
Abstract
Objective:
Type 1 diabetes (T1D) affects around 3 million people across Europe. Despite insulin therapy, T1D can lead to diabetic ketoacidosis (DKA), microvascular and macrovascular complications, hypoglycemia, and increased mortality, placing a substantial financial burden on European health care systems. Advances in automated insulin delivery (AID) systems have shown promise in improving glycemic control. This study evaluated the affordability of AID systems compared with standard of care (multiple daily insulin [MDI] injections with intermittently scanned continuous glucose monitoring [isCGM]) by examining the budgetary impact of improved glycemic control and reduced complication rates across nine European countries.
Methods:
The model estimated the impact of T1D complications on health care costs over a 5-year time horizon, using a hypothetical cohort of 100 individuals with T1D. Two distinct populations were considered based on baseline glycemic control: those with HbA1c ≥8% and those with HbA1c <8%. The model simulated the annual incidence and progression of chronic complications and two acute complications. Incidence rates were driven by HbA1c levels, which varied by treatment and baseline population. Severe hypoglycemia events (SHEs) were modeled separately using treatment- and population-specific rates. A treatment-neutral price was assumed, with country-specific costs applied to complications.
Results:
The AID system substantially reduced complication rates compared with MDI with isCGM. Among individuals with HbA1c ≥8%, overall complications declined by 61%, including a ∼70% reduction in DKA, resulting in per-person 5-year cost savings ranging from €1595 to €2810 across the modeled countries. In those with HbA1c <8%, complications excluding SHEs fell by 26%; DKA was reduced by approximately 34%, and SHEs were eliminated, translating to per-person savings of €508 to €2819 over 5 years.
Conclusion:
This analysis highlights the health care budget that could be freed up through the use of AID systems, enabling decision-makers to improve glycemic control in people with T1D without increasing total expenditure.
Keywords
Introduction
In Europe, more than 3 million people of all ages were estimated to live with type 1 diabetes (T1D) in 2022. 2 In the same year, 34,000 deaths in Europe were attributable to this insulin-deficient state. Current therapy with multiple daily insulin (MDI) injections can help improve glucose control but does not restore it to physiological levels. As a result, glucose can accumulate in the bloodstream, potentially leading to serious outcomes such as diabetic ketoacidosis (DKA), severe hypoglycemia events (SHEs), and long-term microvascular and macrovascular complications.3–5 Estimates from Germany, for example, suggested a mean rate for DKA of 4.8 hospital admissions per 100 person-years in young people living with T1D, while 2022 data from Scotland indicated a crude rate of 1.26 severe hospitalized hypoglycemic events per 100 person-years in people living with T1D overall, with a rate of 2.30 events per 100 person-years observed in those aged <20 years.3,6 In terms of vascular complications, 18.5% of people living with T1D were estimated to present with chronic kidney disease in Sweden, and even those with preserved estimated glomerular filtration rate (eGFR) and without albuminuria were found to be at an excess risk of declines in eGFR, kidney failure, major adverse renal or cardiac events, and all-cause mortality. 7
This clinical burden is associated with a significant humanistic burden. The quality of life of both children living with T1D and their caregivers has been found to be impaired, with anxiety and depression frequently due to disease-related events such as hypoglycemia and the need for constant vigilance in managing T1D. 8
T1D also imposes considerable costs on health care systems and society, most frequently due to the treatment of diabetes-related events and complications. For T1D in the United Kingdom (UK) in 2021/2022, management costs were estimated at GBP 1.21 billion, with another GBP 74 million incurred for acute event complications and GBP 237 million and GBP 95 million, respectively, attributable to microvascular and macrovascular complications. 9 In Germany, the 2010 cost of T1D was estimated at more than EUR 1 billion, which was projected to rise to about EUR 2 billion by 2040. 10
Technological advancements in the production of insulin analogues, glucose monitoring, and automated insulin delivery (AID) systems have improved glycemic control, contributing to a reduction in the clinical, humanistic, and economic burden of T1D.5,9,11,12 Prior modeling for the UK, for example, suggested that achieving a target glycated hemoglobin (HbA1c) level of 7.0% (53 mmol/mol) instead of 8.5% (69 mmol/mol) would reduce cumulative direct costs by GBP 687 million over 5 years, leading to total savings of more than GBP 1 billion, or GBP 8400 per person, when also considering indirect costs. 13 Diabetes technologies, in general, have been found not only to improve glucose outcomes but also to promote improved health behavior and well-being, while AID systems specifically were found, in a meta-analysis of randomized controlled trials, to increase time in range (TIR), improve HbA1c, and reduce diabetes distress, without a loss in safety.14–16
Despite the advantages of AID systems, concerns around cost have limited their uptake in some settings, necessitating comprehensive health economic assessments. 17 Such assessments typically include an evaluation of cost-effectiveness and affordability. 18 The cost-effectiveness of AID systems has already been established, for example, for the MiniMed™ 780 G (MM™ 780G) system (Medtronic, Northridge, CA), which was found cost-effective versus standard of care—usually consisting of intermittently scanned continuous glucose monitoring (isCGM) with self-injection of MDI or continuous subcutaneous insulin infusion (CSII)—in multiple settings, including Austria, Greece, Italy, The Netherlands, Spain, and Sweden.19,20 Evaluations of affordability, implemented using budget impact analysis (BIA), however, are still lacking for AID systems.
