
Abstract
Introduction
Over four out of every five adults with diabetes live in LMICs, where health infrastructure is often underresourced, and access to trained health care professionals and essential medicines is limited. Furthermore, 46.1% of people with diabetes in LMICs are undiagnosed.1,2 These alarming data underscore an urgent global imperative: the development and implementation of sustainable, scalable interventions that can strengthen primary health care systems, promote early diagnosis, and ensure timely intervention to limit the development of costly end-stage complications in settings that are already resource-constrained.
In response to this growing crisis, a transformative, hybrid digital-ambulatory care model is proposed, rooted in International Diabetes Federation (IDF)’s global education standards and underpinned by real-time Clinical Decision Support Systems (CDSS). This innovative model aims to bridge systemic gaps by integrating digital health technologies with real-world clinical practice, offering a comprehensive solution to diagnose and manage cardiometabolic diseases in countries with a high burden of cardiometabolic diseases, particularly LMICs.
Designed with adaptability and scalability in mind, the model is being positioned for phased implementation in high-burden countries such as Bangladesh, Cambodia, India, Maldives, Mauritius, Nepal, Pakistan, and Sri Lanka. These settings, marked by a rising prevalence of diabetes and limited access to specialized care, underscore the pressing need for decentralized yet effective service delivery models. While initial focus is on countries in the Southeast Asia region, similar needs and opportunities for adaptation exist across other IDF regions, including parts of Africa, the Middle East, and Latin America.
Legacy of the International Diabetes Federation
For over seven decades, the IDF has led global advocacy and awareness efforts in diabetes care. It is a key source of global epidemiological data through the IDF Diabetes Atlas and has set international standards in education via its evidence-based IDF Education Framework.
Building on this legacy, the IDF launched the multilingual, CME (Continuing Medical Education)-accredited IDF School of Diabetes in 2016 to strengthen the capacity of health care professionals worldwide. To date, the platform has supported over 110,000 learners across 180 countries with tiered, evidence-based training in diabetes care. 3 Its wide-ranging, evidence-based offerings, including the IDF Global Clinical Practice Recommendations 2025, support learners at various levels of expertise with dedicated tracks for both basic and advanced diabetes management.
This educational infrastructure is especially critical in low- and middle-income countries (LMICs), where primary care providers are often the first—and sometimes only—point of contact for people living with diabetes. These professionals frequently manage complex cardiometabolic cases without specialist support. While access to quality educational resources is vital, knowledge alone is not enough to ensure better outcomes. Structured support and integration into real-world practice are essential. These elements ensure that learning translates into sustained improvements in care.
Since 2023, IDF, as the global technical lead, has partnered with the not-for-profit Sanofi Global Health Unit (GHU) to strengthen cardiometabolic care in 40 priority LMICs. This collaboration combines IDF’s expertise in workforce training, clinical standardization, and system integration with Sanofi GHU’s focus on expanding access to affordable essential medicines and delivery innovations. Working closely with Ministries of Health, WHO regional offices, IDF members, and academic partners, the initiative supports scalable, country-led models that embed global standards into local systems and expand ambulatory care for underserved populations, under IDF’s independent technical oversight. To date, over 5000 health care professionals have been enrolled in structured learning programs through the IDF School of Diabetes. Building on this foundation, IDF and the World Heart Federation are currently exploring a joint initiative to strengthen cardiovascular disease management through integrated capacity-building efforts aligned with national NCD strategies.4,5
Translating Knowledge into Action: The Role of CDSS
CDSS assist clinicians in delivering evidence-based management to their patients and significantly improve the quality of care. The implementation of CDSS is recognized as a best practice, supported by robust evidence of its effectiveness and impact. 6 Developed collaboratively by the AIIMS, New Delhi; Centre for Chronic Disease Control (CCDC), Emory University, USA; and ClinAlly™, the “CARDIOMETCARE-M,” a copyrighted CDSS platform, includes evidence-based algorithms to support the comprehensive management of diabetes, hypertension, dyslipidemia, and related multimorbidity, thereby enabling standardized and high-quality care. The CARDIOMETCARE-M CDSS offers evidence-based care tailored to individual patient profiles. It achieves this by utilizing complex clinical management algorithms by generating personalized and customized management plans, which include screening, management, referral, and follow-up care. These plans include optimal drug recommendations, dosage information, and titration, as well as contraindications, among other relevant details. The CARDIOMETCARE-M CDSS functionality can be seamlessly integrated into digital health platforms to support the continuum of care, which is especially critical for individuals with chronic conditions. One of the key advantages of the CARDIOMETCARE-M CDSS is that all calculations are performed in the backend, relieving health care providers of the burden of memorizing or manually referencing clinical guidelines. The CARDIOMETCARE-M CDSS provides recommendations on the use of evidence-based drugs and starting as well as optimal dosage, as well as contraindications, in a user-friendly manner. This enables the implementation of CDSS recommendations in clinical practice, which are easily understandable and accessible for all health care professionals.
