
Abstract
Introduction:
Automated insulin delivery (AID) systems have improved treatment for people with type 1 diabetes (T1D). Treatment with AID may also improve sleep. However, there is a need to examine this further.
Objective:
To systematically collect and synthesize data from available studies that have assessed subjective and objective sleep parameters in people with T1D transitioning to AID systems.
Methods:
Searches were performed in multiple databases, and the systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Meta-analyses were performed for randomized clinical trials (RCTs) and prospective studies when feasible; incompatible studies were reviewed narratively. Data from adults, children, and caregivers of children were analyzed separately.
Results:
A total of 27 studies met eligibility criteria. Sufficient data for meta-analysis were available only for subjective sleep quality measured by the Pittsburgh Sleep Quality Index (PSQI). Among adult AID users, no significant change in PSQI scores was observed in RCTs, while prospective studies found a minor improvement with AID systems (study n = 7, mean −0.42 points, 95% confidence interval [CI]: −0.81, −0.04, p = 0.03). For caregivers of children with T1D, analyses of both RCTs and prospective studies found improved sleep quality with AID systems (RCTs: n = 2, mean −1.79 points, 95%CI: −2.96, −0.61, p = 0.003 | Prospective studies: n = 4, mean −1.24 points, 95%CI: −2.02, −0.46, p = 0.002). Data on children with T1D were not sufficiently available for meta-analysis. Studies varied considerably in terms of comparator treatments and populations of interest. Most studies were based on secondary or ad hoc analyses.
Conclusion:
AID systems may improve perceived sleep quality in caregivers of children with T1D. The effect on adults with T1D is inconclusive, although prospective studies suggest a benefit. Studies reporting objective sleep measures and data regarding children with T1D are limited. Further research in these areas is needed.
Introduction
Automated insulin delivery (AID) systems have substantially reduced the treatment burden and improved glycemic outcomes across all age groups in individuals with type 1 diabetes (T1D). Beyond glycemic control, AID systems have been shown to alleviate diabetes distress in adults and in caregivers of children with T1D. 1 Broader psychosocial and quality of life outcomes are also being explored. However, this field remains in its early stages of development. Sleep plays a vital role in physical and mental health. People with T1D often experience shorter sleep duration and poorer sleep quality compared with individuals without diabetes, which in turn may negatively influence glycemic control. 2 Observational studies and large-scale surveys have reported improved sleep quality among AID users compared with those using other treatment modalities.3,4 These may be due to reduced glycemic variability and fewer nocturnal hypoglycemic episodes.5,6 While being an important factor, sleep is a complex outcome to assess. Objective measures such as sleep architecture, duration, and efficiency can be obtained through various methods, whereas subjective sleep measures are acquired through structured questionnaires, each with inherent strengths and limitations. 7 Polysomnography (PSG) remains the gold standard for accurately assessing sleep duration and architecture. 8 Alternatively, actigraphs—accelerometers combined with a real-time clock—provide similar objective estimates of sleep. 9 Both methods yield several quantitative measures; PSG offers the most precise measurements, whereas actigraphy benefits from being easier to perform at home for extended durations.
Subjective sleep quality is commonly assessed with validated questionnaires such as the Pittsburgh Sleep Quality Index (PSQI). 10 The PSQI captures many of the above parameters based on self-reported sleep habits during the past month and reports seven subscores, covering a range of subjective sleep metrics. A total composite score is then calculated, which is most commonly reported.
Given the potential impact of AID systems on sleep and per extension on health and quality of life, and the lack of cohesive information in this developing field, a systematic synthesis of the evidence is warranted. This systematic review aims to comprehensively assess the current literature on the effects of AID systems on sleep outcomes in people with T1D and their caregivers.
Methods
Literature search and study selection
The review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, 11 and the study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO). 11 We systematically searched MEDLINE, Embase, CENTRAL, and CINAHL for all studies examining sleep measures in people with T1D transitioning to AID systems from inception to January 3, 2024. An updated search was performed in all databases on June 30, 2025.
The search string combined medical subject heading terms (e.g., MeSH) with free-text words describing each concept. No restrictions on study types were applied at the search stage. An information specialist (THA) developed and evaluated the search strategy by testing if key articles were retrieved. We provide the full search strategy in Supplementary Table S1.
Records were imported and managed using the EPPI-Reviewer 6 software. 12 This system automatically detected duplicates for manual verification and exclusion. It was also used for abstract and full-text screening. For abstracts or registered study protocols, we conducted manual searches to identify published results. Following the screening of studies, the SpiderCite tool from The Evidence Review Accelerator (TERA) software 13 was used to retrieve cited and citing references of the included studies on August 27, 2025.
Two investigators independently performed study selection, data extraction, and quality assessments. Disagreements were resolved through reconciliation meetings, involving a third party if needed for reaching consensus. We implemented a broad search and conservative abstract screening to prevent the erroneous exclusion of studies, as we expected sleep parameters would often not be highlighted in abstracts.
Criteria for study selection
Eligible studies had to include individuals with T1D transitioning to an AID system from their usual treatment, and study populations including people with type 2 diabetes were excluded. All types of AID systems—including open-source systems—were eligible. Comparators included multiple daily injections (MDIs), sensor-augmented pump (SAP) systems, and standalone insulin pumps. Studies had to involve at least 10 participants, and AID systems had to be used in an at-home setting for at least 1 month before follow-up. Finally, randomized clinical trials (RCTs), prospective interventional or observational studies, or cross-sectional studies were all eligible, and no language restrictions were applied, but studies were required to be peer-reviewed.
Data extraction, quality assessment, and synthesis
For all studies, we extracted the following information: year of publication, study name, authors and country of origin, interventions (i.e., brand name of the AID systems), comparators, sample characteristics (age, gender distribution, and diabetes duration), sample sizes, and outcome measures. When required, additional data were requested from the corresponding authors.