The present study, therefore, aimed to assess the affordability of AID systems (MM 780G) with a hybrid closed-loop system relative to MDI with isCGM, based on their respective effectiveness for achieving glycemic control. The analysis considered two distinct populations defined by baseline HbA1c levels: those with HbA1c ≥8%, representing individuals with elevated HbA1c, and those with HbA1c <8%, representing individuals with lower HbA1c. The analysis was designed to project the budget impact of increased AID use in nine European countries (Austria, France, Germany, Greece, Italy, The Netherlands, Spain, Sweden, and the UK), in order to facilitate a multicountry perspective on AID system affordability across both clinically relevant groups.
Methods
A budget impact model (BIM) was developed in Microsoft Excel. The BIM used a hypothetical cohort of 100 adults with T1D over a 5-year time horizon and modeled costs from a health care payer perspective. The incidence of complications was calculated based on the risk of each complication for each treatment, with country-specific costs applied.
Model Structure
To estimate the impact of diabetes complications on health care costs, the model employed a structured approach to model the incidence and history of complications in T1D, and has been previously used as the basis of a UK BIA. 13 The model operated with a yearly cycle length, with complications assessed in each cycle. It incorporated a number of economically consequential chronic complications commonly associated with T1D, as reported in the DCCT/EDIC studies, including retinopathy (proliferative diabetic retinopathy, macular edema, laser treatment, and blindness), nephropathy (macroalbuminuria, renal insufficiency, and kidney transplant), neuropathy (neuropathy, ulcers, and amputations), and cardiovascular disease (CVD) (angina, myocardial infarction, heart failure, and stroke).21,22 Acute complications included DKA and SHEs.
The simulated cohort entered the model with all individuals initially at risk of both acute and chronic complications (Fig. 1). Individuals who did not experience a complication in a given cycle remained at risk in the next cycle. Those who experienced an acute complication were assumed to recover within one cycle and then reenter the at-risk cohort, becoming susceptible to future complications.
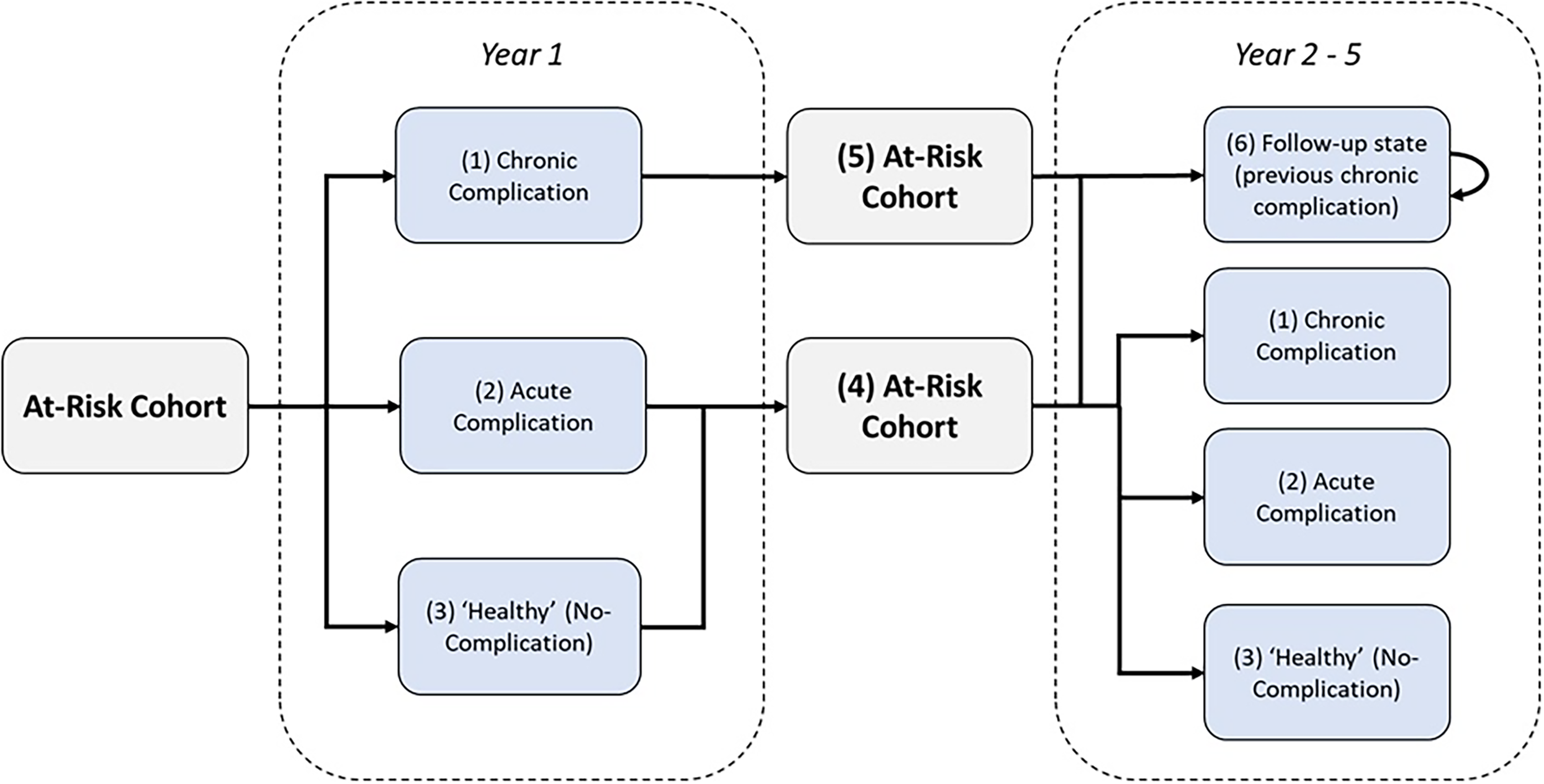
Model schematic. Upon model initiation, the entire cohort is classified as “at-risk,” meaning all individuals are eligible to experience either a chronic or acute complication in year 1. Individuals who develop chronic complications (retinopathy, nephropathy, neuropathy, or cardiovascular disease) transition to the chronic complication state. Those who experience acute complications (diabetic ketoacidosis [DKA] or severe hypoglycemic events [SHEs]) enter the acute complication state. The number of individuals entering each complication state is calculated by multiplying the size of the at-risk cohort by the probability of each complication. Individuals who do not experience any complications in year 1 transition to the healthy state and reenter the at-risk cohort in year 2. Acute complications are assumed to resolve within one cycle, with individuals returning to the at-risk cohort in the following year. Those who develop chronic complications enter a follow-up state specific to the complication and also return to the at-risk cohort for year 2 but are no longer eligible to experience the same chronic complication again. This process repeats in each annual cycle. Individuals may accumulate multiple complications over time, but each chronic complication can only occur once. The total number of complications (acute and chronic) is summed over the 5-year model horizon.