The proposed model has a lot of similarities with the successful HIV clinics concept. The HIV clinics have incorporated CDSS to streamline clinical workflows, facilitate adherence to CDC guidelines for HIV and STI screening, and enhance the delivery of pre-exposure prophylaxis. These systems generate electronic alerts, prompt appropriate testing and medication orders, and support standardized decision-making based on individual patient risk factors. Practice coaching and user-centered design have further boosted the usability and effective adoption of CDSS in HIV care settings, improving provider efficiency, testing rates, and patient outcomes. Overall, CDSS helps HIV clinics deliver guideline-based, timely, and equitable care to diverse populations.7–9 This CARDIOMETCARE-M CDSS platform has been developed and validated through an iterative process involving rigorous testing at multiple levels of care, including randomized clinical trials and real-world implementation projects. The findings of different trials are summarized in Table 1.
Finding of Trials in Development of the CDSS
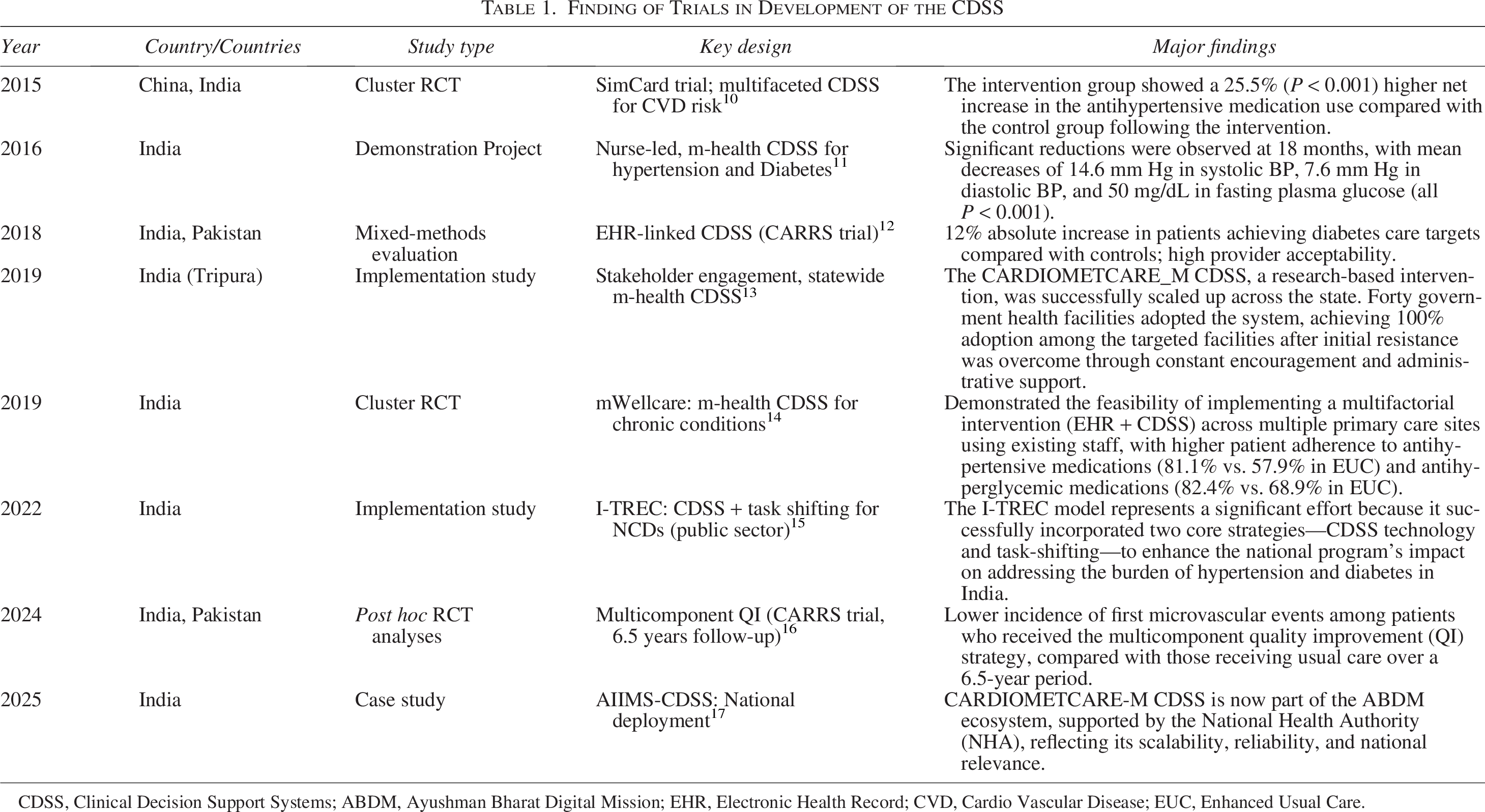
CDSS, Clinical Decision Support Systems; ABDM, Ayushman Bharat Digital Mission; EHR, Electronic Health Record; CVD, Cardio Vascular Disease; EUC, Enhanced Usual Care.
