
Abstract
Objective:
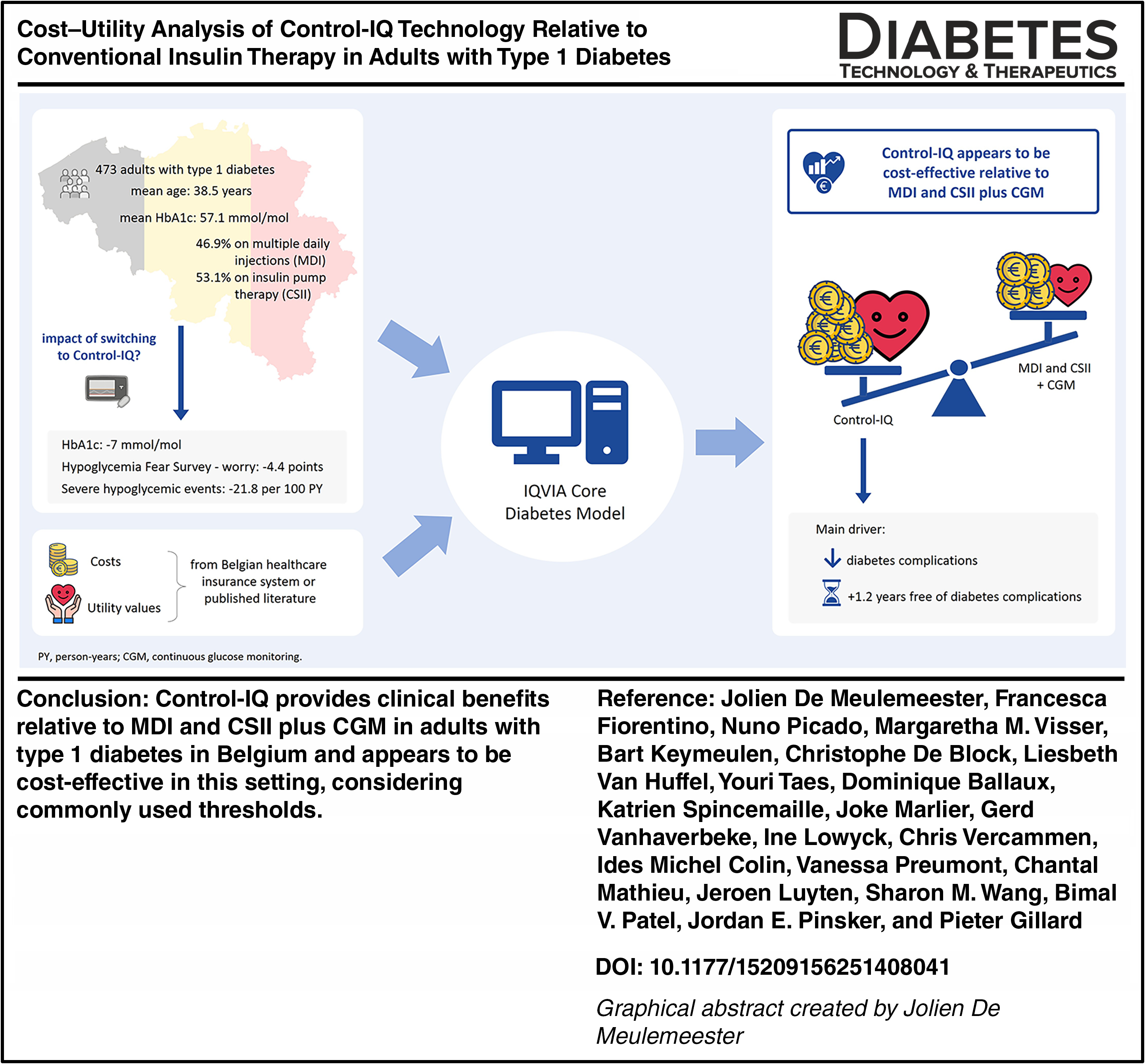
This study evaluated the cost utility of the t:slim X2 insulin pump with Control-IQ technology (Control-IQ) relative to multiple daily injections (MDIs) and standard insulin pump therapy, both used in combination with continuous glucose monitoring (CGM), in adults with type 1 diabetes from a payer perspective in Belgium.
Research Design and Methods:
A lifetime cost–utility analysis was conducted using the IQVIA CORE Diabetes Model. Baseline characteristics and treatment effects were informed by the Belgian real-world, multicenter, prospective INRANGE study. Direct medical costs included treatment, complication management, and severe hypoglycemic events. Country-specific costs were based on RIZIV-INAMI data and other publicly available sources. Utility values were based on published literature and included the reduction in fear of hypoglycemia associated with Control-IQ as reported in the INRANGE study. Outcomes included quality-adjusted life years (QALYs) and incremental cost–utility ratios (ICURs). Scenario analyses explored variations in the comparator (MDI + CGM only), reduced HbA1c efficacy, and time horizon.
Results:
Control-IQ yielded 19.50 QALYs versus 17.92 for MDI and standard insulin pump therapy plus CGM, with total costs of €193,588 and €160,129, respectively, resulting in an ICUR of €21,111/QALY. Scenario analyses confirmed robustness: MDI + CGM as sole comparator (ICUR: €41,701/QALY), reduced HbA1c efficacy (ICUR: €25,967/QALY), and a 20-year time horizon (ICUR: €30,183/QALY).
Conclusions:
Control-IQ provides clinical benefits relative to MDI and standard insulin pump therapy plus CGM in adults with type 1 diabetes in Belgium and appears to be cost-effective in this setting, considering commonly used thresholds. These findings support the broader adoption of automated insulin delivery systems in diabetes management.
