
Abstract
Objective:
Adjunctive use of tirzepatide or semaglutide has demonstrated benefits in improving glucose control (HbA1c, Time in Range), reducing body weight, and insulin requirements, in overweight (OW) or obese (OB) adults with type 1 diabetes (T1D). However, the adverse event (AE) profiles with these agents in this population have not been documented. This study evaluated real-world AEs associated with tirzepatide or semaglutide use in OW/OB adults with T1D.
Materials and Methods:
In this single-center study at the Barbara Davis Center for Diabetes, we surveyed 230 adults with T1D who were using tirzepatide or semaglutide as adjunctive therapies. Demographics, data for diabetes control metrics, details of tirzepatide or semaglutide use, and related AEs were collected.
Results:
Male participants had a higher baseline mean body weight (107.8 ± 18.9 kg vs. 89.6 ± 19.2 kg, P < 0.01) and were older (44.2 ± 12.2 years vs. 40.4 ± 11.5 years, P < 0.05) compared to female participants using tirzepatide or semaglutide at the time of initiation. Symptomatic hypoglycemia was more frequent in the tirzepatide-treated group compared to the semaglutide-treated group (29% vs. 13.4%, P < 0.001). Gastrointestinal AEs did not differ between the two groups. Young adults and females were more likely to report gastrointestinal AEs regardless of the medication. The proportion of individuals who reduced their dose due to AEs was similar.
Conclusions:
We conclude that symptomatic hypoglycemia was more commonly reported by the tirzepatide-treated group compared to the semaglutide-treated group, while gastrointestinal AEs were comparable between groups. We recommend that individualized risk assessment and close supervision on insulin dose changes are required when prescribing off-label tirzepatide or semaglutide in adults with T1D.
Introduction
Many adults with type 1 diabetes (T1D) are not able to achieve glycemic goals despite advances in therapeutics and technologies. 1 In addition, the majority of adults with T1D in the USA are either overweight (OW) or obese (OB), following a similar pattern to the USA general population. 2 We previously have shown that the adjunctive, off-label use of tirzepatide and semaglutide improves glycemic outcomes, decreases body weight, insulin dose requirements, and improves many continuous glucose monitor (CGM) metrics in adults with T1D.3–8 However, the adverse events (AEs) profile is not known in adults with T1D while using tirzepatide or semaglutide in the real world. We conducted a prospective study to investigate AEs in the real-world use of off-label tirzepatide or semaglutide in OW/OB adults with T1D.
Methods
At the Barbara Davis Center for Diabetes (BDC), using electronic medical records (EMRs), we determined the number of OW/OB adults with T1D who were prescribed tirzepatide or semaglutide in the last 8 years (since the Food and Drug Administration [FDA] approval of semaglutide for patients with type 2 diabetes [T2D] and tirzepatide FDA approval in July of 2022 for T2D). We sent a secure online link to all the subjects for a survey using REDCap. The survey link was sent twice to their emails, a week apart. Demographic and diabetes control data were obtained from the EMRs. Details of tirzepatide or semaglutide use, and associated AEs were obtained via a questionnaire. An AE was defined as any event that the patient attributed to tirzepatide or semaglutide treatment and that occurred at least once during the treatment period. Symptomatic hypoglycemia was defined as an event in which glucose levels were ≤ 70 mg/dL, measured by the CGM or blood glucose meter, accompanied by symptoms. This study was approved by the Colorado Multiple Institutional Review Board.
