
Abstract
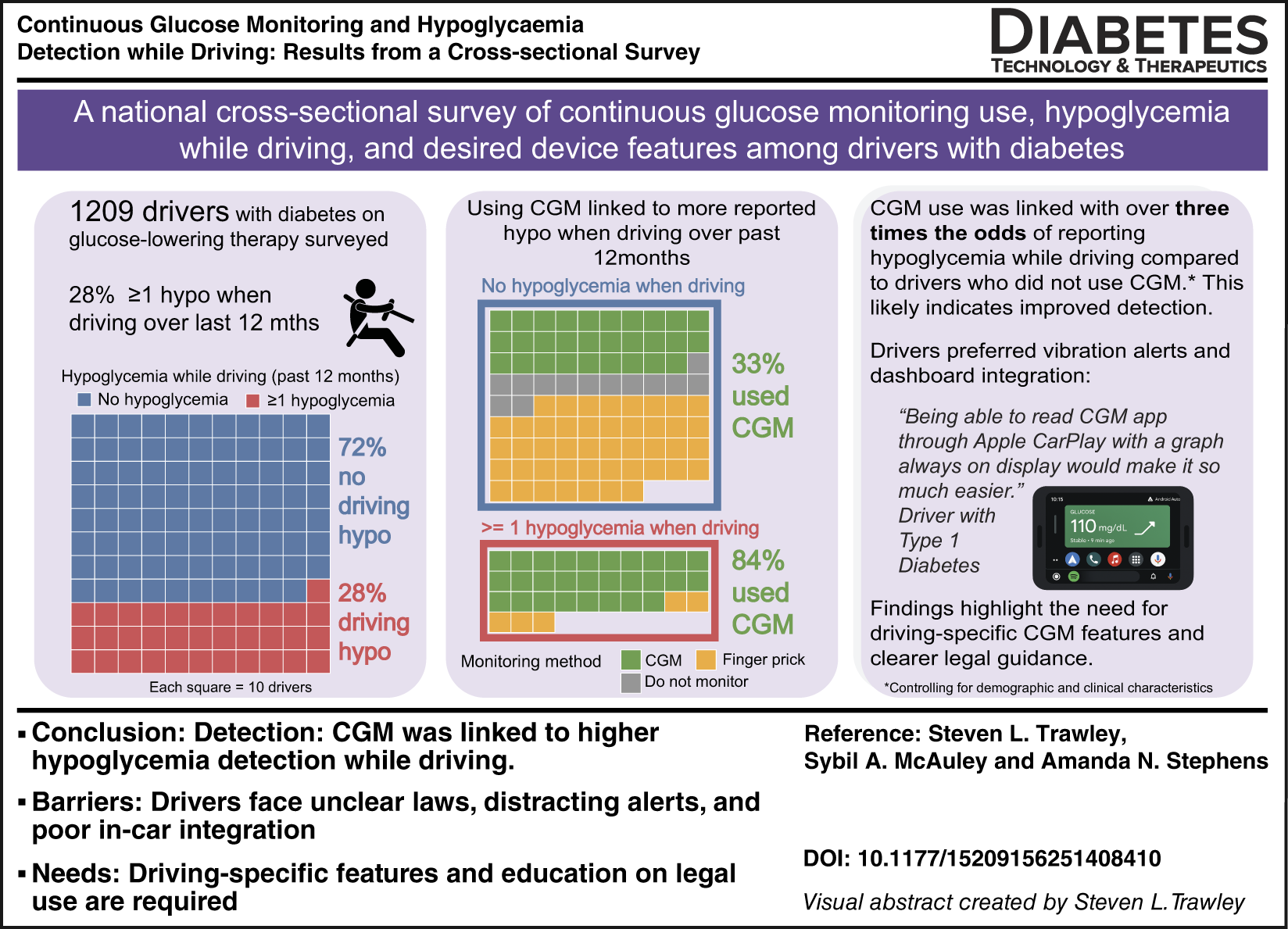
Hypoglycemia is a major safety concern for drivers with diabetes. Continuous glucose monitoring (CGM) improves detection of low glucose levels while driving, yet evidence regarding real-world use remains limited. We conducted a national survey of 1209 Australian drivers with diabetes treated with glucose-lowering medication (mean age 55, standard deviation15 years; 47% using CGM; 39% with type 1 diabetes). Twenty-eight percent of participants reported hypoglycemia while driving in the past 12 months. CGM use was associated with higher odds of reporting hypoglycemia while driving (adjusted odds ratio 3.61 [95% confidence interval: 2.19–5.68]), likely reflecting greater detection. Two-thirds of CGM users relied on CGM vibration or audio alerts, and fewer than one in five adjusted alert thresholds for driving. Difficulty using CGM while driving (50%) and legal uncertainty (43%) were the most frequent barriers. Drivers expressed strong interest in safer in-car CGM integration and clearer legal guidance to support glucose monitoring while driving.
