
Abstract
Continuous glucose monitoring (CGM) technology is becoming increasingly available to people with diabetes using insulin therapy; however, availability for people with type 2 diabetes (T2D) not on insulin remains limited. For people with T2D, there is strong evidence of glycemic benefit with CGM use for those treated with insulin, and CGM is accepted as standard of care. This review explores the impact of CGM use on glycemic and patient-reported outcomes in noninsulin treated populations with T2D, reporting outcomes from 10 identified randomized controlled trials and 15 nonrandomized studies. We report evidence that supports the use of this technology in people with T2D not using insulin.
Keywords
Introduction
Continuous glucose monitoring (CGM) systems have revolutionized diabetes management by providing real-time glucose data with predictive and threshold-based alarms and alerts, enabling better glycemic management and reduction in acute and chronic complications of diabetes. The benefits of CGM are well-documented in individuals with type 2 diabetes (T2D) treated with insulin therapy.1,2 Studies show significant improvements in hemoglobin A1c (HbA1c), increased time in range (TIR), reduced hypoglycemia, decreased health care resource utilization, improved patient-reported outcomes, and significant cost savings with the use of CGM in insulin-treated (IT) people with T2D.1–7 Studies in T2D IT individuals have demonstrated up to a 1.4% reduction in HbA1c, a 15% increase in TIR, and a decrease in emergency room visits and hospitalizations due to severe hypoglycemia and hyperglycemia.3,4,8 CGM initiation in insulin users showed a reduction in per member per month spending by $341 to $424,6,7 as well as improvements in patient quality of life and treatment satisfaction. 9
The weight of evidence supports reductions in HbA1c of 0.4%–0.5% as clinically meaningful10,11 and strongly associated with lower risk of long-term microvascular and macrovascular complications in people with type 1 diabetes (T1D)12,13 or T2D.14,15 In addition, the U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) recognize a ≥ 0.3% change in HbA1c in a randomized controlled trial (RCT) setting as a clinically meaningful difference for evaluating glycemic control interventions.16,17 Therefore, reducing HbA1c is a crucial goal of comprehensive care for people with diabetes. However, it has been estimated that 47% of adults in the United States with diagnosed diabetes had an HbA1c value ≥ 7%, higher than the recommended clinical target, 18 and a substantial amount of people with T2D do not meet their glycemic goals.19–21 Suboptimal glycemic management increases risk of diabetes-related complications 22 and health care costs. 23
