
Abstract
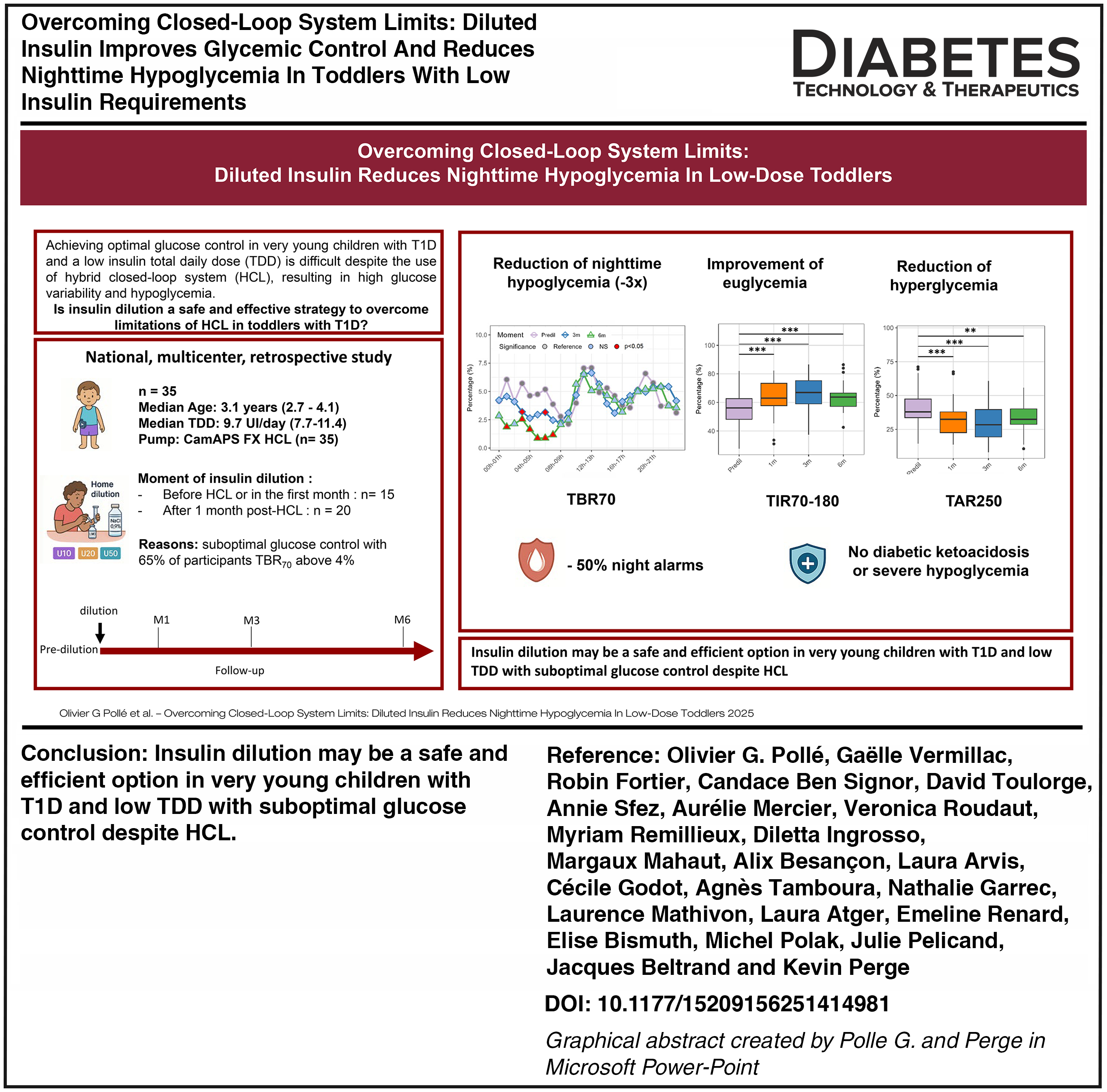
Background and aim:
Very young children with type 1 diabetes (T1D) and low total daily dose (TDD) struggle to achieve optimal glucose control despite hybrid closed-loop (HCL) system. The aim of the study was to evaluate the impact of diluted insulin on glucose control in a real-world setting.
Methods:
This retrospective multicentric French study included 35 children with T1D (below 6 years of age) using CamAPS FX HCL system. Participants were transitioned from U100 insulin to a diluted formulation (U10, U20, or U50). Clinical and continuous glucose monitoring (CGM) data were collected before (predilution) and at 1, 3, and 6 months postdilution. Comparisons between predilution and each postdilution period were performed using linear mixed models.
Results:
Participants had a median TDD of 9.7 (7.7–11.4) UI/day before dilution and a suboptimal glucose control. Insulin dilution was associated with a reduction of time below range (TBR70), glucose variability (coefficient of variation) and pump alarms during the night, with TBR70 decreasing by 3-fold between 4 to 7AM. Transition to diluted insulin led to a significant increase of time in range (TIR70–180) and a decrease of time above range (TAR180) by, respectively, 1.5 h and 1 h per day. These results were observed independently of the time of dilution. No episodes of severe hypoglycemia or ketoacidosis occurred during the follow-up.
Conclusions:
In very young children with T1D and low TDD who are exhibiting suboptimal glucose control despite HCL, insulin dilution may be a safe and efficient option.