Keywords
Introduction
Driving is an important activity for independence and daily living, 1 requiring sustained attention and coordination. For drivers with diabetes using glucose-lowering medication, hypoglycemia can impair these abilities2,3 and compromise safety. 4 Although crash risk among drivers with diabetes overall is similar to the general population, those with insulin-treated diabetes or impaired hypoglycemia awareness face higher risk and potential license restrictions. 5 International guidelines recommend starting journeys above a minimum glucose level,6–8 yet offer little direction on how to monitor or respond to changes while driving. Continuous glucose monitoring (CGM) can provide real-time alerts to help prevent hypoglycemia, but its role when driving remains unclear. A single experimental study suggests CGM alerts can reduce hypoglycemic driving, though evidence from real-world driving is limited. 9 With increasing CGM uptake 10 and new road rules in Australia permitting mounted medical devices, 11 this national survey examined associations between CGM use and hypoglycemia while driving and drivers’ views on improving device safety and usability.
Methods
A national online cross-sectional survey was administered via the Qualtrics survey platform between June and August 2025. The survey examined the prevalence of self-reported hypoglycemia while driving among Australian adults with diabetes using glucose-lowering medication, as well as perceptions of CGM as a road safety tool and preferences for use. Ethical approval was obtained from The Cairnmillar Institute Human Research Ethics Committee (2025051501). Eligible participants were aged ≥18 years, had any type of diabetes treated with glucose-lowering medication, and held a valid driver’s license. Recruitment occurred nationally via paid social media advertisements (Facebook) and a research panel (Octopus). 12
Before the national launch, a soft pilot phase was conducted with five drivers who met study eligibility criteria. These participants completed the draft online survey and provided feedback on clarity, flow, and completion time. Based on their feedback and subsequent author review, minor revisions were made to improve readability and reduce survey length. Specifically, shorter validated scales were selected (e.g., PAID-5 instead of PAID-20), redundant or overlapping items were removed, and instructions were clarified. The final survey included ∼90 items (depending on responses) and required a median of 14 min (interquartile range (IQR): 10–21) to complete, based on recorded Qualtrics metadata.
Hypoglycemia awareness was assessed using the Gold score and two Clarke items on severe episode frequency and symptom threshold.13,14 Additional items captured history of severe hypoglycemia (“Over the past 12 months, how many times have you experienced a hypoglycemic (low blood glucose) event where you required help from someone else to treat it?”, frequency of hypoglycemia while driving (past 12 months), and diabetes distress (PAID-5). 15 Participants reported their most recent HbA1c, restricted to results obtained within the past 12 months; older or unknown values were coded as missing or “unknown.” Visual or dexterity impairments were coded dichotomously.
Driving exposure was reported across 11 predefined categories (0–5000 km to ≥50,001 km) and recoded into three groups: low (≤10,000 km), average (10,001–15,000 km), and high (>15,000 km), corresponding to national norms. 16 Additional variables included years licensed, crash history, and safety behaviors (checking glucose before driving and carrying fast-acting glucose).
The primary outcome was any self-reported hypoglycemia while driving during the past 12 months. This was defined as any episode that participants personally recognized as a low glucose event when driving, whether identified through symptoms, CGM alerts, or CGM or blood glucose readings. Participants also reported glucose-related near misses, accidents, or whether they ever continued driving despite suspected hypoglycemia. Awareness of CGM driving regulations and perceived barriers to safe in-car use were assessed. CGM users provided details about device use, alert settings, and desired improvements.