Quality assessments were conducted using the Joanna Briggs Institute (JBI) Critical Appraisal Tools for prospective studies, RCTs, and cross-sectional studies.14–16 There were no strict criteria for the final quality gradings, but the following guiding criteria were used: For studies to be considered of high quality, it would need to have no issues or only minor issues in up to two domains from their respective JBI tool. Studies were considered of medium quality if there were moderate issues in one domain or minor issues in more than two domains and were considered low quality if there were severe issues in one or more domains and/or moderate issues in several domains. Gradings were decided through reconciliation meetings between the two primary investigators, with the possible inclusion of a third party. Prospective studies were further characterized using the checklist published by Reeves et al.—and recommended by the Cochrane handbook—to ensure a homogeneous approach to data acquisition for meta-analysis.17,18
We performed meta-analyses of RCTs that reported either primary or secondary endpoints, complemented by meta-analyses from prospective studies.
Three groups were analyzed separately: adults (≥18 years) with T1D; children and adolescents (<18 years) with T1D; and caregivers of children and/or adolescents with T1D.
We did this to ensure comparable sleep patterns for analyses. Studies not fit for meta-analyses were synthesized narratively.
Outcomes of interest
Both subjective and objective measurements were included in this review. This included data from PSG, actigraphy, PSQI, and other structured questionnaires.
General metrics of interest included total sleep time, sleep latency (time from going to bed to falling asleep), wake after sleep onset (WASO) time, and sleep efficiency (percentage of time in bed spent sleeping). These metrics are measured by both actigraphy and PSG and to some degree by PSQI.
Additionally, sleep architecture data (time in deep, light, and REM sleep) were included when available.
PSQI specific metrics included subscores (0–3, with higher scores showing greater detriments) and total scores (0–21).
For other structured questionnaires, data of relevance were evaluated on individual basis.
Sleep efficiency was chosen as the primary outcome measure as it is consistently defined across methods, directly clinically relevant, and is highly affected by fragmented sleep, as we would expect from the populations of interest.
Outcomes were analyzed as between-group differences at follow-up when comparator groups were available or as the change from baseline to follow-up in prospective studies.
Statistics
Extracted data from studies considered eligible for meta-analysis were analyzed in R (version 4.5.0) using the package “meta.”19,20 The data were modeled with the random effects model. Data not presented as mean and standard deviation, including median and interquartile range or mean and standard error of the mean, were transformed to mean and standard deviation for the purpose of analysis. The inverse variance-weighted method was used to estimate the mean differences with the corresponding 95% confidence intervals (CIs). P values <0.05 for the pooled effect sizes were considered statistically significant.
Heterogeneity between studies was assessed using the I2 statistic and the Cochran’s Q test. Publication bias was evaluated visually with a funnel plot and formally using Egger’s regression test with the “dmetar” package. 21 The test is based on study effect sizes and standard errors derived from calculated CI values, with P < 0.05 indicating a statistically significant risk of small-study bias.
Results
Literature search
The database search identified 555 articles. After excluding duplicates, 388 articles remained for abstract screening. Through the selection process—outlined in Figure 1—we identified 25 studies that met the inclusion criteria.22–45
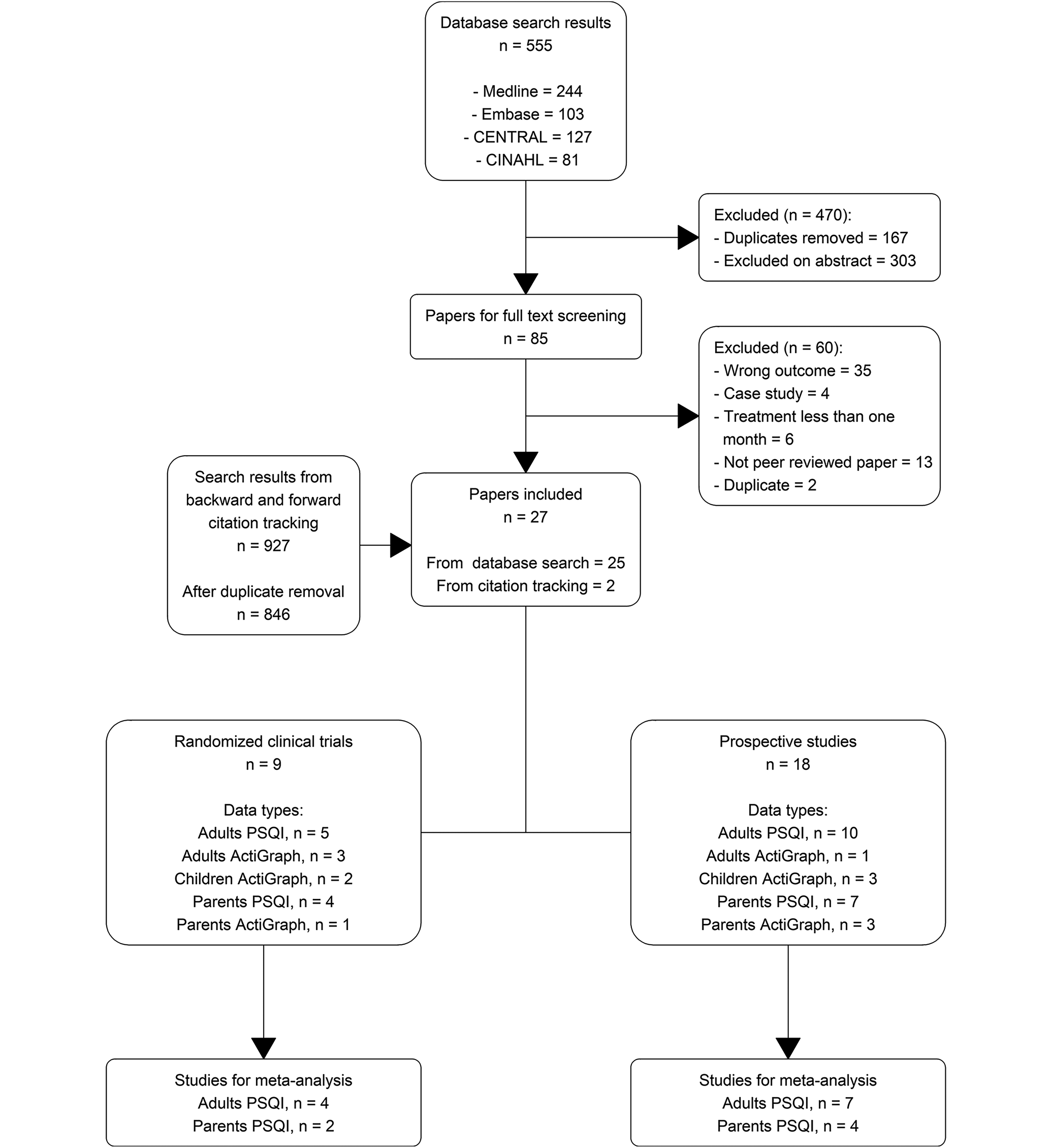
Flowchart showing process of study selection.