Keywords
Introduction
Globally, more than 9 million individuals are living with type 1 diabetes, and this number is projected to rise to 14.7 million by 2040. 1 This growing prevalence poses a major clinical and economic challenge, as effective diabetes management necessitates lifelong intensive insulin therapy and glucose monitoring to mitigate acute complications and reduce the risk of long-term micro- and macrovascular complications. From an economic perspective, the burden of type 1 diabetes encompasses not only direct medical costs, such as insulin, glucose monitoring devices, insulin delivery systems, structured education and follow-up, and hospitalizations, but also substantial indirect costs, such as productivity loss from diabetes-related complications and premature mortality.2–4
In recent years, technological advances have sought to ease the demands of diabetes self-management while improving clinical outcomes. Automated insulin delivery (AID) systems have emerged as a promising approach by integrating continuous glucose monitoring (CGM) with algorithm-driven insulin delivery, thereby minimizing the need for constant manual adjustments. One such system, the t:slim X2 insulin pump with Control-IQ technology (Control-IQ; Tandem Diabetes Care, San Diego, CA, USA), automatically adjusts basal insulin delivery based on 30-min glucose predictions to maintain glucose levels within the target range of 6.3–8.9 mmol/L. 5 Several randomized controlled trials (RCTs) 6 and real-world studies7–10 have demonstrated the superiority of Control-IQ over other insulin regimens, with consistent improvements in time in range (TIR, 3.9–10 mmol/L) of 0.5%–13.0%, reductions in HbA1c of 3–7 mmol/mol (0.3%–0.7%) and time in hypoglycemia of 0.1%–3.0%, and favorable effects on person-reported outcomes (PROs), including less diabetes distress and more treatment satisfaction.
Despite these well-established clinical benefits, the higher upfront and ongoing costs of AID systems compared with multiple daily injections (MDIs) or standard insulin pump therapy have resulted in cautious and often restrictive reimbursement policies in many countries. In Belgium, for instance, reimbursement of Control-IQ was made conditional upon the prospective collection of real-world data on both glycemic outcomes and PROs over a 12-month follow-up period in select diabetes centers.7,8 As health care payers face increasing budgetary constraints, the widespread adoption of advanced technologies must be justified not only by robust clinical evidence but also by long-term evaluations demonstrating cost-effectiveness and financial sustainability in a broad population. To date, only one cost-effectiveness analysis with Control-IQ has been published, involving 84 children with type 1 diabetes, showing the system to be cost-saving compared with MDI or standard insulin pump therapy combined with CGM. 11
Using Belgian real-world data, 7 this study aimed to provide comprehensive evidence on the cost utility of Control-IQ relative to MDI and standard insulin pump therapy in adults with type 1 diabetes from a Belgian health care payer perspective.
Methods
Model structure
This cost–utility analysis (CUA) was conducted using the IQVIA CORE Diabetes Model (CDM, version 10), a validated and widely used, non-product-specific simulation tool designed to estimate long-term clinical and economic outcomes of interventions for people with type 1 or type 2 diabetes. The CDM comprises 17 interdependent Markov submodels that simulate the progression of diabetes-related micro- and macrovascular complications. Transitions between health states are based on probabilities derived from landmark studies, such as the Swedish National Diabetes Registry (SNDR) 12 and United Kingdom Prospective Diabetes Study (UKPDS),13,14 and depend on short-term inputs such as population characteristics, disease states, and treatment effects. Risk equations from the SNDR were used for cardiovascular complications prediction. 12 UKPDS-90 was used to inform risk factor progression for systolic blood pressure, body mass index, high-density lipoprotein, and low-density lipoprotein over time. 13 Mortality prediction was based on a combined UKPDS-82 mortality approach. 14 The CDM has undergone rigorous validation for both short- and long-term projections and is adaptable to country-specific health care systems, making it a robust instrument for informing reimbursement and policy decisions in diabetes care.15–17
Key model outputs reported in this CUA include cumulative incidence and time to onset of diabetes-related complications, years free of complications, quality-adjusted life years (QALYs), and (in)direct costs. The primary outcome was the incremental cost–utility ratio (ICUR), expressed as the incremental cost per additional QALY gained with Control-IQ versus conventional insulin therapy (hereafter referred to as the comparator, including MDI with CGM and standard insulin pump therapy with CGM).
Baseline cohort characteristics and treatment effects
Baseline cohort characteristics and treatment effects were primarily derived from the INRANGE study (ClinicalTrials.gov identifier: NCT04414280), which was a 12-month multicenter, prospective, observational real-world study involving 473 adults with type 1 diabetes who initiated Control-IQ between December 2021 and December 2022 across 13 participating centers in Belgium. No inclusion criteria were defined, leaving the decision of which adult to start Control-IQ to the clinical judgment of the treating health care professional at each center. Data were collected at the start and at 4, 8, and 12 months of routine follow-up. The primary end point was the change in TIR from start to 12 months after the start of Control-IQ. A detailed description of the methods and results of the INRANGE study has been published previously. 7 Where necessary, data from the INRANGE study were supplemented with data from other published studies (Table 1).