We powered the survey to estimate the 12-month prevalence of self-reported hypoglycemia while driving with ±3% precision (95% CI). Because a directly comparable prior 12-month estimate was unavailable, we used a conservative assumption of 50% prevalence, which maximizes the required sample size, providing a target of ∼1000 participants with a 95% CI: ±3%. The final sample (N = 1209) included 338 drivers (28%) reporting hypoglycemia while driving. This corresponds to approximately 21 events per variable (EPV) for the final 16-predictor model, exceeding the commonly recommended threshold of >10 EPV for reliable logistic regression estimates.(12). For context, the Australian National Diabetes Services Scheme reported 491,767 adults (aged >20 years) using insulin between July and September 2025. 17
Descriptive statistics summarized demographics, clinical characteristics, and driving behaviors. Continuous variables are presented as mean ± standard deviation (SD) or median [IQR]; categorical variables as n (%). Statistical comparisons described differences between participants who did and did not report hypoglycemia while driving, using Welch’s t-tests or Wilcoxon rank-sum tests for continuous variables and χ2 or Fisher’s exact tests for categorical variables (Table 1).
Participant Clinical and Driving Characteristics
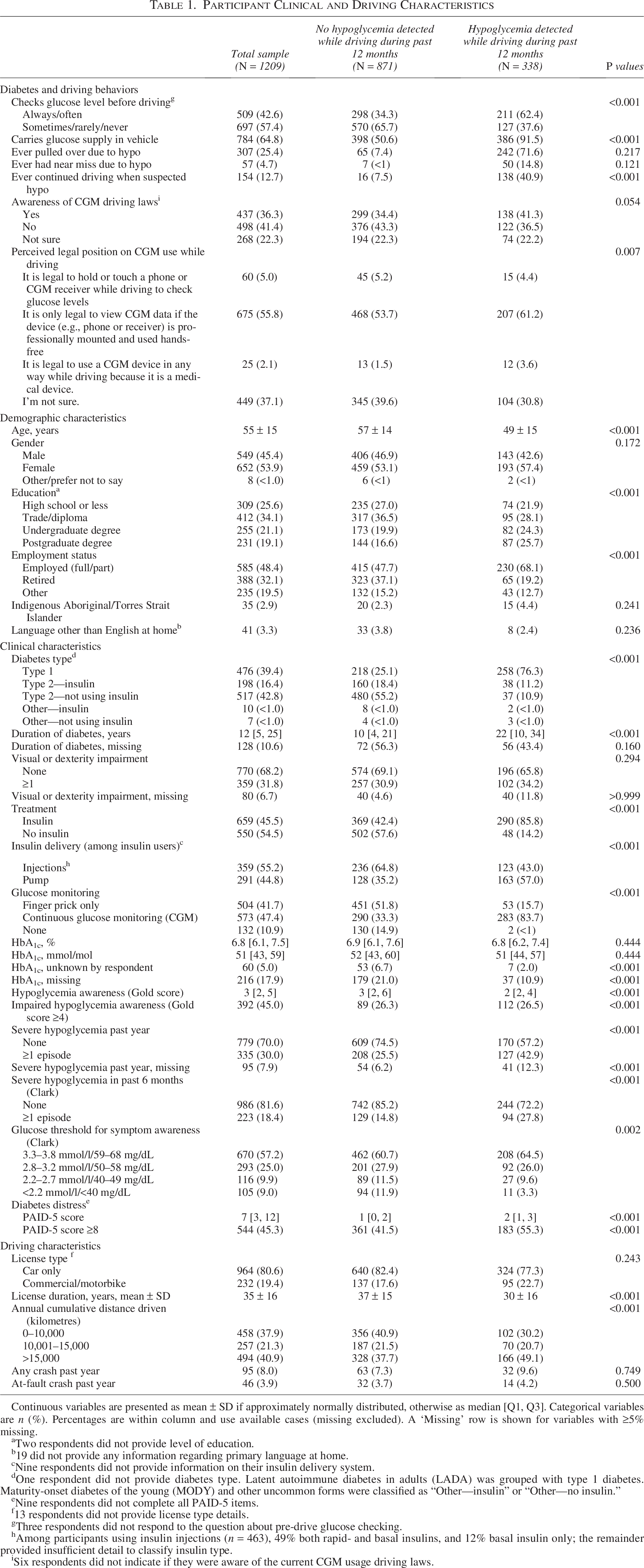
Continuous variables are presented as mean ± SD if approximately normally distributed, otherwise as median [Q1, Q3]. Categorical variables are n (%). Percentages are within column and use available cases (missing excluded). A ‘Missing’ row is shown for variables with ≥5% missing.
Two respondents did not provide level of education.
19 did not provide any information regarding primary language at home.
Nine respondents did not provide information on their insulin delivery system.
