
Abstract
Objective:
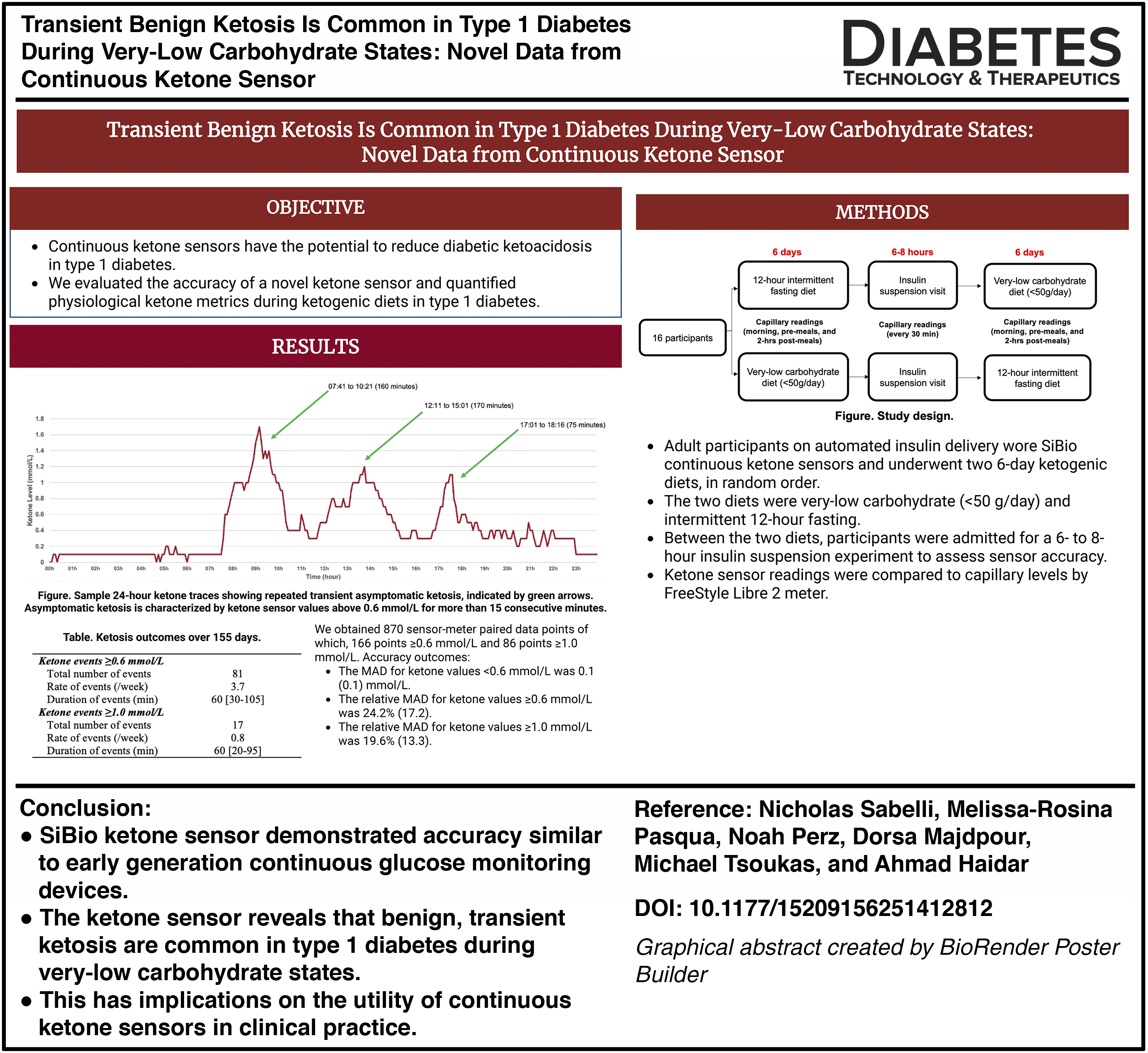
Continuous ketone sensors have the potential to reduce diabetic ketoacidosis in type 1 diabetes. We evaluated the accuracy of a novel ketone sensor and quantified physiological ketone metrics during ketogenic diets in type 1 diabetes.
