
Abstract
Background:
Daily use of continuous glucose monitoring (CGM) has been shown to reduce diabetes-related events and associated costs in individuals with type 2 diabetes (T2D) regardless of their therapy. However, adoption of CGM among the large majority of T2D adults in the United States who are treated with noninsulin therapies has been limited.
Methods:
This retrospective database study assessed the effects of CGM acquisition on health care resource utilization (HCRU) in a large cohort of T2D adults treated with noninsulin, antidiabetes therapies. Inclusion criteria were T2D diagnosis, age ≥18 years, treated with noninsulin therapies, CGM-naive before CGM acquisition, and continuous medical/pharmacy insurance coverage during the 12-month preindex and postindex periods. The primary outcome measures were changes in all-cause hospitalizations (ACH), emergency department (ED) visits, acute diabetes complications, hyperglycemic events (HGE), and diabetic ketoacidosis (DKA) during the 12 months following CGM acquisition.
Results:
A total of 20,468 adults with T2D were included in this analysis. CGM acquisition was associated with significant reductions in event rates in the postindex period compared with the preindex period HCRU at 12 months: ACH (−25%), ED visits (−7%), HGE (−7%), DKA (−86%), and acute diabetes complications (−7%), all P < 0.0001. Similar reductions in events per person were also observed: ACH (−20.6%), ED visits (−7.2%), HGE (−6.2%), DKA (−63.0%), and acute diabetes complications (−6%), all P < 0.0001. Significant reductions were also seen in patients with cardiovascular disease. ACH and ED visits decreased by 35% and 12%, respectively; in those with liver disease by 25% and 13%; in those with renal disease, ACH decreased by 33%; and in those with hypertension, ACH and ED visits decreased by 26% and 7%, respectively. All reductions were statistically significant (P < 0.01).
Conclusions:
This analysis demonstrated an association between CGM acquisition and reductions in HCRU in adults with T2D treated with noninsulin therapies.
Keywords
Introduction
The acute and long-term complications of poorly managed diabetes are well recognized1–3; however, glycemic control remains suboptimal in most people living with type 2 diabetes (T2D) in the United States. 4 According to recent findings by Hankosky et al., only 25.2% of individuals with diabetes using mealtime insulin and just 12.3% of those on basal insulin in the United States are meeting the American Diabetes Association’s recommended target for glycated hemoglobin (HbA1c) of less than 7%. 5
In addition to its clinical consequences, the rising cost of treating the complications of diabetes is threatening to overwhelm U.S. health care systems. Over $108 billion (35%) of the $307 billion in direct costs estimated for diagnosed diabetes in the United States is attributable to increasing emergency department visits, inpatient hospitalizations, and outpatient hospital visits resulting from suboptimal glycemic control and other diabetes-related conditions. 6 In addition, more than $102 billion is estimated for indirect costs resulting from absenteeism, reduced productivity at work, reduced labor force participation due to disability, and mortality. 6
Over the past 20 years, innovations in glucose monitoring technology have led to the development of continuous glucose monitoring (CGM). Unlike traditional finger-stick blood glucose monitoring (BGM), CGM provides real-time, interstitial glucose readings, trends, and alerts, enabling people with diabetes (PwD) and health care providers to make swift, informed decisions about treatment adjustments.
Numerous studies have shown that CGM improves glycemic control7–22 and reduces diabetes-related complications, hospitalizations, and associated costs13,23–25 in PwD treated with intensive insulin therapies.
Recent studies have also associated daily CGM use with reductions in diabetes-related events23,24,26–28 and cost effectiveness13,25,29,30 in individuals with T2D regardless of their therapy. However, the benefits of CGM among the large majority of T2D adults in the United States who are treated with noninsulin therapies have been limited.
To better understand the potential benefits of CGM in this population, we investigated the impact of acquiring a CGM on health care resource utilization (HCRU) in a large cohort of adults with T2D not on insulin therapies.