Baseline Cohort Characteristics
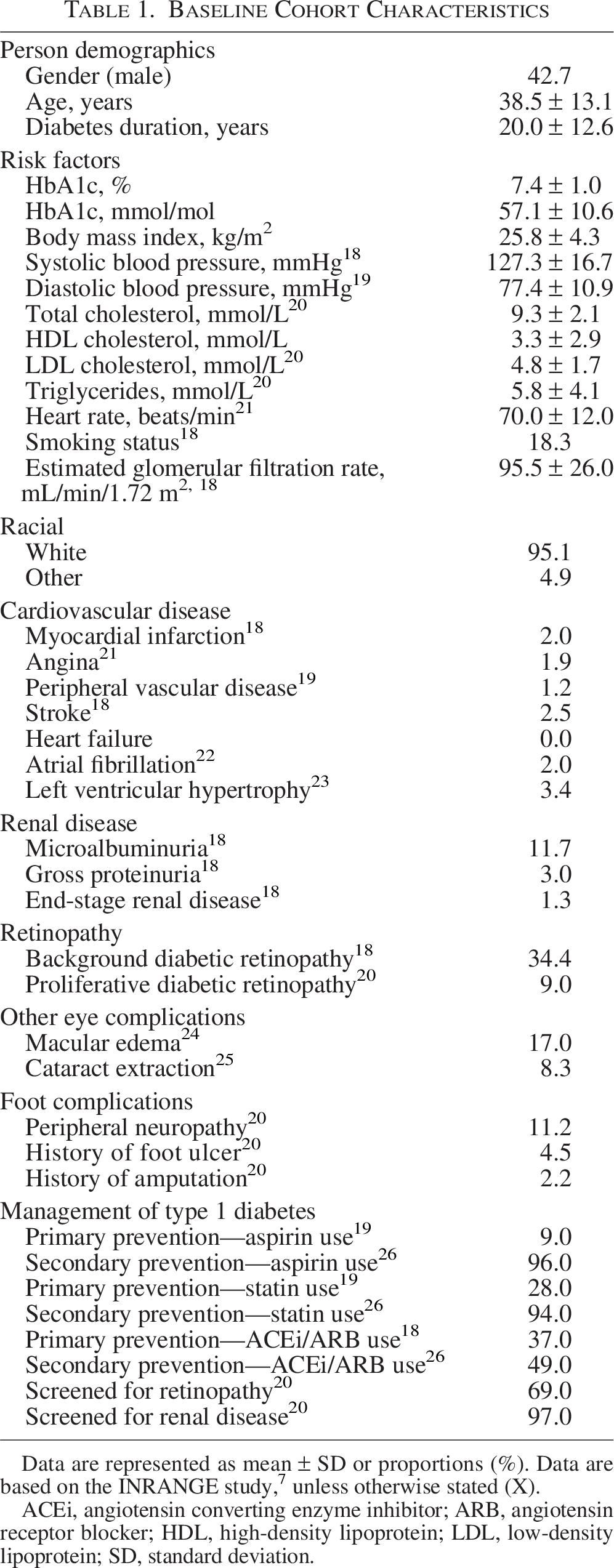
Data are represented as mean ± SD or proportions (%). Data are based on the INRANGE study, 7 unless otherwise stated (X).
ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
The baseline cohort had a mean age of 38.5 ± 13.1 years and a mean HbA1c of 57.1 ± 10.6 mmol/mol (7.4 ± 1.0%). In the INRANGE study, HbA1c decreased significantly from 57.3 mmol/mol (95% confidence interval [CI] 56.1–58.5) (7.4% [95% CI 7.3–7.5]) at start to 49.5 mmol/mol (95% CI 48.5–50.6) (6.7% [95% CI 6.6–6.8]) at 12 months, corresponding to a mean reduction of 7 mmol/mol (95% CI 6–8 mmol/mol) (0.7 percentage points [95% CI 0.6–0.8]). This treatment effect of 7 mmol/mol (95% CI 6–8 mmol/mol) (0.7 percentage points [95% CI 0.6–0.8]) was applied in the CDM during the first year of simulation and was assumed to persist unchanged over the remaining modeled time horizon. HbA1c in the comparator group was assumed to remain stable at start levels (57.1 mmol/mol [7.4%]) throughout the modeled period. Rates of severe hypoglycemic events (SHEs) were also drawn from the INRANGE study: the number of self-reported SHEs was found to decrease significantly from 37.5 (21.3–65.9) events per 100 person-years in the 12-month period before start of Control-IQ to 15.7 (9.7–25.3) events per 100 person-years during the study.
Costs
The CUA was conducted from a Belgian health care payer perspective, considering only direct medical costs related to type 1 diabetes management. Direct nonmedical costs (e.g., transportation costs) and productivity losses were excluded. Costs associated with diabetes-related health states or events and concomitant medications were sourced from the literature and inflated to 2025 values using the health consumer price index 27 (Supplementary Table S1). Treatment costs were defined by the standard reimbursement conventions for people with type 1 diabetes in Belgium (Supplementary Data S1). In the base-case analysis, Control-IQ was priced at €16.53/day (or €6037.58/year) and the comparator at a weighted average cost of €11.84/day (or €4323.30/year) based on the proportion of participants in the INRANGE study on MDI (46.9%) versus standard insulin pump therapy (53.1%) at baseline. A temporary reimbursement scenario, reflecting higher pricing for Control-IQ in a limited number of Belgian centers, was included in the one-way sensitivity analysis (€22.53/day during the first year and €16.53/day in subsequent years; Supplementary Data S2).
