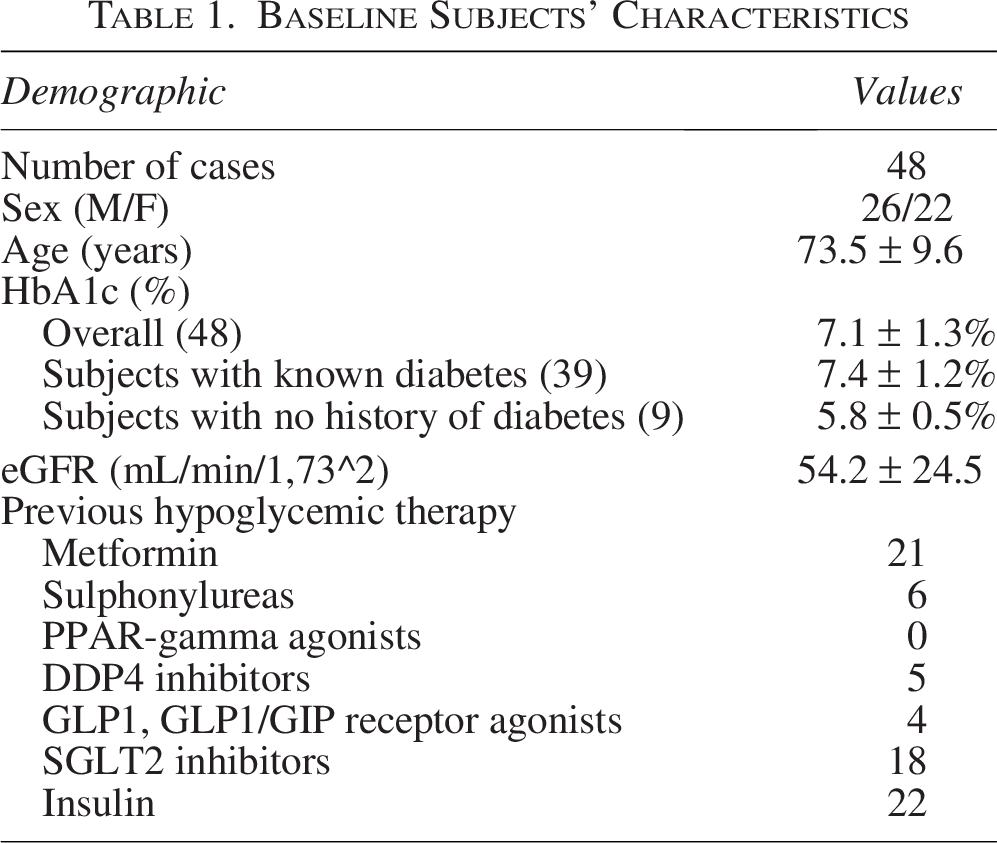
A total of 48 patients were enrolled in the study. Twenty-six were male (54.2%). The mean age was 73.5 ± 9.6 years. Thirty-nine had a known history of diabetes. The mean HbA1c was 7.1 ± 1.3%. Baseline patient characteristics are presented in Table 1. During their stay in the CICU, 38 patients received oxygen therapy, and 14 patients required vasopressor infusions. In 8 patients, data collection was completed after the sensors reached the end of their 10-day lifespan; 36 patients were transferred to other departments before the sensors expired, and 2 died during the observation period.
Baseline Subjects’ Characteristics
CGM accuracy
In total, 999 CGM-reference glucose pairs from 51 sensors were obtained. CGM duration was 4.0 ± 3.2 days. There were 3 blood glucose reference readings <70 mg/dL (59, 59, and 67 mg/dL), 658 within 70–180 mg/dL range, and 338 > 180 mg/dL.
Overall, MARD was 11.6%. MARD of first day of CGM use was 11.9%, and MARD of days from 2 to 10 was 11.5%. 362 pairs were obtained during vasopressor infusion, 725 during oxygen therapy, and 280 during combined vasopressor and oxygen therapy, and MARD was 12.3%, 11.4%, and 12.2%, respectively.
In the CEG analysis, 99.6% of glucose pairs were within zones A + B, 0.4% within zone C, and none within zones D + E, as shown in Figure 1. Numerical accuracy is summarized in Table 2.