The additional citation and reference search yielded 927 records. After removing duplicates, 846 records remained. Two additional articles meeting the inclusion criteria were found through abstract and full-text screening of these records.46,47 These two studies did not include any of our keywords in abstracts, therefore not appearing in the primary search. Including these brought the final count to 27 studies. Of these, 9 were RCTs and 18 were prospective studies.
PSQI data were collected in 5 RCTs and 10 prospective studies involving adults, as well as in 4 RCTs and 7 prospective studies for caregivers of children using AID. For adults, actigraphy data were collected in three RCTs and one prospective study; for children, in two RCTs and three prospective studies; and for caregivers, in one RCT and three prospective studies. We identified no studies assessing sleep using PSG.
All acquired data are listed in Tables 1, 2, and 3, while Supplementary Tables S2 and S3 provide an overview of quality assessments for included studies and reasons for exclusion.
Characteristics of Studies Examining Adult Populations
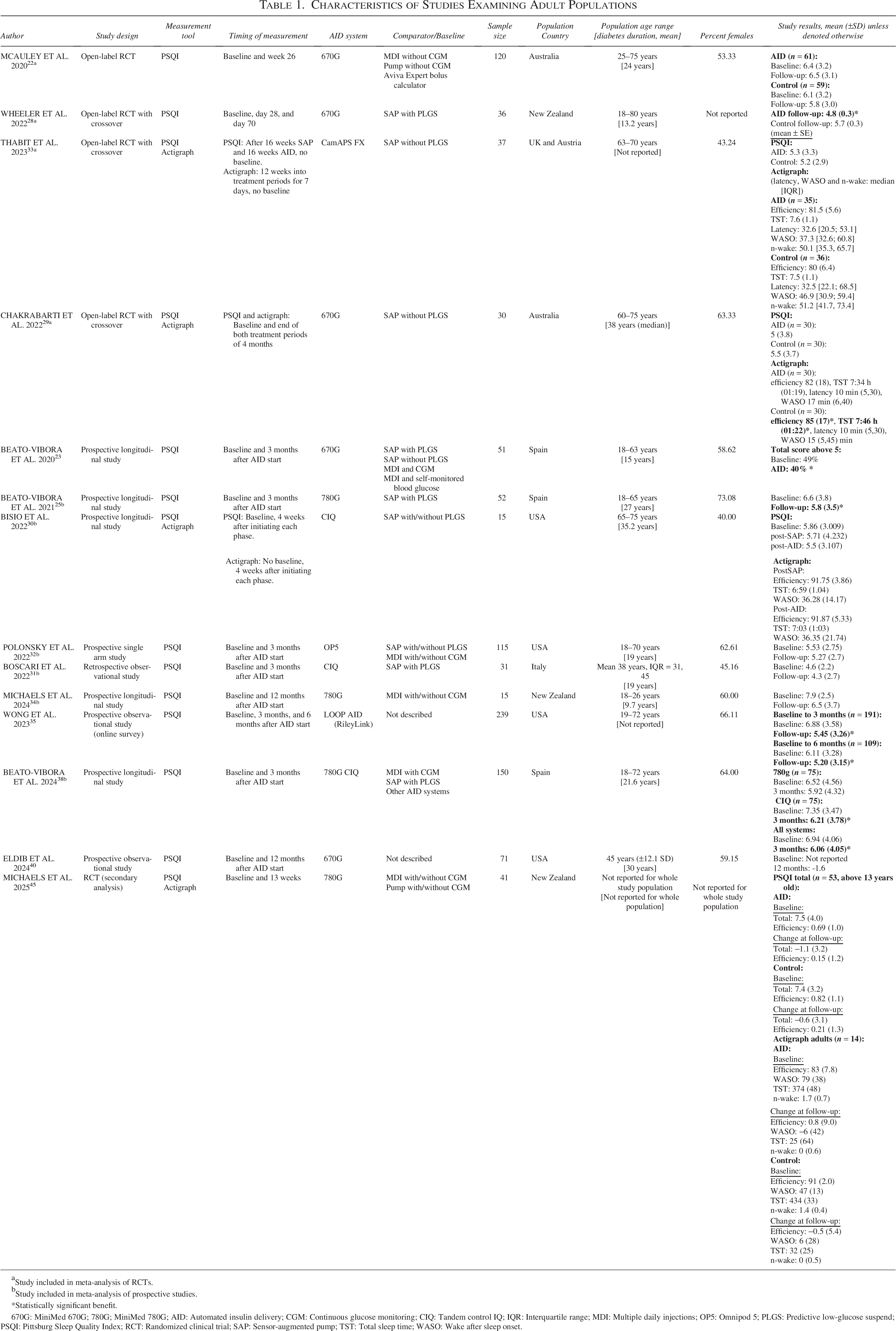
Study included in meta-analysis of RCTs.
Study included in meta-analysis of prospective studies.
*Statistically significant benefit.
670G: MiniMed 670G; 780G; MiniMed 780G; AID: Automated insulin delivery; CGM: Continuous glucose monitoring; CIQ: Tandem control IQ; IQR: Interquartile range; MDI: Multiple daily injections; OP5: Omnipod 5; PLGS: Predictive low-glucose suspend; PSQI: Pittsburg Sleep Quality Index; RCT: Randomized clinical trial; SAP: Sensor-augmented pump; TST: Total sleep time; WASO: Wake after sleep onset.