Glucose monitoring supports diabetes self-management and can provide information on the effect of diet, physical activity, and medications on glucose levels and patterns. 24 For people with noninsulin treated T2D, self-monitoring of blood glucose (SMBG) has been shown to have very limited effect on glycemic management.25–27 While CGM has demonstrated clear benefits for IT populations, substantial emerging evidence suggests that its advantages can extend to populations with T2D on noninsulin therapy (NIT), with similar trends in improved glycemic outcomes. This body of evidence has contributed to the updated clinical recommendations of the American Diabetes Association (ADA) Standards of Care, specifically recommending the consideration of CGM for adults with T2D treated with medications other than insulin. 25
This literature review explores the impact of CGM use on diabetes-related outcomes in noninsulin treated T2D populations, reviewing RCTs and real-world evidence including nonrandomized observational studies, systematic reviews, and meta-analyses. The literature search was conducted in PubMed to identify relevant studies up to January 31, 2025. Additionally, backward citation tracking of bibliographies from selected articles was performed to capture additional studies.
This report describes the characteristics of study cohorts and the outcomes associated with CGM use, particularly HbA1c, TIR 70–180 mg/dL, and patient-reported outcomes (PROs), extracting baseline and follow-up data and adjusted between-group differences for glycemic outcomes. The findings provide an overview of the evidence base underscoring CGM’s potential to improve glycemic management, thereby reducing diabetes-related complications and supporting lifestyle changes in the noninsulin treated T2D population.
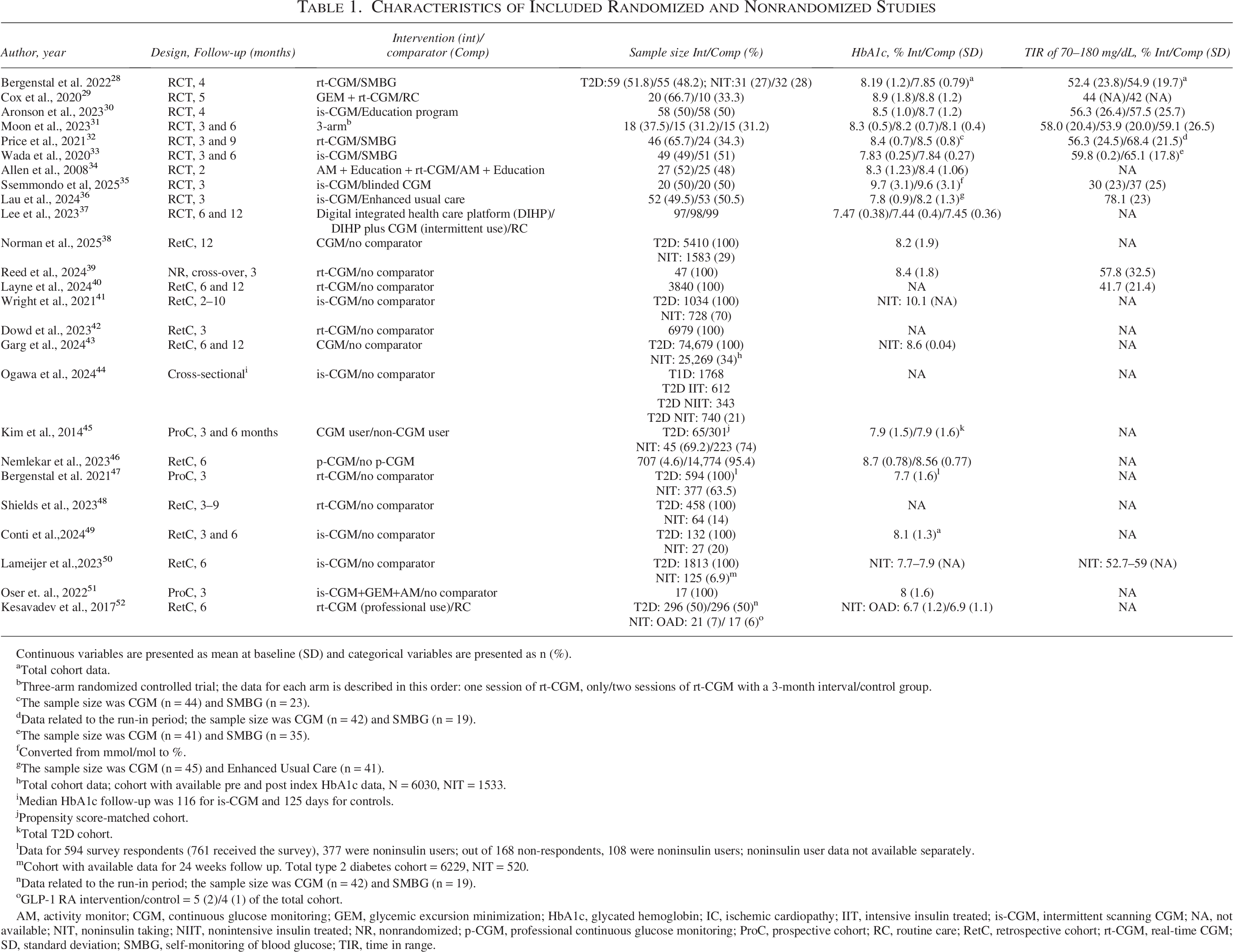
The literature search resulted in 10 RCTs28–37 and 15 nonrandomized observational studies38–52 that reported HbA1c or TIR 70–180 mg/dL as an outcome (Table 1). All 10 of the RCTs reported between-group differences in change in HbA1c ranging from 0.0% to −1.11% (Fig. 1, Table 2). Thirteen of the nonrandomized studies reported a within-group change in HbA1c ranging from −0.50% to −2.00% (Fig. 2). For TIR, 8 RCTs reported a between-group difference in change ranging from 0.54% to 20.2% (Fig. 3), while only three of the nonrandomized studies reported within-group TIR change ranging from 17.30% to 25.0% (Fig. 4). In addition, 14 studies were found in the T2 NIT population that reported on at least one PRO measure (Table 3). Nine of these studies were included in Table 1 (6 RCTs, 3 nonrandomized studies), while 5 studies did not report HbA1c or TIR outcomes.5,53–56
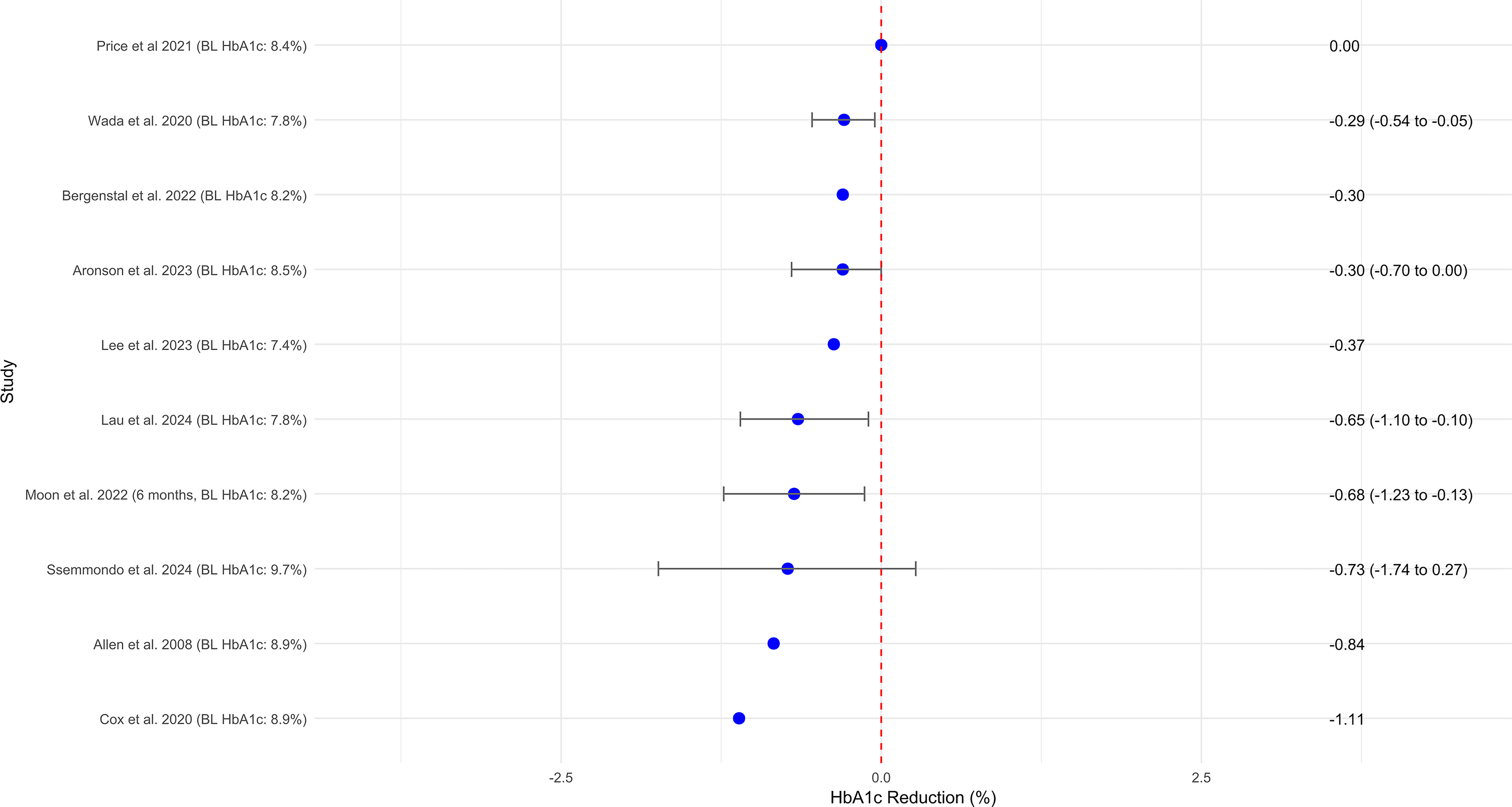
HbA1c change (%) reported in randomized controlled trials (RCTs).
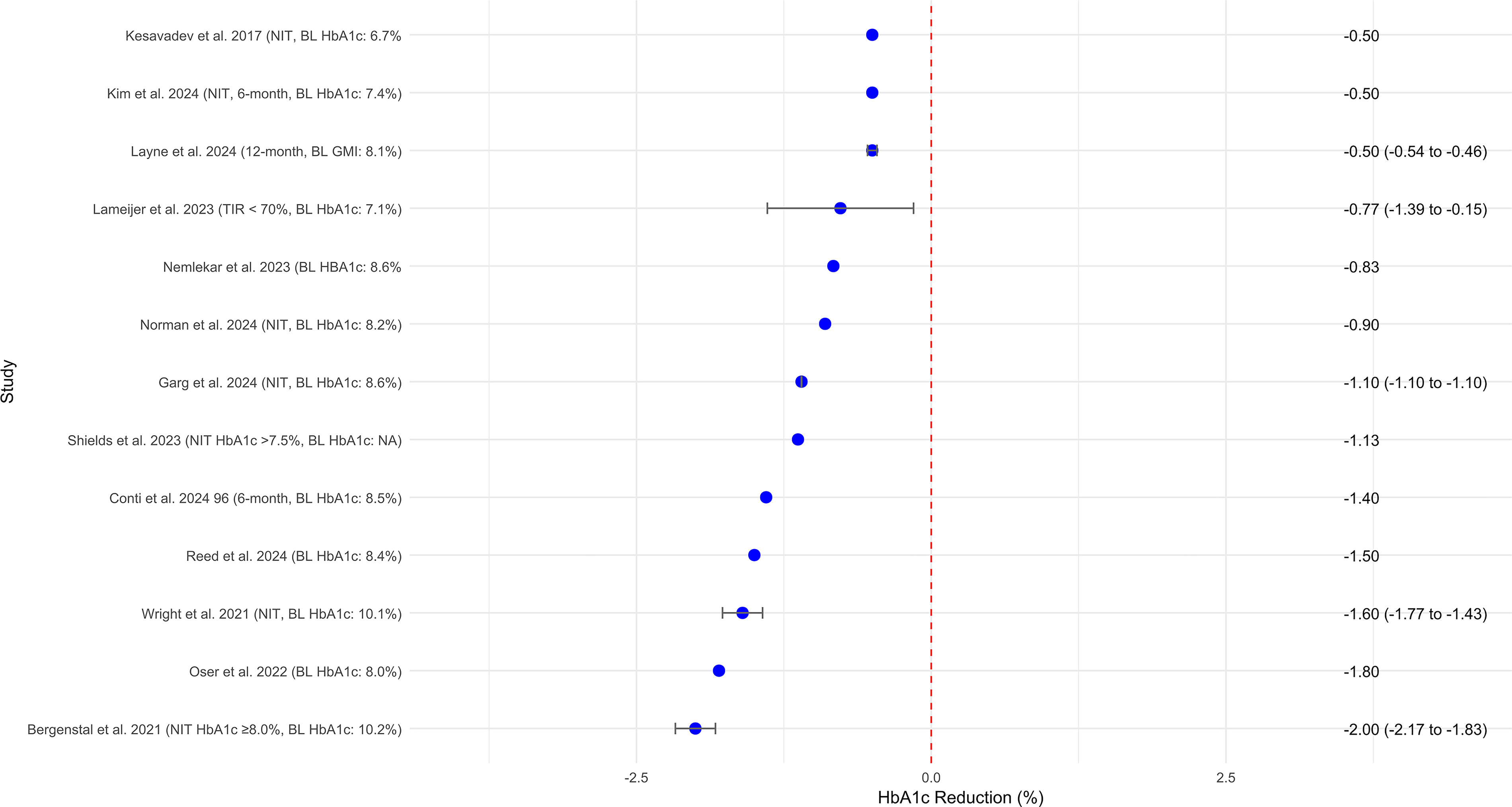
Within-group HbA1c change (%) reported in nonrandomized studies.