One respondent did not provide diabetes type. Latent autoimmune diabetes in adults (LADA) was grouped with type 1 diabetes. Maturity-onset diabetes of the young (MODY) and other uncommon forms were classified as “Other—insulin” or “Other—no insulin.”
Nine respondents did not complete all PAID-5 items.
13 respondents did not provide license type details.
Three respondents did not respond to the question about pre-drive glucose checking.
Among participants using insulin injections (n = 463), 49% both rapid- and basal insulins, and 12% basal insulin only; the remainder provided insufficient detail to classify insulin type.
Six respondents did not indicate if they were aware of the current CGM usage driving laws.
Missing data were modest (HbA1c 18%, diabetes duration 11%; others <5%). Multiple imputation by chained equations (20 imputations, 20 iterations) was used under a missing-at-random assumption. Logistic regression examined associations between CGM use and driving hypoglycemia. Model 1 included CGM use only; Model 2 (fully adjusted) added diabetes type (including insulin status), diabetes duration, HbA1c, impaired awareness, age, gender, impairments, safety behaviors, and driving exposure. A secondary sensitivity analysis included additional covariates that were significant in univariate comparisons. Results are reported as adjusted odds ratios (aORs) with 95% confidence intervals (CI). Model assumptions (linearity, collinearity, calibration, and discrimination) were satisfactory. Analyses were performed in R (v4.5.1). Open-text responses from CGM users underwent content analysis to identify recurring themes.
Results
From 11 June to August 1, 2025, 1209 eligible participants completed the survey (700 via research panel, 509 via social media). Based on Octopus Research Panel data, there were 646 potentially eligible contacts available, while Meta advertisements generated 9935 link clicks (click-through rate 7.9%). Across both recruitment streams, approximately 10,600 individuals were reached, and 1209 participants completed the survey, representing an overall response rate of ∼11%. Participants’ mean age was 55 ± 15 years; 54% were women, and 97% were nonindigenous Australians (Table 1). Median diabetes duration was 12 years [IQR: 5–25]. The sample included 39% with type 1 diabetes, 59% with type 2 diabetes, and 1% with other diabetes types, which is broadly consistent with national registry data. 17 Among those with type 2 diabetes, 198 (28%) reported using insulin, similarly consistent with national registry data. A total of 131 participants (18%) used CGM. The relatively low uptake among those with type 2 diabetes likely reflects the absence of subsidy for this group in Australia, where CGM must be self-funded. Overall, 47% used CGM. Median Gold score was 3 [IQR 2–5]; 45% met criteria for impaired awareness of hypoglycemia (Gold score ≥4); and 30% reported severe hypoglycemia in the past year.
During the previous 12 months, 28% (n = 338) reported at least one occurrence of hypoglycemia; 23% (n = 278) reported 1–3 hypoglycemic episodes, and 5.0% (n = 60) reported ≥4 episodes (Table 1). Compared with respondents reporting no hypoglycemia during driving in the past 12 months, these drivers were younger, more often had type 1 diabetes (70% vs 23%), and were more likely to be treated with insulin (86% vs 42%); more of the insulin users were on pump therapy (57% vs 35%) (all P < 0.001). One in four drivers (25%, n = 307) reported ever pulling over due to low glucose, and 4.7% (n = 57) reported a driving near miss or accident relating to glucose levels. Drivers who reported hypoglycemia while driving during the past 12 months were substantially more likely to have ever pulled over due to low glucose (72% vs. 7.4%), to report a near miss attributed to hypoglycemia ever (15% vs. <1%), and to acknowledge continuing to drive despite suspecting they were hypoglycemic (41% vs. 7.5%). Impaired awareness of hypoglycemia was also more prevalent among these drivers (P < 0.001).
Drivers who reported hypoglycemia while driving in the past 12 months were more likely to use CGM (65% vs 23%), check glucose before driving (62% vs 34%), and carry glucose supplies (92% vs 51%). Awareness of CGM driving laws was low, with only 36% indicating they knew the current national law. When presented with options, 56% correctly identified that CGM data may only be viewed if professionally mounted and hands-free, while 37% remained uncertain.