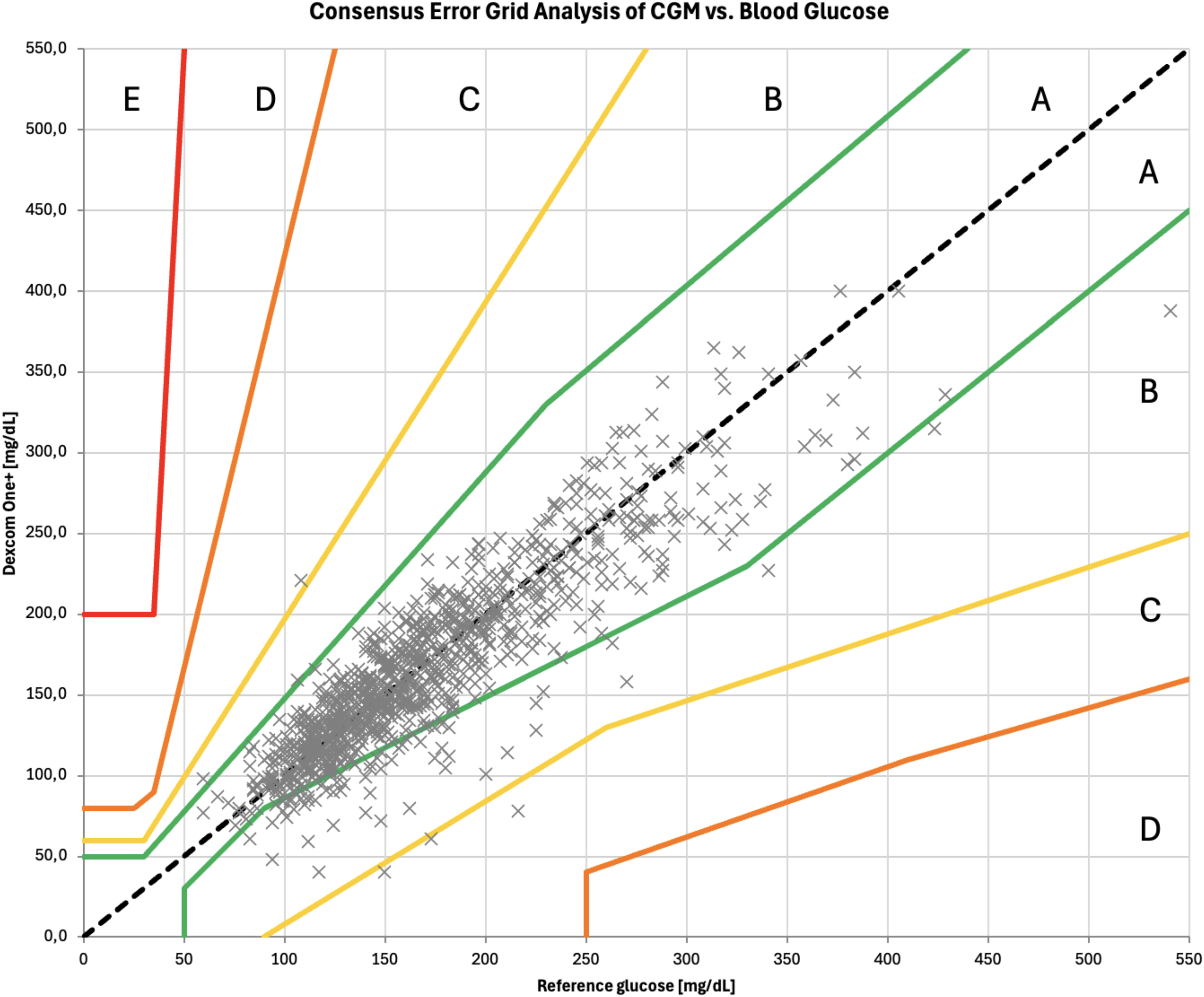
CEG analysis comparing Dexcom One+ sensor results to capillary blood glucose results. CEG, consensus error grid.