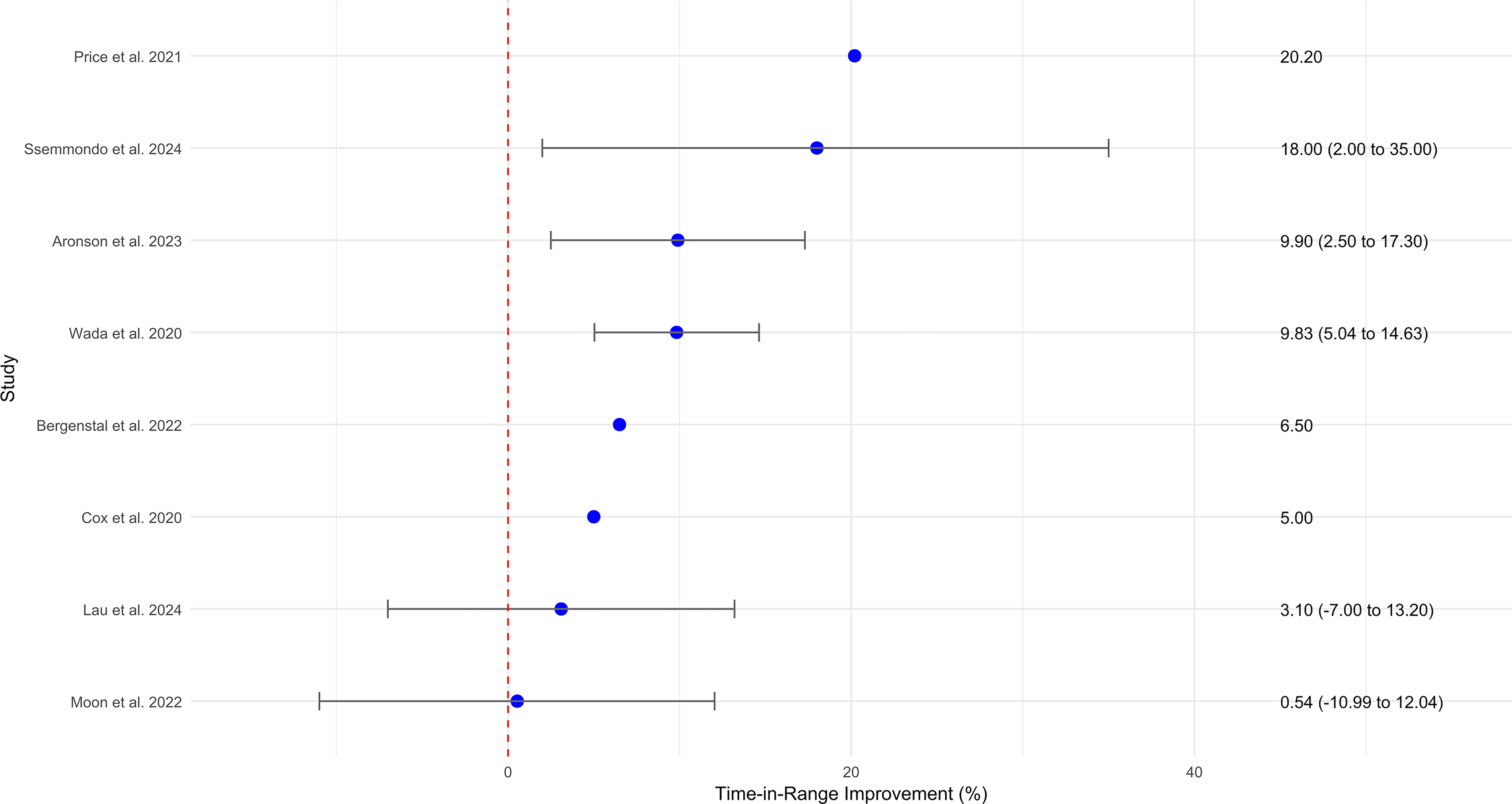
Time in range change (%) reported in randomized controlled trials.
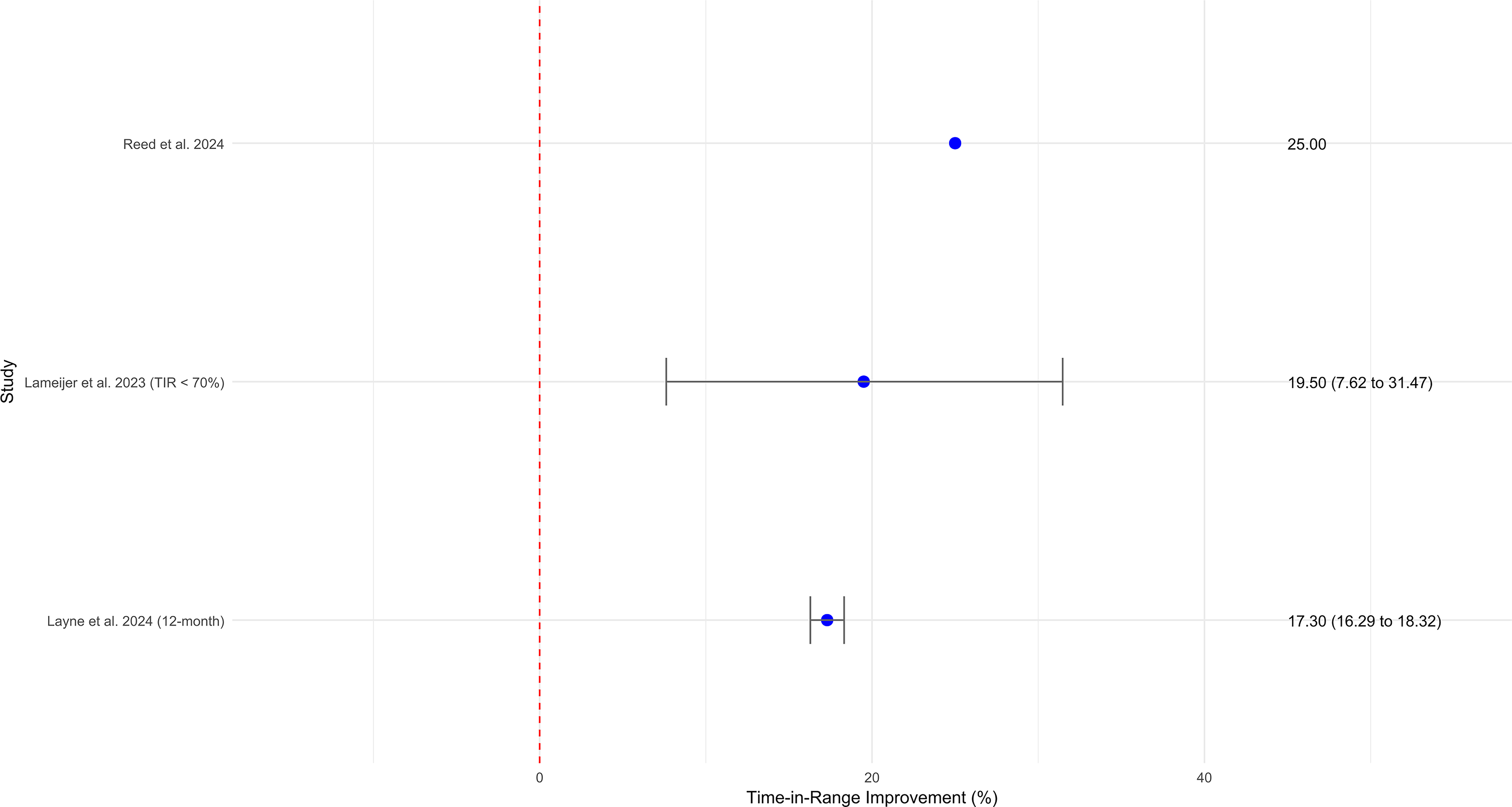
Within-group time in range change (%) reported in nonrandomized studies.