Among CGM users who indicated that they use their devices when driving (n = 494; Supplementary Table S1), most relied on audio or vibration alerts while driving (67%), with smaller proportions using smartwatches (27%) or mounted smartphones (23%). Only 15% (72/494) adjusted low-glucose alerts for driving. Among those who provided a value (55/72), the median threshold was 5.0 mmol/L (IQR 4.4–5.5; range 3.6–8.0), with over half (53%) setting alerts at 5.0 mmol/L and most (∼85%) between 4.0 and 6.0 mmol/L. Among respondents who used the same alert threshold all the time, over 60% provided a valve (209/341); the median threshold was 4.0 mmol/L (IQR 3.8–4.5), with most values between 3.5 and 4.5 mmol/L. Most perceived CGM as beneficial for road safety (84%) and glucose management (85%), yet many reported uncertainties about its legal status when driving (43%), difficulty viewing displays (27%), and distraction concerns (20%). When combined into a composite measure, half of CGM users (50%) indicated difficulty using CGM while driving. Desired features included a driving-specific CGM app (55%), in-car dashboard integration (51%), and tailored audible alerts (49%).
Content analysis of open-text responses identified three themes (Fig. 1). In-car integration was the most common request, with drivers calling for Android Auto or Apple CarPlay access to display CGM data when driving. Usability and alerts were also emphasized, with frustration over repetitive, hard-to-silence alerts and suggestions for voice-based options. Under the legal and safety theme, many expressed confusion about what was permitted, especially when checking devices at traffic lights or using smartwatches, which are prohibited under Australian road rules. 11
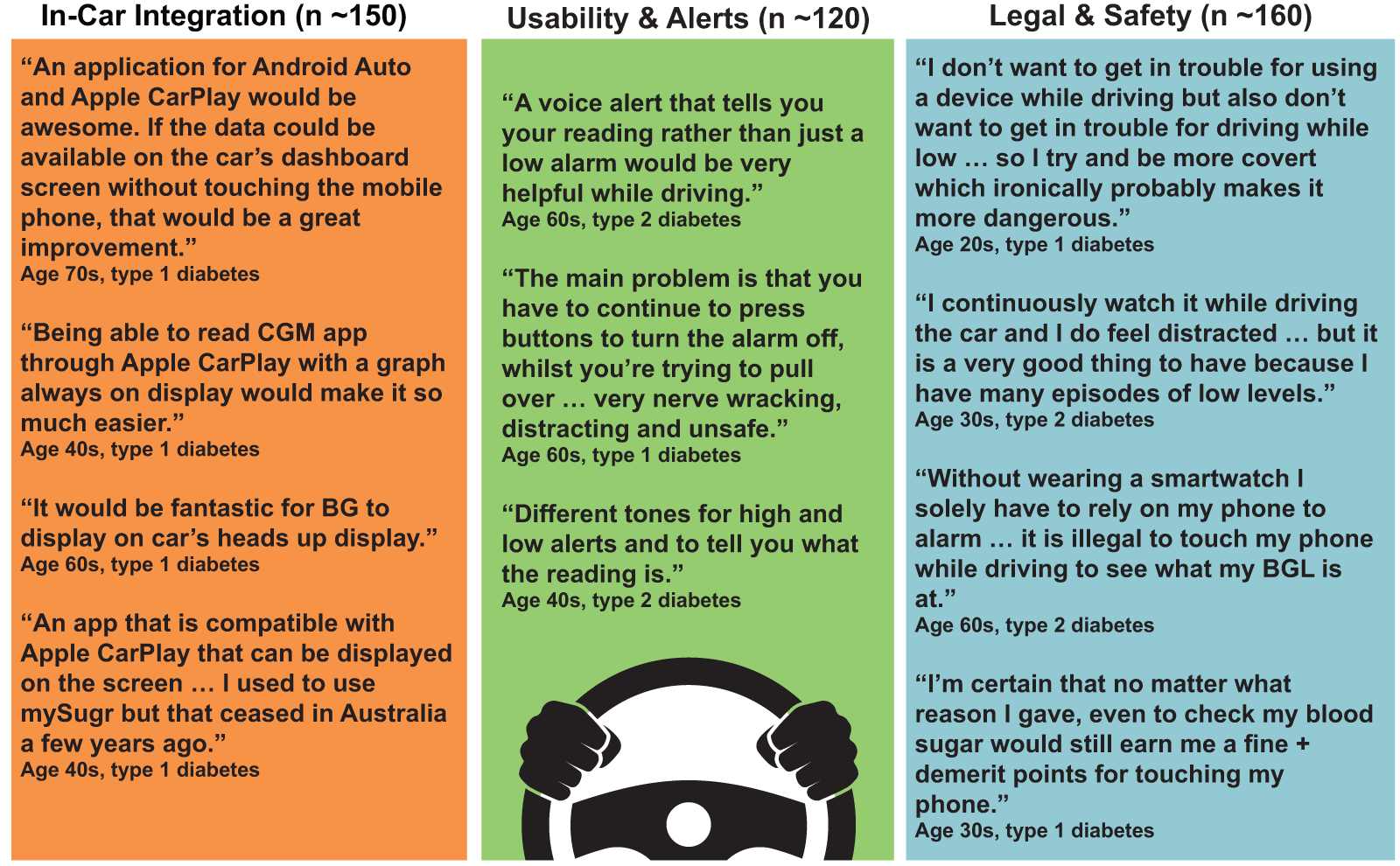
Themes and illustrative quotes from open-text responses on CGM use while driving Quotes illustrate typical experiences, challenges, and future wants described by participants. Ages are presented in 10-year bands to protect confidentiality. Adjustments were applied only for presentation and did not affect the analyses. CGM, continuous glucose monitoring.