These studies underscore the adaptability, effectiveness, and scalability of CDSS and m-health tools in diverse high-burden countries, particularly within LMIC contexts. This initiative is also poised to play a pivotal role in systematically screening and preventing diabetes-related complications. By integrating structured risk assessment protocols, point-of-care diagnostics, and evidence-based clinical decision support tools within routine ambulatory care, the model enables the timely identification and management of emerging microvascular/macrovascular complications. This anticipatory approach not only enhances the quality of care but also contributes to reducing the long-term clinical and economic burden associated with end-stage complications (e.g., blindness, foot ulceration, and renal failure with loss of livelihood), which has an especially profound impact in resource-constrained settings.
To consolidate these proven interventions at the clinic level, IDF and its partners are launching the IDF clinics, a global network of branded, quality-assured, digitally enabled ambulatory care clinics specializing in cardiometabolic conditions. These clinics will deliver structured education through masterclasses and certified training, embed CDSS into outpatient workflows for real-time decision support, and operate in private and mixed-sector settings. They will be supported by regional coordination units and quality monitoring mechanisms, all under the trusted IDF clinics brand, which lends credibility, visibility, and assurance to providers and patients alike.
Path to Implementation: A Multicountry, Multipartner Approach
This innovative, hybrid digital-ambulatory model (Fig. 1) will be implemented through a robust multicountry, multipartner approach, ensuring both reach and sustainability. The IDF will be the lead implementing agency, leveraging its global reputation, technical expertise, and extensive network. Technical partners such as the AIIMS, Delhi, the CCDC, and ClinAlly™ will bring specialized clinical research, digital health, and data integration capabilities. IDF Regions and Member Associations will be regional anchors to ensure contextual relevance and on-the-ground coordination, bridging the gap between international standards and national health priorities.
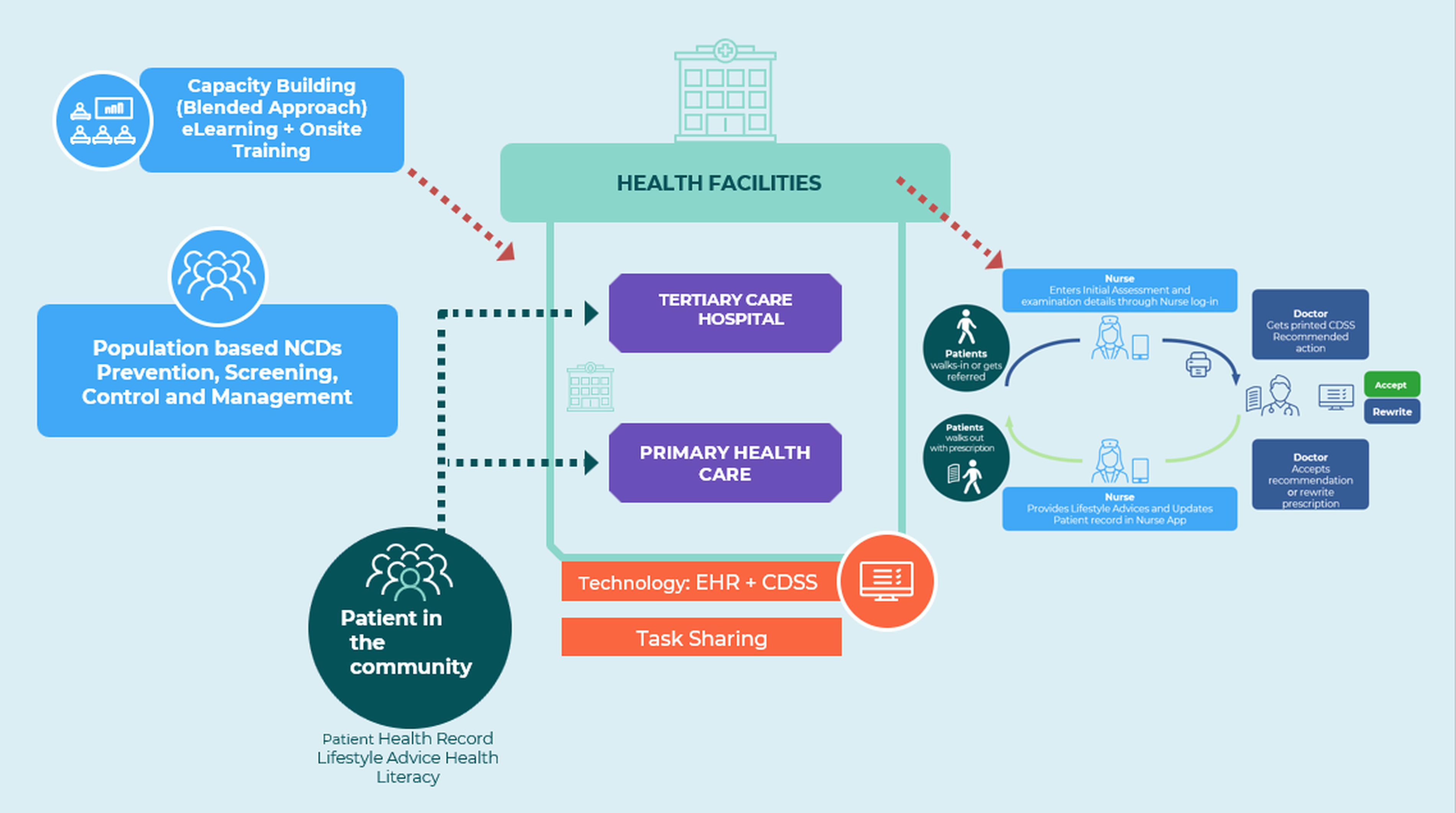
CARDIOMETCARE-M CDSS implementation model. CDSS, Clinical Decision Support Systems.
Local implementation will be driven by health authorities, clinics, and frontline health care providers who are best positioned to tailor the model to the needs of their communities. These stakeholders will be supported by training, capacity building, and clinical tools aligned with IDF’s global education standards. Interested donor agencies will play a pivotal role in funding the initiative and enabling scale-up, ensuring that innovation is not limited to pilot sites but reaches wider populations across multiple