Materials and Methods
Study design
This retrospective, database study assessed the effects of CGM utilization on HCRU in a large cohort of T2D adults treated with noninsulin, antidiabetes therapies. The objective was to determine the impact of CGM use on all-cause hospitalizations (ACH), emergency department (ED) services, and acute diabetes complications following acquisition of CGM, comparing the incidence by type of events during the 12 months before acquiring CGM (preindex period) and during the 12-month follow-up (postindex period). The date of the first CGM acquisition was used for determining the index date for each patient. The study schemata are presented in Figure 1. Review and approval of the study by an institutional review board or ethics committee was not required.
Study schemata.
Data sources
Patient data were extracted from the Inovalon® Insights claims dataset (Inovalon, Bowie, MD) from January 1, 2016, to December 31, 2024. The dataset contains individual-level, de-identified health care claims data for privately insured (employer-sponsored employees and dependents), Medicare Advantage, and Managed Medicaid beneficiaries throughout the United States. The data include detailed claims for prescription drugs and supplies, including CGM devices. International Classification of Diseases, 10th Revision (ICD-10) codes were used to identify patients diagnosed with T2D, diabetes-related events (hyperglycemic events [HGE] and diabetic ketoacidosis [DKA]), gestational diabetes (GDM), and end-stage renal disease (ESRD). National Drug Codes (NDCs), Healthcare Common Procedure Coding System (HCPCS), and Current Procedural Terminology codes were used to identify patients acquiring a CGM device. NDCs and HCPCS codes were used to identify patients using insulin. NDCs were used to identify patients who were using noninsulin therapies.
Study Population
Inclusion criteria were T2D diagnosis, age ≥ 18 years, treated with noninsulin therapies, CGM-naive before CGM acquisition, and continuous medical and pharmacy insurance coverage during the 12-month preindex and postindex periods. Individuals with GDM, ESRD, or claims for insulin formulations were excluded.
Outcome measures
The primary outcome measures were changes in HCRU, encompassing ACH, all-cause ED visits, HGE, DKA, and acute diabetes complications defined as a composite outcome of DKA, hyperglycemia, hypoglycemia, hypoglycemic coma, and hyperosmolarity. Subgroup analyses examined changes in HCRU according to baseline comorbidities and payer type (commercial, Managed Medicaid, Medicare Advantage).
Statistical analysis
Baseline patient demographics, comorbidities, and medication usage were summarized. Wilcoxon signed-rank tests were used comparing preindex with postindex event rates. We used mixed-effects negative binomial regression models with a random intercept for each patient to account for within-subject correlation over time. For the overall adjusted analyses, we included covariates for age, gender, race and ethnicity, and payer type. Estimates are reported as adjusted incidence rate ratios with 95% confidence intervals. Stratified analyses were conducted by key comorbidities, including cardiovascular disease, liver disease, renal disease, hypertension, and payer type.
Results
Patients
A total of 20,468 adults with T2D were included in this analysis. Patients were mostly older, White, and Hispanic/Latino and covered by commercial insurance. A large proportion of patients were treated with biguanide therapies, followed by sulfonylurea and glucagon-like peptide-1 receptor agonist. The most common comorbidities were hypertension, pulmonary disease, and cardiovascular disease. Patient characteristics are presented in Table 1.