Characteristics of Included Randomized and Nonrandomized Studies
Continuous variables are presented as mean at baseline (SD) and categorical variables are presented as n (%).
aTotal cohort data.
bThree-arm randomized controlled trial; the data for each arm is described in this order: one session of rt-CGM, only/two sessions of rt-CGM with a 3-month interval/control group.
cThe sample size was CGM (n = 44) and SMBG (n = 23).
dData related to the run-in period; the sample size was CGM (n = 42) and SMBG (n = 19).
eThe sample size was CGM (n = 41) and SMBG (n = 35).
fConverted from mmol/mol to %.
gThe sample size was CGM (n = 45) and Enhanced Usual Care (n = 41).
hTotal cohort data; cohort with available pre and post index HbA1c data, N = 6030, NIT = 1533.
iMedian HbA1c follow-up was 116 for is-CGM and 125 days for controls.
jPropensity score-matched cohort.
kTotal T2D cohort.
lData for 594 survey respondents (761 received the survey), 377 were noninsulin users; out of 168 non-respondents, 108 were noninsulin users; noninsulin user data not available separately.
mCohort with available data for 24 weeks follow up. Total type 2 diabetes cohort = 6229, NIT = 520.
nData related to the run-in period; the sample size was CGM (n = 42) and SMBG (n = 19).
oGLP-1 RA intervention/control = 5 (2)/4 (1) of the total cohort.
AM, activity monitor; CGM, continuous glucose monitoring; GEM, glycemic excursion minimization; HbA1c, glycated hemoglobin; IC, ischemic cardiopathy; IIT, intensive insulin treated; is-CGM, intermittent scanning CGM; NA, not available; NIT, noninsulin taking; NIIT, nonintensive insulin treated; NR, nonrandomized; p-CGM, professional continuous glucose monitoring; ProC, prospective cohort; RC, routine care; RetC, retrospective cohort; rt-CGM, real-time CGM; SD, standard deviation; SMBG, self-monitoring of blood glucose; TIR, time in range.
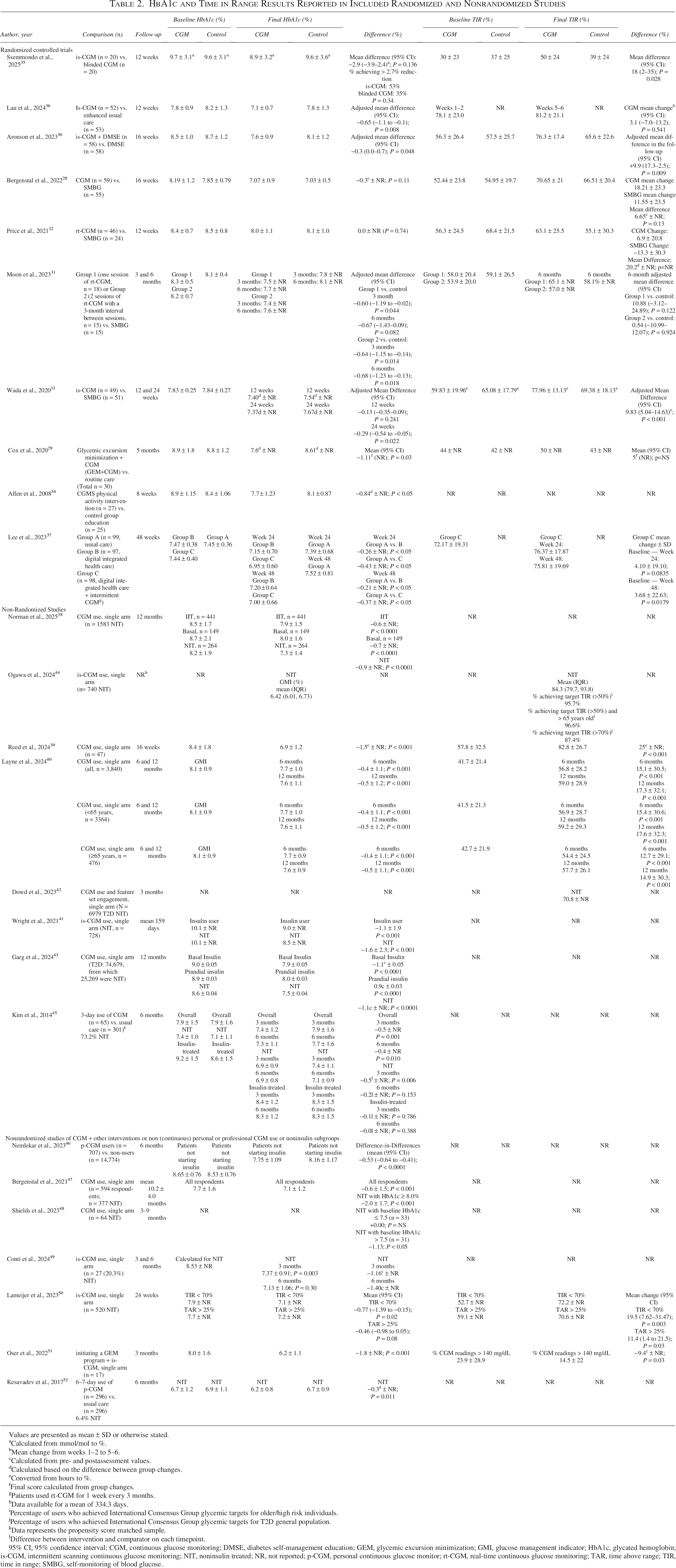
HbA1c and Time in Range Results Reported in Included Randomized and Nonrandomized Studies
Values are presented as mean ± SD or otherwise stated.
Calculated from mmol/mol to %.
Mean change from weeks 1–2 to 5–6.
Calculated from pre- and postassessment values.
Calculated based on the difference between group changes.
Converted from hours to %.
Final score calculated from group changes.
Patients used rt-CGM for 1 week every 3 months.
Data available for a mean of 334.3 days.
Percentage of users who achieved International Consensus Group glycemic targets for older/high risk individuals.
Percentage of users who achieved International Consensus Group glycemic targets for T2D general population.
Data represents the propensity score matched sample.
Difference between intervention and comparator on each timepoint.
95% CI, 95% confidence interval; CGM, continuous glucose monitoring; DMSE, diabetes self-management education; GEM, glycemic excursion minimization; GMI, glucose management indicator; HbA1c, glycated hemoglobin; is-CGM, intermittent scanning continuous glucose monitoring; NIT, noninsulin treated; NR, not reported; p-CGM, personal continuous glucose monitor; rt-CGM, real-time continuous glucose monitoring; TAR, time above range; TIR, time in range; SMBG, self-monitoring of blood glucose.
