
Abstract
Background:
Continuous glucose monitoring (CGM) systems predominantly rely on oxygen-dependent enzymatic electrochemistry. While their accuracy is well established in normoxic conditions, little evidence exists regarding their performance during hypoxia, a situation encountered during altitude exposure, air travel, or specific medical conditions. This study assessed the accuracy of two widely used glucose-oxidase CGM systems (FreeStyle Libre® and Dexcom G6®) during controlled hypoxia.
Methods:
In a randomized controlled study, healthy volunteers and participants with diabetes were exposed to standardized normobaric hypoxia (fraction of inspired oxygen of 14.5%). Participants simultaneously wore FreeStyle and Dexcom sensors. Venous plasma glucose, analyzed using the hexokinase method, served as the reference. To induce glycemic excursions, participants consumed a standardized mixed meal and performed moderate-intensity cycling exercise. The primary end point was the mean absolute relative difference (MARD) comparing CGM values with reference glucose. Secondary assessments included consensus error grid analysis (CEGA).
Results:
Thirty participants were included (15 healthy volunteers and 15 with diabetes). Median age was 29.5 (interquartile range [IQR]: 23.0–41.0) years, and median body mass index was 23.3 (IQR, 22.0–26.4) kg/m2. Among participants with diabetes, 53% had type 1 diabetes and 47% type 2, with a median diabetes duration of 16.3 [IQR, 11.3–21.6] years and HbA1c of 7.5% [IQR, 6.6–7.8]. During hypoxia MARD values were 21.2% for FreeStyle and 41.8% for Dexcom in healthy volunteers and 11.8% and 17.5%, respectively, in participants with diabetes. CEGA showed that 97% of FreeStyle and 87% of Dexcom readings fell within zones A or B during hypoxia.
Conclusions:
Both CGM systems showed reduced accuracy under hypoxia, particularly during dynamic glycemic changes. Awareness of these limitations and selective confirmation with capillary testing can assist safe use when clinically relevant decisions are required. The implications for automated insulin delivery systems warrant further dedicated evaluation.
Keywords
Introduction
Diabetes mellitus, characterized by chronic hyperglycemia, 1 is one of the most prevalent metabolic disorders worldwide. In 2021, approximately 537 million adults aged 20–79 years were living with type 2 diabetes (T2D), representing 10.5% of the global adult population. Without effective preventive measures, this number is projected to reach 783 million by 2045. 2
Glucose monitoring is useful for diabetes self-management and can be realized by capillary blood glucose or interstitial continuous glucose monitoring (CGM).3,4 Most of CGM devices available on the market (Abbott, Dexcom, and Medtronic Diabetes) rely on an enzymatic glucose oxidation reaction that generates an electrical potential difference detected by transcutaneous sensors, allowing continuous measurement of interstitial glucose concentrations.5–7
The use of CGM among patients with diabetes has grown substantially in recent years, transforming diabetes management for both patients and health care professionals. 8 Several studies have demonstrated that systematic CGM use improves glycemic control and reduces the risk of hypoglycemia in patients with type 1 diabetes (T1D) and T2D, particularly with the FreeStyle Libre® (FSL) and Dexcom® systems. 9 Heinemann et al. showed in their multicenter randomized controlled trial that Dexcom use, compared with self-monitoring, reduced hypoglycemic events by 72% in patients with T1D. 10 Regarding FSL, a number of meta-analysis of clinical trials and observational studies have shown a decrease in hypoglycemic episodes, despite a decline in glycated hemoglobin (HbA1c).11,12 In addition, the efficacy of closed-loop systems and the modification of insulin delivery based on CGM glucose data are contingent upon the accuracy and reliability of these data. The consequences of compromised accuracy and reliability of these systems may be severe, as they can lead to adverse medical outcomes.