Individuals who experienced a chronic complication transitioned to a follow-up status in the next cycle, where they remained for the remainder of the analysis time horizon. They also reentered the at-risk cohort and remained susceptible to other complications, both acute and chronic, but were unable to experience the same chronic complication again. As a result, individuals could experience multiple different acute and chronic complications over time, but each chronic complication could only occur once.
To simplify the model, mortality was not considered, reflecting the short time horizon typical of BIAs. The total population size therefore remained constant throughout. In each cycle, individuals were assigned to one of the following complication-related states: (1) experiencing a new chronic complication, (2) experiencing an acute complication, or (3) no complications. In parallel, individuals could also occupy the follow-up state if they have previously experienced a chronic complication.
Country-specific costs were applied to each complication and inflated to the present year as needed. For some chronic complications, the resource use, and therefore costs, differed between the first year and subsequent years, resulting in different costs for the incident cycle versus later cycles. The incidence of complications was assumed to be consistent across countries.
Model Outputs
Key model outputs included the incidence of acute and chronic events, and total and per-person cost savings, both annually and cumulatively, over the 5-year model time horizon for each country.
Model Inputs
Complication rates
The complication rates for both treatment arms were based on HbA1c levels. For individuals with baseline HbA1c ≥8%, expected values were 9.00% for MDI with isCGM and 7.38% for AID, derived from a custom regression model developed using individual patient-level data from the ADAPT trial. ADAPT was a multicenter, randomized controlled study in adults with T1D and HbA1c ≥8%, comparing 6-month outcomes of an advanced AID system versus MDI plus isCGM, with change in HbA1c as the primary end point. 16 Given the high baseline HbA1c and the anticipated minimal difference between treatment arms, SHEs were not considered in this population.
For individuals with a baseline HbA1c <8%, expected values were 7.43% for those on MDI with isCGM and 6.87% for those using AID, derived from a prospective study involving adolescents and adults with T1D who initiated AID system using either the MiniMed 780 G or Tandem t:slim X2 systems, which assessed glycemic control and patient-reported outcomes over a 3-month follow-up period.23,24 Using data from the same study, individuals on MDI were estimated to experience SHEs requiring hospitalization at a rate of 10.7 events per 100 person-years, modeled as an acute complication.23,24 In contrast, individuals using AID were assumed to experience no SHEs requiring hospitalization. This reflects the known risk of SHEs in individuals treated with MDI, particularly in the context of tighter glycemic control without automated insulin adjustment.