Statistical analyses were performed in R (version 4.4.3) and SPSS (version 31.0). Normality of continuous variables (age at first prescription, HbA1c, weight, and diabetes duration) was assessed with the Kolmogorov–Smirnov test; HbA1c deviated from normality (KS P = 0.004), whereas others did not (all P > 0.05). Between-group comparison for normal variables used an independent samples t-test, with Welch’s t-test when variances were heterogeneous; non-normal variables were compared using the Mann–Whitney U test. Categorical outcomes were compared with the χ2 test or Fisher’s exact test when expected values were small; where relevant, odds ratios with 95% confidence intervals were reported. For drug-specific binary outcomes (e.g., any adverse effect, dose decrease), percentages were calculated using the number of starters for the drug as the denominator; for reason-specific and drug-type analysis, the appropriate sub-cohort (e.g., stoppers or those who used any drug) served as a denominator. Among participants who started both drugs, within-person comparison (e.g., tirzepatide vs. semaglutide for adverse effects, dose decrease) used McNemar’s test, employing an exact two-sided binomial test when discounted pairs were few and a continuity-corrected χ2 otherwise. All tests were two-sided with α = 0.05, and P values in the table correspond to the specific test described above.
Results
At the time of this writing, the adult clinic at the BDC had 739 adults with T1D who were prescribed tirzepatide or semaglutide in the last 8 years. Out of 739 adults with T1D who received the survey via email, 251 (34%) adults with T1D responded. Of 251 respondents, 21 participants were excluded due to not reporting enough data; therefore, final analyses included 230 participants (Fig. 1).
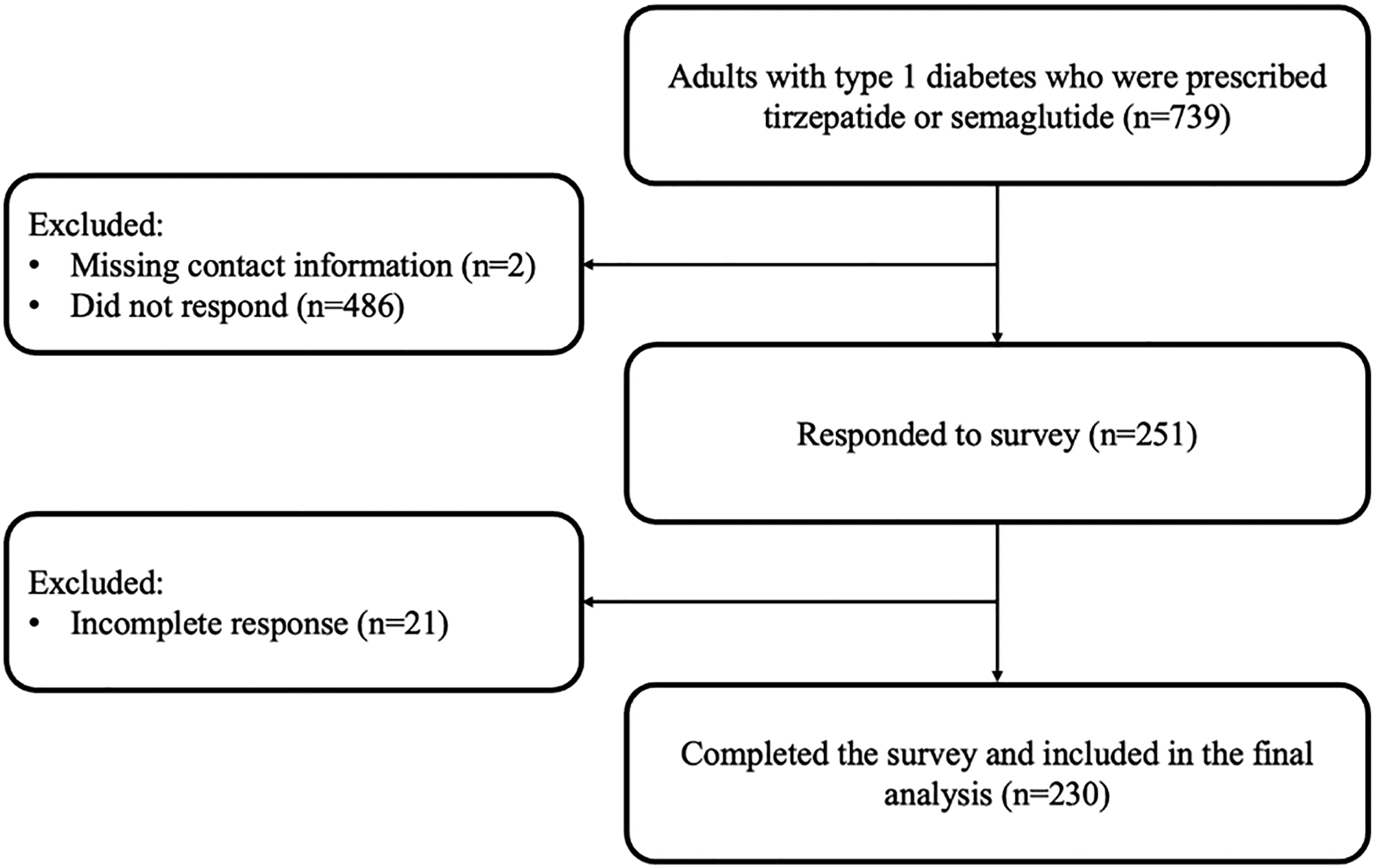
Study flowchart.
