
Abstract
Background:
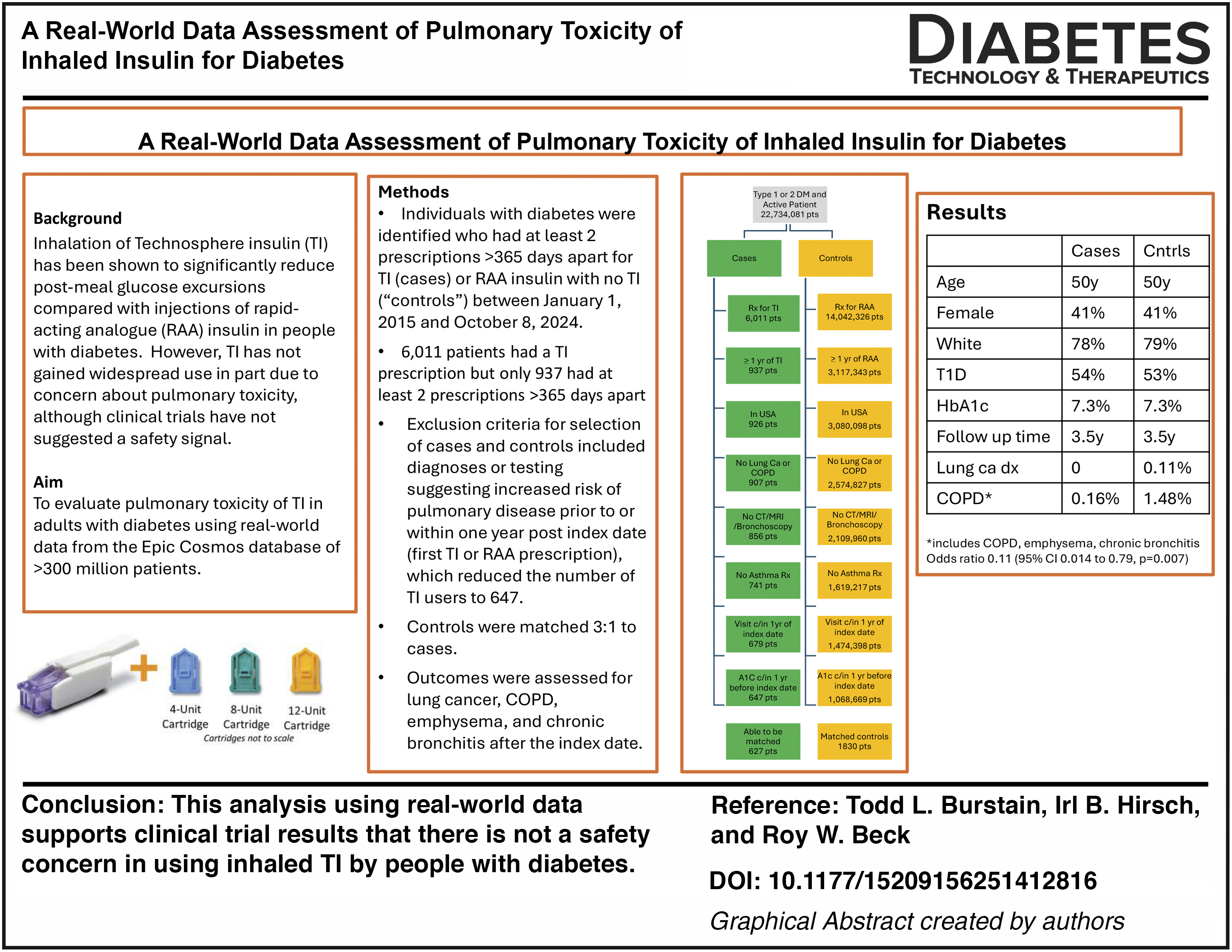
Inhalation of technosphere insulin (TI) has been shown to significantly reduce postmeal glucose excursions compared with injections of rapid-acting analogue (RAA) insulin in people with diabetes. However, TI has not gained widespread use in part due to concern about pulmonary toxicity, although clinical trials have not suggested a safety signal. To evaluate the pulmonary toxicity of TI, an analysis was performed using real-world data (RWD) in the Epic Cosmos database of approximately 300 million patients.