Research Design and Methods:
Adult participants on automated insulin delivery wore SiBio continuous ketone sensors and underwent two 6-day ketogenic diets, in random order. The two diets were very-low carbohydrate (<50 g/day) and intermittent 12-h fasting. Between the two diets, participants were admitted for a 6- to 8-h insulin suspension experiment to assess sensor accuracy. Ketone sensor readings were compared with capillary levels by FreeStyle Libre 2 meter.
Results:
Sixteen participants completed the study (age 36.5 [17.0] years, HbA1c 7.0% [0.6], insulin dose 0.72 [0.26] units/kg) and provided 870 sensor-meter paired data points. The mean absolute difference (MAD) for ketone values <0.6 mmol/L was 0.1 (0.1) mmol/L and the relative MADs for ketone values ≥0.6 and ≥1.0 mmol/L were 24.2% (17.1) and 19.6% (13.3), respectively. During the ketogenic diets (155 days), there were 81 ketosis events (3.7 events/week) ≥0.6 mmol/L of more than 15 min, with a median duration of 60 (30–105) min/event. All ketosis events except one were asymptomatic. Glucose levels, basal insulin delivery, and time of the day were not related to ketosis events.
Conclusions:
SiBio ketone sensor demonstrated preliminary accuracy and reveals that benign, transient ketosis are common in type 1 diabetes during very-low carbohydrate states. This has implications on the utility of continuous ketone sensors in clinical practice.
Trial Registration:
Clinicaltrials.gov NCT06420518.
Introduction
Insulin deficiency in type 1 diabetes impairs glucose uptake and cellular metabolism, prompting hyperglycemia and a metabolic shift toward lipolysis and ketogenesis. 1 Although this adaptation protects against starvation, excessive ketone accumulation overwhelms the body’s buffering capacity and can result in diabetic ketoacidosis. Diabetic ketoacidosis remains a serious complication of type 1 diabetes and a major cause of hospitalizations and deaths, particularly in youth.2,3
Ketoacidosis may also occur in type 1 diabetes through a different mechanism with the use of sodium-glucose cotransporter-2 (SGLT2) inhibitors. 4 Several trials have shown that SGLT2 inhibitors increase the risk of diabetic ketoacidosis, including during euglycemia, compared with placebo, particularly in women, insulin pump users, and people with lower body mass index (BMI).5,6 SGLT2 inhibitors are thus not approved in type 1 diabetes, but despite their risk, their off-label use is increasing 7 due to their glycemic, renal, and cardiac benefits. 8
Feasibility of continuous ketone monitoring has recently been demonstrated in humans 9 and it is currently undergoing development and clinical testing. Continuous ketone monitoring may help reduce the risk of ketoacidosis from all causes;10,11 however, the practical utility of ketone sensors remain unclear and healthy physiological ketone fluctuations are poorly understood in type 1 diabetes. Here, we used a novel continuous ketone sensor to assess metrics of ketosis during two ketogenic diets in adults with type 1 diabetes on automated insulin delivery. This, to our knowledge, is the first detailed reporting of continuous ketone kevels during outpatient free-living settings in type 1 diabetes.
Methods
The study enrolled 16 participants aged 18 years or older with a clinical diagnosis of type 1 diabetes for at least 1 year and who had been using a closed-loop insulin pump and continuous glucose monitor system for more than 30 days. Exclusion criteria included recent (≤2 weeks) use of SGLT2 inhibitors, current use of ascorbic acid (vitamin C) as it may impair sensor accuracy, severe hypoglycemia episode or diabetes ketoacidosis in the last month, pregnancy, or any medical or psychiatric illness that interferes with the study procedures. The study was approved by the Advarra research ethics board.
Participants underwent 6-day very-low carbohydrate diet (<50 g/day) and 6-day intermittent 12-h fasting diet, in random order, separated by 1 day (Supplementary Fig. S1). On the 12-h fasting diet, participants were permitted to modify their fasting window from day to day, provided the fasting duration remained constant, while no restriction on carbohydrate consumption was imposed. Similarly, on the very-low carbohydrate diet, participants were allowed unrestricted meal timing, provided their carbohydrate intake stayed below 50 g per day. Hypoglycemia treatments were allowed at all times and were not counted toward the diets. Participants were asked to measure capillary ketone levels by FreeStyle Libre 2 meter every morning, pre-meals, and 2 h postmeals.