Dexcom One+ Accuracy
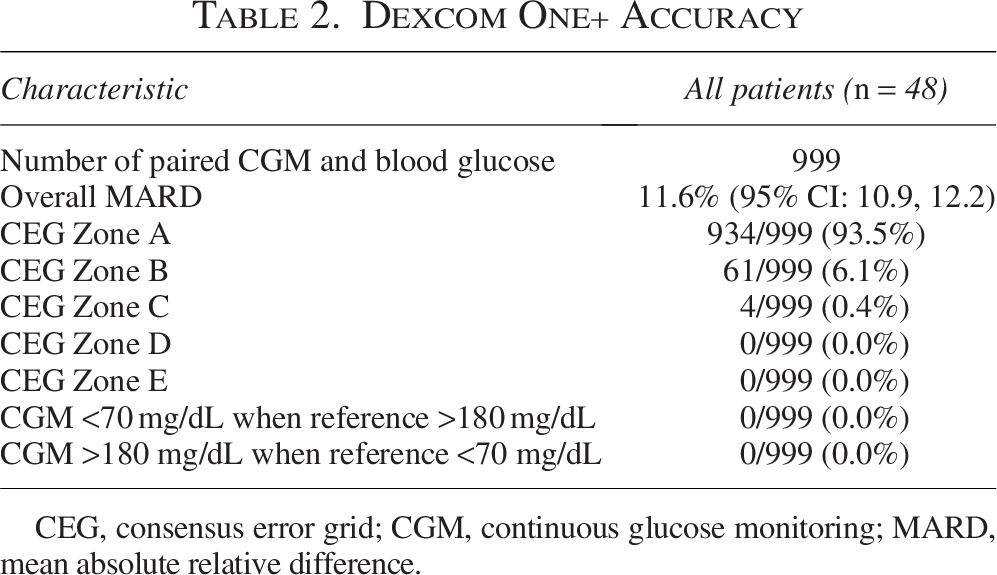
CEG, consensus error grid; CGM, continuous glucose monitoring; MARD, mean absolute relative difference.
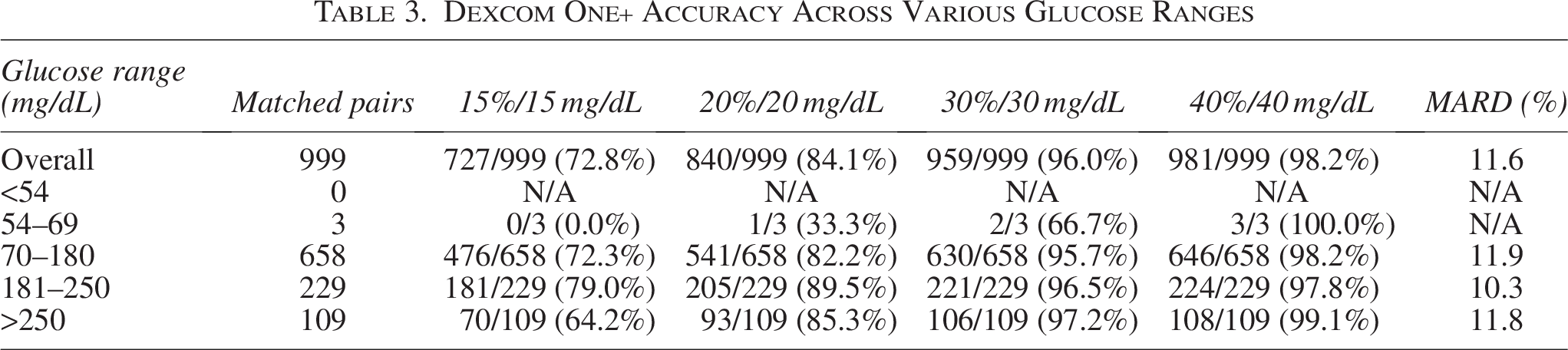
Sensor accuracy across various glucose ranges is shown in Table 3.
Dexcom One+ Accuracy Across Various Glucose Ranges
The Bland–Altman analysis showed a mean bias of −2.6 mg/dL (95% CI: −4.3, −1.0) with a lower limit of agreement of −55.2 mg/dL (95% CI: −58.0, −52.3) and an upper limit of agreement of 49.9 mg/dL (95% CI: 47.1, 52.7), as shown in Figure 2.