Due to variability in data across complication types, different methods were used to estimate annual incidence. For retinopathy, nephropathy, and neuropathy, a relative risk (RR) adjustment was applied: the baseline absolute annual rate from a reference study was modified by the ratio of RRs for the treatment arms compared with the reference, based on HbA1c levels and assuming a linear relationship between RR and HbA1c. 25 At an HbA1c level of 7.1%, the 30-year probability of retinopathy and nephropathy was 21% and 9%, respectively, corresponding to annual probabilities of 0.783% and 0.314%. 21 For neuropathy, the 6.5-year probability was 5.81% at an HbA1c level of 7.4%, translating into an annual probability of 0.783%. 26 For CVD, a hazard ratio (HR) approach was used. An HR of 1.25 was derived from a proportional hazards model accounting for time-dependent covariates and treatment groups, representing a 25% increased risk of CVD for every 10% increase in HbA1c from the study baseline of 7.4%. 21 The study’s baseline CVD risk was then scaled according to this HR, based on the HbA1c differences between the treatment arms and the baseline. For DKA, an exponential function was used to model annual incidence directly as a function of HbA1c levels. 3
Using these approaches, the estimated annual incidence rates of complications for individuals with baseline HbA1c ≥8% on MDI with isCGM were: 1.97% for retinopathy, 0.70% for nephropathy, 1.62% for neuropathy, 0.54% for CVD, and 7.27% for DKA. In contrast, individuals using AID experienced lower incidence rates across all complications due to their comparatively lower HbA1c levels: 0.90% for retinopathy, 0.35% for nephropathy, 0.94% for neuropathy, 0.38% for CVD, and 2.16% for DKA.
For individuals with baseline HbA1c <8%, the estimated annual complication rates on MDI with isCGM were: 0.92% for retinopathy, 0.36% for nephropathy, 0.96% for neuropathy, 0.38% for CVD, and 2.24% for DKA. Those using AID again showed lower rates: 0.70% for retinopathy, 0.28% for nephropathy, 0.78% for neuropathy, 0.34% for CVD, and 1.47% for DKA.
Complication costs
Each complication was associated with its own incidence rate and cost, with the costs split by incident year and subsequent years where appropriate (Supplementary Table S1). Weighted complication costs were derived by combining the frequency and costs of the respective subcomplications, with costs inflated to the current year where required.
For retinopathy, the subcomplications included proliferative diabetic retinopathy, macular edema, laser treatment, and blindness, with 30%, 39%, 30%, and 2% weightings applied, respectively. 5 For nephropathy, the subcomplications included macroalbuminuria, renal insufficiency, and renal transplantation, with 66%, 24%, and 10% weightings applied, respectively. 21 For neuropathy, the subcomplications included neuropathic signs and symptoms, ulceration, and amputation, with 94%, 4%, and 2% weightings applied, respectively. 27 For CVD, the subcomplications included angina, myocardial infarction, heart failure, and stroke, with 36%, 15%, 35%, and 14% weightings applied, respectively. 28 It was assumed that severe hypoglycemic episodes would require hospital care (100%). The cost of DKA was input as a single value.
Treatment costs
The model used a treatment-neutral approach, enabling the estimation of the potential investment each respective health care system could make in significantly improving diabetes control without increasing total budget expenditure.
Results
Baseline HbA1c >8%
Over the 5-year period, the model estimated a 61% reduction in all complications among individuals with a baseline HbA1c ≥8% treated with the AID system compared with MDI with isCGM. Reductions were observed across all chronic complications, including retinopathy (61%), nephropathy (53%), neuropathy (49%), and CVD (41%) (Table 1 and Fig. 2). The largest reduction was in the incidence of DKA, which decreased by approximately 70% with the use of the AID system.
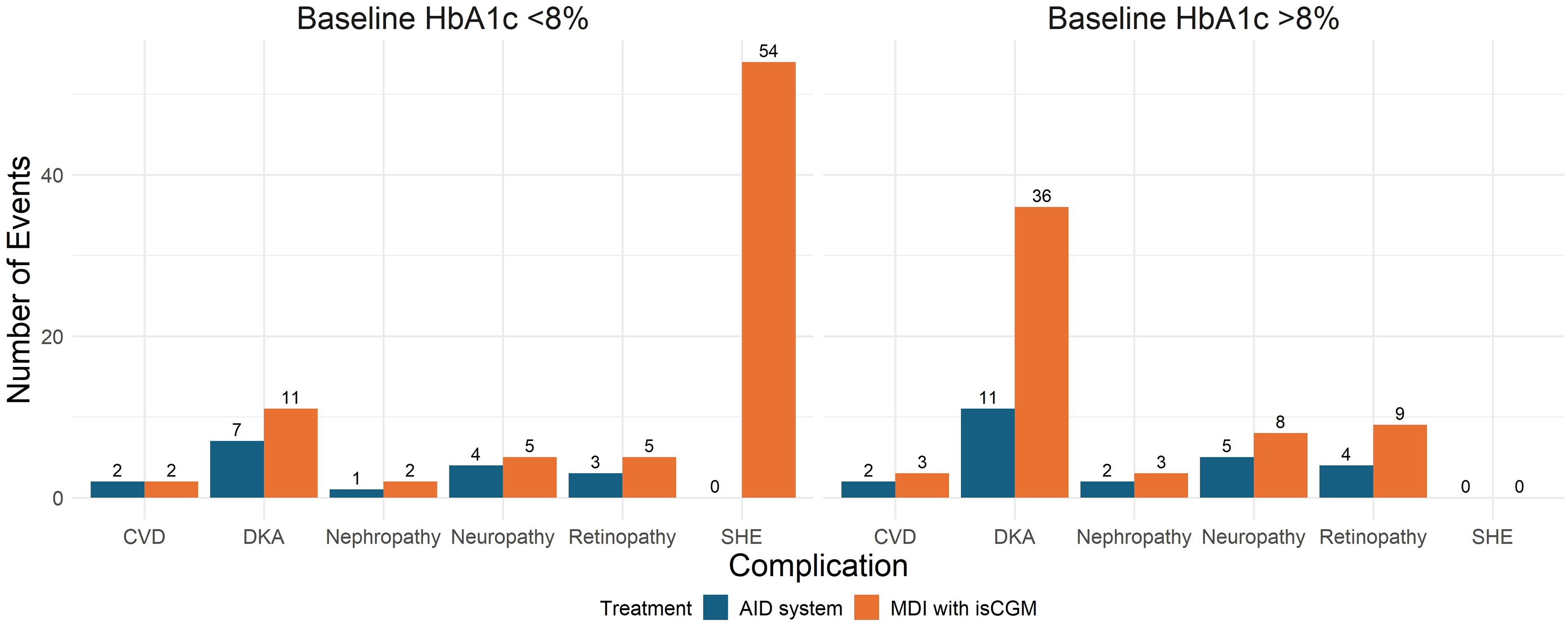
Five-year cumulative incidence of diabetes-related complications by treatment type and baseline HbA1c level in a modeled cohort of 100 individuals with type 1 diabetes. Rates were rounded to the nearest whole number. AID, automated insulin delivery; CVD, cardiovascular disease; isCGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injections.