On the morning of the day between the two diets, participants were admitted to our clinical research facility for a 6- to 8-h insulin suspension experiment. Participants arrived fasted from 22 h the previous day and were provided with a breakfast containing less than 5 g of carbohydrates prior to initiating insulin suspension. Participant’s insulin pumps were suspended for a maximum of 8 h, halting both basal and bolus insulin delivery, and capillary ketone measurements were taken every 30 min. Insulin delivery was resumed if capillary ketone levels exceeded 2.5 mmol/L, capillary glucose levels exceeded 22.0 mmol/L, or participants experienced intolerable symptoms. After discharge, participants were not bound by any diet for the remainder of the day. On the following day, participants initiated the second diet strategy, which was followed for the next 6 days.
Throughout the study, participants wore a continuous ketone sensor (SiBionics, Shenzhen, China). The ketone sensor was hypodermic and was installed on the back of the upper arm. The sensor was factory-calibrated (i.e., does not require calibrations with capillary values), had a 14-day lifespan, was waterproof, and provided continuous readings to a companion mobile application every 5 min in the range of 0–8 mmol/L with 0.1 mmol/L increments. Glucose sensor and insulin pump data were downloaded, for analysis but were not used during the study period.
Sensor accuracy was assessed using the mean difference (MD), the mean absolute difference (MAD), and the relative MAD between time-matched sensor and capillary ketone levels. The relative MAD was only reported for capillary ketone levels ≥0.6 and ≥1.0 mmol/L since lower ketone levels will result in a misleading or an undefined relative MAD (e.g., a trivial error of 0.1 mmol/L will be reported as 100% error if capillary ketone level was 0.1 mmol/L, relative MAD will lead to a division by zero if capillary ketone level was 0 mmol/L).
The number and duration of ketone sensor events ≥0.6 and ≥1.0 mmol/L were reported as well as the times spent in different ranges of ketone levels and rates of change vents ≥0.4, ≥0.6, and ≥1.0 mmol/L/h. Data were reported as mean (SD) or median [IQR].
Results
Sixteen participants completed the study (11 females, age 36.5 [17.0] years, BMI 26.7 [7.6] kg/m2, HbA1c 7.0% [0.6], insulin dose 0.72 [0.26] units/kg, no use of adjunct therapies). During insulin suspensions (Supplementary Fig. S2) and the outpatient phase, we obtained a total of 870 sensor-meter paired data points. For ketone values <0.6 mmol/L (704 data points), the MAD between the sensor and meter readings was 0.1 (0.1) mmol/L (Table 1). For ketone values ≥0.6 (166 data points) and ≥1.0 mmol/L (86 data points), the relative MADs were 24.2% (17.1) and 19.6% (13.3), respectively (Table 1). We conclude that the ketone sensor demonstrated preliminary accuracy and may be used to assess physiological ketone fluctuations. Supplementary Figures S3 and Figure S4 show the Bland–Altman and correlation plots of the sensor-meter paired data points, further supporting the sensor accuracy.