Characteristics of Studies Examining Caregivers of Children Transitioning to AID Treatments
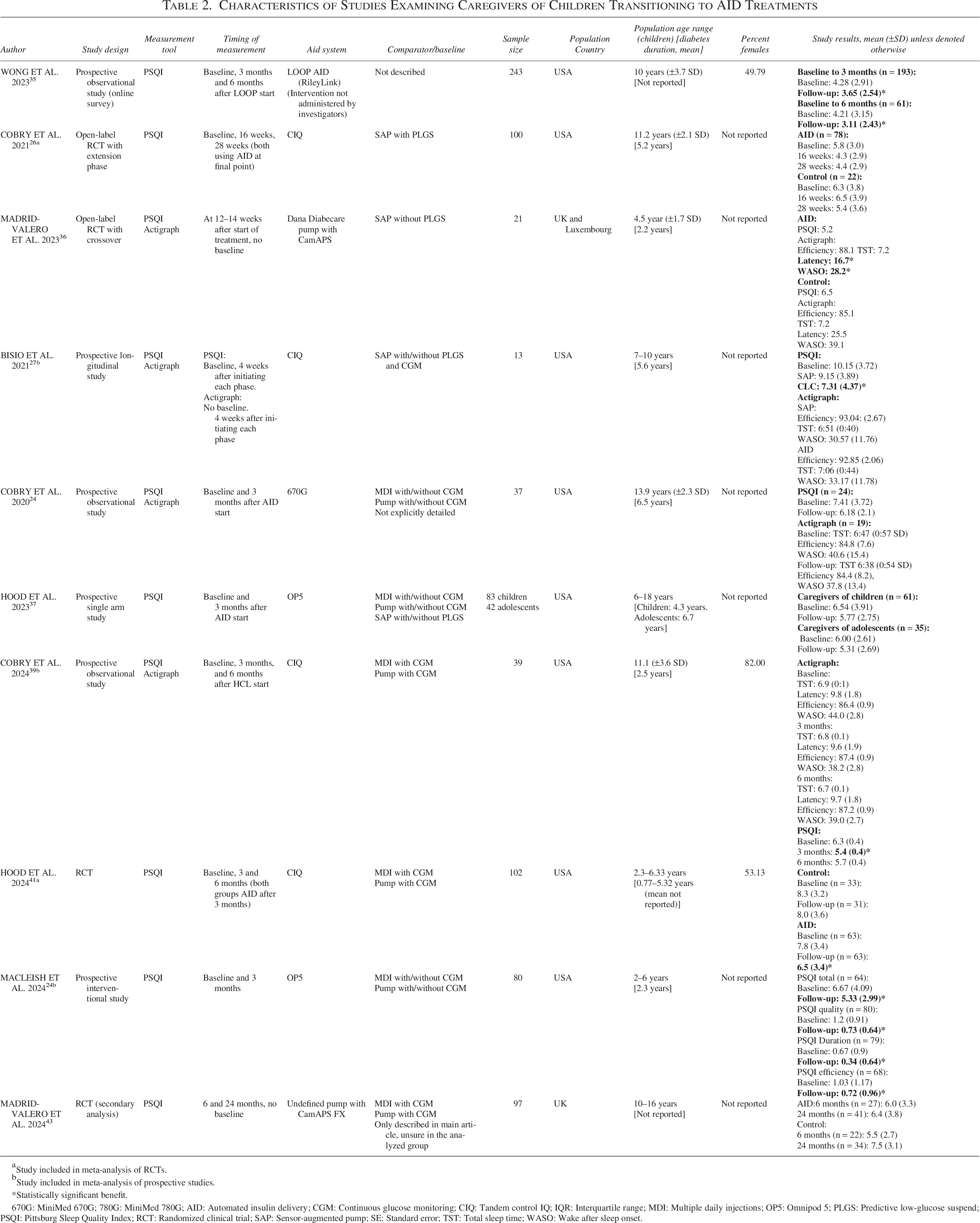
Study included in meta-analysis of RCTs.
Study included in meta-analysis of prospective studies.
*Statistically significant benefit.
670G: MiniMed 670G; 780G: MiniMed 780G; AID: Automated insulin delivery; CGM: Continuous glucose monitoring; CIQ: Tandem control IQ; IQR: Interquartile range; MDI: Multiple daily injections; OP5: Omnipod 5; PLGS: Predictive low-glucose suspend; PSQI: Pittsburg Sleep Quality Index; RCT: Randomized clinical trial; SAP: Sensor-augmented pump; SE: Standard error; TST: Total sleep time; WASO: Wake after sleep onset.
Characteristics of Studies Examining Children Transitioning to AID Treatments

670G: MiniMed 670G; 780G: MiniMed 780G; AID: Automated insulin delivery; CGM: Continuous glucose monitoring; CIQ: Tandem control IQ; IQR: Interquartile range; MDI: Multiple daily injections; OP5: Omnipod 5; PLGS: Predictive low-glucose suspend; PROMIS: Patient-Reported Outcomes Measurement Information System; PSQI: Pittsburg Sleep Quality Index; RCT: Randomized clinical trial; SAP: Sensor-augmented pump; TST: Total sleep time; WASO: Wake after sleep onset.
Meta-analyses
Two meta-analyses were conducted summarizing total PSQI scores from RCTs in adults and in caregivers, respectively. To supplement these results, two additional meta-analyses of prospective studies were performed using the same outcome for each of the two groups. Results are summarized in detail in Figures 2 and 3.