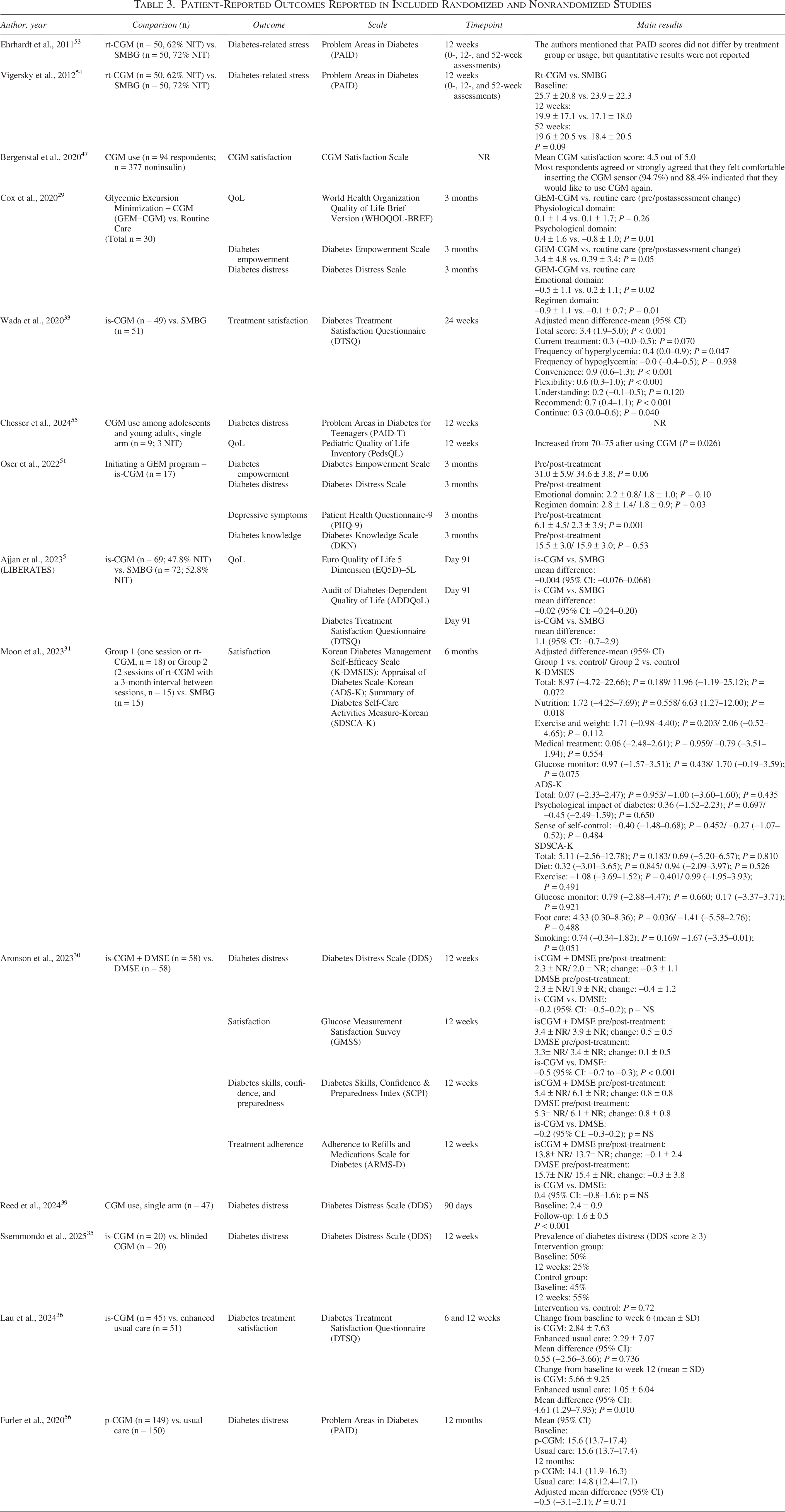
Patient-Reported Outcomes Reported in Included Randomized and Nonrandomized Studies
Study Population Characteristics
This literature search identified 10 RCTs, 9 of which recruited 100% of participants managed with NIT29–37 (one study included a mixed population but reported outcomes for NIT individuals separately 28 ), and 15 nonrandomized studies (Table 1).38–52 The RCTs reported diabetes durations ranging from 5.4 to 13.9 years29–33,35,36 and the nonrandomized studies reported durations ranging from 9 to 19 years,40,45,49,52 with one study focused on newly diagnosed participants. 51 All RCTs reported mean body mass index (BMI) values greater than 25 kg/m2, and seven RCTs28–30,32,34–36 along with three nonrandomized studies39,47,51 reported mean BMI values exceeding 30 kg/m2. Types of noninsulin therapies were reported in only five RCTs28,30,32,35,36 and eight nonrandomized studies.39,41,43,45–47,49,52 Among these, metformin was the most used agent, with prevalence ranging from 61% to 100%, followed by sulfonylureas, sodium-glucose cotransporter-2 inhibitors, and dipeptidyl peptidase-4 inhibitors. Glucagon-like peptide-1 receptor agonist use was reported in 12.5%–35% of RCTs and 1%–51% of nonrandomized study participants. All RCTs reported baseline HbA1c levels above 8.0%, except for a study by Wada et al., which reported a slightly lower baseline HbA1c of 7.83%, 33 and Lau et al., 2024, with a baseline HbA1c of 7.8% in the CGM group. 36 Baseline HbA1c levels were reported in 11 nonrandomized studies and ranged from 6.7% to 10.8%.
Impact of CGM on HbA1c
Results from the RCTs of CGM use versus nonuse showed statistically significant between-group HbA1c reductions ranging from 0.29% to 1.11% (Table 2; Fig. 1).28–31,33,34,36,37 A recent systematic review and meta-analysis estimated the effect size of HbA1c change across 6 of the 10 identified studies and reported a pooled effect size of −0.31% (95% CI: −0.21 to −0.42), favoring CGM (Table 4). 57 Another systematic review 58 that evaluated the effects of intermittently-scanned CGM (isCGM) on glycemic control estimated the effect size of HbA1c change for the entire T2D cohort and provided a subgroup analysis for the NIT users, which showed a pooled effect size of −1.03% (95% CI: −1.55 to −0.50), favoring CGM in that subgroup. Among the 10 identified RCTs, only three did not show a statistically significant reduction in average HbA1c between groups, two of which used nonstandard study designs.28,32,35 However, in one of the studies, the proportion of patients achieving HbA1c <7.5% in the CGM group was double that of the control group (34.1% vs. 17%). 32 Another trial used a more frequent and systematic SMBG testing schedule in the control group 28 than would be expected with standard care. The third trial, which compared isCGM with blinded CGM and included only 20 participants per group, reported clinically meaningful improvements in glycemic outcomes, including an 8 mmol/mol (∼0.73%) reduction in HbA1c and an 18% increase in TIR. 35
HbA1c and Time in Range Results Reported in the Included Systematic Review and Meta-Analysis
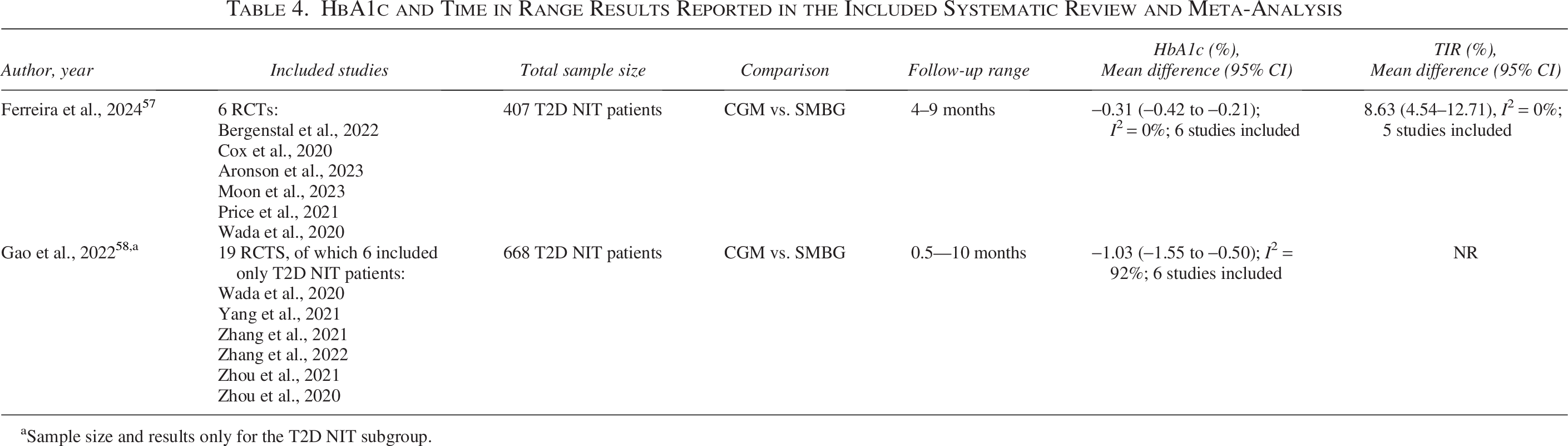
Sample size and results only for the T2D NIT subgroup.