In the minimally adjusted model, CGM use was strongly associated with reporting hypoglycemia while driving (OR: 10.31, 95% CI: 7.47–14.22). After full adjustment for demographic, clinical, behavioral, and driving factors, the association remained significant (aOR: 3.61 [2.29–5.68]). Drivers with type 1 diabetes were more than four times as likely to report hypoglycemia while driving compared with those with non-insulin-treated type 2 diabetes (aOR: 4.33, 95% CI: 2.53–7.44). Adults with type 2 diabetes who used insulin also had higher odds of reporting hypoglycemia while driving compared with those not using insulin (aOR: 2.13; 95% CI: 1.22–3.70). Younger age, insulin use, longer diabetes duration, and a history of severe hypoglycemia were additional independent predictors, while regular pre-drive glucose checking was associated with lower odds of hypoglycemia during driving (aOR: 0.67, 95% CI: 0.46–0.98). Participants who did not know their HbA1c were also less likely to report hypoglycemia (aOR: 0.21, 95% CI: 0.06–0.67). Full results are presented in Supplementary Table S2. A secondary sensitivity analysis that additionally adjusted for education, employment status, diabetes distress, and awareness of CGM driving laws is not reported here; results were materially unchanged.
Given the association between CGM use and self-reported hypoglycemia while driving, we conducted an exploratory analysis limited to participants who reported using CGM when driving to determine whether their self-reported low-glucose alert threshold was related to hypoglycemia occurrence. Across these participants, alert thresholds ranged from 3.6 to 8.0 mmol/L (median 5.0 mmol/L, IQR: 4.4–5.5), but there was no significant association between alert level and reported hypoglycemia while driving (W = 8571, P = 0.96; see Supplementary Fig. S1).
Discussion
This national survey highlights key roles of CGM use by drivers with diabetes, as well as areas for CGM advancement to enhance driving-related usability. CGM users were more likely to report hypoglycemia while driving than nonusers, likely reflecting greater detection rather than higher risk. Even after adjusting for factors such as age, insulin use, recent severe hypoglycemia, and impaired awareness, CGM use remained strongly associated with reported events, suggesting that drivers without CGM may be less aware of hypoglycemia and potentially at greater risk. Drivers who reported hypoglycemia while driving were also more likely to have pulled over, indicating that detection often prompted corrective action rather than being ignored. While a small minority continued driving despite symptoms, this pattern supports CGM’s potential safety value in prompting timely behavioral responses.
As expected, insulin use, longer diabetes duration, and a history of severe hypoglycemia predicted greater risk of driving hypoglycemia, consistent with previous evidence. 4 Drivers with type 1 diabetes were more likely to report hypoglycemia while driving than those with non-insulin-treated type 2 diabetes, likely reflecting greater symptom awareness and more intensive day-to-day self-management. Drivers with insulin-treated type 2 diabetes also had elevated odds of reporting hypoglycemia while driving, consistent with the increased risk associated with exogenous insulin use. Gender, HbA1c, and impaired awareness scores were not associated. Interestingly, participants who did not know their HbA1c were less likely to report hypoglycemia, perhaps reflecting lower engagement with diabetes self-management. 18 Regular pre-drive glucose checking was associated with lower odds of reporting hypoglycemia while driving, highlighting its protective value in real-world settings.6,7 However, this association was not consistently significant across all models that were tested, indicating that while pre-drive testing may reduce the risk of hypoglycemia onset, it does not necessarily influence whether drivers become aware of glucose changes once the journey has started.