Patient Characteristics
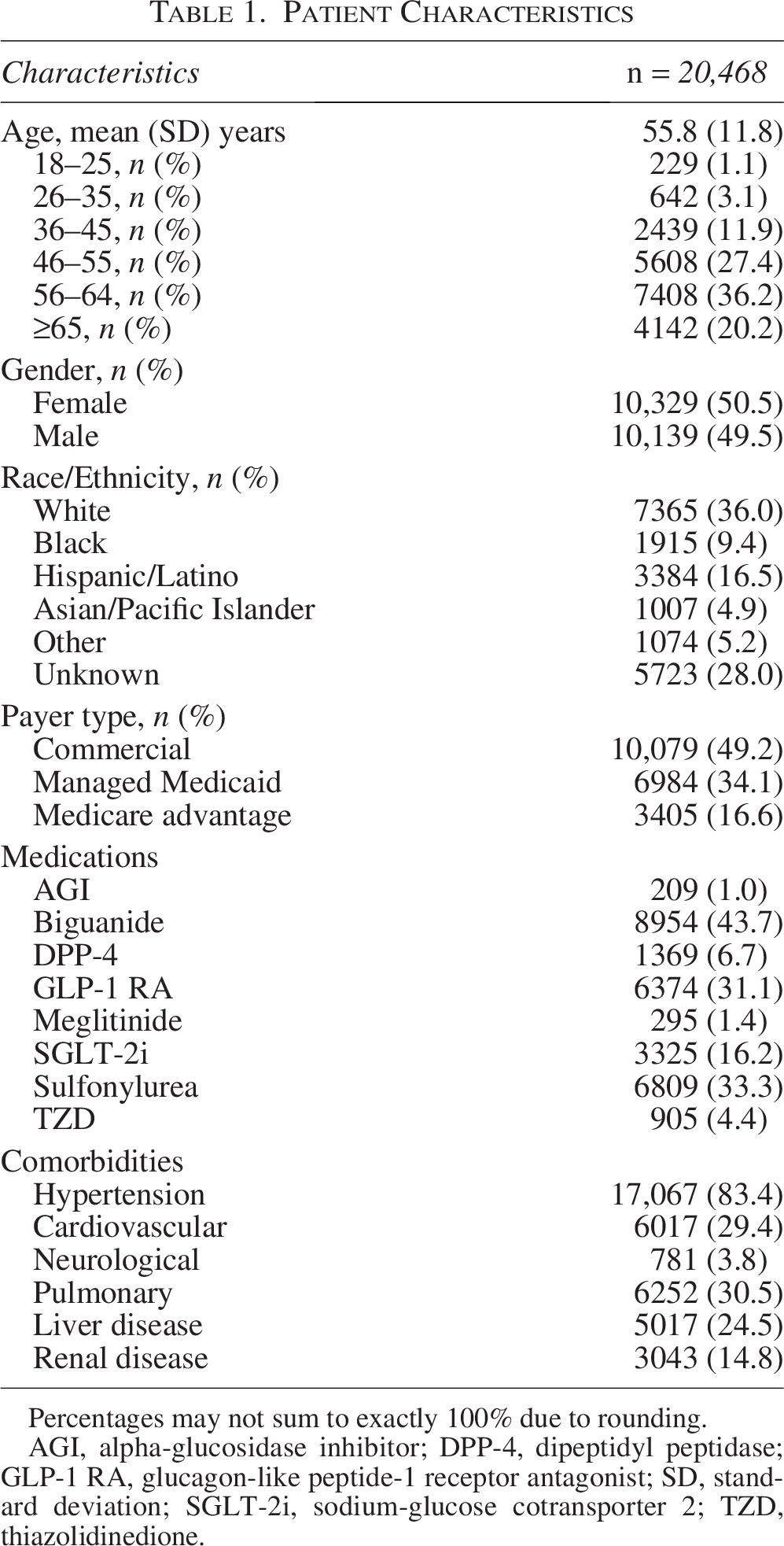
Percentages may not sum to exactly 100% due to rounding.
AGI, alpha-glucosidase inhibitor; DPP-4, dipeptidyl peptidase; GLP-1 RA, glucagon-like peptide-1 receptor antagonist; SD, standard deviation; SGLT-2i, sodium-glucose cotransporter 2; TZD, thiazolidinedione.