Beyond diabetes care, CGM technology has recently been adapted for sports performance monitoring. Since 2020, devices such as the Supersapiens Libre Sense biosensor (Abbott Laboratories) have been made available for elite and recreational athletes, enabling real-time tracking of glucose dynamics to optimize energy management during physical activity. 13
Whether used by patients with diabetes or by athletes, CGM devices are typically designed and validated under normoxic conditions.14,15 However, hypoxic environments, characterized by reduced oxygen partial pressure or impaired tissue oxygenation, may arise during altitude exposure (mountain stay), during flight, or in medical conditions such as chronic respiratory or cardiac disease. This is notably the case in patients with hemoglobinopathies or conditions affecting red blood cell turnover, where clinicians rely more heavily on CGM-derived metrics to assess glycemic control and guide therapeutic decisions. 16 In such settings, the limited availability of dissolved oxygen can potentially alter the dynamics of the enzymatic reactions upon which most CGM sensors depend, resulting in biased or attenuated sensor readings (e.g., underestimation of glucose). 17 Moreover, conditions like acute mountain sickness (AMS) manifest with symptoms such as headache, fatigue, nausea, and dizziness, which overlap substantially with those of hypoglycemia, thus complicating clinical interpretation. 18 Therefore, assessing CGM accuracy under induced hypoxia is essential to ensure the validity of their use in such challenging physiological contexts.
To assess the impact of hypoxia on the precision of CGMs in everyday, recreational or medical conditions to provide the best possible care to patients living with diabetes, we evaluated the performance and calibration accuracy of two CGM systems—FSL and Dexcom—under induced hypoxia in participants with diabetes and healthy volunteers.
Material and Methods
Study design
We performed a double-arm randomized clinical study to assess the accuracy of the FreeStyle (FSL-CGM) and Dexcom (Dexcom-CGM) devices in comparison with hexokinase (HK) plasma glucose measurements under hypoxic conditions among healthy volunteers and participants with diabetes (primary objective).
The secondary objectives were to assess the concordance between interstitial and venous plasma glucose values obtained with each CGM device during hypoxia in both healthy volunteers and participants with diabetes and to analyze sensor-related adverse effects. Additional objectives were to evaluate tolerance to acute hypoxia induced by the hypoxic chamber (14.5% of fraction of inspired oxygen [FiO2]) and to assess the safety of hypoxia exposure based on the occurrence of adverse events.
The study was conducted at the Clinical Investigation Center CIC1402, Poitiers University Hospital (Poitiers, France), with a controlled normobaric hypoxic chamber built in 2019 in our center.
Participants were enrolled between May 2022 and November 2024. The study was conducted in accordance with Good Clinical Practice and the principles of the Declaration of Helsinki. The protocol was approved by the Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM) (n°ID RCB2021-A01611-40) and the Sud Méditerranée I Ethics Committee. All subjects provided written informed consent before enrollment in the study (ClinicalTrials.gov identifier: NCT05144802).
Participants
The inclusion criteria for healthy volunteers were as follows: (1) aged 18–40 years; (2) no history of diabetes; (3) not taking any medication, including systemic corticosteroids; and (4) a body mass index (BMI) between 18.5 and 29.9 kg/m2.
The inclusion criteria for participants with diabetes were as follows: (1) aged 18–75 years; (2) T1D or T2D, as defined by the American Diabetes Association 1 ; (3) absence of diabetes chronic complications, defined as neuropathy, coronary artery disease, peripheral arterial disease, or proliferative retinopathy; (4) stable antidiabetic treatment for at least the previous 3 months; and (5) no contraindications to the use of contrast agents or radiotracers for either coronary CT angiography or myocardial stress scintigraphy.
The main noninclusion criteria for all participants were as follows: (1) history of respiratory disease, notably asthma or respiratory allergies; (2) major cardiovascular events within the past 3 months (including myocardial infarction, unstable angina, or significant arrhythmias); (3) current smoking; and (4) anemia (Hb < 12 g/dL). In addition, women were required not to be pregnant or breastfeeding and to have effective contraception.
Participants were excluded if they had resting peripheral oxygen saturation (SpO2) below 95%, decompensated heart failure, estimated glomerular filtration rate < 45 mL/min/1.73 m2, Hb < 12 g/dL, or severe hypertension (≥180/110 mmHg). Participants were also excluded if they had known allergies to the sensors or skin lesions at the sensor insertion sites. Additional exclusion criteria included a history of severe AMS and any condition judged by the investigator to compromise participant safety.
During the screening period, participants with diabetes underwent noninvasive coronary assessment (coronary CT angiography or myocardial stress scintigraphy for participants over 70 years) and pulmonary function testing. Participants were excluded if they had obstructive or restrictive ventilatory disorders, thoracic distension, or coronary or myocardial abnormalities.
Study procedure
Pre-exposure procedures
Participants attended the Clinical Investigation Center after an overnight fast. Upon arrival, a clinical examination was performed, including measurement of heart rate and blood pressure in the seated position. Continuous monitoring of SpO2 was initiated by pulse oximetry.