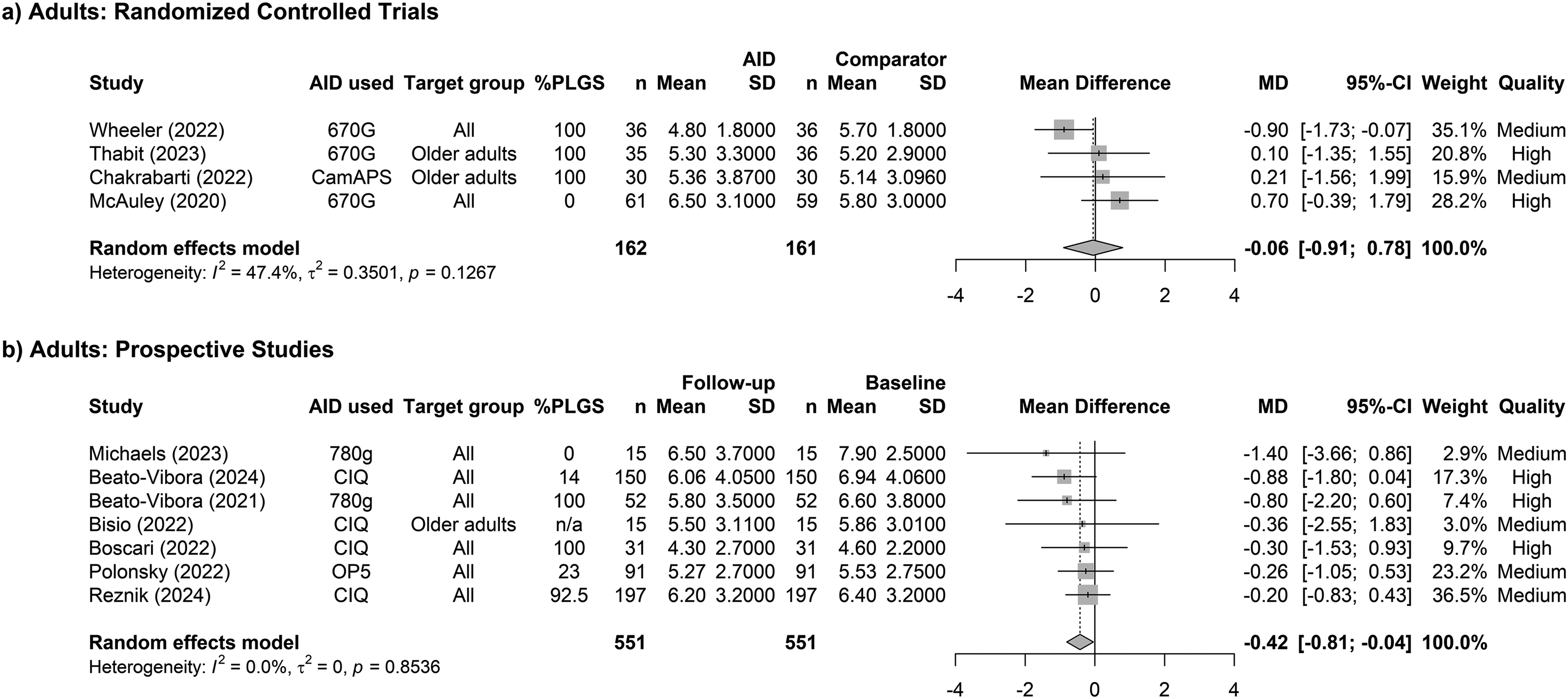
Results of the meta-analysis of studies involving adults with T1D.
Total PSQI scores were used as only two studies reported subscores.42,45 For all remaining studies, an attempt was made at acquiring subscores, although we were unsuccessful.
Although some studies reported quantitative sleep parameters from actigraphy, insufficient data were available for meta-analyses in any subgroups, and these data were, therefore, synthesized narratively.
Sleep quality in adults using AID
RCTs
For the meta-analysis of RCTs on adults, 4 studies—with a total of 222 participants—were included.22,28,29,33 The pooled effect on total PSQI scores was −0.06 points (95%CI: −0.91, 0.78, p = 0.88, Fig. 2a), providing no evidence that AID improved sleep quality in adults. Between studies, average differences ranged from −0.9 to +0.7. The inferred importance of each study was moderately asymmetrical, with the largest weight assigned to the study by Wheeler, 28 which reported improvement in sleep quality for AID users, whereas the study by McAuley 22 reported the opposite effect. Between-study heterogeneity was moderate, with an I2 value of 47.4%. The associated funnel plot showed an atypical pattern, with the two largest studies having the broadest spread from the pooled mean effect, suggesting methodological issues or a general lack of studies. The risk of small-study bias was assessed as low using Egger’s test (p = 0.4014, Supplementary Fig. S1a).
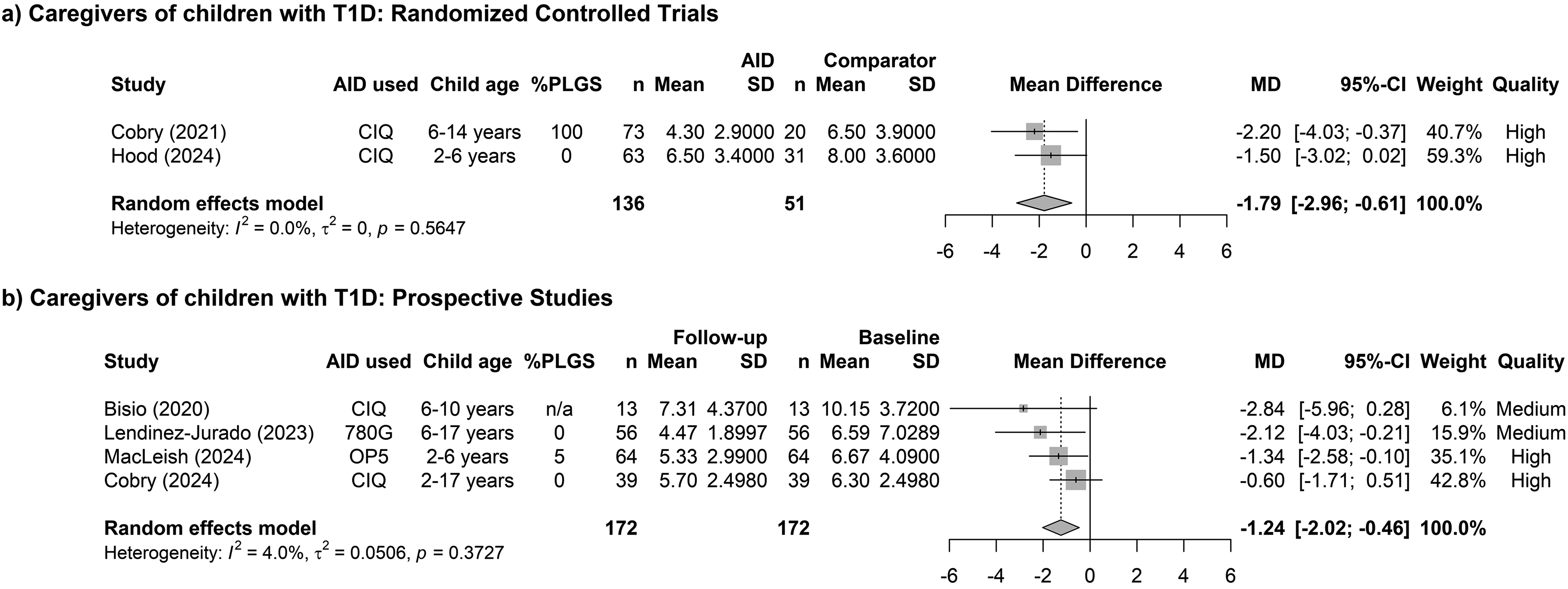
Results of meta-analysis of studies involving caregivers of children with T1D.