The mean age was 41.6 ± 11.9 years, diabetes duration was 25.2 ± 12.2 years, HbA1c was 7.2 ± 1.1%, and 69% were females. The mean weight was 107.8 ± 18.9 kg and 89.6 ± 19.2 kg (P < 0.01), and the mean age was 44.2 ± 12.2 and 40.4 ± 11.5 for male and female participants, (P < 0.05), respectively. Among participants, 82 individuals used both tirzepatide and semaglutide at different times, 73 used only tirzepatide, and 75 used only semaglutide. HbA1c, diabetes duration, and body weight did not differ between individuals with and without AEs for both the tirzepatide and semaglutide-treated groups. There were no hospitalizations from severe hypoglycemia or diabetic ketoacidosis reported in either group.
Common gastrointestinal AEs did not differ between tirzepatide and semaglutide: nausea (59.4% vs. 59.2%, P = 0.99), diarrhea (38.7% vs. 32.5%, P = 0.28), constipation (37.4% vs. 28.7%, P = 0.12), gastroesophageal reflux (31% vs. 24.8%, P = 0.26), and vomiting (24.5% vs. 21%, P = 0.50), respectively (Table 1). Females and younger individuals reported gastrointestinal AEs more frequently in both the tirzepatide and semaglutide-treated groups.
Adverse Events Reported by Participants
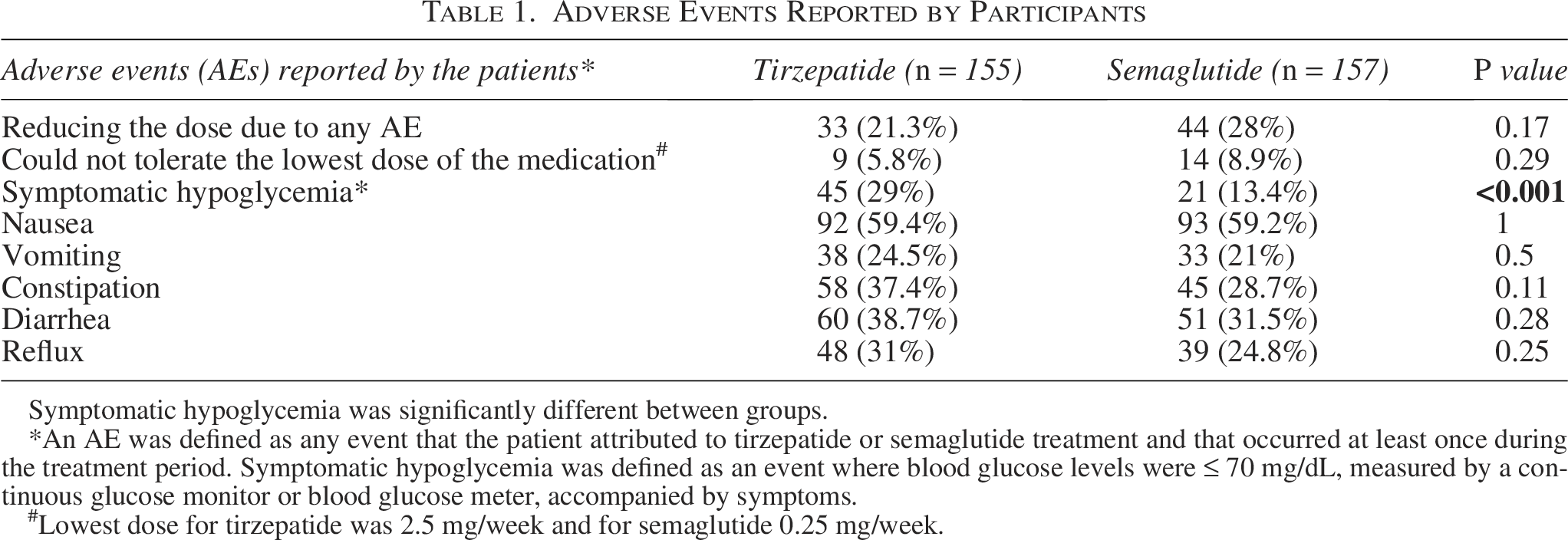
Symptomatic hypoglycemia was significantly different between groups.
*An AE was defined as any event that the patient attributed to tirzepatide or semaglutide treatment and that occurred at least once during the treatment period. Symptomatic hypoglycemia was defined as an event where blood glucose levels were ≤ 70 mg/dL, measured by a continuous glucose monitor or blood glucose meter, accompanied by symptoms.
#Lowest dose for tirzepatide was 2.5 mg/week and for semaglutide 0.25 mg/week.