Model-Estimated Number of Diabetes-Related Complication Events Over 5 Years in a Hypothetical Cohort of 100 Individuals with T1D Treated with AID Versus MDI with isCGM, Stratified by Baseline HbA1c (≥8% and <8%), Applicable Across All Modeled Countries
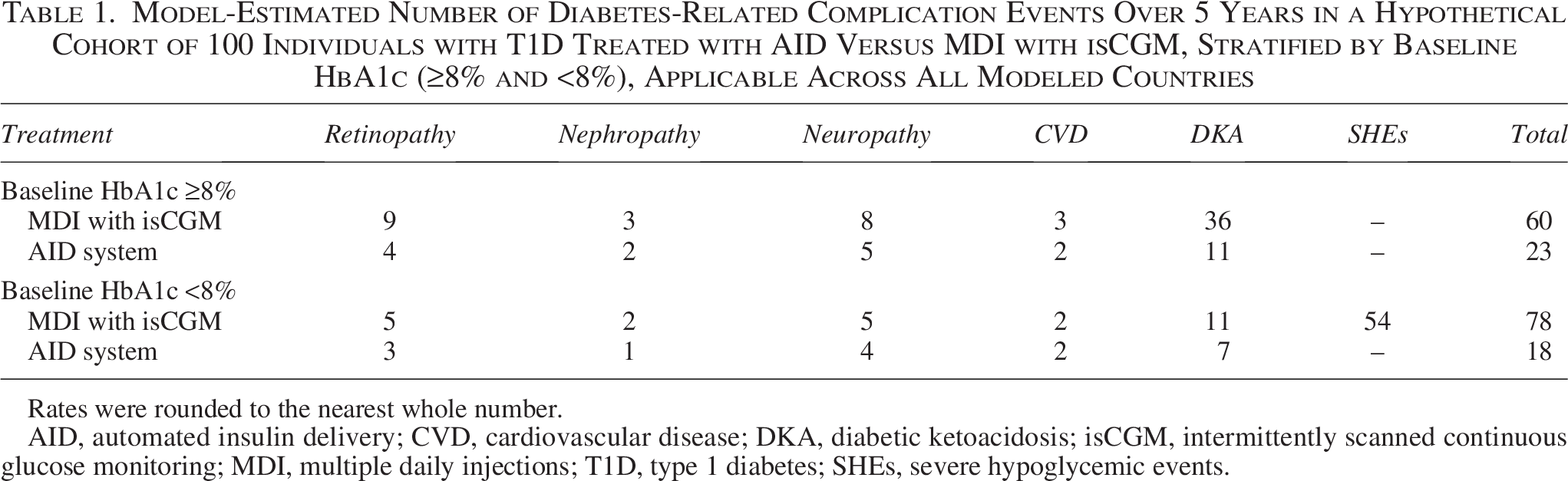
Rates were rounded to the nearest whole number.
AID, automated insulin delivery; CVD, cardiovascular disease; DKA, diabetic ketoacidosis; isCGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injections; T1D, type 1 diabetes; SHEs, severe hypoglycemic events.
These clinical benefits translated into significant cost savings across all modeled countries, both cumulatively over the 5-year horizon and annually. The 5-year per-person cost savings ranged from €1595 in The Netherlands to €2810 in France (Table 2 and Fig. 3).