Accuracy Outcomes Comparing the SiBio Ketone Sensor with Capillary Levels Measured by FreeStyle Libre 2 Meter
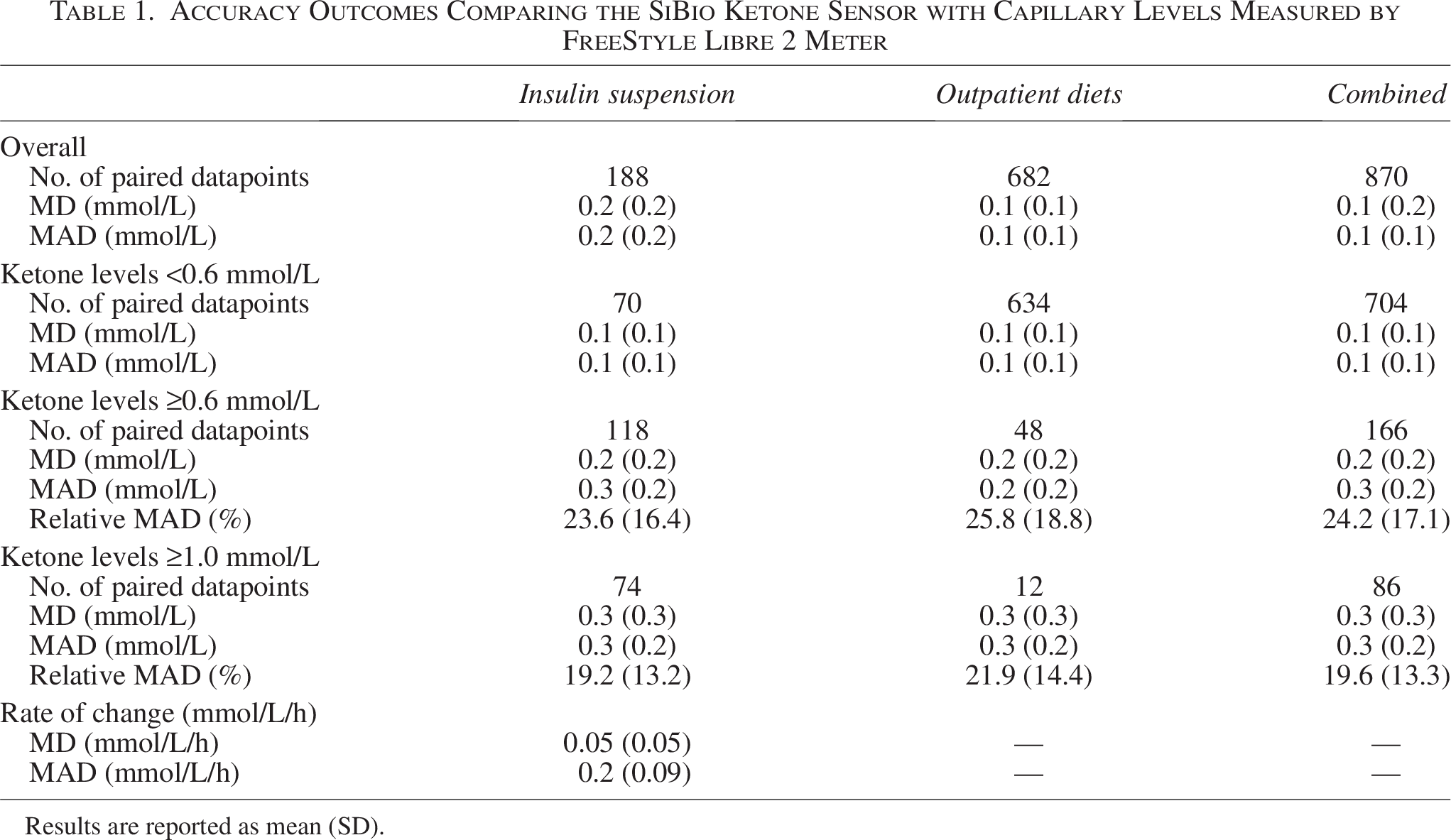
Results are reported as mean (SD).
We evaluated diet adherence and excluded all very-low-carbohydrate diet days for four participants due to noncompliance. In contrast, all participants adhered to the 12-h fasting diet. Supplementary Table S3 summarizes the ketone metrics from the excluded very-low carbohydrate days.
During the ketogenic diets (155 days), the number of continuous ketosis events ≥0.6 mmol/L of more than 15 min was 81 events (3.7 events/week), with a median duration of 60 (30–105) min/event (Table 2). The number of continuous ketosis events ≥1.0 mmol/L of more than 15 min was 17 events (0.8 events/week), with a duration of 60 (20–95) min/event. All ketosis events except one were asymptomatic and thus considered benign (Table 2).