Introduction
Type 1 diabetes (T1D) is increasing among children under the age of 5 years of age.1,2 Maintaining adequate glucose control and preventing hypoglycemia in very young children is critical as the onset of T1D during early childhood is associated with increased morbidity and mortality compared to onset later in life. 2 The management of T1D in very young children presents both metabolic and psychosocial challenges for the family and the health care team. 2 Achieving optimal glucose control in this age group is particularly demanding due to highly variable insulin requirements and unpredictable behaviors such as eating and activity.2–4
Hybrid closed-loop (HCL) systems have improved glycemic outcomes and the quality of life in this population.5–19 Nevertheless, current HCL algorithms are challenged by physiological and clinical specificities of the very young children with T1D. 2 Consequently, improvement in time in range (TIR70–180 mg/dL) remains limited as compared with older participants. 20 The lack of precision in delivering very small insulin doses, often below the minimum required in most HCL systems (i.e., 5–8 units daily), contributes to the difficulty in reducing glucose variability and the high incidence of hypoglycemic episodes observed in this population.5–19
Diluted insulin through continuous subcutaneous insulin infusion offers a promising solution to overcome minimal insulin dose challenges, as it appears safe and allows more accurate adjustments.21–23 Nevertheless, only a single system coupled with HCL currently allows the use of diluted insulin. Some case series using insulin pumps reported a reduction of nocturnal hypoglycemia episodes, a decrease of insulin absorption variability and improved HbA1c levels while others did not find significant modification of glucose control. 24 Data on toddlers using diluted insulin in HCL system are even poorer with only few case series and a single randomized clinical trial with participants having a total daily dose (TDD) above 10UI per day.25–32
Our study aims to determine whether transition to diluted insulin in very young children with T1D using CamAPS FX HCL system improved glycemic control.
Methods
Study design and participants
This study was designed as a national, multicenter, retrospective investigation involving 12 expert French pediatric diabetes centers (including five university centers: Lyon, Paris, Nice, Nancy, Dijon; and seven nonuniversity centers: Marne-la vallée, Beauvais, Fontainebleau, Villefranche-sur-Saône, Rochefort, Meaux, Gonesse), with the aim of evaluating the use of the HCL system with diluted insulin in very young children with T1D. Data were collected between October 2023 and June 2025. The analysis focused on the mylife YpsoPump (Ypsomed, Switzerland) combined with CamAPS FX (CamDiab, U.K.), as the system was the only HCL approved for children < 6 years in France at the time of data collection. The study protocol was approved by the ethical committee of Necker Enfants-Malades (number NCK-2024-R-151). In accordance with the prevailing French regulations, parents were informed of the study by post or mail, and were granted the option to decline participation. The database was declared to the National Data Protection Commission (Commission Nationale de l’Informatique et des Libertés, CNIL) and registered according to the MR004 protocol.
Very young children transitioned from U100 insulin to a manual diluted formulation. Insulin U100 Aspart (NovoNordisk, Denmark) was diluted in glass reservoirs with saline solution as follows: U10 (0.2 mL of U100 insulin and 1.8 mL of saline), U20 (0.4 mL of U100 insulin and 1.6 mL of saline) and U50 (1 mL of U100 insulin and 1 mL of saline). All centers followed a training and advice from an expert center (i.e., Lyon-HFME Hospital or Paris-Necker Hospital), which contributed to harmonizing clinical approaches. Reasons of physicians for transitioning the participant to diluted insulin were collected by questionnaire. Participants were classified in two groups according to the timing of HCL initiation at the moment of insulin dilution with respectively ≥ 1 month (i.e., late transition) or < 1 month (i.e., early transition). Regular follow-up by their diabetes team was continued after dilution. The diagnosis of T1D was made according to the International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines with at least one autoantibody described in the medical record. Exclusion criteria included dilution before initiation of HCL system, use of other HCL systems, duration of diabetes below 3 months or intermittent dilutions.
Prior to dilution (i.e., predilution), an array of demographic data (age, sex, diabetes duration, anthropometrics, age at diabetes onset, age at HCL initiation), clinical data (TDD, glycated hemoglobin [HbA1c]) and raw continuous glucose monitoring (CGM) data were collected. From the dilution visit, similar data and pump settings (i.e., glucose targets, glucose ratios, TDD including percentage of basal and bolus insulin) were collected at initiation (15 days) and 1-, 3-, and 6 months postdilution, using a standardized protocol applied across all centers. Episodes of severe hypoglycemia (SH) and diabetic ketoacidosis (DKA) were collected before and after dilution.
CGM data
CGM data including glycemic values and alarms were retrieved from Glooko XT® over a 15-day period before dilution (i.e., Pre-dil), directly after dilution (i.e., initiation) and at each subsequent visit (1, 3, and 6 months) using a standardized protocol applied across all centers. All participants were on Dexcom G6® (Dexcom, CA, USA). Data were first manually checked and retained when ≥75% of CGM values and ≥80% closed-loop use were available. CGM data were processed using R software (version 4.4.5) and analyzed by the same investigator (O.P.). First, they were aggregated using cgmanalysis package and quality-checked using Iglu statistical package. A total of 46 CGM metrics were further calculated on a both daily and hourly basis using provided functions in the iglu package (Supplementary Table S1). These included metrics of euglycemia (i.e., TIR70-180 and time in normal glycemia [TING70-140]), of hypoglycemia (time below 70 mg/dL [TBR70], time below 54 mg/dL [TBR54]) and of hyperglycemia (time above 180 mg/dL [TAR180], time above 250 mg/dL [TAR250]). Glucose variability was calculated as global (i.e., coefficient of variation [CV]), intraday (CONGA, MAGE) and interday (i.e., MODD). Absolute counts of alarms were calculated per day and classified as hypoglycemic or hyperglycemic according to glucose values at that moment.