Changes in HCRU measures
CGM acquisition was associated with significant reductions in HCRU at 12 months. Adjusted analyses showed significant decreases in event rates in the postindex period compared with the preindex period by 25%, 7%, 7%, 86%, and 7% for ACH, ED visits, HGE, DKA, and acute diabetes complications, respectively. (Table 2)
Unadjusted and Adjusted Analysis of 12-Month Pre/Post Health Care Resource Utilization in Type 2 Diabetes Noninsulin Population
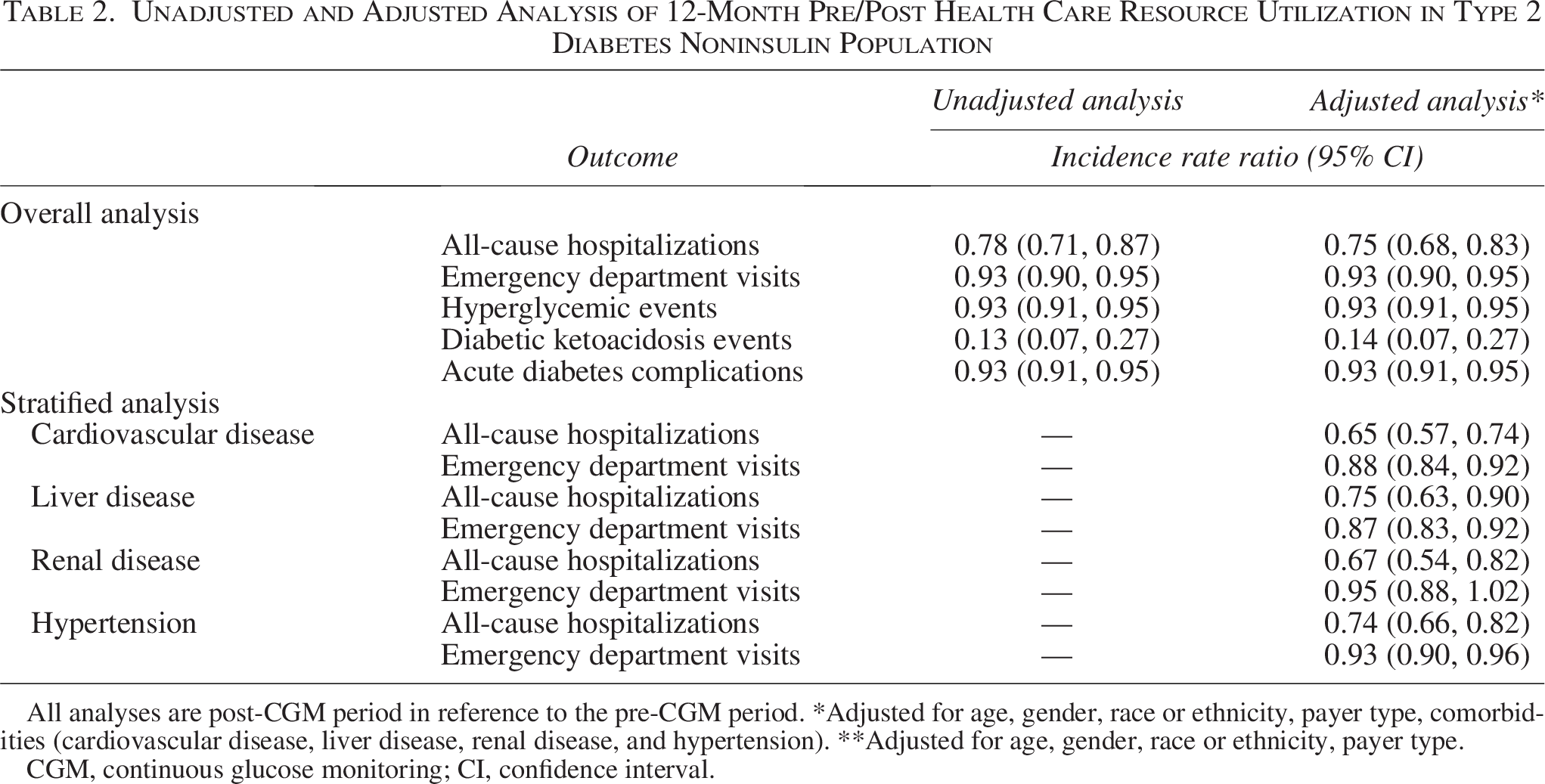
All analyses are post-CGM period in reference to the pre-CGM period. *Adjusted for age, gender, race or ethnicity, payer type, comorbidities (cardiovascular disease, liver disease, renal disease, and hypertension). **Adjusted for age, gender, race or ethnicity, payer type.