Both CGM sensors from the two systems were randomized in a 1:1 ratio and inserted simultaneously for each participant 2 h before hypoxic exposure (Group 1: FSL-CGM on the right arm and Dexcom-CGM on the left arm; Group 2: opposite configuration). Sensors were calibrated according to the manufacturers’ instructions when required.
The randomization process was centralized. The randomization list was generated by the study’s methodologist (S.R.), who maintained its confidentiality. This dynamic randomization was carried out online and was centralized, accessible to investigators via a personal username and password.
A venous catheter was inserted for repeated blood sampling, and baseline blood samples were collected before hypoxic exposure.
Exposure protocol
Participants were exposed for 3 h to normobaric hypoxia with an inspired oxygen fraction of 14.5% (Supplementary Fig. S1).
At T0, participants entered the hypoxic chamber. A standardized breakfast containing 60 g of carbohydrates was provided. Participants with diabetes administered their insulin doses as usually prescribed with no modification of their dosage. Continuous SpO2 (Saturometre Berry Pulse Oximeter, Berry Electronic Tech Co., Ltd., 1188 Lianhang Road, Shanghai) monitoring was maintained throughout the exposure. Venous and interstitial glucose concentrations were measured every 15 min during the entire protocol, resulting in a total of 13 measurement time points. Venous blood glucose was analyzed using the reference enzymatic HK method, 19 with fluorinated tubes used to limit intraerythrocytic glycolysis. From T0 to 90 min, participants remained at rest. From T90 to 120 min, participants performed a 30-min exercise session on a cycle ergometer at 60% of their age-predicted maximal heart rate (HRmax = 220 − age) to induce glycemic variability. Heart rate and cardiac rhythm were continuously monitored using a 3-lead electrocardiogram (BIOPAC mo 150, BIOPAC Systems, Inc. AcqKnowledge Software [Version 4.4]), and exercise intensity was adjusted accordingly to maintain the target heart rate. From T120 to 180 min, participants returned to a resting state.
The 2018 Lake Louise Acute Mountain Sickness score 20 was administered three times hourly throughout the exposure.
Safety procedures
All adverse events were prospectively recorded. Predefined safety criteria included clinical monitoring and interruption of exposure in the event of significant symptoms or intolerance to hypoxia.
Outcomes
CGM accuracy was assessed using both analytical and clinical metrics. Analytical accuracy, considered the primary end point, was quantified using the mean absolute relative difference (MARD) and the mean absolute difference between CGM values and reference venous glucose measurements. MARD was reported for the entire range of HK values and according to HK quintiles: <75 mg/dL, 75–89 mg/dL, 90–132 mg/dL, 133–209 mg/dL, and > 209 mg/dL.
Clinical accuracy was evaluated using the consensus error grid analysis (CEGA). The CEGA classifies paired CGM and reference glucose values into five zones (A to E) according to their potential impact on clinical decision-making. Zone A includes values that are clinically accurate or would lead to correct treatment decisions. Zone B includes values that are outside strict analytical accuracy limits, but would result in benign or no clinically significant treatment errors. Values falling within zones A and B are generally considered clinically acceptable. Zones C, D, and E represent increasing degrees of potential clinical risk due to inappropriate or dangerous treatment decisions. In accordance with current recommendations, CGM performance was considered clinically acceptable when most paired values were located within zones A and B of the CEGA.
Safety was evaluated based on the occurrence of any adverse event. Hypoxia tolerance was assessed using SpO2 and the Lake Louise score. Severe AMS was defined as a Lake Louise score > 3. 20
Statistical analysis
This pilot study addresses the lack of existing data on the impact of hypoxic conditions on medical device measurements. Consequently, no a priori power calculation was feasible, and a sample size of 30 participants was chosen in accordance with recommendations for pilot studies.21,22 Results are expressed as mean ± standard deviation or standard error of the mean, or median (interquartile range [IQR]) for normally and non-normally distributed data, respectively. A mixed model was used to analyze sensor side effects with subjects as a random effect and the interaction between the device and the side as a fixed effect. Values measured by each CGM were compared with venous blood glucose values using a mixed model with subjects as a random effect and measurement method as a fixed effect. The Wilcoxon signed-rank test was applied to compare paired differences between methods at different time points. A Pearson correlation was utilized to ascertain the correlation between the difference between CGM and HK and SpO2. A significant level of 5% (two-sided) was used. All statistics were obtained without imputation and performed using R version 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism version 10.6.0 (GraphPad Software, San Diego, CA, USA).