Three studies used crossover designs.28,29,33 The duration of AID treatment ranged from 4 to 26 weeks across all studies. Participants were aged 18–80 years, with two studies aimed specifically at older populations.29,33 Two different pump systems were used, and studies used mixed comparators but primarily standalone pumps or SAP systems. Detailed individual study data can be found in Table 1.
Studies had good overall quality, with only minor issues (Supplementary Table S2).
Prospective studies
The supplementary meta-analysis of prospective studies was larger in terms of both number of studies and participants (study n = 7; 551 participants). The pooled mean change in total PSQI scores was −0.42 (95%CI: −0.81, −0.04, p = 0.03, Fig. 2b), indicating a small benefit with AID treatment.25,30–32,34,38,46 The average mean differences varied from −1.4 to −0.2 between studies. Two studies found significant improvements in sleep quality.25,38 The studies were highly asymmetrical in inferred importance, although there was no between-study heterogeneity, with an I2 value of 0%. The funnel plot of study effect sizes was symmetrical, indicating no evidence of publication bias. Formal analysis with Egger’s test confirmed this (p = 0.18, Supplementary Fig. S1b).
This analysis included more, and newer AID systemsand comparators were mixed but consisted primarily of insulin pumps, with a high proportion having predictive low-glucose suspend (PLGS) functionality. All studies reported baseline data and participants had 1–12 months of follow-up after AID initiation. The study by Bisio targeted an older population (65 years or older), 30 whereas the rest included participants between the ages of 18–75 years (see Table 1 for more details).
All studies were of medium to high quality, with only minor issues in some related to attrition and reported study demographics (Supplementary Table S3).
Sleep quality in caregivers of AID-users
RCTs
The primary analysis of PSQI total scores for caregivers consisted of two moderate-sized studies.26,41 In total, this included 136 participants in the intervention group and 51 being comparators. The pooled effect size was −1.79 (95%CI: −2.96, −0.61, p = 0.003, Fig. 3a ), favoring AID systems. There was a slight difference in the inferred importance of studies and no between-study heterogeneity, with I2 at 0%. The studies reported mean changes in PSQI scores ranging from −2.2 to −1.5, with moderately large CIs. Due to the limited number of studies, the funnel plot interpretation was inconclusive, and formal analysis with Egger’s test was not possible (Supplementary Fig. S2a).
Only one pump type was studied and compared with mixed treatments, with studies having durations from 3 to 4 months. Hood et al. included caregivers of children aged 2–6 years, 41 whereas Cobry et al. included caregivers of children aged 6–14 years. 26 More details are available in Table 2.
Both studies were assessed to have high data quality, with only minor unaccounted attrition. The decision to conduct a meta-analysis on these limited studies was based on these quality assessments and the moderate sizes of the studies.
Prospective studies
Finally, a supplementary meta-analysis was conducted on prospective studies of caregivers. PSQI total scores were analyzed in 172 participants across four studies.27,39,42,47 The pooled effect size was −1.24 (95%CI: −2.02 to −0.46, p = 0.002, Fig. 3b), indicating a benefit of AID systems. All studies showed trends toward improvement, and two achieved statistical significance at follow-up.39,42 There was negligible between-study heterogeneity with I2 of 4%. The inferred importance of studies varied considerably between included studies. A funnel plot based on the four studies found the effect size to be closest to the two studies with the least standard error. Funnel plot asymmetry suggested potential small-study bias, but this was not confirmed by formal testing with Egger’s test (p = 0.11, Supplementary Fig. S2).
The studies were evenly split between interventional and observational designs, with participants being assessed at baseline and followed up after up to 6 months. Two studies included caregivers of children as young as 2 years,39,42 and the rest included caregivers of children who were at least 6 years old.27,47 Three different AID systems were used, and comparators varied significantly between studies. Studies were of medium to high quality assessments (see Table 2 and Supplementary Table S3 for more details).
Narrative synthesis of data
Adults using AID
A number of studies were excluded from the meta-analyses of adults with T1D (n = 4) and were instead analyzed narratively.23,35,40,45
The results of these studies varied substantially, and outcomes were measured in different ways, although two studies did demonstrate statistical significant differences in total PSQI score favoring AID systems.23,35 These included one prospective study by Beato-Vibora 23 finding a 9 percent absolute reduction in total PSQI score in participants with baseline PSQI total score >5, and Wong et al. 35 who found a significant reduction in total scores based on online questionnaires. A third prospective study by Eldib 40 found a small, statistically insignificant difference at follow-up, without reported baseline values for comparison. Additionally, the RCT by Michaels 45 found no change between AID and control groups at follow-up but did not report absolute values at this timepoint. All studies had moderate to large sample sizes and included participants aged between 18 and 72 years. Two studies did not report comparator treatments,35,40 and the remaining two used mixed comparators. Three different AID systems were assessed.