CGM, continuous glucose monitoring; CI, confidence interval.
The number of events and absolute events per 1000 patient years (1000/p/yrs) declined. This included reductions in ACH (from 18,189 to 14,442 [888.7–705.6 per 1000/p/yrs]), ED visits (from 9807 to 9101 [479.1–444.6 per 1000/p/yrs]), HGE (from 27,276 to 25,589 [1332.6–1250.2 per 1000/p/yrs]), DKA (from 246 to 86 [12.0–4.2 per 1000/p/yrs]), and acute diabetes complications (from 29,822 to 28,041 [1457.0–1370.0 per 1000/p/yrs]). All reductions were statistically significant (P < 0.0001). Similar reductions in the number of events per patient were observed during the postindex period in ED visits (7.2%), HGE (6.5%), and acute diabetes complications (6.0%) (Fig. 2).
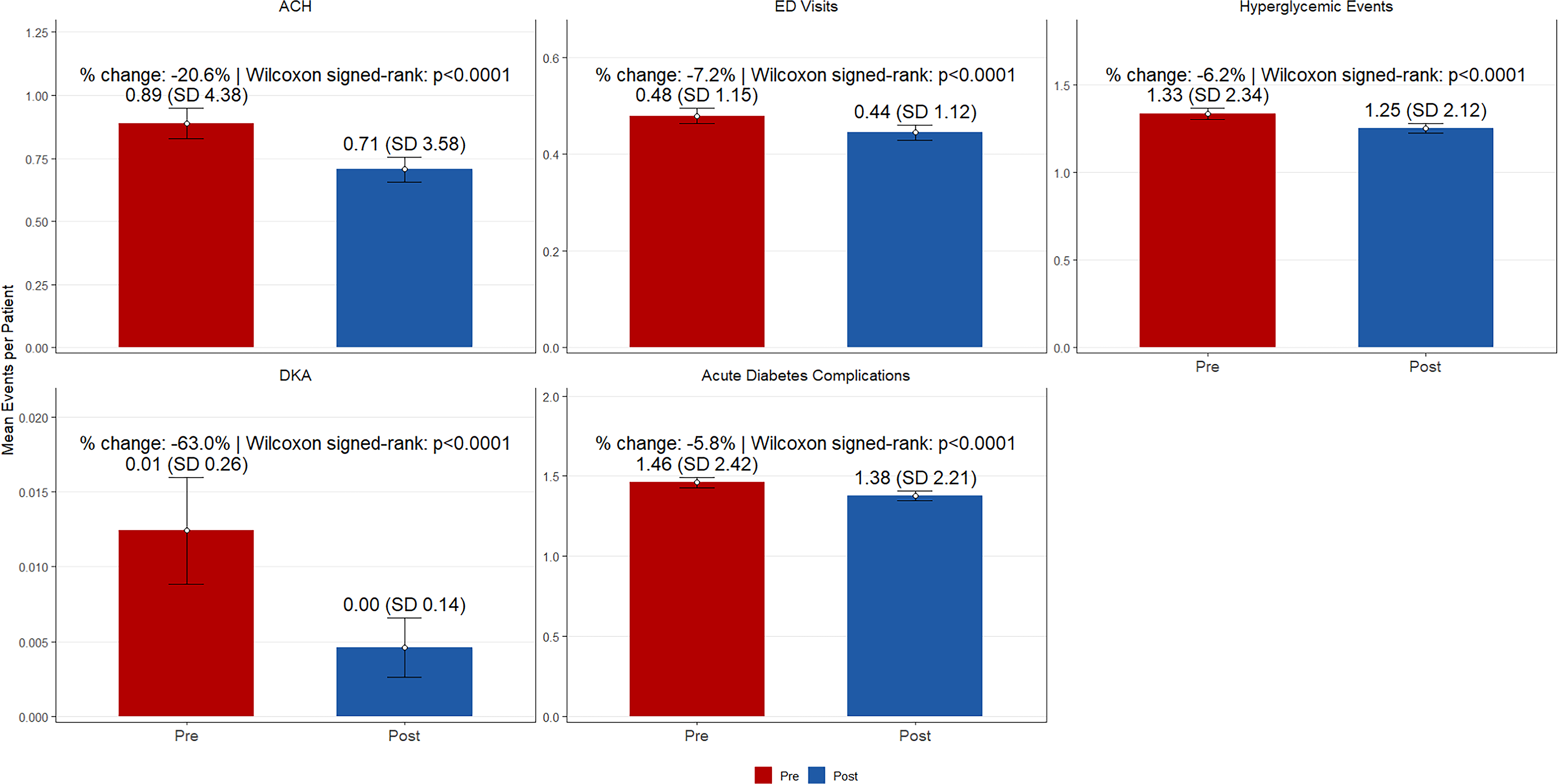
Pre–post comparison of acute care utilization and acute diabetes complications. Bars show the mean events per patient during the 12-month pre and 12-month post periods for each outcome. Error bars denote 95% confidence intervals around the mean. Values above bars report the mean (SD) for each period. Panel annotations display percent change from pre to post, calculated as (Meanpost−Meanpre)/Meanpre×100, and the paired t-test P value comparing post versus pre within individuals. Outcomes are plotted with free y-axis scaling to accommodate differing distributions. SD, standard deviation.
Significant reductions were also observed in patients with cardiovascular disease, ACH and ED visits decreased by 35% and 12%, respectively; in those with liver disease, by 25% and 13%; in those with renal disease, ACH decreased by 33%, and in those with hypertension, ACH and ED visits decreased by 26% and 7%, respectively. Commercially insured patients showed significant improvements, with a 41% decrease in ACH and a 7% reduction in ED visits. All reductions were statistically significant (P < 0.01).