Health state (dis)utilities
Utility and disutility values for diabetes-related health states and events were obtained from published sources (Supplementary Table S2). A utility value reflects the strength of the preference of an individual for a given health state or event, with 1 representing perfect health, 0 representing death, and negative values representing states or events worse than death. A disutility value represents the reduction in utility due to the negative impact of a certain health state or event (e.g., diabetes complication) and is expressed as a negative value. For people with type 1 diabetes without complications, a mean utility score of 0.839 was used based on the EuroQol-5 Dimension Questionnaire. 28 To account for improvements in health-related quality of life related to reduced fear of hypoglycemia (FoH), the model incorporated an additional utility benefit derived from data of the INRANGE study. FoH was measured using the Hypoglycemia Fear Survey (HFS)—worry subscale, with the total score ranging from 0 to 72 and higher scores indicating more concerns about hypoglycemia. Over 12 months, the mean HFS—worry score decreased from 22.5 points (21.3–23.7) to 18.1 points (17.0–19.3), reflecting a reduction of 4.4 points. 7 Based on prior literature linking a one-point reduction in HFS—worry score to a utility gain of 0.008, this corresponds to a utility increase of 0.0352 associated with Control-IQ use. 29 A minimum approach for quality-adjusted life expectancy estimation was used, in which the utility score of the event with the lowest quality of life was applied when handling multiple adverse events.
Time horizon and discount rates
The base-case analysis was performed over a lifetime horizon to capture the full health impact of the intervention. In accordance with Belgian guidelines for economic evaluations and budget impact analyses, future costs were discounted at an annual rate of 3% and future clinical outcomes at an annual rate of 1.5%. 30
Sensitivity analyses
Sensitivity analyses were conducted to assess the impact of parameter uncertainty on the estimated cost–utility outcomes.
A probabilistic sensitivity analysis (PSA) was performed by assigning probability distributions to key model parameters, including baseline cohort characteristics, treatment effects, utility values, and cost inputs. When possible, these distributions were informed by their reported measures of variance (standard deviation or standard error). The model was run 1000 times using Monte Carlo simulation, with each iteration randomly sampling from the defined distributions. This process generated a unique set of input values per iteration, from which incremental costs and incremental QALYs were calculated. The results were plotted on a cost-effectiveness plane to evaluate robustness of the model under parameter uncertainty. Additionally, based on these PSA results, a cost-effectiveness acceptability curve (CEAC) was generated to illustrate the probability of Control-IQ being cost-effective across willingness-to-pay (WTP) thresholds ranging from €0 to €100,000 per QALY gained.
A series of one-way sensitivity analyses was conducted to test the impact of individual model assumptions (Supplementary Data S2). Parameters such as treatment effects, costs, utility values, time horizon, and discounting rates were varied independently relative to the base case, while holding all other inputs constant. For each scenario, the probability of Control-IQ being cost-effective at a WTP threshold of €50,000 per QALY gained was calculated. 31
Results
Base-case analysis
In the base case, use of Control-IQ resulted in a mean gain of 1.58 QALYs per participant relative to conventional insulin therapy use. Mean total direct costs were projected to be €33,459 higher with Control-IQ (€193,588) than with the comparator (€160,129), primarily due to higher treatment costs (Supplementary Fig. S1). Combining incremental costs and the gain in QALYs with Control-IQ versus the comparator yielded an ICUR of €21,111 per QALY gained from the Belgian health care payer perspective (Table 2).
Results of Base-Case Analysis and One-Way Sensitivity Analyses

In each sensitivity analysis, one parameter was varied (decreased or increased) relative to the base case (see Supplementary Data S2 for a more detailed overview of the one-way sensitivity analyses performed). Data for costs and QALYs are mean values. *Dominant indicates that Control-IQ was both less expensive and more effective compared with standard insulin pump therapy.
FoH, fear of hypoglycemia; ICUR, incremental cost–utility ratio; MDI, multiple daily injections; QALY, quality-adjusted life year; SHE, severe hypoglycemic event; TIR, time in range; WTP, willingness-to-pay.
Higher device costs were partly offset by a reduction in costs associated with a lower cumulative incidence of diabetes-related complications over the lifetime horizon. For example, the projected cumulative incidence of proliferative diabetic retinopathy was estimated at 5.8 cases per 100 participants in the Control-IQ group versus 13.3 cases per 100 participants for the comparator group (Fig. 1). On average, individuals using Control-IQ lived 1.2 additional years free of complications relative to those receiving conventional insulin therapy (Supplementary Fig. S2).