Real-world, single-arm evidence studies corroborate the RCT evidence and show meaningful reductions in HbA1c compared with baseline, ranging from 0.4% to 2.3% (Table 2; Fig. 2). In addition, retrospective studies highlight that individuals with T2D on NIT using CGM often achieve greater HbA1c reductions than those treated with insulin.38,43,45,47,48 Wright et al., 2021, 41 explored glycemic outcomes among participants with T2D managed with basal insulin or NIT. Both groups showed a significant reduction in HbA1c; however, the reduction in the NIT group was greater than in the basal IT group (1.6% vs. 1.1%). 41 Garg et al., 2024, using OPTUM Market Clarity data, reported that people treated with NIT achieved greater HbA1c reductions compared with those treated with prandial insulin (1.1% vs. 0.9%) despite having lower baseline HbA1c levels (8.6% vs. 9.0%). 43 Norman et al., 2025, examined HbA1c changes using Aetna’s administrative claims data, including commercially-insured and Medicare Advantage beneficiaries, and found that T2D NIT individuals had a greater drop in HbA1c (0.9%) compared with T2D on intensive insulin (0.5%) and nonintensive insulin (0.7%). 38 In a retrospective analysis using electronic health records and administrative claims, Shields et al., 2023, reported a 1.13% reduction in HbA1c among NIT individuals compared with a 0.76% reduction in individuals on intensive insulin therapy. 48 In a prospective cohort that compared Korean CGM users versus nonusers, Kim et al., 2014, reported a −0.5% difference in HbA1c at 3 months and −0.2% at 6 months in the NIT subgroup, favoring the CGM group (P = 0.006 and P = 0.153, respectively). On the other hand, no significant difference was observed among insulin users at 3 or 6 months. 45 The benefit of CGM use was also demonstrated in high-risk populations, such as those with atherosclerotic cardiovascular disease (ASCVD). Reed et al., 2024, evaluated the impact of CGM use in patients at high risk for cardiovascular disease, 48.9% of whom had existing ASCVD and reported a significant reduction in HbA1c of 1.5% and a decrease of approximately 8% in the absolute 10-year predicted risk for ASCVD. 39
One study reported change in glucose management indicator (GMI) rather than laboratory-measured HbA1c.40,55 GMI is calculated from mean glucose values obtained through CGM. GMI was developed as an estimate intended to reflect average glycemia over time, offering a CGM-based metric that correlates with, but does not replace, HbA1c. 59 While this study did not capture laboratory HbA1c values, the observed reduction in GMI reflected sustained improvement in long-term glycemic control and underscored CGM’s value in NIT individuals where conventional laboratory measures may not have been collected.
These findings reflect the difference in disease states between people treated with insulin and those treated with NIT. Patients on intensive insulin therapy often have more advanced disease, characterized by greater insulin resistance and deficiency. 60 In such cases, treatment targets may differ, particularly due to the heightened risk of hypoglycemia, the presence of comorbidities, and the need for less aggressive glycemic goals compared with NIT individuals.24,61 By contrast, NIT patients often exhibit less advanced disease with greater residual beta-cell function, enabling more substantial HbA1c reductions with interventions like CGM. 60 This highlights the potential value of initiating CGM earlier in the disease course, particularly in individuals treated with NIT, to optimize glycemic management before the disease progresses. Early use of CGM may help avert the trajectory toward greater disease severity and improve long-term outcomes by addressing glycemic variability and associated complications at a more manageable stage.15,62
It is well established that baseline HbA1c is an important predictor of the treatment effect of glucose lowering therapies with attenuated reductions in HbA1c at lower baseline levels. 63 This relationship has also been found for CGM among people with T1D64,65 and in a post hoc analysis of the DIAMOND study for people with T1D or T2D using multiple daily injections of insulin. 8 Thus, change in HbA1c should be evaluated relative to baseline levels.
Figure 5 shows an inverse relationship between the within-group changes in HbA1c and baseline HbA1c for the RCT and nonrandomized studies. While not statistically significant for the 22 studies, the overall relationship had a correlation of r = −0.35 (P = 0.12). The correlation was somewhat stronger when RCTs (r = −0.48; P = 0.23) and nonrandomized studies (r = −0.43; P = 0.18) were considered separately. The magnitude of these relationships is similar to that reported by Bloomgarden and colleagues (R2 = 0.18, which equals an r = 0.42). 63 As seen in Figure 3, while higher baseline HbA1c tended to be related to greater HbA1c reductions, overall clinically meaningful within-group changes in HbA1c were observed across the range of initial HbA1c levels. This finding suggests people with T2D NIT can benefit from CGM regardless of their level of glycemic control prior to starting CGM, likely from feedback on how medications, diet, and physical activity affect their glucose levels.
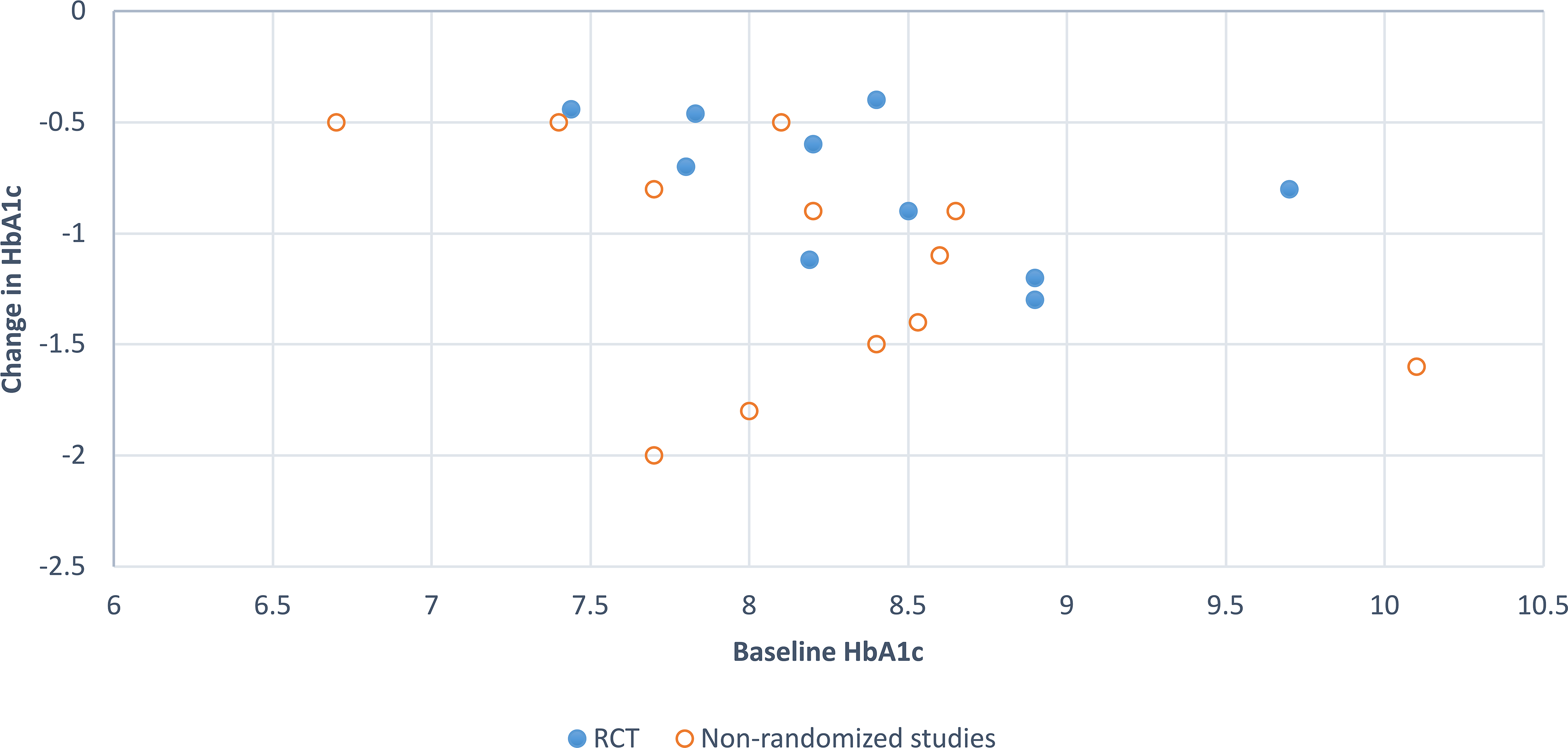
Change in HbA1c by baseline HbA1c in RCTs and nonrandomized studies.