Results
A total of 40 participants were enrolled, including 30 available for analysis: 15 participants with diabetes and 15 healthy volunteers (Fig. 1). The characteristics of the study population are presented in Table 1. Participants (53% male) had a median age of 30 (IQR, 23–41) years and a median BMI of 23 [IQR, 22–26] kg/m2. Participants with diabetes (53% type 1 and 47% type 2) had a median diabetes duration of 16 [IQR, 11–22] years and a median HbA1c of 7.5 [IQR, 6.6–7.8]%.
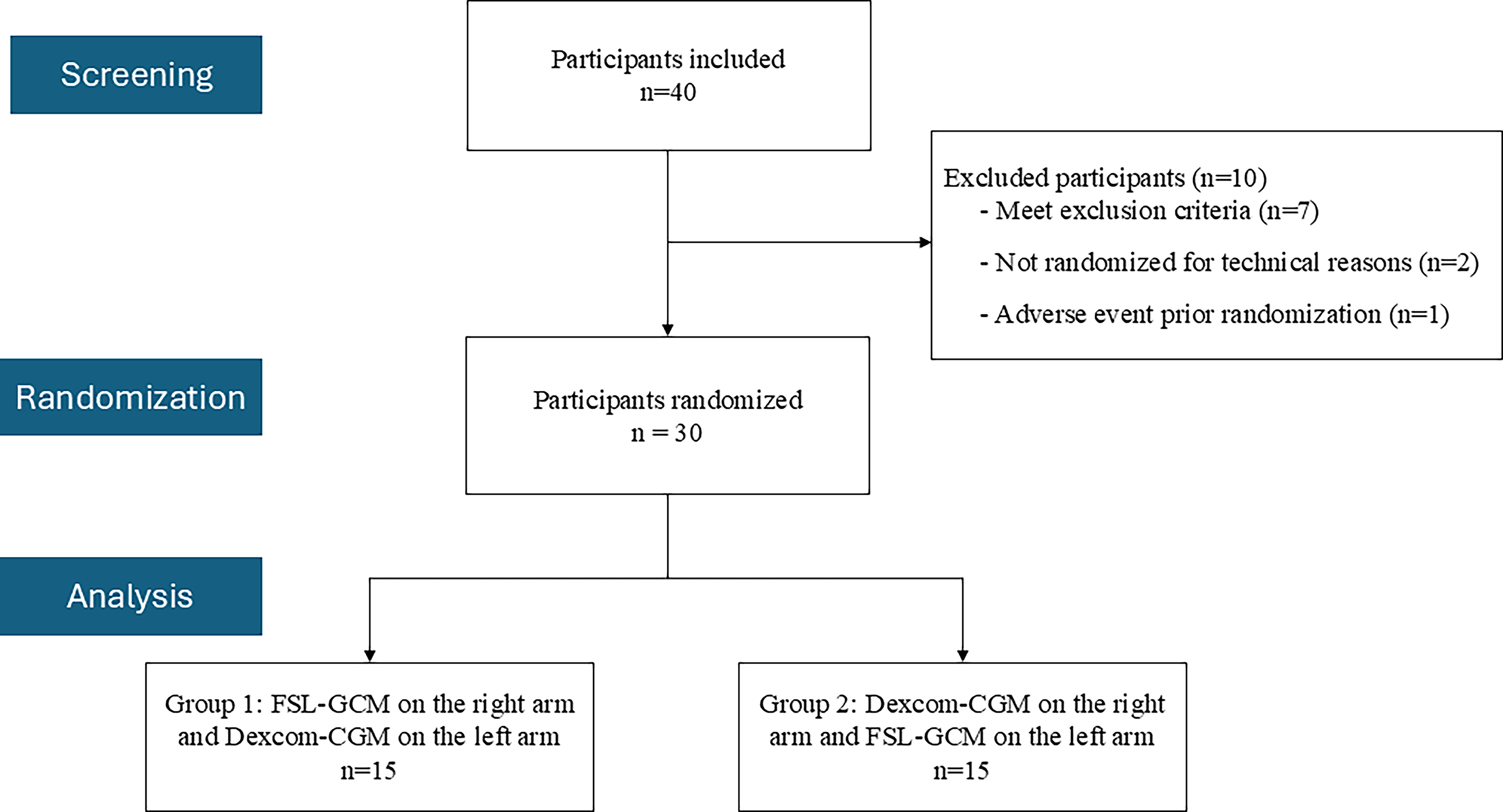
Flowchart of the study. Dexcom-CGM, Dexcom G6; FSL-CGM, FreeStyle Libre 2.