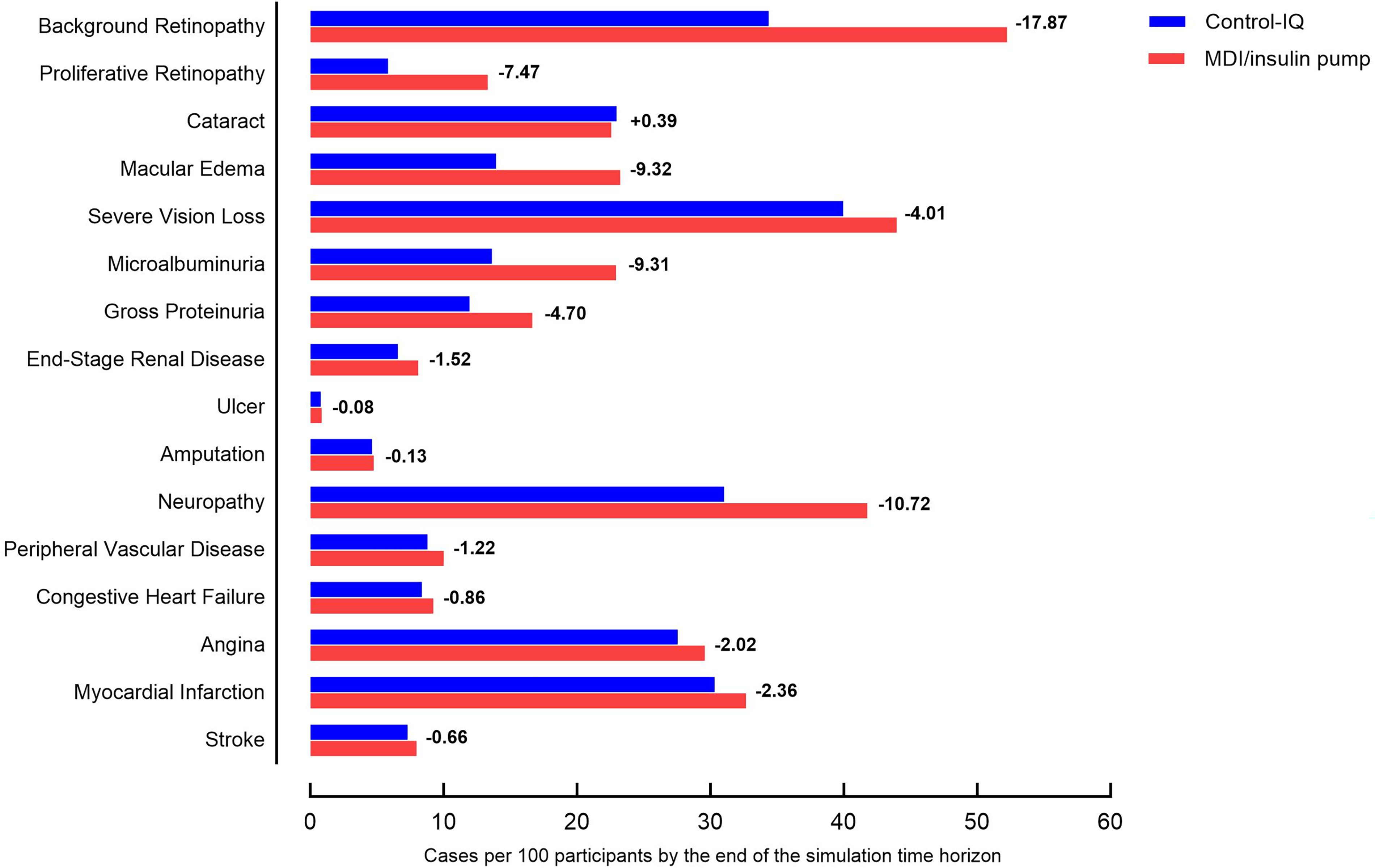
Mean projected cumulative incidence of long-term complications in the base case. The differences reflect the reduction in cases observed in the Control-IQ group. MDI, multiple daily injections.
Sensitivity analyses
In the PSA, all 1000 iterations fell within the north east quadrant of the cost-effectiveness plane, indicating that Control-IQ consistently provided QALY gains at higher costs versus the comparator (Fig. 2A). The ICURs were tightly clustered, demonstrating limited variability around the base-case estimate. The CEAC derived from the PSA showed that at WTP thresholds of €20,000, €30,000, €40,000, and €50,000 per QALY gained, the probability of Control-IQ being cost-effective was 41.2%, 92.9%, 99.2%, and 99.9%, respectively (Fig. 2B).
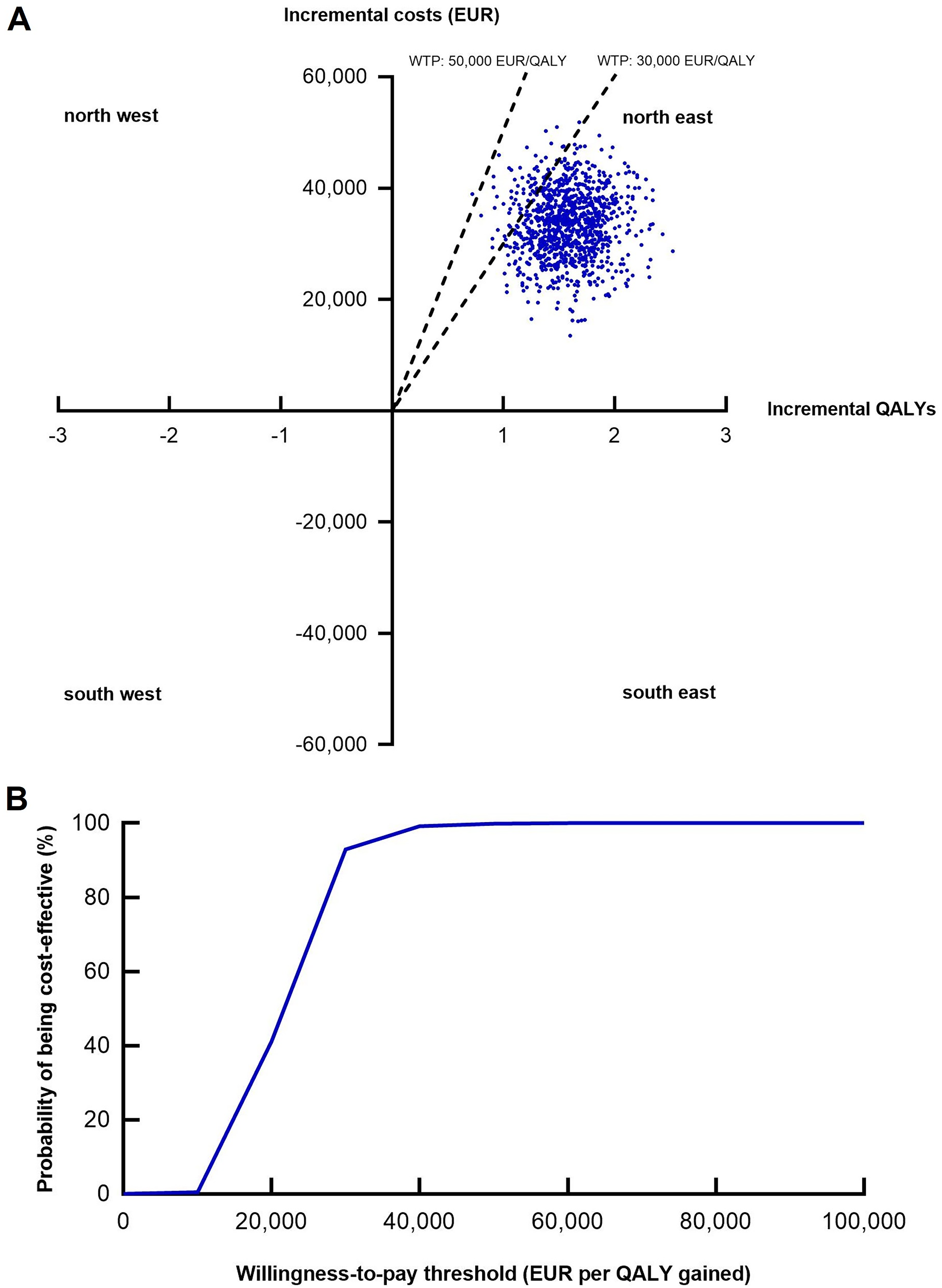
Results of the PSA for the base case.