Statistical analysis
All analyses were performed in R (version 4.4.5). The statistical significance level used for all analyses was α = 0.05. Demographic and clinical data are reported as median (interquartile range [IQR]) for continuous variables and as numbers and proportions for categorical variables. Comparisons between dilution subgroups (i.e., late and early transition) were performed using Student’s t test and χ2 test, or their nonparametric equivalent (Mann–Whitney U test and Fisher exact test, respectively) as appropriate.
Comparison of glycemic parameters between predilution and each postdilution time points were performed using linear mixed models generated with LmerTest and lme4 statistical packages. The models included the different time points (i.e., Pre-Dilution, Initiation, 1 month, 3 months, 6 months) and the centers as fixed effects and the patient identity as a random intercept. Residuals were inspected on Q-Q plots. Post-hoc pairwise comparisons of glycemic parameters to predilution were performed using emmeans package with correction for multiple tests. Principal component analysis (PCA) was conducted in R based on CGM data across all timepoints (n = 131). Prior to PCA, glucose metrics were standardized and imputed by a regularized expectation–minimization PCA algorithm with the missMDA package.
Results
Characteristic of participants
A total of 35 participants from 12 clinical sites (46% females [n = 16]) were included in this retrospective study. Characteristics of the cohort and each transition subgroup (i.e., early and late) are summarized in Table 1 and Supplementary Table S2. Participants were started on HCL system at 2.9 (2.4–3.7) years old after 1.1 (0.6–1.5) years