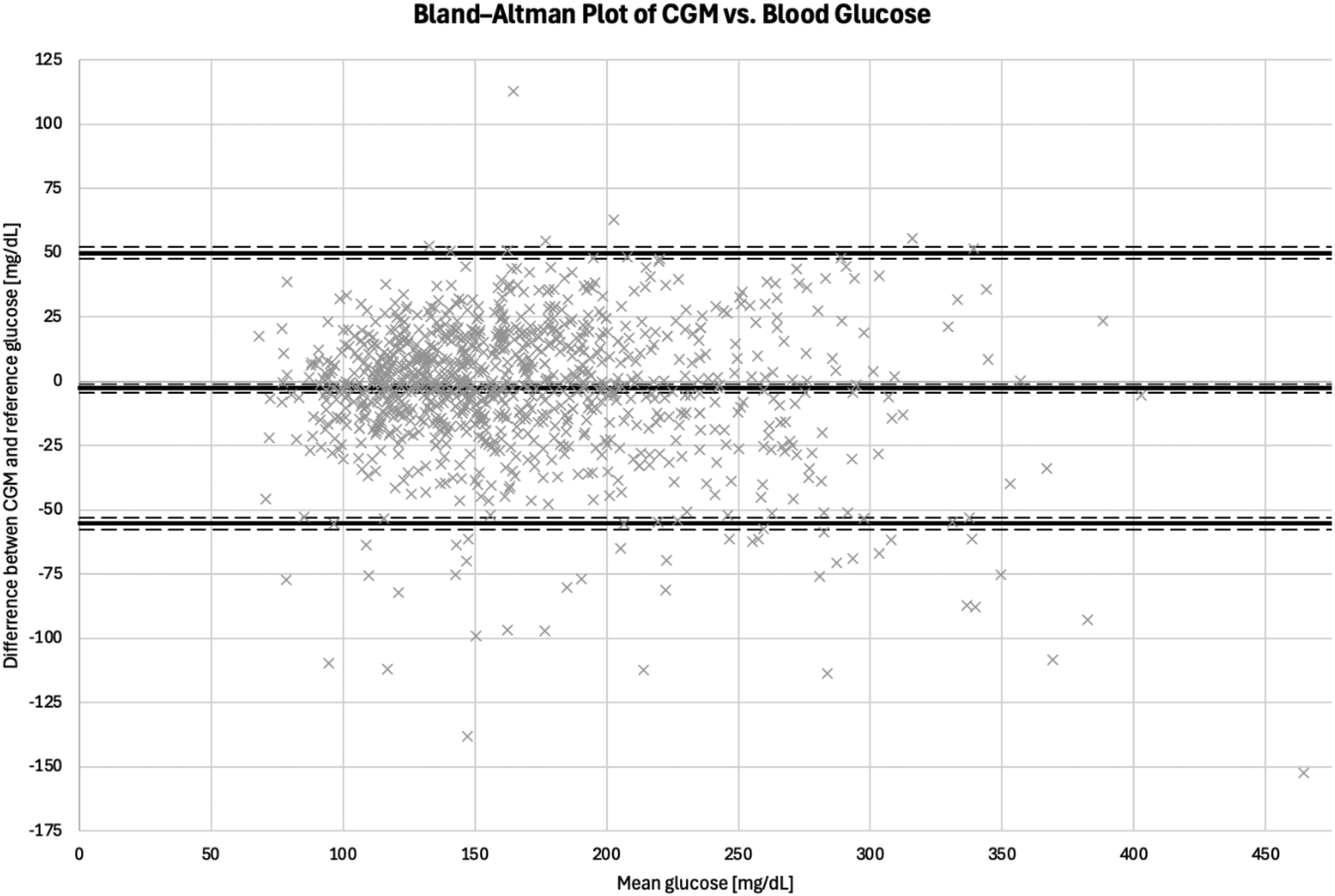
Bland–Altman plot showing the mean difference and 95% limits of agreement between 999 paired Dexcom One+ and capillary glucose values. Horizontal dashed lines represent 95% CI.
A review of concomitant medications revealed that no subjects were receiving treatments known to interfere with One+ accuracy (acetaminophen >4 g/day or hydroxyurea), and no patients required extracorporeal membrane oxygenation during the study.
CGM feasibility and tolerability
We have noticed three sensors failures and three early sensor detachments. In one subject, a mild hamartoma was observed at the sensor insertion site; no skin allergic reaction was found.
Discussion
In this observational study, we evaluated the accuracy of inpatient Dexcom One+ using glucometer measurements as reference values. CGM accuracy was assessed in patients with either diabetes or stress hyperglycemia who were hospitalized in the CICU for HF or acute coronary syndrome. Most CGM–reference blood glucose pairs were obtained during oxygen therapy, and a large proportion during vasopressor infusion. No specific protocols were implemented during the study, and all reference blood glucose measurements were collected as part of routine clinical practice.
Compared with standard blood glucose measurements, the Dexcom One+ demonstrated acceptable accuracy, as overall MARD was <14%, and 99.6% of CGM readings were found within zones A and B of the Consensus Error Grid. As expected, CGM accuracy was slightly lower in patients requiring vasopressor infusion.