Discussion
In this large-claims database analysis of adults with T2D treated with noninsulin therapies, we identified a significant association between device acquisition and reductions in ACH, ED visits, HGE, DKA events, and acute diabetes complications. These findings are notable given the relatively high number of patients with hypertension, pulmonary conditions, and cardiovascular disease.
Our findings align with results from a retrospective analysis that assessed the effects of FreeStyle Libre system use on acute diabetes complications and ACH in 10,282 adults with T2D treated with basal insulin or noninsulin therapies. 24 Utilizing the claims data from the MarketScan® databases, Miller et al. reported significant decreases in acute diabetes complications and ACH at 6 months postacquisition of the CGM device ([from 0.076 to 0.052 events/patient-year, P < 0.001] and [from 0.177 to 0.151 events/patient-year, P = 0.002], respectively). Similarly, Garg et al. conducted a retrospective cohort analysis using Optum’s de-identified Market Clarity® database to assess the impact of CGM on hospitalizations and glucose control in adults with T2D. 31 Among the 25,269 patients treated with noninsulin therapies, investigators reported significant reductions in ACH (−14.2%), acute diabetes complications (−33.6%), and ED treatment (−30.1%) events during the 6–12 months following acquisition of a CGM device. The noninsulin group also showed HbA1c reductions of 1.0%–1.4%, depending on the type and timing of medication changes.