The one-way sensitivity analyses indicated that the model was robust to variation in individual model parameters (Table 2), with Control-IQ remaining cost-effective even under assumptions of reduced QALY gains or higher direct medical costs. Varying the costs of Control-IQ or comparator had the biggest impact: increasing the daily price of Control-IQ to €22.53 in the first year and €16.53 in subsequent years (instead of €16.53 for all years) resulted in an ICUR of €50,295/QALY, using MDI plus CGM as the only comparator led to an ICUR of €41,701/QALY, while Control-IQ was dominant when compared solely with standard insulin pump therapy plus CGM. Robustness of the results was further demonstrated in scenarios with a reduced utility benefit from FoH (ICUR: €29,939/QALY), lower efficacy with a HbA1c decrease of 3 mmol/mol (0.3 percentage points; ICUR: €25,967/QALY), substitution of the treatment effect of HbA1c by a 12.1% increase in TIR (ICUR: €24,067/QALY), higher discount rates of 3% for future clinical outcomes and costs (ICUR: €28,315/QALY), and a shortened 20-year time horizon (ICUR: €30,183/QALY). Conversely, lower ICURs relative to the base case were observed under several scenarios: when complication costs were increased by 20%, when the effect of Control-IQ on SHE was increased by 50%, and when the utility benefit associated with FoH was increased by 50%.
Discussion
From a Belgian health care payer perspective and compared to conventional WTP thresholds of cost-effectiveness, 32 Control-IQ appeared to be cost-effective over conventional insulin therapy, defined as either MDI or a standard insulin pump in combination with CGM. The results proved robust across a wide range of one-way sensitivity analyses exploring alternative scenarios relative to the base case.
To the best of our knowledge, this is the first study to investigate the cost-effectiveness of Control-IQ in an adult population with type 1 diabetes. Although access to AID systems remains limited, primarily related to their higher costs, our analysis suggests that these are justified when considering the wider clinical, psychosocial, and economic benefits. The demonstrated improvement in HbA1c, reduction in SHEs, and mitigation of FoH with Control-IQ translated into long-term health gains and cost savings for the health care system. These benefits were driven by a reduced incidence and delayed onset of diabetes-related complications in the Control-IQ group, resulting in an average of 1.2 additional years living free of complications relative to the comparator.
Our results are consistent with other studies demonstrating the cost-effectiveness of AID systems across different health care settings. For example, most evaluations of the Medtronic MiniMedTM 780G were based on the ADAPT RCT, which reported a 14 mmol/mol (1.4%) reduction in HbA1c in favor of the Medtronic MiniMedTM 780G versus MDI plus intermittently scanned CGM in adults with type 1 diabetes and suboptimal glycemic management (baseline HbA1c 75 mmol/mol [9.0%]). 33 These data-informed cost-effectiveness analyses in six European countries, 34 Singapore, 35 France, 36 and the United States, 37 all of which concluded that the Medtronic MiniMedTM 780G was a cost-effective intervention in their respective health care settings. Additional studies confirmed the cost-effectiveness of the Medtronic MiniMedTM 780G in Sweden, 38 Greece, 39 and The Netherlands, 40 using comparators such as MDI, standard insulin pump, or sensor-augmented pump therapy. Similarly, favorable outcomes have been reported for Control-IQ, 11 Omnipod 5, 41 and CamAPS FX 42 in adult and pediatric populations. However, health economic evaluations are highly context-specific due to variations in device pricing, treatment costs, and national reimbursement policy, limiting the generalizability of findings across health care systems. This highlights the importance of conducting country-specific evaluations to inform national funding decisions. By using input data from the real-world INRANGE study, 7 in which all Belgian adults who were proposed to initiate Control-IQ were required to participate, we believe our population is reflective of national clinical practice.