of T1D duration. In the predilution period, most participants had a suboptimal glucose control as shown by the glucose metrics in Table 1. More than 65% of participants (n = 23) had a nighttime TBR70 above 4% (ranging from 0% to 14%) (Table 1, Fig. 1). Median TDD before dilution was low: 9.7 (7.7–11.4) UI/day [0.6 UI/kg/d (0.5–0.8)]. Main reported reasons underlying dilution included low TDD (n = 14) or a combination of suboptimal control, nocturnal hypoglycemia, and/or low TDD in nearly half of the participants (n = 15) (Supplementary Fig. S1).
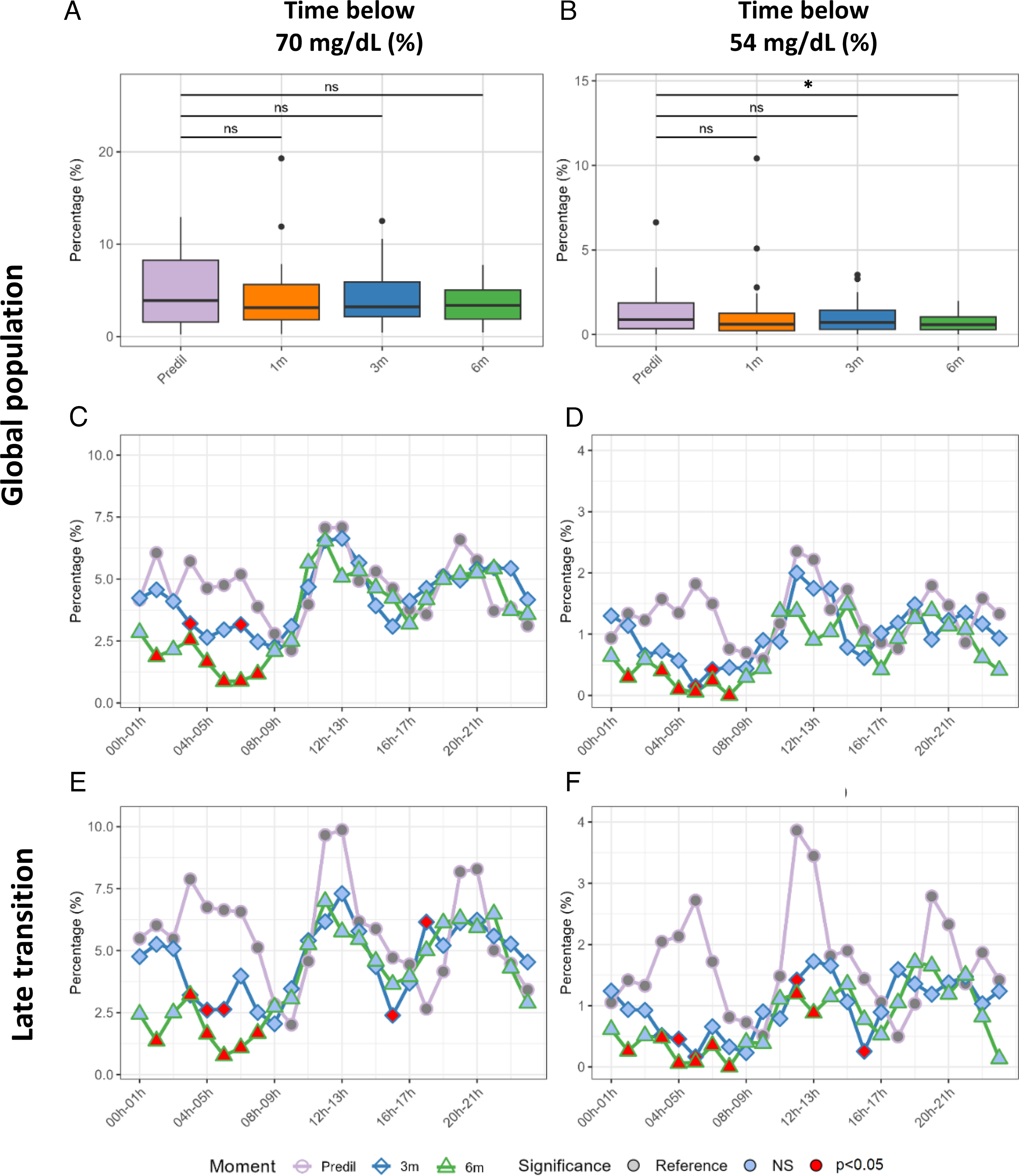
Evolution of the time spent in hypoglycemia (reference or purple circle and line), and at 1 month, 3 months (blue square and line), and 6 months (green diamond and line) postdilution in the whole population
Characteristics of Participants Before and After Insulin Dilution
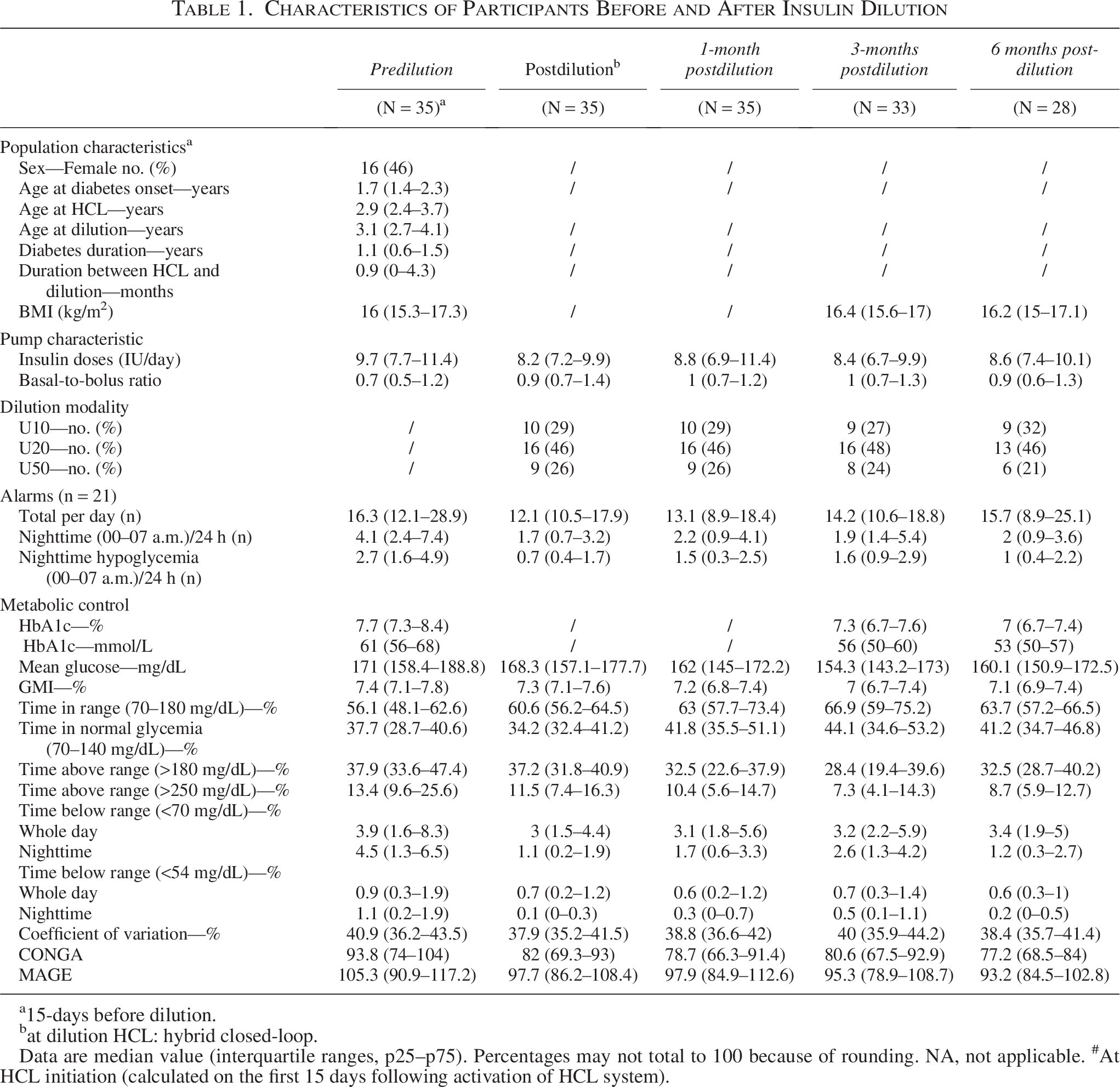
15-days before dilution.
at dilution HCL: hybrid closed-loop.
Data are median value (interquartile ranges, p25–p75). Percentages may not total to 100 because of rounding. NA, not applicable. #At HCL initiation (calculated on the first 15 days following activation of HCL system).
Participants were transitioned to diluted insulin at 0.9 (0–4.3) months after HCL initiation with 15 participants at the moment of HCL system initiation (early transition group) and 20 participants after (late transition group). Parents of every participant performed insulin dilution at home following a careful teaching by the diabetes care team. Two participants stopped dilution before 3 months and another one between 3 and 6 months as TDD increased above 15 UI/day. No episodes of DKA or SH were reported after insulin dilution.