Additionally, four studies assessed sleep using actigraphy.29,30,33,45 Only one of these studies was assessed to have acceptable quality and/or had compatible reported outcomes, making meta-analysis not applicable.
None of the studies found significant improvements to any objective sleep parameters with AID treatment. All studies were small, each used a separate AID system and three of the studies specifically included adults aged 60–75 years,29,30,33 whereas the fourth included young adults aged 18–25 years. 45 Most studies were RCTs,29,33,45 and all studies compared AID to insulin pumps with or without PLGS, with one study also comparing with MDI treatment. 45
Detailed information on the above studies can be found in Table 1, and individual reasons for exclusion are listed as part of quality assessment overviews in Supplementary Table S2 and S3.
Children using AID
A total of six studies assessed sleep in children with T1D transitioning to AID systems. Actigraphy parameters were assessed in five of the studies,24,27,39,43,45 whereas two used the Patient-Reported Outcomes Measurement Information System (PROMIS) parent-proxy sleep disturbance questionnaire.39,44,48
No difference was found in any actigraphy measurements in the five studies measuring these, which included two RCTs43,45 and three prospective intervention studies.24,27,39 However, only two of these studies met quality and/or methodological requirements for meta-analysis, and these were of such small sizes that the choice was made to analyze these data narratively.27,39
Studies were all small to moderate in sizes and included children aged 7–17 years. Follow-up varied substantially between studies, from 1 to 24 months, and not all studies included baseline data. Four different AID systems were used across studies and comparators were mixed in three of the studies27,39,45 and not clearly described in two.24,43
The two prospective studies assessing sleep with PROMIS included children aged 2–17 years being followed for 3–12 months. Samples consisted of 39 and 251 participants, respectively. Both studies used the Tandem CIQ AID system, with Ng et al. 44 using two additional systems. Only the study by Cobry reported comparators, which were mixed. 39
Ng et al. 44 found a significant reduction in PROMIS values at 6 and 12 months, whereas Cobry et al. 39 did not find any significant difference at 3 and 6 months. Given the small number of studies, the decision was made not to do meta-analysis.
The full study details can be found in Table 3, with quality assessments and reasons for exclusion being available in Supplementary Table S2 and S3.
Caregivers of AID-users
Finally, five studies of caregivers were excluded from the meta-analyses of total PSQI scores, of which three were prospective studies24,35,37 and two were RCTs.36,43 All studies reported small to moderate improvements in mean PSQI total scores in favor of AID systems. However, only one demonstrated a statistically significant difference. 35 Follow-up varied from 1 to 6 months, and two studies did not include baseline data.36,43 Most studies consisted of caregivers of children aged 6–17 years, although some included caregivers of children down to 2 years.35,36 Sample sizes varied from 19 to 197 participants, and each of the studies examined 1 of 4 different AID systems. Three studies did not sufficiently describe comparator treatments.24,35,43
Some of these studies supplemented PSQI scores with actigraphy data,24,36 both of which were ineligible for meta-analysis. Additionally, two studies included in meta-analyses of total PSQI data also included actigraphy data, but due to limited sample sizes the choice was made not to meta-analyze these data.27,39
Only the study by Madrid-Valero found a significant difference in actigraphy parameters, with a reduction in WASO time. 36 This difference was only 10 minutes though, and did not have a significant effect on overall sleep efficiency.
See Table 2 and Supplementary Table S2 and S3 for detailed data and quality assessments.
Discussion
In this comprehensive systematic review, we synthesized data narratively and through meta-analyses, from all available publications examining the potential benefits of AID systems on sleep quality and quantity.
Our analyses revealed very little evidence for significant impact of new AID systems on subjectively and objectively measured sleep for adults, no impact on the sleep of children, and some support for sleep improvements in caregivers of children with T1D.
Specifically, for adults, the meta-analyses showed no or almost no effect on PSQI total scores. Narratively reviewed data showed ambivalent results for this outcome, whereas actigraphy showed no changes at all.
Data on children with T1D were limited to the extent that meta-analyses could not be performed. Moreover, there was no directly measurable difference in actigraphy outcomes in any of the individual studies. In one study, where outcomes were reported by a proxy and the comparator was unspecified, a minor improvement was found after 6 months. 44
Caregivers of children with T1D seemed to have the most to gain in sleep quality, as measured by the PSQI. This was found in meta-analyses of RCTs as well as prospective studies, whereas narratively reviewed data likewise had a consistent trend toward improvement with AID treatment. However, no meaningful changes were found in actigraphy.
Importantly, while none of the groups saw major improvements to sleep. there are several things to consider when interpreting these results. First, the effect might differ between various AID systems. The MiniMed 670G, a first-generation AID system, has well-documented issues with frequent exits from the automatic function and frequent demands for sensor calibrations. 49 Cobry et al. reported low adherence with AID treatment at the end of the study with the 670G, possibly due to these issues, 24 and it is not known whether the other studies examining this system experienced similar limitations.22,23,28,29,40 Considering the high frequency of alarms and the limited improvement in glycemic variability associated with these systems, the potential impact on sleep may be multifaceted or even adverse. This would be most evident in the meta-analysis of RCTs on adults (Fig. 3a), where most studies used this system. It may also explain the opposing results from the two studies with the greatest impact. Additionally, the study that found a small but significant decrease in sleep efficiency with AID systems—as assessed by actigraphy—used the MiniMed 670G. 29 Second-generation AID systems improved on these issues, which may explain the more consistent but still varied improvements in sleep quality found in studies using these systems.