Symptomatic hypoglycemia was higher in the tirzepatide-treated group compared to the semaglutide-treated group (29% vs. 13.4%, P < 0.001). Hypoglycemia tended to be lower among automated insulin delivery (AID) system users (20.8% [31/149]) than subjects on multiple daily injections (MDI) (30.9% [25/81], P = 0.1). Use of AID systems was associated with a significantly lower prevalence of hypoglycemia among semaglutide users (8.8% with AID vs. 21.8% with MDI; P = 0.02). Among tirzepatide users, hypoglycemia rates were also lower in those using AID compared with MDI, although this difference did not reach statistical significance (25.0% vs. 36.4%; P = 0.14). However, hypoglycemia was reported more frequently in tirzepatide users on AID systems (25/100) compared to semaglutide users on AID systems (9/102; P = 0.002). Changes in body weight, BMI, or insulin dose adjustments were not evaluated in this study.
A total of 10 (6.5%), 11 (7.1%), 4 (2.6%), 2 (1.3%), and 6 subjects (3.9%) were on tirzepatide doses of 2.5, 5, 7.5, 10, and 12.5 mg/week, respectively. However, 7 (4.5%), 14 (8.9%), 8 (5.1%), and 1 (0.6%) semaglutide-treated subjects were on 0.25, 0.5, 1, and 2 mg/week, respectively. Subjects reducing the medication dose due to AEs did not differ between the tirzepatide or semaglutide-treated groups (21.3% vs. 28%, respectively, P = 0.17). Among tirzepatide-treated subjects, 5.8% could not tolerate the starting dose of 2.5 mg/week. Similarly, in the semaglutide-treated subjects, 9.6% could not tolerate the starting dose of 0.25 mg/week.
A total of 82 participants who had used both drugs at different times showed a similar pattern: symptomatic hypoglycemia was more frequent with tirzepatide than semaglutide (25.6% vs. 13.4%; P = 0.006; Table 2). In contrast, within-person rates of nausea, vomiting, constipation, diarrhea, and gastrointestinal reflux did not differ between semaglutide or tirzepatide groups (all P > 0.05), consistent with the unpaired comparisons above.