Hypoglycemia reduced during the nighttime after dilution
Change in daily TBR70 and TBR54 are shown in Figure 1A–B. Episodes of hypoglycemia during the nighttime were markedly reduced from the first weeks after dilution. TBR<70 and TBR<54 between 4 AM and 7 AM decreased by three-fold and to near-to-zero from 3 months (P < 0.001), with results being sustained at 6 months post dilution (Fig. 1C–D, Supplementary Table S2). Participants with late transition showed an even greater reduction of these nighttime hypoglycemic episodes (Fig. 1E–F, Supplementary Table S2). Simultaneously, pump alarms were halved during the nighttime (Table 1, Supplementary Fig. S2).
Dilution of insulin improves euglycemia and reduces hyperglycemia
Shortly after dilution, TIR70–180 increased by 6% ± 10% (+1.5 h per day, P < 0.05) and TAR180 decreased by 4% ± 12% (− 1 hour per day, P < 0.05) (Fig. 2A–D, Table 1). Participants in the late transition group achieved slightly better glycemic outcomes at 3 months compared with those in the early transition group, with TIR70–180 and TAR180 progressively reaching respectively 67% (+ 2.7 h per day) and 28% (− 2.5 h per day) (Supplementary Table S2). TIR70–180, TING70–140, and TAR180 strongly improved during the nighttime (Fig. 2E–H). Participants in late transition group also exhibited a reduction of post-prandial hyperglycemic excursions from 3 months postdilution (P < 0.05) (Fig. 2I–L). Importantly, TAR250 was nearly halved at 3 months postdilution (Table 1, Fig. 2D). Overall mean glucose decreased from 174 mg/dL to 158 mg/dL at 3 months with significant reduction of HbA1C levels of –0.7%, and −0.9% at 3 months and 6 months, respectively (Table 1). HbA1c remained significantly lower in participants with late transition throughout the follow-up (Supplementary Table S2).
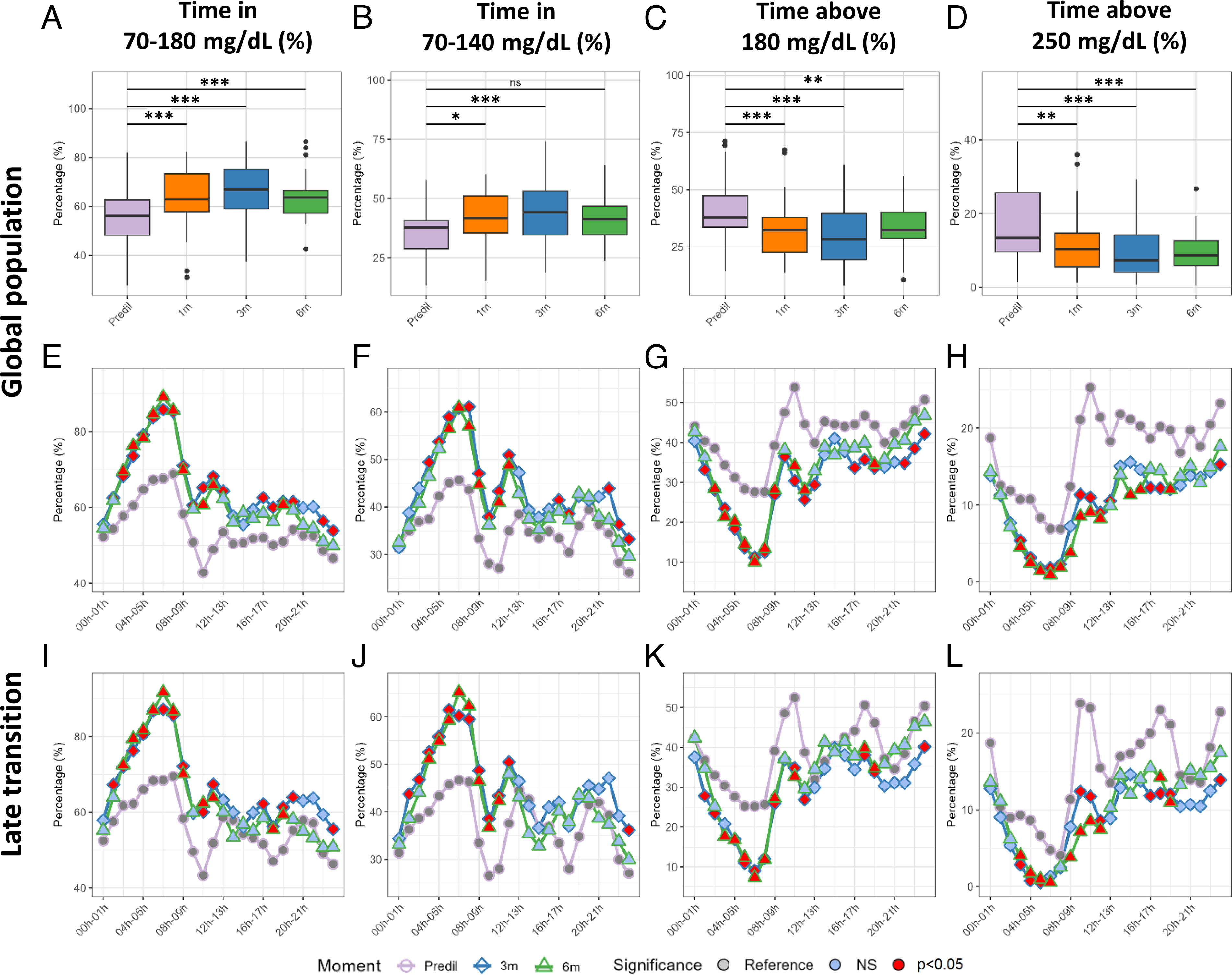
Evolution of the time spent in normoglycemia and in hyperglycemia before dilution (Reference or purple circle and line), and at 1 month, 3 months (blue square and line), and 6 months (green diamond and line) postdilution in the whole population
Interday and intraday glucose variability improved with insulin dilution
Concomitantly to the reduction of TBR70 and the increase of TIR180, daily CV remained similar after dilution until a significant decrease at 6 months (Fig. 3). Nonetheless, insulin dilution was associated with a decrease of CV below 36% over the whole night (Fig. 3). Furthermore, transition to diluted insulin was associated with a decrease of interday variability (i.e., IQR, SD, CONGA24, and MODD) (Table 1 and Fig. 3). Metrics of intraday variability (MAGE, CONGA-1h) decreased with greater improvement during the nighttime (Table 1 and Fig. 3). These results were sustained until 6 months postdilution.