The accuracy of the inpatient Dexcom One+, as assessed by MARD, appears to be better than that reported in recent studies of the previous generation of CGM (Dexcom G6). However, this finding should be interpreted with caution, as no head-to-head comparison was performed, and recent studies involved different populations and potentially variable protocols.30–33
In an observational study comparing 6648 matched Dexcom G6 and reference point-of-care and laboratory glucose measurements during subjects’ hospitalization, MARD was 19.2%, and 11.4% if once-daily calibration performed, with 98.2% of values in zones A and B. 30 Another study in non-critically ill adult patients with diabetes in inpatient settings reported MARD of 12.8%, and CEG analysis showed 98.7% of values fell within zones A and B, based on 4067 matched Dexcom G6 and point-of-care measurements. 31 A retrospective analysis of 2,904 CGM and point-of-care measurement pairs in pediatric patients with diabetes hospitalized for various reasons, including diabetes-related, infectious, neurological, gastrointestinal, mental health, and other, showed a MARD of 15.9%, with 96.6% of values in zones A and B of the CEG analysis. 32 In a recent study assessing Dexcom G6 use in ICU settings, based on a total of 1015 matched Dexcom G6 and laboratory or point-of-care measurements pairs, a MARD was 22%–23%. 33
An extensive multicenter study evaluating the accuracy and safety of Dexcom G7 in adults with T1DM or T2DM on intensive insulin therapy or not (619 sensors, 77,774 matched pairs) reported overall MARDs of 8.2% and 9.1% for arm- and abdomen-placed sensors, respectively, showing accurate glucose readings in outpatient settings. 22 Limited data on the performance of Dexcom G7/One+ in the inpatient setting are available. A study on Dexcom G7 accuracy during and after major surgery based on a total of 619 matched pairs shown intraoperative MARD of 12.5% and 83.4% of values in zones A and B (265 pairs), and in the postoperative period, MARD was 9.0% (354 pairs). 34 A recently published study on Dexcom G7 accuracy in an intensive care unit, based on 1515 pairs, showed MARD 13% using plasma glucose and 17% using capillary glucose as reference. The reported mean bias was −12 mg/d. 35
MARD values calculated in inpatient settings are significantly higher than those observed in outpatient settings, with even greater discrepancies reported in the ICU. This worst accuracy is thought to result from impaired capillary blood flow and tissue edema, hypoxia, anemia, and pressure on sensors resulting from bed positioning. Nevertheless, CGM devices continue to show improvements in accuracy, even within such a challenging population as patients in the ICU receiving vasopressor therapy.
Our study has some limitations. First, this is a study of a relatively small sample size, and a hospital point‐of‐care device was used as the reference instead of YSI. No specific protocol was implemented in terms of the timing and frequency of glucometer measurements; for example, no meal or insulin test was performed; instead, measurements were performed in accordance with the standard clinical practice. 36 Next, reference glucose levels were mostly in the range of 70–180 mg/dL and above 180 mg/dL, with only three reference measurements below the range, so we were unable to conduct a rigorous assessment of the accuracy and clinical utility to detect hypoglycemia. As the CGM used in the study was real-time (unblinded), we cannot exclude the possibility that the small number of hypoglycemic events observed in our study resulted, at least in part, from actions taken to prevent predicted hypoglycemia. No additional sensor calibrations were performed as such approach is not required for maintaining device performance and would increase work overload. In worst scenario, inappropriate calibrations could even lead to lower accuracy. However, there are studies demonstrating enhanced sensor accuracy if additional calibrations were performed within specific time ranges. 37
Nevertheless, the results of our study offer further real-world evidence supporting the accuracy of Dexcom G7/One+ in hospitalized adults with diabetes. Consistent with other studies on Dexcom G7/One+ use in hospitals, the new generation of CGM by Dexcom is characterized by improved accuracy, showing that Dexcom G7/One+ is a valuable tool to monitor glucose levels in hospitalized patients.
Conclusions
In patients with diabetes or stress hyperglycemia admitted to the cardiac intensive care unit for HF or acute coronary syndrome, the Dexcom One+ system demonstrated acceptable accuracy and could facilitate glucose monitoring. Its enhanced features could reduce the overall management burden in CICU.
Authors’ Contributions
J.H.: Conception and design, data acquisition, data analysis, and drafting the article; B.Z.: Data acquisition; M.A.H.: Data acquisition; M.B.: Data acquisition; S.B.: Conception and design; T.K.: Conception and design, supervision, and critical revision; M.T.M.: Conception and design, supervision, and critical revision.
Footnotes
Author Disclosure Statement
J.H. has received fees from Dexcom for lecturing; T.K. and M.T.M. have received fees from Abbott Diabetes Care, Ascensia, Dexcom, and Medtronic for lecturing and participating in the advisory panels. M.B., B.Z., M.A.H., and S.B. declare no conflict of interest related to this article.
Funding Information
Funding: Jagiellonian University Medical College Grant awarded to J.H. (N41/DBS/001471, N41/DBS/001195).
Bioethics Committee Approval
The study was approved by the Jagiellonian University Bioethics Committee (1072.6120.49.2024, 1072.6120.21.2025) and conducted in accordance with the Helsinki Declaration. All patients gave written informed consent prior to inclusion in the study.