Impact of CGM on TIR between 70 and 180 mg/dL
Findings from 8 of the 10 RCTs compared TIR 70–180 mg/dL between the treatment and comparator study arms and 6 studies showed a clinically meaningful increase (i.e., ≥ 5.0%), favoring CGM among people with T2D who are not managed with insulin therapy, which was sustained for up to 6 months (Table 2; Fig. 3).28–33,35,36 In some studies, the CGM group had improved TIR, while the control group had a decreased31,32 or only slightly increased TIR.28–30,33,35 All studies, however, demonstrated favorable results for the CGM group. Between-group differences in change in TIR did not seem to depend on length of follow-up, with effects ranging from 3.1% to 20.2% at 12 weeks,32,35,36 6.5% to 9.9% at 16 weeks,28,30 and 0.54% to 9.8% at 20–24 weeks.29,31,33 The meta-analysis by Ferreira et al., 2024, 57 evaluated the impact of CGM on TIR and estimated the effect size by pooling data from 5 of the 8 RCTs identified in the current study and reported a pooled effect size of 8.63% (95% CI: 4.54–12.71), favoring the CGM group (Table 4).29–33
Of the eight RCTs that included HbA1c and TIR as outcomes, the correlation between decreased HbA1c and increased TIR was positive (r = 0.49, P = 0.22), where smaller reductions in HbA1c related to larger improvements in TIR, which is not the expected direction (Fig. 6). This may be a spurious finding given it is based on only eight studies. Additional studies that measure change in HbA1c and TIR would help to clarify the relationship between these measures of glycemic control among the T2 NIT population.
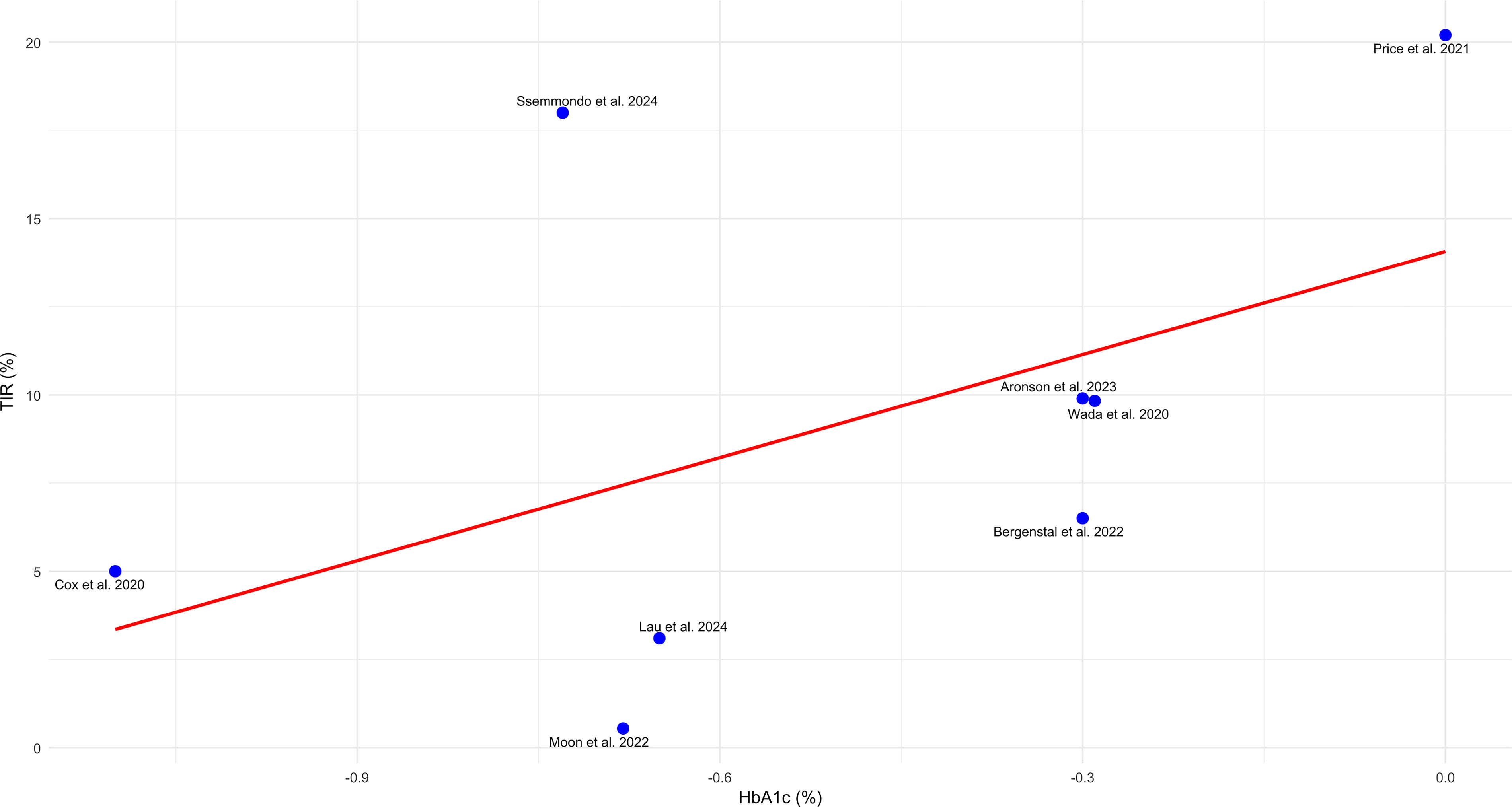
Relationship between change in HbA1c and change in time in range (TIR).