The second important consideration is which comparators are used. Given the limited number of available studies, we chose to include all types of comparators, including insulin pumps with PLGS functionality, which reduces insulin basal rate in case of pending hypoglycemia. The features of these pumps may already contribute to improved sleep quality, potentially attenuating the observable benefits of AID systems in this context. This could have impacted the meta-analysis of prospective studies in adults, where a substantial proportion of participants used such systems (Fig. 2b). In contrast, the use of these systems is lower in both meta-analyses of caregivers, meaning the impact of AID systems might be more prominent and consistent here. Regardless of comparators used in the studies, it would be expected that the benefits of the AID systems may first be fully realized after some time after initiation. This is due to the need for optimizing the systems and for individuals to develop trust in the automated functionality, meaning an initial decline in sleep quality might be seen. We tried to compensate for this by requiring 1 month of follow-up to be considered eligible, but it would likely require several months to fully adapt.
Importantly, sleep is complex to measure, involving both subjective and objective components. In our study, we could only meta-analyze subjective measurements, specifically total PSQI scores. Drawing conclusions from these will likely result in an oversimplification, as it is a composite score based on many subscores. These include not only sleep duration and efficiency but also the use of sleep medication and perceived sleep quality. Interpretations can vary dramatically depending on which of these parameters primarily drove the overall change. We were unsuccessful in acquiring these subscores from all corresponding authors. Consequently, we were unable to conduct in-depth data analyses of our primary outcome, sleep efficiency, which we acknowledge as a major limitation of our review.
The use of the composite score also makes it difficult to determine the clinical relevance of the results. However, the reported changes appear small in comparison to the entire range of the scale from 0 to 21. Conversely, many studies reported a relatively low (i.e., good) baseline PSQI total score, which we would expect to be rather difficult to improve further. In that context, the changes found might have a clinical impact with greater potential in other populations. Moreover, sleep varies throughout life, and since some studies specifically included older adults, this could influence the analyses. Importantly though, while it is hard to determine if improvements are clinically significant, it would seem with certainty that use of AID systems overall does not worsen sleep quality.
Although actigraphy is a well-validated tool for assessing sleep, it has limitations in younger children, as these may move during REM sleep and actigraphy has low specificity in identifying WASO. This means actigraphy often underestimates sleep duration in this age group. Conversely, for adults, actigraphy might overestimate sleep durations in case of individuals lying still in bed while being awake, adding limitations to the method for this group as well. Furthermore, as sleep duration and composition carry substantially throughout childhood and given the wide age ranges included in many studies, interpreting our limited findings in children with T1D remains challenging.
Optimally, the inclusion of studies using PSG—the gold standard for measuring sleep metrics—would be included, to give the most exact measuring of sleep for participants. However, even this method has limitations, given it commonly requires admission to the hospital and involves a complicated setup with many wearable devices, which in itself possibly compromises sleep. It becomes apparent then, that the development of new and standardized methods to measure and report sleep metrics would be desirable. Indeed, home-based sleep electroencephalography devices are starting to find usage in trials, although studies into the optimal use of these are ongoing. These devices could possibly be a good way to estimate sleep in studies going forward.
A major issue for this review was the limited available literature which—given the low number of RCTs available—led to our decision to include prospective studies for meta-analysis, to ensure enough data were available. This issue was exacerbated by the division into the three study groups, but pooling the data would conversely have made the results significantly more challenging to interpret. To control the potential bias, we meta-analyzed the RCTs and prospective studies separately. Additionally, as expected, most studies were secondary or post hoc analyses, likely contributing to the issues described above.
The strengths of this review are the highly systematic and organized approach to data collection, the comprehensive literature search with citation screening, and the strict quality assessments. Therefore, although the meta-analyses are small, we are confident in the results they produced.
In light of the above-described limitations of included studies, we believe the possible effects on sleep that can be achieved with AID treatment are underestimated and with this review, we have demonstrated that further studies in this field are needed. The new studies should be powered specifically for sleep outcomes, should include both subjective and objective measurements, and be of longer follow-up durations to compensate for early adaption of AID systems. Conducting such studies would help determine if AID systems can alleviate the impaired sleep experience by many people with T1D. Such an improvement, in turn, could substantially improve the health and quality of life of users with T1D, as shorter sleep duration worsens cardiovascular risk, metabolic health, cognitive performance, and mental health. 50
Conclusions
Caregivers of children with T1D experience improvements in sleep quality when their children transition to AID systems, whereas evidence of direct benefits in pediatric AID users remains inconclusive. In adult AID users, the evidence of improved sleep quality is ambiguous, but they may experience minor improvements with second-generation AID systems compared with usual care. Further studies are needed, particularly those incorporating quantitative sleep measures and trials specifically powered to assess sleep outcomes.
Authors Disclosure Statement
K.N. serves on behalf of her institution as an adviser to Medtronic, Abbott Diabetes Care, Convatec, Tandem, and Novo Nordisk; owns shares in Novo Nordisk; has received research grants to the institution from Novo Nordisk, Zealand Pharma, Dexcom, and Medtronic; and has received fees for speaking from Medtronic, Abbott Diabetes Care, and Novo Nordisk. J.S. has served as an educator for Medtronic. She has received funding from Medtronic and Novo Nordisk. J.S. owns shares in Novo Nordisk and has been invited as part of advisory board for Sanofi Aventis. J.S. has received fees for speaking on behalf of Medtronic, Sanofi Aventis, Rubin Medical, and Novo Nordisk. M.Z.S., M.B.C., T.H.A., and T.S. have no conflicts of interest to disclose.
Authors’ Contributions
All authors listed have made substantial, direct, and intellectual contributions to the work in question and have approved it for publication. Specifically, the following is applicable for each author: M.Z.S.: Conceptualization, writing of original draft (lead), data collection and curation, investigation, and visualization. T.H.A.: Methodology (lead), validation, resources, investigation, and review and editing of article. T.S.: Formal analysis (lead), data curation, methodology, software, resources, and review and editing of article. J.S.: Conceptualization, supervision, validation, and review and editing of article. K.N.: Conceptualization, project administration, validation, supervision, and review and editing of article. M.B.C.: Conceptualization, supervision (lead), data collection and curation, validation, and review and editing of article.
Footnotes
Funding Information
All authors are employed at Steno Diabetes Center Copenhagen, a public hospital and research institution under the Capital Region of Denmark, which is partly funded by a grant from the Novo Nordisk Foundation. The funders had no role in any part of this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.