Methods:
From the Cosmos database, individuals with diabetes were identified who had at least two prescriptions for TI (cases) or RAA insulin with no TI prescriptions (“controls”) between January 1, 2015, and October 8, 2024, with >365 days between the first and last prescription. The first TI or RAA prescription was considered as the index date. Exclusion criteria for selection of cases and controls included diagnoses or testing suggesting increased risk of pulmonary disease prior to or within 1 year postindex date. Controls were matched 3:1 to cases on a variety of factors. Outcomes were assessed for diagnosis codes for lung cancer, chronic obstructive pulmonary disease (COPD), emphysema, and chronic bronchitis at least 1 year after the index date.
Results:
Inclusion criteria were met for 647 cases, which were matched to 1830 controls. Beginning 1 year postindex date, a lung cancer diagnosis was recorded in no cases and in two controls (0.11%), while a diagnosis of COPD, emphysema, or chronic bronchitis was recorded in 1 (0.16%) case and in 27 (1.48%) controls (odds ratio = 0.107, 95% CI: 0.014–0.787, P = 0.007).
Conclusions:
While there are limitations to the interpretation of results from a study using RWD, it is reassuring that there was no increase in pulmonary toxicity attributable to inhaled TI for treatment of diabetes with respect to lung cancer, COPD, emphysema, and chronic bronchitis.
Introduction
Since the publication of the first study utilizing real-world data (RWD) from electronic health records in 2004, 1 more than 2000 articles based on RWD have been published. 2 Although RWD cannot be used to address all research questions, RWD studies can be very powerful for addressing clinically relevant issues related to the effectiveness and safety of treatments in real-life use, provided that potential sources of bias and confounding are considered when interpreting the results. Compared with randomized controlled trials (RCTs), RWD studies may be more representative of the general population than a cohort enrolled in an RCT and can be conducted far more quickly and at lower cost.
Inhaled technosphere insulin (“TI,” Afrezza®, MannKind Corporation, Danbury, CT), which was approved for use in adults with diabetes by the Food and Drug Administration in 2014, is a dry-powder formulation of recombinant human insulin absorbed onto Technosphere microparticles for oral inhalation using a breath-powered inhaler. It is used instead of subcutaneously injected rapid-acting analogue (RAA) insulin for meals to limit postmeal hyperglycemia and at other times when a correction dose is needed to reduce hyperglycemia. It has pharmacokinetic advantages over RAA insulin with a more rapid onset of action and more rapid dissipation.3–5 Since it is inhaled and absorbed in the lungs, there has been theoretical concern about pulmonary toxicity.
A comprehensive review of available clinical trials and other data did not show a pulmonary safety concern. 6 However, a recent RWD analysis using the TriNetX database, while not finding an increase in lung cancer, did find an apparent increase in cases of chronic obstructive pulmonary disease (COPD), 7 although a commentary suggested that this could be due to ascertainment bias. 8 The lack of availability of patient-level anonymized data in the TriNetX database limited the authors’ ability to evaluate the bias.
Another RWD database is Epic Cosmos, which includes longitudinal records of data collected across U.S. health systems utilizing the Epic electronic health record for approximately 300 million patients (as of October 23, 2025). 9 The database includes comprehensive patient-level inpatient and outpatient data integrating outpatient visits, hospitalizations, lab and imaging results, and all other testing results. The patients in the database closely mirror U.S. Census data for age, race, ethnicity, insurance coverage, and social vulnerability index. 10
We utilized the Cosmos database to compare the incidences of lung cancer and COPD in individuals with diabetes using TI versus RAA insulin.
Methods
Cosmos data (updated October 8, 2025) were obtained for the analyses, using structured query language queries of the Expertly Determined De-Identified data. Individuals with diabetes were identified in the database who had at least two prescriptions for TI (coded as Afrezza human insulin inhalation powder, “cases”) or RAA insulin with no TI prescriptions (lispro, aspart, glulisine, fast-acting aspart, lispro-aabc; “controls”) between January 1, 2015, and October 8, 2024, with > 365 days between the first and last prescription. The January 1, 2015, date was based on the approval of TI for adults with diabetes by the Food and Drug Administration in 2014, and the October 8, 2024, date was selected to have a minimum 1-year follow-up period after at least 1 year of drug exposure. The first TI or RAA prescription was considered as the treatment index date. Additional inclusion and exclusion criteria for the cases and controls are shown in Table 1.