Baseline Characteristics
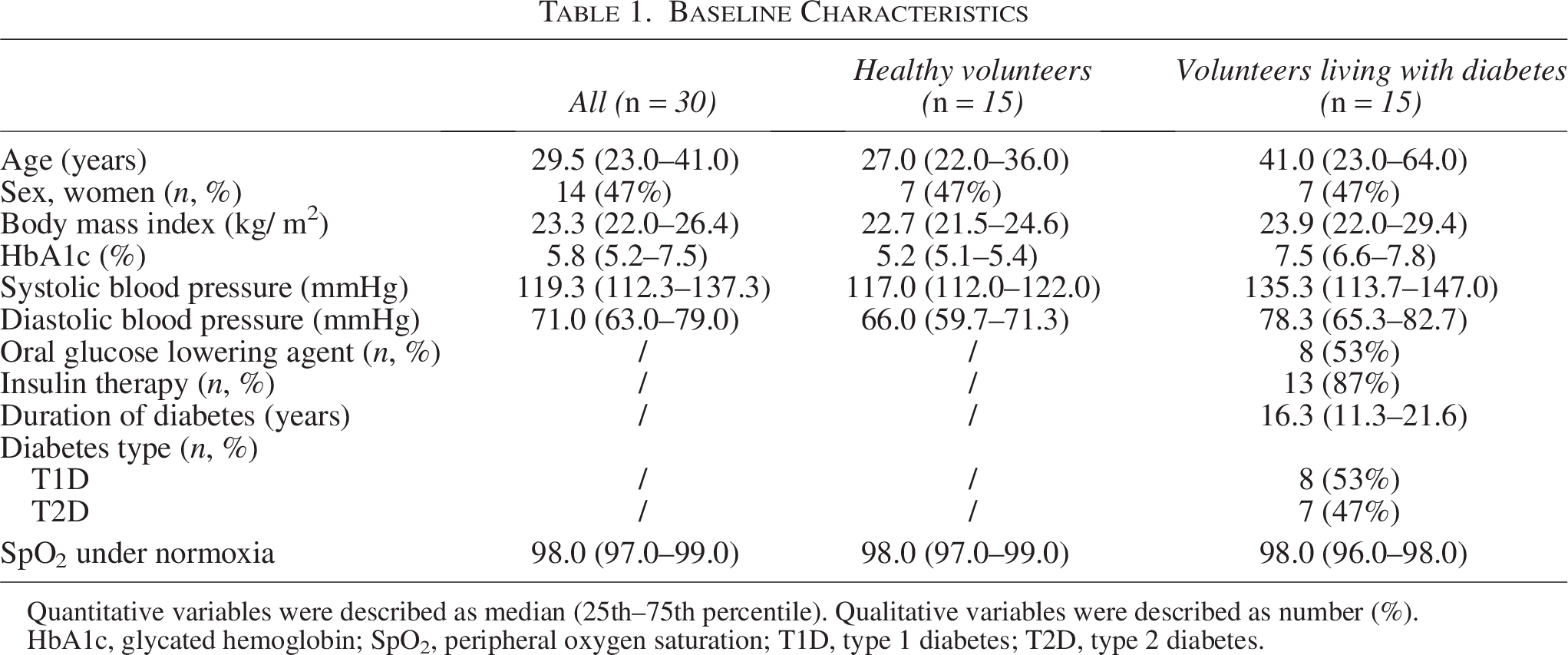
Quantitative variables were described as median (25th–75th percentile). Qualitative variables were described as number (%).
HbA1c, glycated hemoglobin; SpO2, peripheral oxygen saturation; T1D, type 1 diabetes; T2D, type 2 diabetes.
As anticipated, HK measurements showed a gradual increase in blood glucose levels after the meal (between 0 and 90 min) corresponding to the postprandial phase. This was followed by a decrease during the cycling period and subsequent stabilization until the end of the observation period (Supplementary Table S1). Similar trajectories were observed with both CGM systems (Fig. 2). During the experiment, mean venous glucose concentration and coefficient of variation were 192.5 mg/dL and 33% for participants with diabetes and 79.1 mg/dL and 20% for healthy volunteers (Table 2).