These findings complement recent experimental data showing that preset CGM alerts while driving can prevent hypoglycemia. 9 In contrast, our real-world data show higher reported hypoglycemia among CGM users. Together, these results suggest that CGM supports safer driving when alerts are optimized and acted upon. Importantly, less than a quarter of our sample reported adjusting their alert thresholds specifically for driving, unlike the Maeda protocol where alerts were preset at 4.4 mmol/L (80 mg/dL). A “driving mode” with earlier, voice-first alerts (e.g., at 5.0 mmol/L/90 mg/dL, as recommended in the UK and Australia and evidenced by naturalistic driving studies)6,7 could help bridge the gap between controlled trial efficacy and real-world effectiveness.
Most CGM users relied on vibration or sound alerts rather than viewing displays, an adaptation to avoid distraction but one that limits access to detailed glucose information. Drivers expressed uncertainty about the legality of interacting with phones or smartwatches for CGM while driving and described anxiety about enforcement. This absence of guidance complements recent evidence from the United States that the majority of people with diabetes report never having received structured education on driving and diabetes management, highlighting an important gap in both clinical and road safety practice. 19
Open-text responses showed that drivers viewed CGM as valuable trip information but felt current devices lack safety, usability, and legal clarity. Consistent with quantitative survey findings, over two-thirds were unaware of current driving laws, and even after being shown the correct rule, one-third remained uncertain. These findings suggest widespread confusion about how drivers can legally use CGM devices while driving.
Drivers consistently called for optimized in-car access to glucose data via CarPlay, Android Auto, heads-up displays, and/or voice prompts—concepts proposed as early as 2008 yet still unrealized. 20 Only one research group has tested in-vehicle hypoglycemia alerts, finding multimodal alerts most effective. 21 Our qualitative data mirror this, with drivers preferring clearer, voice-based feedback and easier alert management. Future research should guide next-generation CGM design to include safe, nonvisual, context-specific alerts and explore how drivers use CGM to avoid hyperglycemia, which can also impair cognitive performance.22,23
Strengths include the large national sample and detailed data on driver behavior, device use, and preferences. Australia’s subsidized CGM program and legislation changes provided an ideal context to examine driver CGM use. Limitations include the self-reported, cross-sectional design and possible selection bias toward technology-engaged participants, with modest overrepresentation of type 1 diabetes, which may limit generalizability. There is also likely selection bias toward individuals motivated or confident enough to complete an online questionnaire, potentially under-representing those with lower digital literacy. Another limitation is that the survey did not ask how participants identified a hypoglycemia episode (e.g., based on symptoms, CGM alerts, or blood glucose readings) or how they typically checked glucose before driving (fingerprick vs. CGM). These items were designed to capture participants’ usual real-world practices, but the lack of definition may have introduced variability in interpretation. In addition, insulin type could not be systematically classified among injection users, as insulin preparation names were entered in a free-text field, limiting the precision of treatment subgroup comparisons.
Conclusions
CGM use was associated with greater reporting of hypoglycemia while driving among adults treated with glucose-lowering medication. This likely reflects improved detection rather than increased risk. Future research should move beyond surveys to capture objective data on how drivers respond to CGM alerts in real driving situations. Such work will be key to informing device design and road safety policy. Incorporating behavioral or sensor-based measures of alertness and responsiveness may further clarify how hypoglycemia affects driving performance and guide the development of safer, more adaptive diabetes technologies and road safety policies.
Authors’ Contributions
S.L.T. developed the original idea and conceptualized the study with S.A.M. and A.N.S. S.L.T. completed the literature review and curated the data. S.L.T. conducted the statistical analyses and wrote the first draft of the article, with input from S.A.M. and A.N.S. All authors critically reviewed the article and approved the final version for submission. S.L.T. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Acknowledgments
The authors thank all participants for generously giving their time to complete this survey.
Author Disclosure Statement
The authors have no conflicts of interest to declare related to this study.
Funding Information
This work was supported by the National Road Safety Action Grants Program (NRSAGP), an initiative of the Australian Government Department of Infrastructure, Transport, Regional Development, Communications and the Arts (NRSAGP-TI1-A85). Dexcom has provided in-kind support for aspects of the broader project, but no financial or material support was provided for this phase of the study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.