Inclusion and Exclusion Criteria for Cases and Controls
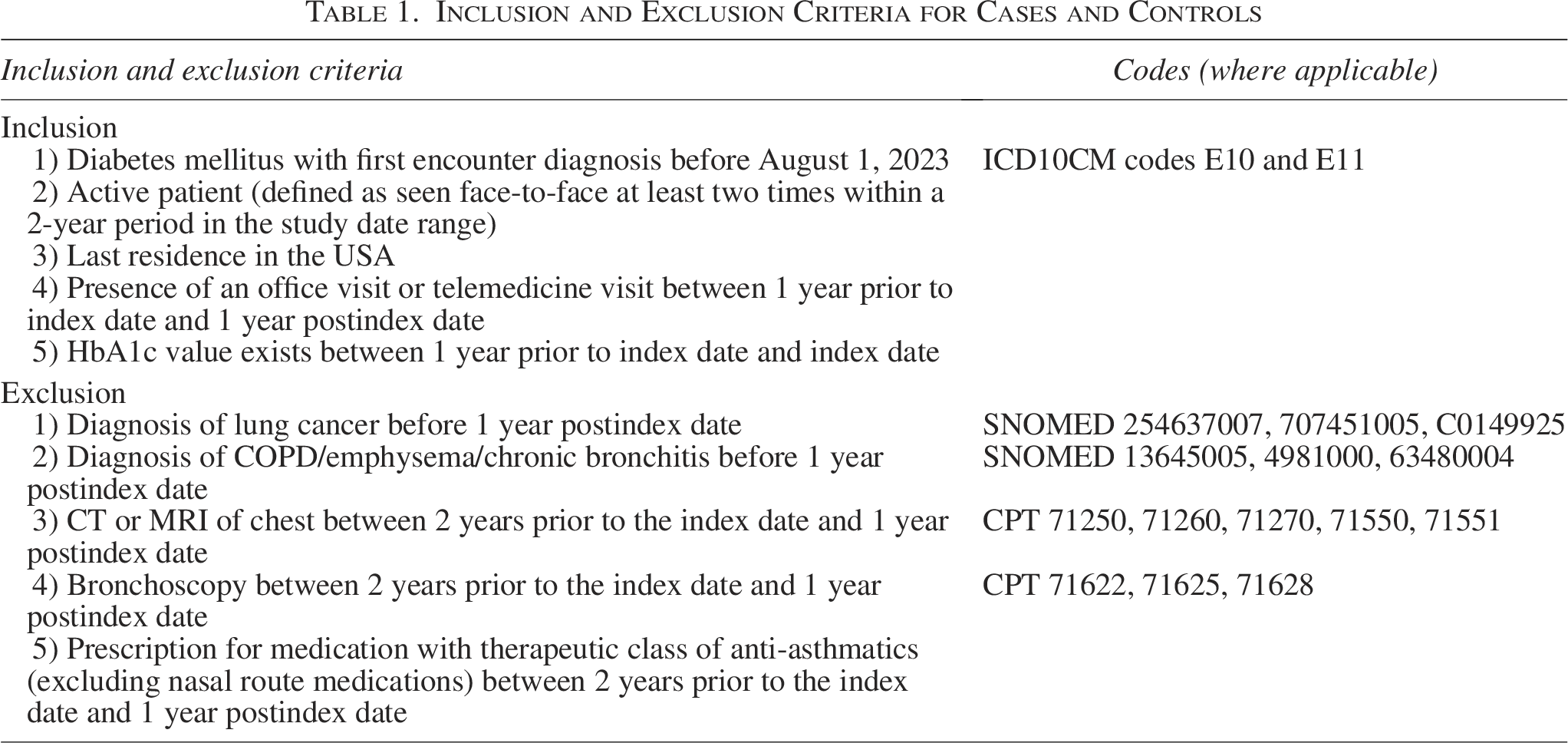
Controls were matched 3:1 to cases using MatchIt package in R Studio (Posit Software PBC. Version 2025.5.1 Build 513), based on type of diabetes (type 1 or type 2), legal sex, race (first race if multiple listed), ethnicity (Hispanic or non-Hispanic), insurance class, birth year ± 2 years, last recorded smoking status, diagnosis of asthma, follow-up time from index date to last encounter, and last HbA1c before index date ± 1%. Utilizing a 3:1 ratio of controls to cases instead of 1:1 increases statistical power by enhancing the precision of the statistical test results.
The outcomes of interest were lung cancer (SnoMed CT codes 254637007, 707451005, C0149925) and a composite of COPD (SnoMed CT code 13645005), emphysema (4981000), and chronic bronchitis (63480004).