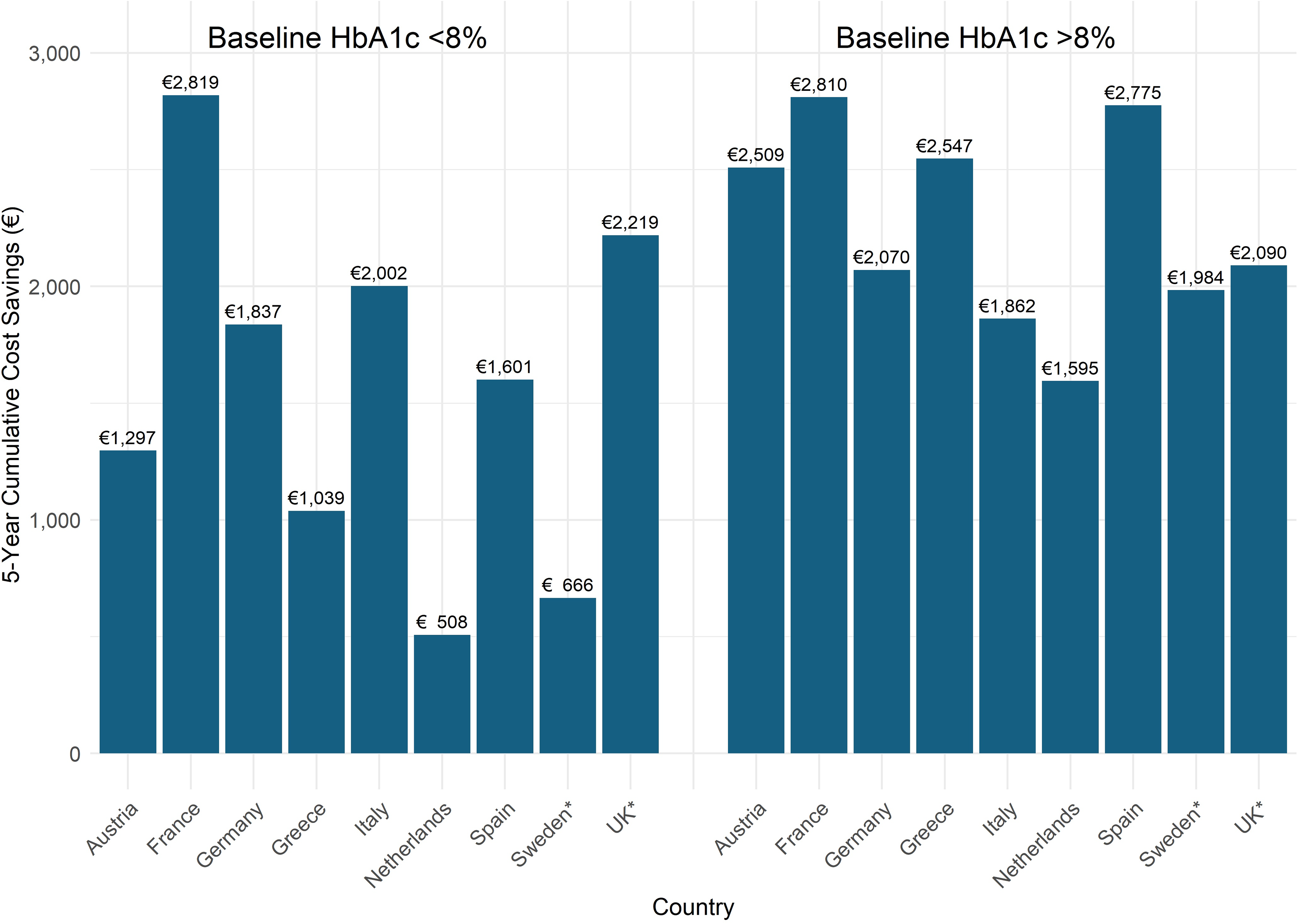
Five-year cumulative cost savings per individual with type 1 diabetes by country and baseline HbA1c level. *Converted to 2024 euros to allow for comparison.
Per-Patient Cost Saving Over 5 Years in Individuals with T1D Treated with AID Versus MDI with isCGM, Stratified by Baseline HbA1c (≥8% and <8%), by Country

Converted to 2024 Euros to allow for comparison.
These findings suggest that in populations with elevated HbA1c, AID systems may provide substantial clinical and financial benefits within a relatively short timeframe.
Baseline HbA1c <8%
Similar trends were observed in individuals with a baseline HbA1c <8%, with the AID system associated with a 26% reduction in all complications over 5 years compared with MDI with isCGM (excluding SHEs). Reductions were observed across all chronic complications, including retinopathy (24%), nephropathy (21%), neuropathy (18%), and CVD (12%) (Table 1 and Fig. 2). The incidence of the acute complication DKA also declined significantly, with a reduction of approximately 34%. Notably, the largest difference in this population was in the incidence of SHEs requiring hospitalization, which dropped from 54 events in the MDI with isCGM group to zero events in the AID group over the modeled time horizon.
Again, these clinical benefits translated into significant cost savings across all modeled countries, both cumulatively over the 5-year horizon and annually. The 5-year per-person cost savings ranged from €508 in The Netherlands to €2819 in France (Table 2 and Fig. 3).
In individuals with a baseline HbA1c <8%, the elimination of SHEs alongside reductions in other chronic and acute complications may offer meaningful savings, reinforcing the case for wider AID adoption.