Adverse Event Comparison in Same Adults with Type 1 Diabetes Who Used Tirzepatide or Semaglutide at Different Times
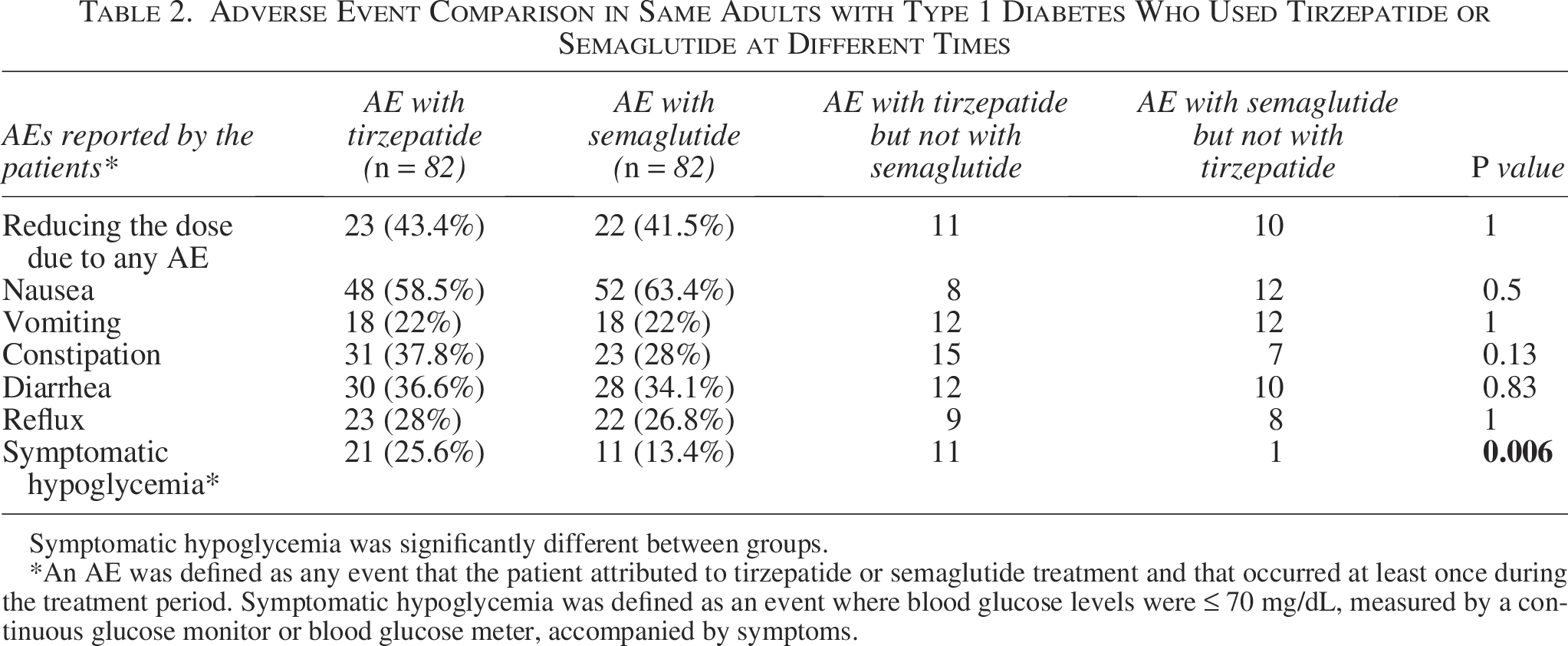
Symptomatic hypoglycemia was significantly different between groups.