For each of the two outcomes, an odds ratio (OR) with 95% confidence intervals comparing the cases and controls was calculated using a 2 × 2 contingency table (two-sided chi-square analysis).
Results
The database search identified 6011 patients with a prescription for TI; however, only 937 met the criteria of having at least two TI prescriptions at least 1 year apart. Other requirements for inclusion as a case (Table 1) reduced the number of TI users to 647, for whom control matching was achieved for 627 (Fig. 1). The selection process for the controls (Fig. 1) resulted in 1830 controls who were using RAA insulin for at least 1 year and were matched on the factors noted in Table 1, including index date and time from the index date to the last encounter in the database.
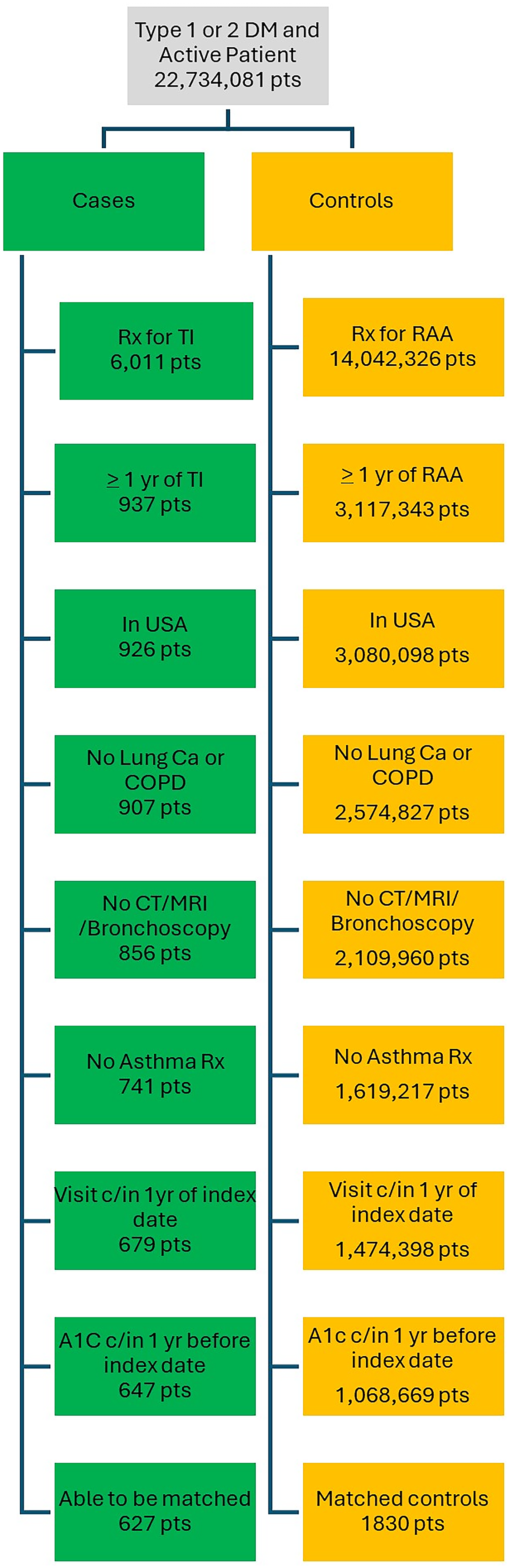
Flow diagram for cohort selection.
Mean age of the cases was 50 years, 41.3% were female, and 77.8% were of the White race. Type 1 diabetes was present in 53.6% and type 2 diabetes in 46.4%; median HbA1c prior to the index date was 7.3%. Characteristics of controls were well matched to the cases (Table 2). With regard to duration of follow-up, median time from the index date to the last encounter of any type in the database was 3.47 years (range −0.81 to 9.80 years, interquartile range 1.99–4.92 years) in the cases and 3.47 years (range −0.96 to 14.94 years, interquartile range 2.13–4.96 years) in the controls. The median duration of TI exposure based on the time between the first and last prescription was 2.21 years (range 1.0–9.7 years, interquartile range 1.4–3.5 years).