Discussion
The present analysis showed that use of the AID system could reduce expenditure on diabetes-related complications over a short 5-year time horizon across all modeled European countries, for individuals with both elevated HbA1c (HbA1c ≥8%) and lower HbA1c (HbA1c <8%) at baseline. Cost savings ranged from €1595 in The Netherlands to €2810 in France for individuals with a baseline HbA1c ≥8%, and from €508 in The Netherlands to €2819 in France for those with HbA1c <8%. These savings were driven by reductions in the incidence of complications associated with the AID system compared with MDI with isCGM. The observed cost savings in both HbA1c subgroups highlight the potential benefit of introducing AID systems over MDI, not only for individuals with T1D who have elevated HbA1c, but also for those with lower HbA1c. The differences in long-term complication rates were relatively modest in the HbA1c <8% group and cost savings in this population were primarily attributable to reductions in acute events, particularly the elimination of SHEs requiring hospitalization.
These findings should be interpreted in the context of a BIA, which differs from a cost-effectiveness analysis (CEA) in purpose and scope. Whereas CEAs assess value for money, BIAs focus solely on estimating the financial implications of introducing new treatments. BIAs typically adopt a short-term time horizon and a health care payer perspective, offering practical insights for resource allocation and budget planning.
A treatment-neutral approach was used in this analysis, excluding the costs of glucose monitoring and insulin delivery. As such, the reported cost savings reflect the maximum additional investment that decision-makers could allocate toward improving glycemic control in people with T1D, without increasing overall health care expenditure.
However, there are some limitations to the analysis. First, mortality impacts related to complications were not accounted for as a simplifying assumption. This is particularly relevant for CVD, which has a significant mortality rate. For instance, a UK study on heart failure diagnosis in primary care found an all-cause mortality rate of 9% per year, with survival rates of 53% and 27% at 5 and 10 years, respectively. 29 Significantly impacted survival was also reported in a study examining mortality incidence and the severity of coronary atherosclerosis. The study found survival rates of 92.9%, 89.7%, and 80% for people with 1-, 2-, and 3-vessel obstructive coronary artery disease, respectively. 30 While not specific to people with T1D, such data illustrate the high mortality burden linked to cardiovascular complications. This assumption likely inflated total costs by overestimating the size of the at-risk cohort and the time spent in the follow-up state, thereby overstating the cost differences. However, it also meant that any mortality benefits associated with improved glycemic control were not captured—a conservative omission that may underestimate the full value of treatment.
A key limitation of the current analysis is the exclusion of real-time continuous glucose monitoring (rtCGM) as a comparator. The use of rtCGM is expanding rapidly across Europe and is expected to become more widely used in clinical practice.31–33 By only considering traditional comparators such as MDI or CSII without rtCGM, the model may not fully reflect contemporary treatment pathways or the clinical and economic impact of newer technologies. Future analyses should consider incorporating MDI + rtCGM and CSII + rtCGM as alternative comparators to better align with evolving real-world practice and improve the relevance of findings. Further to this, the model does not incorporate continuous ketone monitoring (CKM), a new technology that could meaningfully reduce the risk of DKA, even among individuals using MDI therapy. 34 Recent studies have shown that CKM is likely to become an integral part of diabetes care, particularly in high-risk populations. 34 However, robust data on CKM’s clinical and economic impact are still being generated, with evidence expected from studies such as the PARTNER study. 35 Accordingly, its inclusion in future models may be necessary to capture the potential clinical and economic benefits accurately.
Another limitation is that the model did not adjust for differences in age distribution, age at diagnosis, or quality of care across countries. Instead, a uniform incidence function was applied, with variation in outcomes driven primarily by treatment-specific HbA1c levels and country-specific unit costs. This reflects the short-term budget impact focus of the analysis and the limited availability of country-level data on age and diagnosis-duration distributions. However, this assumption may underestimate heterogeneity across populations, and future research could explore age- or duration-stratified approaches where robust data are available.
Another potential limitation is that some observational studies suggest a decrease in the risk of complications over time despite no corresponding reduction in HbA1c levels.36,37 This highlights a broader limitation of relying solely on HbA1c to characterize glycemic control. Growing evidence suggests that TIR may be a more sensitive or complementary predictor of complications and could be considered in future model iterations. 38 Related, another limitation is that complication rates were assumed to remain constant over the 5-year horizon. This simplifying assumption reflects the short timeframe typical of BIAs but does not capture potential changes in event rates over time due to aging, diabetes duration, or accumulation of complications.
Finally, a further limitation is the use of a 5-year time horizon. While this is typical of BIAs aligned with payer budget cycles, it may underrepresent the role of chronic, long-term complications. Over longer horizons (10–20 years or lifetime), these complications would be expected to become the main cost drivers. Long-term projections have been explored in cost-utility analyses of the AID systems in people with T1D, which have demonstrated favorable cost-effectiveness outcomes across European settings.19,39
Although there is limited literature on the cost savings of improved glycemic control in most European countries—where studies typically focus only on costs related to the major complications of T1D—several studies have examined this issue specifically in the UK. For instance, one study estimated that a 0.4% improvement in glycemic control for adults with T1D could yield a 5-year cost saving ranging from £184 per person with a baseline HbA1c greater than 75 mmol/mol (9.0%) to £66 per person with a baseline below 59 mmol/mol (7.5%) in the UK. 40 Similarly, another study evaluated the 3-year cost savings associated with a 0.5% reduction in HbA1c achieved using the FreeStyle Libre flash glucose monitoring system for people with T1D. This study estimated cost savings of £196 per person due to reduced health care resource use related to modeled complications. 41 While direct comparisons across studies are challenging due to heterogeneity in study design and person characteristics, these findings broadly align with the cost savings observed in this study for the UK.