One-way sensitivity analyses revealed that the ICUR was most sensitive to changes in Control-IQ pricing. A daily cost of €16.53, corresponding to reimbursement practice across all Belgian diabetes centers, kept the ICUR within commonly accepted WTP thresholds. 32 In line with previous health economic evaluations on AID therapy,34,36 FoH also emerged as a key driver of cost-effectiveness. This is not surprising, given the well-documented negative impact of FoH on quality of life. 43 AID systems have been shown to alleviate FoH,7,33 although more research is warranted to identify the underlying drivers of reduced hypoglycemia-related fear when using these systems.
Economic evaluations of diabetes interventions have traditionally relied on HbA1c to estimate long-term health outcomes, giving its well-established link to chronic complications. 44 In recent years, however, people with type 1 diabetes as well as health care providers have increasingly recognized the added value of TIR as a complementary measure to HbA1c. Unlike HbA1c, TIR reflects short-term glucose fluctuations and variability, thereby offering a more comprehensive picture of an individual’s daily glucose profile. 45 Although widely used in clinical practice, TIR has not yet been accepted by regulatory agencies as a validated end point for establishing efficacy claims in clinical trials, mainly because long-term prospective studies directly linking TIR to complication risk are still lacking. Nevertheless, emerging cross-sectional and retrospective evidence suggests that TIR is predictive of chronic complications.46–50 Within the IQVIA CDM version 10, a TIR-based approach was included as an alternative to HbA1c, allowing users to define treatment effects in terms of TIR rather than changes in HbA1c. Since validated cardiovascular risk equations based on TIR were not identified, the CDM internally converts changes in TIR to equivalent changes in HbA1c. This conversion is based on data from Beck et al., 51 which analyzed four RCTs involving 545 adults with type 1 diabetes, as implemented in the IQVIA CDM version 10. By contrast, Vigersky et al. reported a slightly larger change in HbA1c for the same change in TIR, based on 18 RCTs covering broader populations and technologies. 52 Using Beck et al., therefore, represents a conservative approach, likely underestimating the potential cost-effectiveness benefits. To our knowledge, this is the first peer-reviewed cost-effectiveness analysis to describe a scenario in which TIR was used as the primary measure of glycemic management. The resulting ICUR of €24,067 per QALY gained was comparable to the estimates based on HbA1c and remained well below commonly accepted WTP thresholds.
In assessing whether health care interventions are cost-effective in the Belgian setting, it is important to recognize the absence of an official reference threshold for WTP per QALY. Decisions about WTP thresholds currently weigh multiple factors, including clinical benefits, disease incidence and severity, and therapeutic positioning relative to existing interventions. Several approaches have been proposed to estimate an appropriate threshold. One based on population surveys estimated the value of an additional year in good health at the pan-European level at €40,000/QALY, although this 20-year-old estimate should be inflated to reflect current values. 53 Another widely used approach considers national prosperity, typically expressed as gross domestic product per capita, 54 which in Belgium was around €50,000 in 2024. 31 Accordingly, we adopted a threshold of €50,000/QALY in our analysis. However, given recommendations to apply multiple thresholds, 55 we also generated a CEAC to illustrate the probability of Control-IQ being cost-effective across a range of WTP values. Notably, even at a more conservative threshold of €30,000 per QALY, Control-IQ had a 92.9% likelihood of being considered cost-effective in the base case.
This study has limitations that should be acknowledged. First, while efforts were made to use input data representative of the Belgian context, cost and utility estimates were sourced from a variety of studies, some of which were conducted outside Belgium and involved different populations. For instance, Van Dongen et al. showed that utility values can vary considerably across different settings, largely due to sociocultural differences, which may in turn affect the outcomes of cost–utility analyses. 56 Although reliance on diverse data sources is common practice in health economic modeling, it highlights the importance of generating population- and country-specific data for future evaluations. Second, 12-month clinical effects were extrapolated over a lifetime horizon, which is inevitably associated with uncertainty, as is typical when projecting long-term outcomes from short-term data. However, given the limited availability of long-term studies on AID therapy, we believe our 12-month data provide a reasonable basis for extrapolating the treatment effect of HbA1c, especially as we could demonstrate that HbA1c improvements achieved within the first few months of Control-IQ tended to persist over time. Third, beyond FoH, the INRANGE study also demonstrated favorable effects of Control-IQ on treatment satisfaction, diabetes distress, and daily burden of diabetes. Incorporating these person-reported benefits into economic modeling, capturing not only the consequences of hypoglycemia but also broader psychosocial dimensions, may provide a more accurate estimate of the overall value of AID therapy. Fourth, although age-adjusted estimates could offer additional insights, particularly because individuals initiating AID therapy at different ages may experience distinct long-term benefits, the IQVIA CDM does not currently support adjustments for age at diagnosis or for age distribution of the study population. Therefore, future modeling efforts should incorporate age-stratified analyses to better account for this heterogeneity. Finally, individuals in the INRANGE study were offered Control-IQ based on their anticipated ability to benefit and adhere to treatment, reflecting real-world clinical decision-making. While this may introduce a degree of selection bias, our findings indicated that Control-IQ was cost-effective even in a relatively well-managed population (HbA1c 57.1 mmol/mol [7.4%] at baseline). The study population also showed a marked overrepresentation of participants identifying as white, with a higher proportion than observed in the general Belgian population, which may further limit generalizability. Future research should address these disparities by including underrepresented racial, ethnic, and socioeconomic groups to ensure equitable access and broader applicability across diverse populations.