Ketone Metrics During Two Ketogenic Diets
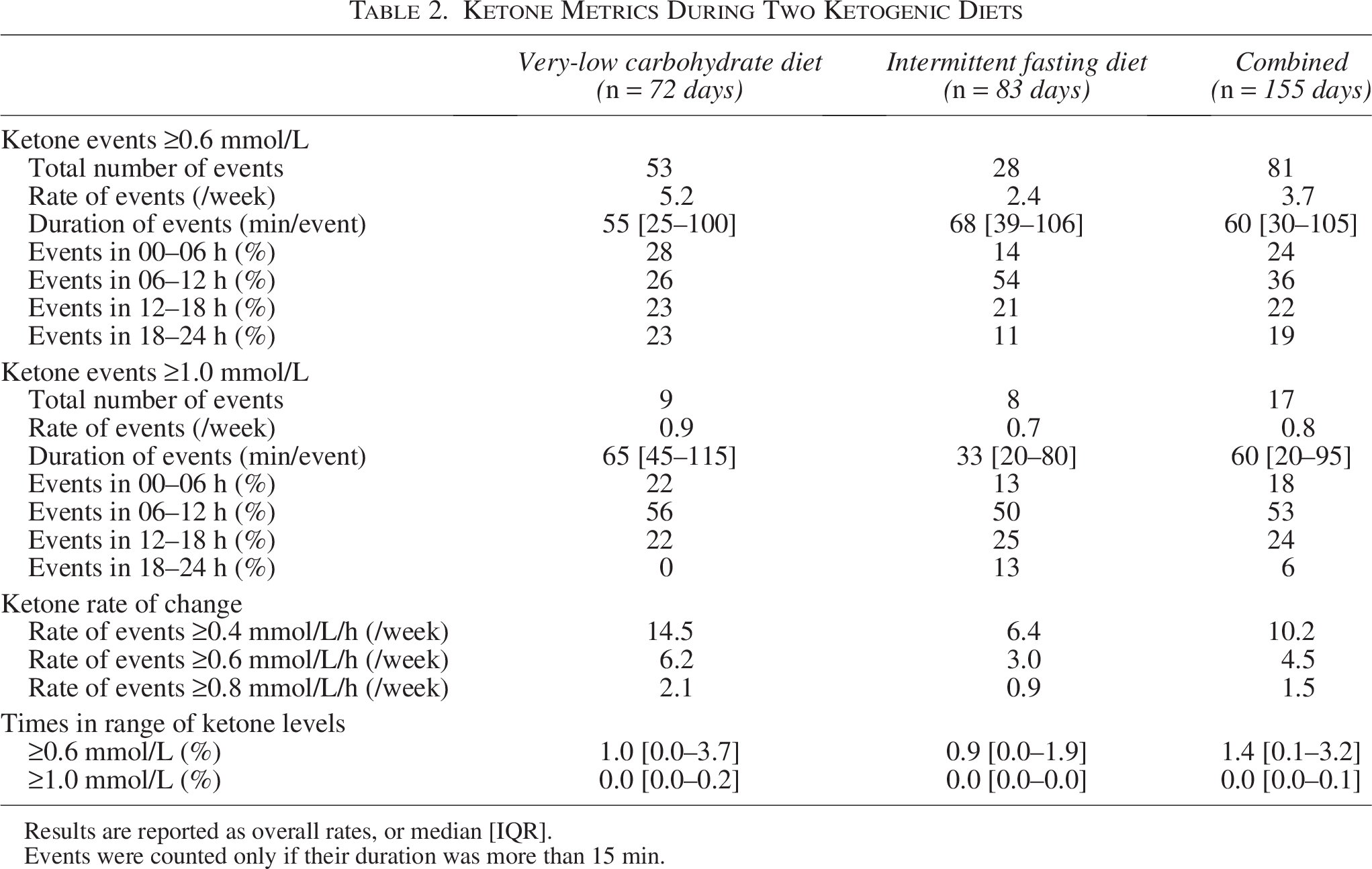
Results are reported as overall rates, or median [IQR].
Events were counted only if their duration was more than 15 min.