Five of the 15 nonrandomized studies reported significant improvements in TIR in up to 12 months among CGM users (Table 2) with three studies reporting mean TIR 70–180 mg/dL at baseline and follow-up (Fig. 4).39,40,44,50,51 In a retrospective study that used anonymized data from Dexcom users, a significant increase in TIR was observed in 6 and 12 months (15.1% and 17.3%, both P < 0.001). The results were consistent across different age groups (adults < 65 and ≥ 65 years old). 40 Other single-arm intervention studies also investigated the effects of CGM on TIR. One single-arm study reported an increase of 25% in TIR in 16 weeks with the use of CGM. 39 In line with these results, another single-arm study found significant improvements in this metric for participants who started CGM with a suboptimal glycemic management (i.e., TIR < 70% or time above range [TAR] > 25%) with mean change of 19.5% (P = 0.003) in TIR at 24 weeks. 50 One study investigated the effects of initiating a glucose excursion minimization program associated with the use of CGM and observed a significant reduction in CGM readings > 140 mg/dL (calculated difference = −9.4; P = 0.03). 51 Finally, a retrospective single-arm study with approximately 11 months of data available reported that 95.7% and 96.6% of all NIT patients and NIT > 65 years old, respectively, achieved TIR > 50%, while 87.4% of all NIT patients achieved the target TIR > 70%. 44
Impact of CGM on Quality of Life
Several studies have assessed PROs, such as quality of life (QoL),5,29,55 diabetes-related stress,53,54 diabetes distress,29,30,35,39,51,56 diabetes empowerment,29,51 satisfaction or treatment satisfaction,5,30,31,33,36,47 depressive symptoms, 51 diabetes knowledge, 51 and diabetes skills, confidence, and preparedness. 30 The studies that evaluated these outcomes are presented in Table 3. Overall, a trend toward improvement in diabetes empowerment,29,51 diabetes-related stress,35,53,54,56 and diabetes skills, confidence, and preparedness 30 was observed for CGM patients. Most studies that assessed treatment satisfaction reported significant improvement.5,30,33,36,47 Regarding QoL, mixed results were observed. In studies that included adults, no significant difference was observed between CGM and control groups, except for the psychological domain, evaluated by the World Health Organization Quality of Life tool, where a significant improvement was observed in the CGM group compared with routine care.5,29 One study that assessed QoL in teenagers and young adults reported a significant improvement in QoL after initiating CGM. 55 There was a trend toward an overall reduction in diabetes distress and a significant reduction in the regimen domain, while mixed results were observed for the emotional domain.29,30,39,51 Reduction in depressive symptoms was reported by patients in the CGM treatment arm. 51
Conclusion
Randomized trials and real-world evidence studies demonstrate that CGM use is associated with significant reductions in HbA1c and improvements in TIR in people with noninsulin treated T2D. The identified studies reported outcomes in people with diabetes durations ranging from 5 to 19 years, BMI greater than 25 kg/m2, varying usage of noninsulin medications, and suboptimal HbA1c levels, demonstrating that these studies collectively are indicative of the heterogeneous T2D NIT population. Among noninsulin treated populations, clinically meaningful HbA1c reductions among RCTs ranged from 0.29% to 1.15%, with consistent advantages for CGM users over SMBG users. Meta-analyses support these findings, with pooled HbA1c reductions exceeding the FDA and EMA threshold for clinical significance.57,58 Nonrandomized real-world studies showed additional significant reductions, ranging from 0.50% to 2.0%. Across real-world evidence studies, NIT cohorts consistently achieved larger HbA1c reductions than insulin users, likely due to less advanced disease and fewer glycemic constraints.
The 2023 international consensus statement published by Battelino et al. supported by Level B evidence according to the 2025 ADA Standards of Medical Care in Diabetes evidence-grading system, defines an absolute increase of ≥ 5% as constituting a clinically meaningful improvement in TIR in clinical trials for an individual participant, while a 3% increase is significant for treatment-group differences in mean TIR. 66 In this literature review, pooled analysis of RCTs reported an average increase in TIR of nearly 9%, with some nonrandomized studies reporting increases of up to 25%, with TIR improvements maintained over 12 months. Taken together, these results suggest that benefits from CGM use are sustainable in NIT-treated cohorts. However, it is important to note that none of the studies included in this review have follow-up points exceeding 12 months. Only two of the RCTs had a follow-up past 6 months,32,37 and four of the nonrandomized studies had a follow-up at 12 months.38,40,41,43 Following people with T2 NIT for longer durations will help further elucidate the long-term benefits of CGM for this population. Additional work is also needed to evaluate the benefits of CGM use in vulnerable populations within the T2D community, in particular pregnant women 67 and youth (age < 21 years), 68 among whom T2D prevalence is increasing. While CGM use may play an important role in diabetes management in these populations, to date there has been limited research published.67,69
The observed improvements in TIR are notable considering the longitudinal evidence of strong correlation between TIR and diabetes-related micro- and macrovascular outcomes. One longitudinal study showed that each 5% decrease in TIR was associated with significant increases in the odds of developing diabetic retinopathy. 70 There is also other evidence showing that each 10% decrease in TIR was associated with a 5% increase in cardiovascular disease-related mortality and an 8% increase in all-cause mortality. 71
In addition to glycemic outcomes, CGM demonstrated positive trends in PROs, such as QoL, diabetes-related stress, and treatment satisfaction. While results for QoL were mixed in adult populations, significant improvements were noted in younger cohorts and psychological and diabetes-related distress domains. Enhanced diabetes empowerment, confidence, and preparedness were also reported, reflecting CGM’s broader impact on mental well-being.
These findings highlight CGM’s role as a comprehensive tool for improving glycemic management and enhancing the overall QoL for individuals with T2D treated with NIT. Emerging evidence demonstrates the power of glucose monitoring with real-time feedback to promote lifestyle changes that improve glycemia. 72 The access to abundant glucose data gives providers unprecedented ability to personalize goals and lifestyle advice to manage glucose levels, an ability that has eluded health care systems for decades. CGM has demonstrated value in noninsulin treated cohorts with suboptimal glucose management and various lengths of diabetes duration. CGM systems have an excellent safety record3,73 and there is growing evidence of their cost-effectiveness.74–76
The evidence continues to grow supporting CGM use as the standard of care for people with T2D. The magnitude of improvements in HbA1c and TIR reported in both clinical trials and real-world use indicate that noninsulin-treated populations can benefit from CGM even in this early stage of the diabetes treatment paradigm.
Authors’ Contributions
H.A., G.J.N., and G.A. conceived and designed the literature review with input from J.B.M., R.G., A.L.C., D.K., G.U., and C.J.L. Analysis of the outcomes in the literature was conducted by H.A., S.I., and J.Y.M. G.J.N. and H.A. produced the first draft. All authors reviewed, edited, and approved the final version of the article. G.J.N. is the guarantor of this work and, as such, takes responsibility for the integrity of this literature review.
Footnotes
Acknowledgments
Medical writing services and article submission support were provided by Sarah B. Andrade, MPH, an employee of Dexcom.
Author Disclosure Statement
G.N., H.A., J.M., and S.I. are employees of Dexcom. G.A. has served as advisor for Eli Lilly, Medscape, and Tandem Diabetes Care; G.A. has received consultant fees from Dexcom and Insulet. G.A.’s employer, Northwestern University, has received research support from Abbvie, Bayer, Fractyl Health, Insulet, MannKind, and Tandem Diabetes Care. A.L.C.’s institution receives consulting and/or research support from: Abbott Diabetes Care, Dexcom, Medtronic, Insulet, Tandem, Mannkind, Novo Nordisk, Eli Lilly, Zealand, and Luna Diabetes. J.B.M. has received research support from NIH, Breakthrough T1D, Biomea, Diamyd, and Novo Nordisk. J.B.M. has served as an advisor for Bayer, Eli Lilly, MannKind, and Novo Nordisk. D.F.K. served as advisor for Dexcom, Abbott, Eli Lilly, Novo Nordisk, MannKind, Corcept, Sequel, Insulet, and CeQuer; Speaker for Eli Lilly, Novo Nordisk, Dexcom, Abbott, Insulet, Tandem Diabetes Care, Sequel, Cequr, Corcept; research funding from Tandem Diabetes Care, Insulet, Sequel, Abbott Diabetes Care. C.J.L. has served as an advisor for Dexcom, Tandem Diabetes Care, and Eli Lilly, and has received research support from NIH, Helmsley Foundation, Breakthrough T1D, Abbott, DEKA/TWIIST, Dexcom, Insulet, Tandem Diabetes Care, and MannKind. G.U. has received research support through Emory University from Abbott, Dexcom, Corcept, and Bayer and has served as a member of advisory boards for Dexcom, Corcept, Glucotrack, and GlyCare.
Funding Information
No funding was received for this article.