Given the rising costs associated with suboptimally managed diabetes6,32 and its increasing prevalence, 33 reducing HCRU is critical to containing diabetes management costs for U.S. health systems. As discussed previously, the estimated cost of emergency department care, inpatient hospitalizations, and outpatient hospital visits associated with suboptimal diabetes management in the United States now exceeds $307 billion. 6 These expenses are compounded by the costs associated with the polychronic complications of persistent suboptimal glucose control.34–38
Our findings support expanding patient access to CGM within the broader T2D population. Currently, many health insurance plans and government payers deny CGM coverage to individuals with T2D who are managed with noninsulin medications. 39 Emerging evidence suggests that health plans may reconsider population eligibility criteria and utilization management requirements to include T2D patients receiving noninsulin therapies. In addition, the increasing reliance on telemedicine and digital diabetes technologies, driven by the COVID-19 pandemic, may further incentivize expanded coverage for CGM, which enables the capability to automatically transmit glucose data to health care providers via cloud-based software, facilitating interpretation, and remote diabetes treatment management decisions. 40 This functionality had demonstrated efficacy in delivering essential health care services during the COVID-19 pandemic 41 and demonstrated telemedicine with cloud-based CGM data as effective tools for diabetes care.
A key strength of our analysis was the use of claims data from a large dataset, which included 20,420 adults with T2D treated with noninsulin therapy. Moreover, the dataset provided reliable information about CGM acquisition, and the use of ICD-10 codes allowed us to accurately quantify HCRU and complications without reliance on patient-reported data.
Our study had several limitations. The observational design precluded the inclusion of a matched control group for comparison, which would have been possible in a randomized controlled trial. Consequently, we were unable to quantify differences in outcomes between CGM acquisition and continued use of traditional BGM or no monitoring. In addition, during the earlier years covered in the study, providers typically prescribed CGM to patients with higher perceived risk, worse symptoms, or higher engagement with their self-management. This could introduce selection bias; these patients were already more closely monitored or motivated. Because the Inovalon Insights claims dataset did not include HbA1c or CGM values, we could not draw correlations between potential improvements in glycemic status and reductions in HCRU. Furthermore, given the rarity of DKA in noninsulin-treated T2D and the very low baseline event counts in this cohort, the large relative reduction in DKA should be interpreted cautiously. Because the study captured only data about CGM acquisition, we cannot determine whether patients actually used their CGM devices or to what degree. Also, the dataset lacked information about patients’ socioeconomic characteristics and diabetes self-management education/training, all of which could influence outcomes. In addition, the study did not directly assess the impact of clinical history on physician prescribing behavior. Moreover, we were unable to determine whether patients continued to scan their devices or used glucose data for daily self-management. Finally, although the limited sample size of individuals aged 18–35 years with T2D may constrain the generalizability of our findings for this subgroup, the results are more broadly applicable to individuals aged 36–64 years, who represent the largest proportion of the T2D population.
Conclusions
This analysis demonstrated an association between CGM acquisition and reductions in HCRU in adults with T2D treated with noninsulin therapies. These findings are important as payers allocate premium dollars while balancing mounting costs related to care for patients with diabetes, especially direct costs for inpatient and outpatient treatments. Additional studies are needed to assess the frequency and persistence of CGM use within this population to determine its impact on longer term clinical outcomes. Data from these studies may add to our understanding of the feasibility and clinical utility of CGM within the broader T2D population and help guide clinicians in developing strategies that support personalized person-centered care.
Authors’ Contributions
B.S.B., Q.P., S.M., A.L., and A.K.S.: Conceptualization, original draft, and review and editing.
Footnotes
Acknowledgment
The authors wish to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for his editorial assistance.
Author Disclosure Statement
A.K.S. is an employee at UHC as a market CMO for Medicare and Retirement and the Chief Medical Advisor for Art Pharmacy. Neither UHC nor Art Pharmacy have provided any funding for this work. B.S.B., Q.P., S.M., and A.L. are employees of Abbott Diabetes Care.
Funding Information
Abbott Diabetes Care funded the development of this article.