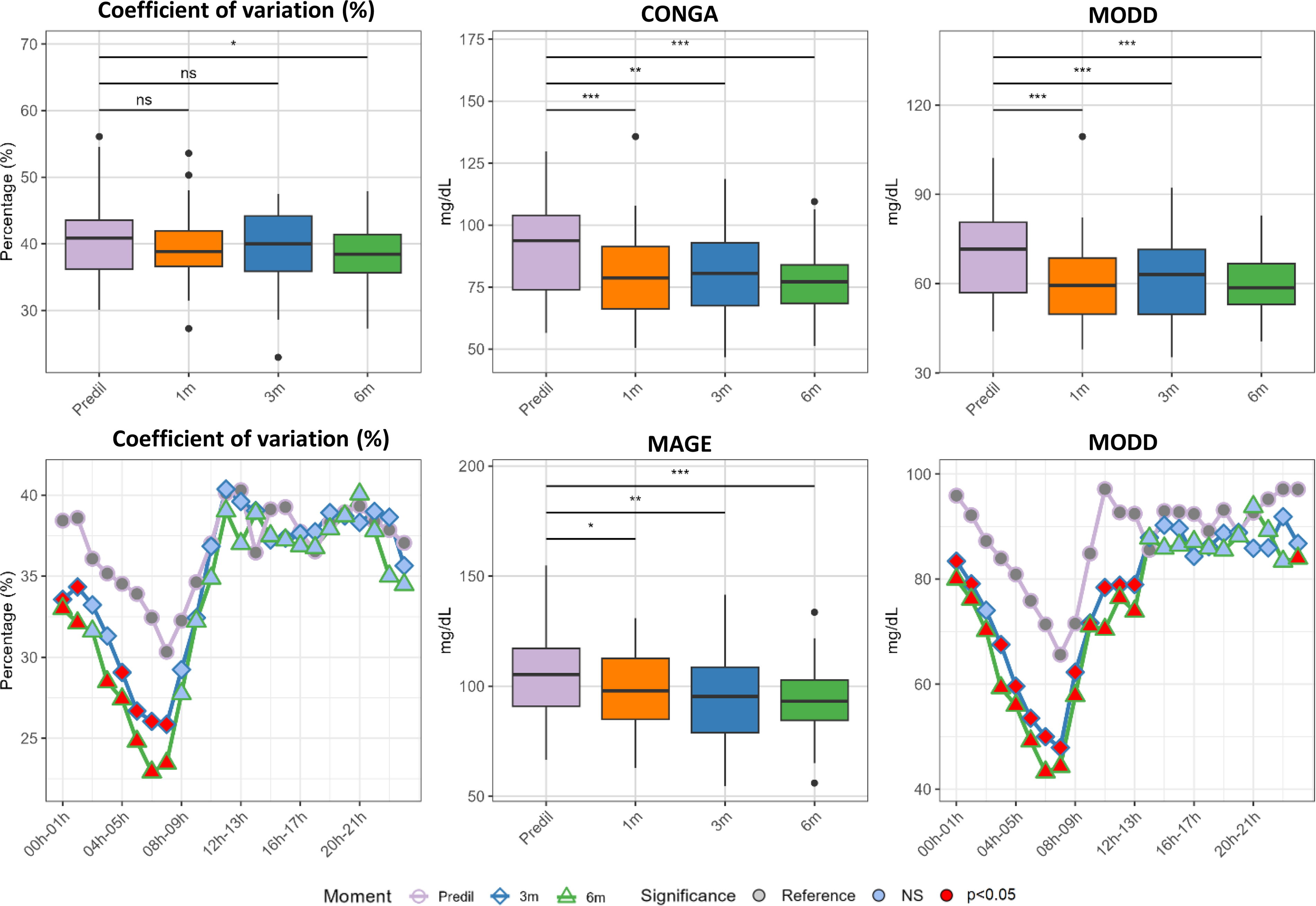
Evolution of glucose variability before dilution (purple line), and after 1 month, 3 months (blue line), and 6 months (green line) postdilution. Lines represent the mean percentage of time spent in the different glycemic ranges. Box plots display the median, 25th, and 75th percentiles. Values were adjuster for the center. Comparisons between Pre-HCL and each time point were performed using linear mixed models. The significance level is represented by the signs above the boxplots (ns = P > 0.05, *= P < 0.05, **= P < 0.01, ***= P < 0.001) or the color of the points (i.e., Reference = gray, P > 0.05 = light blue, P < 0.05 = red).