Characteristics of Cases and Control
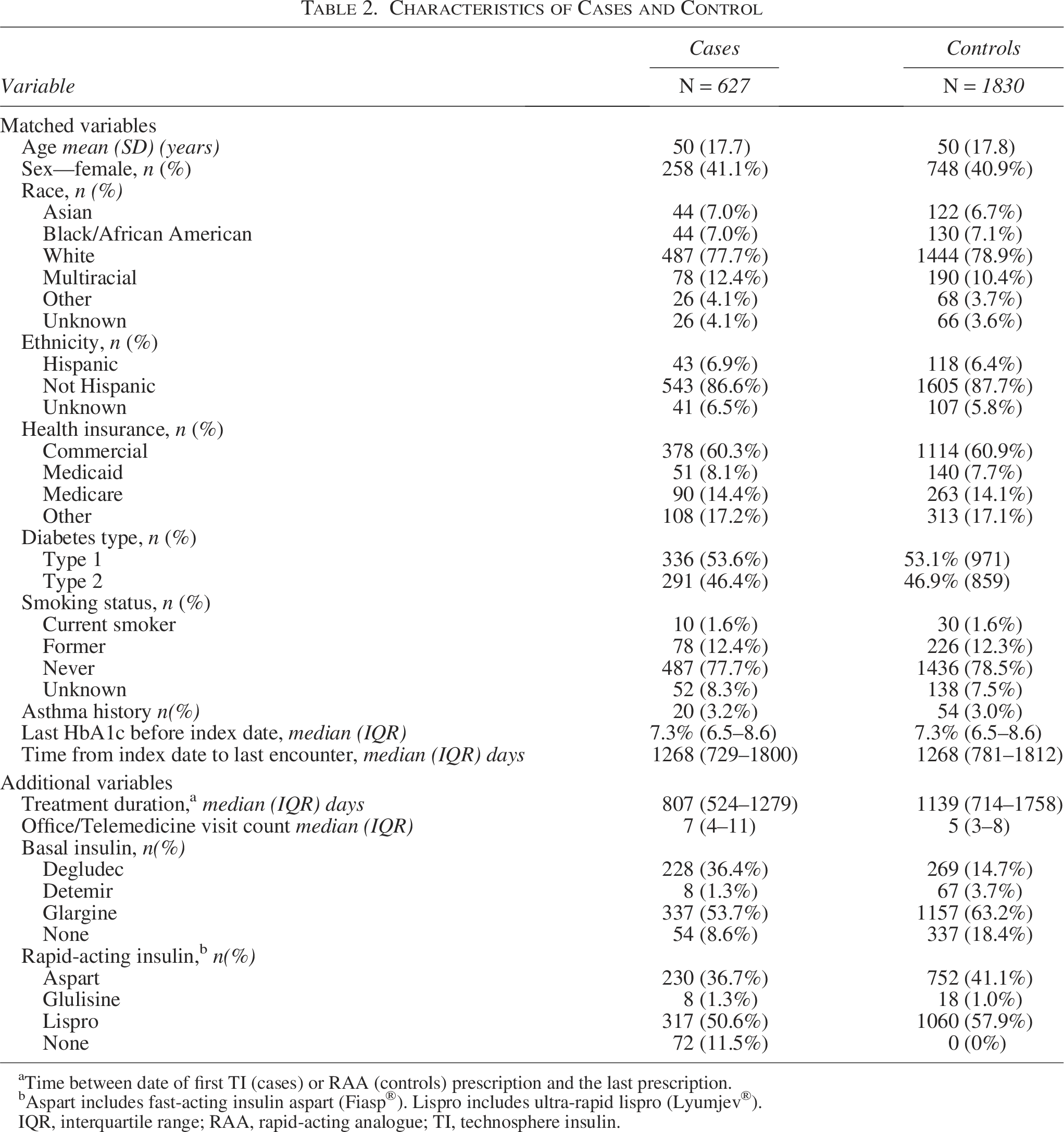
Time between date of first TI (cases) or RAA (controls) prescription and the last prescription.
Aspart includes fast-acting insulin aspart (Fiasp®). Lispro includes ultra-rapid lispro (Lyumjev®).
IQR, interquartile range; RAA, rapid-acting analogue; TI, technosphere insulin.
In the time period beginning 1 year postindex date, a lung cancer diagnosis was recorded in no cases and in two controls (0.11%), while a diagnosis of COPD, emphysema, or chronic bronchitis was recorded in 1 (0.16%) case and in 27 (1.48%) controls (OR = 0.107, 95% CI 0.014–0.787, P = .007).