In conclusion, use of Control-IQ was found to be cost-effective relative to MDI and standard insulin pump therapy in a real-world population of adults with type 1 diabetes. The QALY gains achieved with Control-IQ were sufficiently large to offset the additional costs associated with AID therapy, keeping it below commonly accepted WTP thresholds. These findings provide robust evidence to inform policymakers and health care providers in Belgium, while also adding to the international body of evidence supporting the broader adoption of AID therapy in diabetes care.
Authors’ Contributions
J.D.M. analyzed and discussed the data, made figures and tables, and wrote the article. F.F., N.P., S.M.W., B.V.P., and J.E.P. conceptualized the analysis, performed the analyses, and edited the article. B.K., C.D.B., L.V.H., Y.T., D.B., K.S., J.M., G.V., I.L., C.V., I.M.C., V.P., C.M., and J.L. analyzed and discussed the data and edited the article. P.G. and M.M.V. analyzed and discussed the data and wrote the article. All authors approved the final version to be published. J.D.M. and P.G. are guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Acknowledgments
The authors would like to thank the local investigators, the data nurses, and their teams for collecting the data in the INRANGE study.
Author Disclosure Statement
J.D.M. received research support from Tandem Diabetes Care and Dexcom via KU Leuven. J.D.M. serves or has served on the speakers bureau for Dexcom; financial compensation for these activities has been received by KU Leuven. F.F. and N.P. were employed at IQVIA at the time the study was conducted. IQVIA receives professional service commissions from various sponsors in the biopharmaceutical sector. UZ Leuven received nonfinancial support for travel from Novo Nordisk and from Boehringer Ingelheim for M.M.V. M.M.V. has served on the speakers bureau for Dexcom, and financial compensation for these activities has been received by KU Leuven. C.D.B. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Medtronic, Novo Nordisk, and Roche. L.V.H. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Medtronic, Merck Sharp and Dohme, Novo Nordisk, Sanofi-Aventis, and Roche. Y.T. reports honoraria for speaking for Boehringer Ingelheim, Eli Lilly, Daiichi Sankyo, and Bayer. K.S. reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Medtronic and Merck Sharp, and Dohme. G.V. serves, or has served, on the advisory panel for Merck Sharp and Dohme, Boehringer Ingelheim, and Eli Lilly. G.V. reports consulting fees and honoraria for speaking for Merck Sharp and Dohme, Boehringer Ingelheim, AstraZeneca, Sanofi-Aventis, Novo Nordisk, and Eli Lilly. C.V. reports honoraria for speaking for Eli Lilly. I.M.C. reports honoraria for speaking for Novo Nordisk, Eli Lilly, Sanofi, and Abbott. I.M.C. serves, or has served, on the advisory panel for Novo Nordisk, Eli Lilly, Sanofi, and Abbott. V.P. reports consulting fees and honoraria for speaking for Novo Nordisk, Sanofi, and Abbott. C.M. serves or has served on the advisory panel for Novo Nordisk, Sanofi, Merck Sharp and Dohme, Eli Lilly, Novartis, AstraZeneca, Boehringer Ingelheim, Roche, Medtronic, ActoBio Therapeutics, Pfizer, Imcyse, Insulet, Zealand Pharma, Avotres, Mannkind, Sandoz, and Vertex. Financial compensation for these activities has been received by KU Leuven; KU Leuven has received research support for C.M. from Medtronic, Imcyse, Novo Nordisk, Sanofi, and ActoBio Therapeutics; C.M. serves or has served on the speakers bureau for Novo Nordisk, Sanofi, Eli Lilly, Boehringer Ingelheim, AstraZeneca, and Novartis. Financial compensation for these activities has been received by KU Leuven. C.M. is the president of EASD. All external support of EASD is to be found on ![]() . S.W., B.P., and J.P. are employees of Tandem Diabetes Care. P.G. serves or has served on the advisory panel for Novo Nordisk, Sanofi-Aventis, Boehringer Ingelheim, Janssen Pharmaceuticals, Roche, Medtronic, Abbott, and Bayer. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the speakers bureau for Merck Sharp and Dohme, Boehringer Ingelheim, Bayer, Medtronic, Insulet, Novo Nordisk, Abbott, Roche, VitalAire, and Dexcom. Financial compensation for these activities has been received by KU Leuven. KU Leuven received for PG nonfinancial support for travel from Sanofi-Aventis, A. Menarini Diagnostics, Novo Nordisk, Medtronic, and Roche.
. S.W., B.P., and J.P. are employees of Tandem Diabetes Care. P.G. serves or has served on the advisory panel for Novo Nordisk, Sanofi-Aventis, Boehringer Ingelheim, Janssen Pharmaceuticals, Roche, Medtronic, Abbott, and Bayer. Financial compensation for these activities has been received by KU Leuven. P.G. serves or has served on the speakers bureau for Merck Sharp and Dohme, Boehringer Ingelheim, Bayer, Medtronic, Insulet, Novo Nordisk, Abbott, Roche, VitalAire, and Dexcom. Financial compensation for these activities has been received by KU Leuven. KU Leuven received for PG nonfinancial support for travel from Sanofi-Aventis, A. Menarini Diagnostics, Novo Nordisk, Medtronic, and Roche.
Funding Information
The INRANGE study was supported by a research grant from Tandem Diabetes Care and Dexcom. IQVIA received an unconditional grant from Tandem Diabetes Care for performing this cost–utility analysis. Representatives of Tandem Diabetes Care and Dexcom reviewed the article but had no role in the study design, data collection, data analysis, data interpretation, writing of the report, or the decision to submit for publication.
Data and Resource Availability
This cost–utility analysis is based on data from the original real-world, multicenter, prospective INRANGE study. Please refer to the original article for information on data availability. 7
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.