Dilution of insulin homogenizes glucose control across participants, in both early and late transition subgroups
Insulin dilution markedly tightened overall glucose control. We observe a reduction of hyperglycemia on the first component (PC1) and a marked reduction of nighttime hypoglycemia on the second (PC2) (Fig. 4). Participants in the late transition yielded greater benefits, especially for the reduction hypoglycemia (Fig. 4B, Supplementary Table S2). Dilution also narrowed glucose inter-individual variability, independently of the transition group, witnessed by the reduction of both the dispersion of glycemic parameters values (Table 1) and the size of the ellipses on the PCA (Fig. 4A–B).
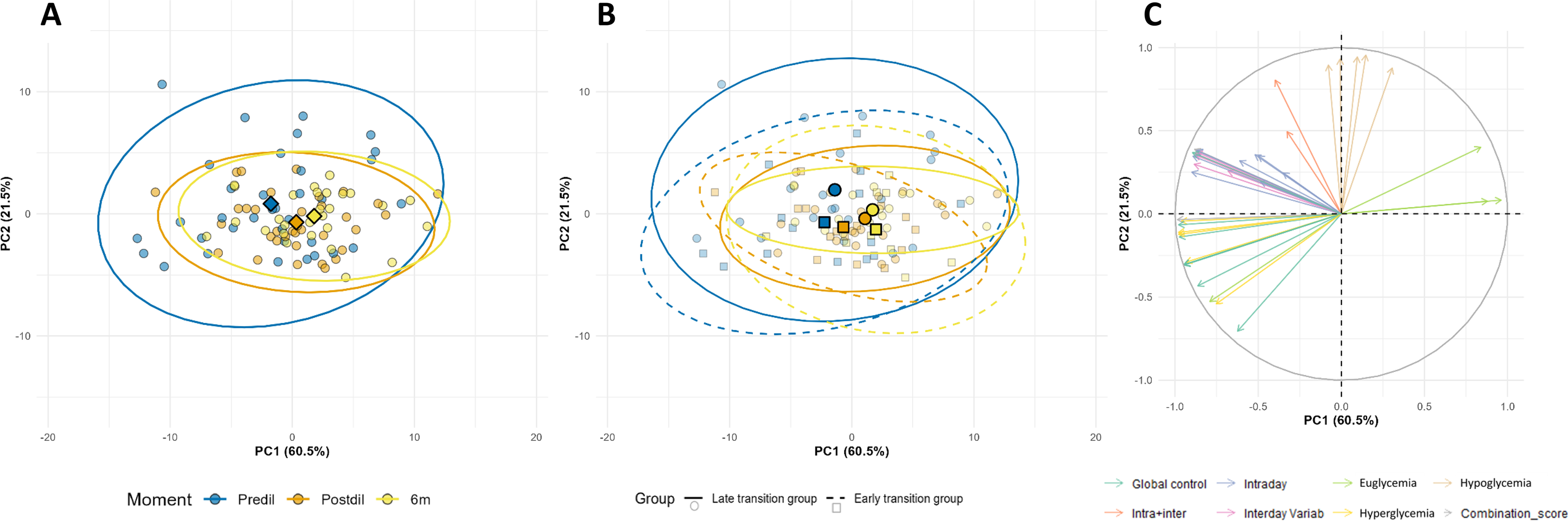
Evolution of glucose control before and after dilution in the whole population
Discussion
Our real-world study suggests that insulin dilution in toddlers with HCL is associated with a substantial reduction of nighttime hypoglycemia. Furthermore, transition to diluted insulin improved glycemic control with an increase in TIR180 and TING70–140, and a concomitant decrease of TAR180. Altogether, these improvements lead to a decrease of glycemic variability and a homogenization of glucose control across the participants. Insulin dilution appears most beneficial for very young children who combine very low total daily insulin doses with marked glycemic variability or recurrent nighttime hypoglycemia—the situations in which current technologies perform least effectively.
Despite progress in HCL systems, only a handful are validated for this age group with their algorithms overlooking some specific needs of the toddlers.5–19 Less than 20% of very young children with T1D currently reach the international glycemic targets, with toddlers being at high risk of hypoglycemia.5–19 Alternative therapeutic approaches are therefore required. Insulin dilution addresses challenges of the very young such as labile insulin sensitivity and very low insulin requirements and may help bridge this gap.2–4,33
Dilution increases the volume of each insulin pulse without increasing its absolute quantity, enabling the algorithm to overcome mechanical pump limitations and deliver smoother, more precise micro-boluses. Pharmacokinetic studies showed preserved potency yet a narrower spread of time-to-peak and clearance, limiting both excessive boluses and frequent pump suspensions.21,22 Participants requiring very low doses of insulin (e.g., below 10 UI per day) may thus get the greatest benefit from the dilution. 24 Several case series mostly in open-loop settings reported reductions in both hyper- and hypoglycemia,24–32 whereas the only randomized controlled trial using HCL found no improvement in glycemic control. 27 In that trial, more than 90% of participants had above 10 UI/day, under-representing children with very low insulin requirements. Conversely, in our cohort, 50% of the participants had a TDD below 10UI/day providing a more suitable context to evaluate the transition to diluted insulin in this specific population.