There was variability in number of ketosis events between participants. While four (25%) participants had 9–14 events ≥0.6 mmol/L over the 12-day period of the two diets, five (31%) participants had not a single event. No correlation was found between number of events and age (ρ = 0.04, P = 0.88), duration of diabetes (ρ = −0.08, P = 0.77), HbA1c (ρ = 0.22, P = 0.41), daily insulin dose (ρ = −0.07, P = 0.81), or BMI (ρ = −0.08, P = 0.77) of participants. Very strong correlation was found between the rate of events and the percentage of ketone time spent ≥0.6 mmol/L (ρ = 0.95, P < 0.001), suggesting that both could be used as therapeutics targets. Four (25%) participants had percentage of ketone time spent ≥0.6 mmol/L of more than 3.2% [equivalent to 46 min/day; Table 2].
We also assessed physiological ketone rate of change from sensor data. During the ketogenic diets, the frequency of events with rate of change ≥0.4, ≥0.6, and ≥0.8 mmol/L/h for more than 15 min were 10.2, 4.5, and 1.5 events/week (Table 2). The ketone rates of change at the start of the ketosis events ≥0.6 and ≥1.0 mmol/L were 0.6 (0.4) and 0.6 (0.3) mmol/L/h, respectively.
Our study did not include periods of normal diets. However, we analyzed ketone events in those four participants who did not follow the very-low carbohydrate diet, and instead consumed their regular diet (average of 175 g of carbohydrates ingested per day). In those participants, there were 0 ketosis events more than 0.6 mmol/L in 24 days. This suggests that the very-low carbohydrate diet was the primary cause for the repeated transient ketosis events observed in our study.
We did not observe differences between average glucose levels during ketosis events ≥0.6 mmol/L compared with other times (8.7 vs. 8.8 mmol/L, respectively; P = 0.79). Similarly, these ketosis events were spread throughout the day (23% of events at 00–06 h, 36% at 06–12 h, 22% at 12–18 h, and 19% at 18–24 h), suggesting no diurnal pattern. Moreover, the amount of basal insulin delivered 1.5–2.5 h prior to the start of these ketosis events was not different from other times (0.86 vs. 0.94 U/h, respectively; P = 0.47), suggesting that basal insulin reductions did not cause these ketosis events.
There were more ketosis events ≥0.6 mmol/L during the very-low carbohydrate diet compared with the intermittent fasting diet (5.2 vs. 2.4 events/week; P = 0.015), but the rate of ketosis events ≥1.0 mmol/L was not different between the two diets (P = 0.93). Similarly, there were higher number of events with rate of change ≥0.4 mmol/L/h (P < 0.001) and ≥ 0.6 mmol/L/h (P = 0.01) during the very-low carbohydrate diet compared with the intermittent fasting diet (Table 2), but not events with rate of change ≥0.8 mmol/L/h (P = 0.16). The third-quartile participant spent 3.7% of the time [equivalent to 53 min/day] with ketone levels ≥0.6 mmol/L during the very-low carbohydrate diet compared with 1.9% of the time [equivalent to 27 min/day] during the intermittent fasting diet (Table 2).
We included sample 24-h ketone traces to illustrate the points raised above and the challenges. Figure 1 shows sample ketone traces with transient asymptomatic ketosis and sample ketone traces that were unchanged in the region of 0–0.1 mmol/L. Supplementary Figure S5 shows sample ketone traces with repeated transient asymptomatic ketosis. Supplementary Figure S6 shows raising ketone levels due to infusion set removal (mimicking a failure) vis-a-vis benign transient ketosis in two consecutive days in the same individual. Furthermore, Supplementary Figures S7–S19 show overlapping ketone and glucose sensor traces for all participants during the insulin-suspension visits.

Sample 24-h ketone traces with transient asymptomatic ketosis (top three panels) and unchanged levels in the region of 0–0.1 mmol/L (bottom three panels). The green arrows indicate an asymptomatic ketosis event, characterized by ketone sensor values above 0.6 mmol/L for more than 15 consecutive minutes.
Discussion
We report first data of physiological ketone fluctuations in adults with type 1 diabetes using automated insulin delivery during ketogenic diets—outside the context of acute illness, diabetic ketoacidosis, and insulin omission. Our data revealed that transient benign ketosis events are common in type 1 diabetes during very-low carbohydrate state.