LMICs. The model is designed for long-term financial sustainability. It promotes coinvestment from participating clinics in areas such as certification, training, and digital tools, while industry support helps subsidize infrastructure and platform deployment. This ensures that financial barriers do not restrict access, supporting equitable care delivery across diverse geographies and populations. Importantly, this model is not theoretical and is rooted in evidence, pilot-tested, and ready for scale.
To ensure smooth uptake and implementation of the innovative model across settings, several safeguards have been incorporated into the technology design. The CARDIOMETCARE-M CDSS does not require any patient identifiers to generate clinical recommendations, thereby minimizing risks related to personal data privacy. The platform is hosted on secure cloud servers with all endpoints protected through client-specific authentication tokens, and data transmission occurs over 128-bit SSL-encrypted networks. The CARDIOMETCARE-M servers are WASA-certified, and regular Vulnerability Assessment and Penetration Testing is conducted to maintain system integrity and compliance with security standards. 18
Regarding medical liability, the CARDIOMETCARE-M CDSS is designed solely as a clinical decision-support tool to assist health care professionals, without substituting or overriding their clinical judgment. Recommendations are generated based on the data entered by qualified health care personnel and are intended to support, not replace, evidence-based decision-making. The final responsibility for diagnosis and prescription remains with the treating clinician, consistent with the legal and ethical framework of medical practice in the respective countries. 19
Conclusion
The IDF clinics initiative offers a scalable, evidence-based framework to integrate global clinical expertise into local health care delivery. By combining structured education, real-time clinical decision support, and community-centered care models, the initiative empowers primary care providers in high-burden settings, particularly in LMICs, to manage cardiometabolic diseases more effectively. Through strategic partnerships with academic institutions, governments, foundations, and the private sector, and supported by strong leadership and community engagement, the initiative is well positioned for broader adoption. These include reduced complications, cost savings through early intervention, and improved workforce efficiency via structured training and digital support, delivering both individual and system-level impact. It aims to deliver integrated, high-quality ambulatory care and to transform primary health care systems by translating knowledge into measurable and sustained improvements in health outcomes.
Footnotes
Funding Information
No funding support is provided for this article.
Disclosure Statement
All authors declare no conflicts of interest.