Very young children with T1D have pronounced intra-day variations in insulin sensitivity, corresponding to an inverse dawn phenomenon. The peak of growth hormone around midnight transiently induces insulin resistance; by dawn the child becomes extremely sensitive with insulin requirements falling to almost zero. 34 Coupled with the very low insulin requirements and reduced gluconeogenesis, 35 this pattern may explain why more than half of SH occurs during the nighttime in this population. 36 The high nocturnal burden results in increased parental stress and fear of hypoglycemia, 37 worsening the glycemic control of the child. 38 HCL system improved both euglycemia and hyperglycemia yet failed to reduce hypoglycemic episodes.5–19 Our team recently showed that very young children with T1D even increased hypoglycemia at initiation of HCL in high-risk windows such as the post-prandial period. 39 Furthermore, in a subset of the cohort, nighttime hypoglycemia resulted from the administration of patency boluses performed by the system to prevent the tubing from becoming blocked. Our results support that insulin dilution mitigate the risk of hypoglycemia in the post-prandial period and during the nighttime. Consequently, we observed a reduction of pump alarms during the night (Supplementary Fig. S2, Table 1) with hypoglycemic alarms being divided by three after 2 weeks (2.7 vs. 0.7 alarms per night), limiting parental nocturnal burden.
As previously described by our study and others,24–26,28–32 dilution was associated with improved glucose control (increase in TIR180 and TING70–140, and a concomitant decrease of TAR180) resulting in a significant decrease of HbA1c. These findings are clinically relevant, as maintaining adequate glucose control in very young children is critical as early-onset T1D is associated with higher morbidity and mortality compared to later-onset disease. 2 The improvement of glucose control was even larger in the late transition group where participants transitioned more than 1 month after HCL initiation, which is beyond the algorithm’s stabilization window. 39 This observation suggests an independent effect of insulin dilution rather than improvements attributable solely to the HCL system. Consequently, when a child with very low TDD (e.g., <10 UI/day) does not reach reasonable glucose targets after 1 month of optimized HCL, dilution may be considered in order to prevent therapeutic failures and preserve the confidence of the parents in the technology.
Safe implementation of insulin dilution for the parents and health care professional remains critical. Nicol et al. recently outlined practical safety guidelines for diluted insulin in HCL systems to avoid insulin over- or under-dosing. 24 They highlighted key features such as pump labeling, caregiver education, and tailored pump settings. 24 Similarly to other case series, we did not record any DKA or SH regardless of whether the dilution was initiated at HCL initiation or later. These findings support that structured education to families and providers may prevent dosing errors and provide safe groundwork for improving glucose control. 24 Nonetheless, although not currently available, the use of commercially pre-diluted cartridges would lighten parental workload and add an extra safety margin.
Our study has several strengths including the description of the largest cohort of children with diluted insulin from 12 expert diabetes centers distributed all over the country. Furthermore, the unrestricted real-world study design supports the external validity and translational utilization of results, emphasizing the ability of generalization of the results to a wider population. 40 Also, our cohort has the lowest insulin TDD (i.e., median below 10UI/day) providing for the first time results in this specific population, which corresponds to the manufacturer suggestion to dilute insulin. Finally, this is the first study collecting physician reasons underlying the dilution and using hour-by-hour analysis of glycemic patterns that yielded key clinical messages.
Our study was also limited by its retrospective design. However, it resulted in very little missing data, particularly with regard to the CGM data. The multicentric design of the study led to different dilution protocols (i.e., U10, U20, or U50) and differences in pump management. However, prior to implementing dilution, all centers also benefited from shared experience and feedback from the pioneering expert center, which contributed to harmonizing clinical approaches. Another limitation of the study is the absence of a control group as CamAPS algorithm has self-learning algorithm, which may participate to improvement of glucose control. Utilization of linear mixed models allowed to partially control these confounders. Despite potential benefits of dilution, we could not directly evaluate the additional diabetes-related workload for the parents. 8 Nonetheless, the analysis of the daily frequency of alarms allowed us to assess part of the burden reduction after dilution.
HCL in very young children is challenging due to their unique physiology. Insulin dilution in HCL systems may provide a solution to manage very young children with diabetes in specific situations. The present study suggests that insulin dilution is safe and feasible whether implemented at HCL initiation or later if therapeutic goals are not achieved. In both situations, transition to insulin was associated with reduced nighttime hypoglycemia, increased euglycemia, and reduced hyperglycemia. Current literature and manufacturer guidance offer limited consensus on when to dilute insulin, leaving a gap in guidance for pediatric participants with low TDD. We propose three main indications for considering insulin dilution: (i) low TDD (<8 U/day), and/or (ii) persistent high glucose variability (CV > 45%) and/or unsatisfactory TIR (TIR < 60%), and/or (iii) persistent nocturnal hypoglycemia (TBR70 > 4% between 0 and 7 AM) despite HCL optimization. Randomized clinical trials are warranted to validate these indications. Dilution requires expertise from both health care providers and parents, with careful preparation, labeling of the device, and monitoring to prevent dose errors and ensure safety. Decision to dilute must be made on an individual basis, as part of a shared decision-making process with all the stakeholders.
Authors’ Contributions
K.P. and O.G.P. Researched data, analyzed the data and contributed to discussion, and wrote the first draft of the article. G.V., R.F., C.B.S., D.T., A.S., A.M., V.R., M.R., D.I., A.B., C.G., A.T., N.G., L.M., L.A., E.R., E.B., M.P., and J.P. Researched data and reviewed and edited the article. K.P., O.G.P., and J.B. Contributed to discussion and reviewed and edited the article. All authors approved the final version of the article.
Footnotes
Acknowledgments
The authors thank Dr. Cécile Gouillard Darnaud and Dr. Elsa Haïne from University Hospital of Nice-Lenval Hospital for their patient management.
Author Disclosure Statement
No potential conflicts of interest relevant to this article were reported.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.