These recurrent transient ketosis events will have important implications on the integration of ketone sensors in clinical practice. First, current guidelines call for action and close monitoring if capillary ketone levels are above 0.6 mmol/L. 12 To avoid unnecessary alarms and alarm fatigue, ketone sensor alarms may need to be set higher than 0.6 mmol/L or should be triggered if ketone values were higher than 0.6 mmol/L for a prolonged duration (e.g., 2 h). Second, a potential application of ketone sensors is to help early detection of infusion set failures in insulin pump, 13 as raising ketone levels is an indicative of lack of insulin administration. However, any simple threshold-based guidelines to initiate an infusion set change may be falsely triggered by the recurrent transient ketosis events. Advanced algorithms might be needed to differentiate between elevated ketone levels due to infusion set problems from benign transient ketosis. Third, ketone sensors may be utilized to allow for the safe use of SGLT2 inhibitors in type 1 diabetes 7 to exploit their cardiorenal benefits. 10 However, recurrent harmless ketosis detected by the sensor may lead to discontinuation of SGLT2 inhibitors due to perceived risks that may not be related to the drug itself or any imminent danger.
Ketosis events were not related to glucose levels, basal insulin delivery, or time of the day. However, we did not collet exercise data. Early literature shows that short-term (1–2 days) very-low carbohydrate diets, as opposed to normal diet, in healthy individuals lead to pronounced (up to 2.5 mmol/L) ketosis 2–3 h post-exercise.14–16 It is our speculation that at least some of the observed ketosis events in our study were caused by exercise.
Integrating additional signals other than glucose values to determine insulin doses in automated insulin delivery systems has been an active area of research.17–19 In a combined continuous glucose and ketone sensor, such an integration would be straightforward from a technical point of view. However, the clinical benefits of adding continuous ketone values to the insulin dosing algorithm are yet to be determined. If a target ketone range is determined (e.g., 0–0.6 mmol/L) above which insulin delivery is increased, transient benign moderate ketosis above this range in the context of euglycemia might lead to needless insulin over delivery. On the other hand, in the event of overt ketosis above 1.0 mmol/L, action outside of automated insulin delivery algorithm is typically needed for resolution (e.g., verifying and changing pump infusion set, eating carbohydrate and injecting a bolus,20,21 etc.). Moreover, the target range of ketone levels are not established yet, as emerging literature suggests that moderate ketosis might have cardiac benefits.22–26
The study had several strengths. The sensor accuracy was assessed in both outpatient free-living settings as well as controlled inpatient settings. We had a sufficient number of data points with ketone levels above 0.6 and 1.0 mmol/L. We tested two different ketogenic diet strategies. The study had several limitations too. The study did not include a period with normal diet to act as a control, and we did not systemically collect physical activity and energy expenditure data to correlate them with ketone levels. Moreover, we did not correct for multiplicity in our several statistical tests.
Wearable digital health technologies have the potential to empower patients and provide them with a greater sense of control over their disease management. 27 In type 1 diabetes, the introduction of continuous glucose sensors has revolutionized clinical care. It is still early to predict what impact ketone sensors will have on clinical practice. Our data provide the first glimpses of continuous ketone measurements in type 1 diabetes on automated insulin delivery systems, subjected to ketogenic diets.
Authors’ Contributions
N.S. conducted and coordinated the trial. N.S. and A.H. wrote the article. N.S., M.R.P., M.T., and A.H. reviewed/edited the article. N.P. performed statistical analysis and data processing. D.M., N.S., and A.H. wrote the study protocol. M.R.P. and M.T. provided clinical oversight for the study and conducted admission visits. A.H. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Author Disclosure Statement
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.S.: None. M.R.P.: Speaker’s Bureau; Abbott, Sanofi, Medtronic. N.P.: None. D.M.: None. M.T.: Speaker’s Bureau; Novo Nordisk, Eli Lilly, Boehringer-Ingelheim, Janssen Pharmaceuticals, Inc, Sanofi. A.H.: Research Support; Tandem Diabetes Care, Dexcom, Ypsomed, Beta Bionics. Consultant; Eli Lilly, Abbott.
Funding Information
This study was funded by Diabetes Quebec.
Data Sharing Statement
All anonymous raw data can be shared free of charge by the corresponding author following a material transfer agreement that respects limitations in the informed consent process. After approval, reasonable efforts will be made for the data to be shared within 3 months.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.