Similarly, a study estimated the economic outcomes associated with poor glycemic control in individuals with T1D in The Netherlands. It evaluated the cost savings of improving HbA1c, considering direct costs related to diabetes-related complications and patient management. The study reported per-person cost savings of €568, €1335, and €42,415 over 1, 3, and 7 years, respectively, when achieving a glycemic target of 7.0% compared with remaining at a baseline HbA1c of 9.0%. 42 Again, while comparisons between the present study and this analysis are challenging, the findings broadly align with the cost savings observed for The Netherlands in this study.
As shown in the present study, a substantial reduction in DKA events contributed significantly to the cost savings observed across the modeled countries. This aligns with findings from recent literature which emphasized that DKA remains a significant source of morbidity and mortality in individuals with T1D, and that innovations in diabetes technology, like AID systems, can alleviate this burden. 43
Despite its limitations, the present study highlights the potential for cost savings across nine European countries with the introduction of the AID system compared with MDI with isCGM for both individuals with elevated (HbA1c ≥8%) and lower (HbA1c <8%) HbA1c, using a treatment cost-neutral approach. While existing literature on the cost implications of improving glycemic control is limited across all modeled countries, and robust comparisons between studies are challenging, findings from the UK and The Netherlands align broadly with the present analysis. Moreover, studies highlight that DKA is a significant cause of morbidity and mortality in individuals with T1D, with AID systems alleviating this burden, which is reflected in the present study, as the reduction in DKA plays a key role in the cost savings associated with AID systems.
Conclusions
This study demonstrated that the introduction of the AID system could lead to a reduction in the incidence of T1D complications, compared with conventional standard care, for both individuals with elevated (HbA1c ≥8%) and lower (HbA1c <8%) HbA1c, through improved glycemic control. This improvement translates into potential health care cost savings across nine European countries, which could be reinvested into the AID system for individuals without increasing overall health care expenditure. However, several limitations should be acknowledged, including the exclusion of mortality, the omission of rtCGM as a comparator despite its increasing uptake across Europe, the omission of CKM which may reduce the risk of DKA, the lack of adjustment for country-level age distributions or age at diagnosis, reliance on HbA1c as the sole driver of complication risk without incorporating other glycemic metrics such as TIR, the assumption of constant complication rates over the 5-year horizon, and the use of a short 5-year timeframe which may underrepresent the impact of long-term complications. These limitations may hinder the model’s ability to accurately estimate the incidence of T1D complications and their associated costs, with their effects influencing the estimates in different directions. Accordingly, further research could be beneficial in addressing these limitations. Despite these limitations, the findings offer a useful framework for decision-makers considering additional investments to improve glycemic control in individuals with T1D, which could enhance long-term health outcomes without increasing overall health care expenditure across nine European countries.
Authors’ Contributions
D.F.: Conceptualization (equal) and writing—review and editing (equal). A.Z.O.S.: Conceptualization (equal), methodology (lead), software (lead), formal analysis (lead), investigation (lead), resources (lead), data curation (lead), writing—review and editing (equal), supervision (lead), and project administration (lead). R.F.P.: Methodology (supporting), validation (equal), visualization (equal), writing—original draft (supporting), and writing—review and editing (equal). M.T.: Methodology (supporting), validation (equal), visualization (equal), writing—original draft (lead), and writing—review and editing (equal). M.I.B.: Writing—review and editing (equal). S.d.P.: Writing—review and editing (equal). V.L.: Writing—review and editing (equal). All authors approved the final version of the article.
Footnotes
Author Disclosure Statement
D.F. is an employee of S. Giovanni Addolorata Hospital, Rome, Italy, and has received honoraria for lectures from Novo Nordisk, Abbott, Movi, and Daiichi Sankyo. A.Z.O.S., S.P., and M.I.B. are full-time employees and shareholders of Medtronic International Trading Sarl, Tolochenaz, Switzerland. R.F.P. is a full-time employee, director, and shareholder of Covalence Research Ltd, which received consultancy fees from Medtronic to conduct the analyses and draft the article. M.T. is a full-time employee of Covalence Research Ltd. V.L. has received honoraria in the context of advisory boards, research grants, clinical trials, speakers’ bureaus, and consultancy from Novartis, Sanofi, Novo Nordisk, MSD, Eli Lilly, Boehringer Ingelheim, Vianex, AstraZeneca, Mylan, Amgen, Elpen, Amryt, Medtronic, Menarini, Bios, and Abbott.
Funding Information
The preparation of this article was funded by Medtronic.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.