Discussion
In this study, utilizing the Epic Cosmos RWD database, we did not find an association between the use of inhaled TI and pulmonary toxicity, specifically lung cancer and COPD. There were no cases of lung cancer recorded in the patients exposed to TI, and there were fewer cases of COPD than in controls. These results are supportive of RCTs that have not indicated an association between TI inhalation and pulmonary toxicity. 6 These studies have shown a slight reduction in pulmonary function testing with TI use; however, this reduction reverses after TI is stopped, suggesting that there are no permanent changes in the lung as would be expected with COPD.
Cowart et al 7 evaluated the association of TI with lung cancer and COPD in the TriNetX RWD dataset using a matched case–control design similar to our study. They found no difference between cases and controls in the incidence of lung cancer but did find a higher incidence of COPD in the TI cases than in the matched controls: 41 (1.6%) among 2493 cases versus 12 (0.5%) among 2514 controls (P < 0.001). A potential source of bias that could explain this finding is the guidance in TI’s FDA label to perform pulmonary function testing prior to starting TI, after 6 months, and then yearly. There is no way to know from their analysis how often the COPD diagnosis was made based on pulmonary function testing results. The authors had only aggregate data available for their analyses and thus were unable to adjust for confounding variables, including evaluating the duration of TI exposure at the time of COPD diagnosis or whether the COPD cases were treated. Thus, they were limited in assessing the potential for ascertainment bias to explain their finding. In our study using Cosmos, we had access to anonymized patient-level data to be able to assess the duration of follow-up time and treatments received on an individual patient level.
Not only did we not observe an increase in COPD diagnoses, but we statistically observed a protective effect of TI. As there is no plausible physiological basis for a protective effect, this could be due to chance (even with P value of 0.007) but seems more likely to be due to selection bias. Due to concern about potential pulmonary effects, a patient’s history of pulmonary toxin exposure, including smoking and secondhand smoke, is scrutinized when TI is being considered, and patients also may undergo pulmonary function testing prior to initiating TI, as this is recommended in TI’s FDA labeling. In addition, patients with a prior history of asthma or other pulmonary disease would be less likely to be prescribed TI. Thus, the patients in the database who initiated TI may have been healthier with respect to pulmonary exposures and function than the matched controls and thus at lower risk of having a COPD diagnosis during the follow-up period. As such, this finding underscores the challenges in RWD analyses in which there may be unmeasurable factors that can influence the results.
There are always limitations when using RWD to address a clinically relevant question, as the data were not collected with this purpose in mind. Our study is no exception. In addition to the potential bias manifested as a “protective” effect of TI on COPD, several additional aspects of the study must be considered in interpreting the results. First, despite the size of the Cosmos database with data for over 300 million individuals, the number of TI users meeting criteria to be included in the analysis (N = 647) was relatively small for assessing uncommon outcomes. Second, the latency period for exposure to a pulmonary toxin to cause lung cancer or COPD is typically many years, often decades. Thus, the duration of follow-up in the study after the index date may be too short to fully assess whether TI exposure could be associated with pulmonary toxicity. Third, we required at least 1 year of exposure to inhaled TI based on prescriptions, but in an RWD study such as this, we have no measure of whether TI was actually used or how often it was used.
In summary, this study highlights the power of analyses conducted using large RWD databases, particularly when anonymized individual patient data are available to control for confounding factors, and the study can be designed to minimize potential sources of bias, as is possible with Cosmos. While there are limitations to the interpretation of the results from this study, it is reassuring that there was no increase in pulmonary toxicity using inhaled TI for the treatment of diabetes with respect to lung cancer, COPD, emphysema, and chronic bronchitis.
Authors’ Contributions
T.L.B., I.B.H., and R.W.B. developed the design for the study. T.L.B. performed the analyses. T.L.B., I.B.H., and R.W.B. wrote the article. All authors approved the final version of the article.
Footnotes
Author Disclosure Statement
T.L.B. reports no personal financial disclosures. I.B.H. reports grant funding to his institution from Sequel Med Tech and MannKind and consulting fees from Abbott, Roche, and Hagar. R.W.B. reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding, study supplies, and consulting fees from Insulet and Tandem Diabetes Care; grant funding and study supplies from Dexcom and Abbott; grant funding from Bigfoot Biomedical, Sequel Med Tech, and MannKind; study supplies from Medtronic; consulting fees and study supplies from Novo Nordisk; and consulting fees from BetaBionics, Hagar, DreaMed, Ypsomed, Eli Lilly, and Zucara.
Funding Information
The study was conducted without a funding source.