*An AE was defined as any event that the patient attributed to tirzepatide or semaglutide treatment and that occurred at least once during the treatment period. Symptomatic hypoglycemia was defined as an event where blood glucose levels were ≤ 70 mg/dL, measured by a continuous glucose monitor or blood glucose meter, accompanied by symptoms.
Discussion
A higher percentage of OW/OB female subjects with T1D used tirzepatide or semaglutide compared to male subjects. Additionally, female subjects were younger and had a lower baseline weight at the initiation of treatment. However, baseline HbA1c levels and diabetes duration were similar in the two groups. We did not evaluate whether the decision to initiate tirzepatide or semaglutide was patient-driven or provider-initiated.
Most often reported AEs were gastrointestinal, with no difference in tirzepatide or semaglutide users. Female and younger subjects reported more gastrointestinal AEs. A small number of participants were unable to tolerate the starting dose (5.8% for tirzepatide, 9.6% for semaglutide). Similarly, 21.3% and 28% of subjects had to decrease the dose of tirzepatide or semaglutide, respectively, due to AEs.
Symptomatic hypoglycemia was reported more often with tirzepatide than with semaglutide. Previous real-world studies in patients with T1D showed that tirzepatide was associated with higher HbA1c reduction compared to semaglutide.4,5,9 It is possible that the higher rate of hypoglycemia with tirzepatide was driven by greater efficacy in weight loss and HbA1c reduction (not evaluated in our study). It is important to actively adjust insulin dose while on tirzepatide or semaglutide in adult subjects with T1D. There are several consensus and expert opinions published to adjust insulin in GLP-1RA, GIP/GLP-1RA use in T1D to prevent hypoglycemia.10,11 At the BDC, we have clinical guidelines to safely use GLP-1RA, GIP/GLP-1RA in OW/OB adults with T1D. 12 We did not assess insulin dose adjustments or changes in body weight in this study (which have been reported earlier). 4
A previous study from our center documented weight loss of about 21% and 9% with similar improvement in glucose control with tirzepatide and semaglutide after 1 year of use in subjects with T1D, respectively. 4 Our study included 82 subjects who had used both tirzepatide and semaglutide at different times, enabling within-person comparisons. Symptomatic hypoglycemia was higher while using tirzepatide when compared with semaglutide use.
The strengths of our study include (1) a large cohort of adults with T1D using tirzepatide or semaglutide, (2) being prospective in nature, and (3) the inclusion of individuals who had used both medications at different times, which allowed for within-person comparisons. The limitations of our study include that it was a patient survey, and results may have been affected by the responder and recall bias. Patients who have used these medications longer and at higher doses may have reported more AEs. The survey response rate was 34%, which limits the generalizability of the results. AEs were self-reported and may not have clinical implications.
We conclude that more females and younger adults with T1D reported gastrointestinal AEs while using tirzepatide or semaglutide. Symptomatic hypoglycemia was higher with tirzepatide compared to semaglutide; however, gastrointestinal AEs did not differ between the groups. Larger, prospective studies are required to better understand the AE profile in patients with T1D using tirzepatide or semaglutide.
Authors’ Contributions
H.K.A. and E.M. contributed to conceptualization, methodology, and data curation. D.C. contributed to the formal analysis and visualization. K.E.K. and H.K.A. contributed to writing—original draft. S.G. contributed to the supervision, reviewing, and editing of this article. All the authors approved the final draft. H.K.A. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Acknowledgment
The authors would also like to thank Bing Wang for data downloads from EPIC.
Author Disclosure Statement
H.K.A. received research support and consultation fees through the University of Colorado from Roche, Dexcom, Abbott Diabetes, and Medtronic. S.G. received research support from Eli Lilly, Medtronic, Diasome, Dexcom, consultation fees from Minimed, Novo-Nordisk, Roche, Dexcom, Vertex, Abbott Diabetes, and Eli Lilly. through the University of Colorado. Other authors do not have any conflict of interest.
Funding Information
There is no funding for this study.