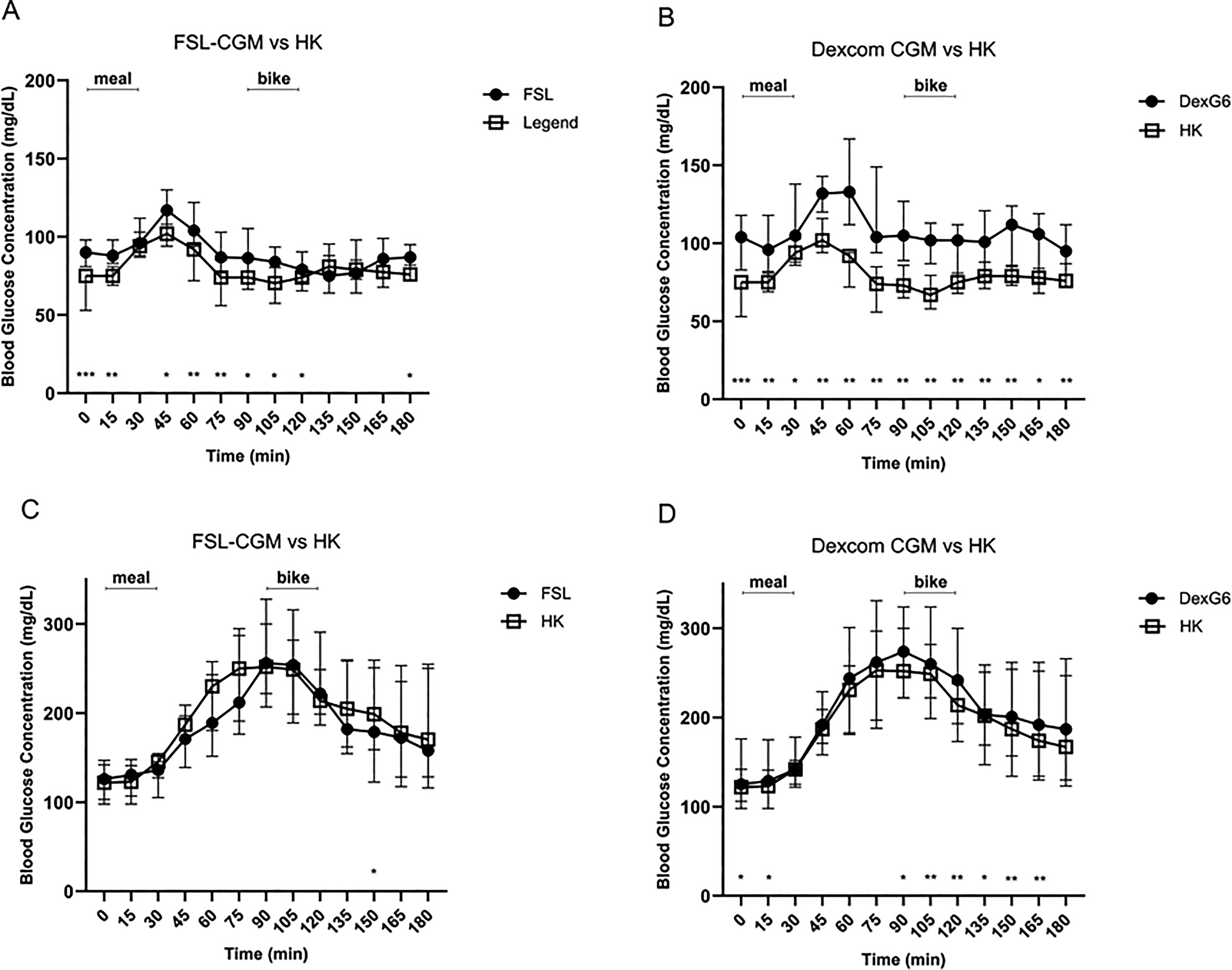
Comparison of FSL-CGM versus venous concentrations and Dexcom-CGM versus venous concentrations for healthy volunteers and patients with diabetes. Dexcom-CGM or DexG6, Dexcom G6; FSL-CGM or FSL, FreeStyle Libre 2; HK, hexokinase. Glucose concentrations were presented as median and interquartile Q1 and Q3.
Average Blood Glucose Levels and Variation Coefficient According to Participant Group (Healthy Volunteers or Patients with Diabetes) and Blood Glucose Measurement
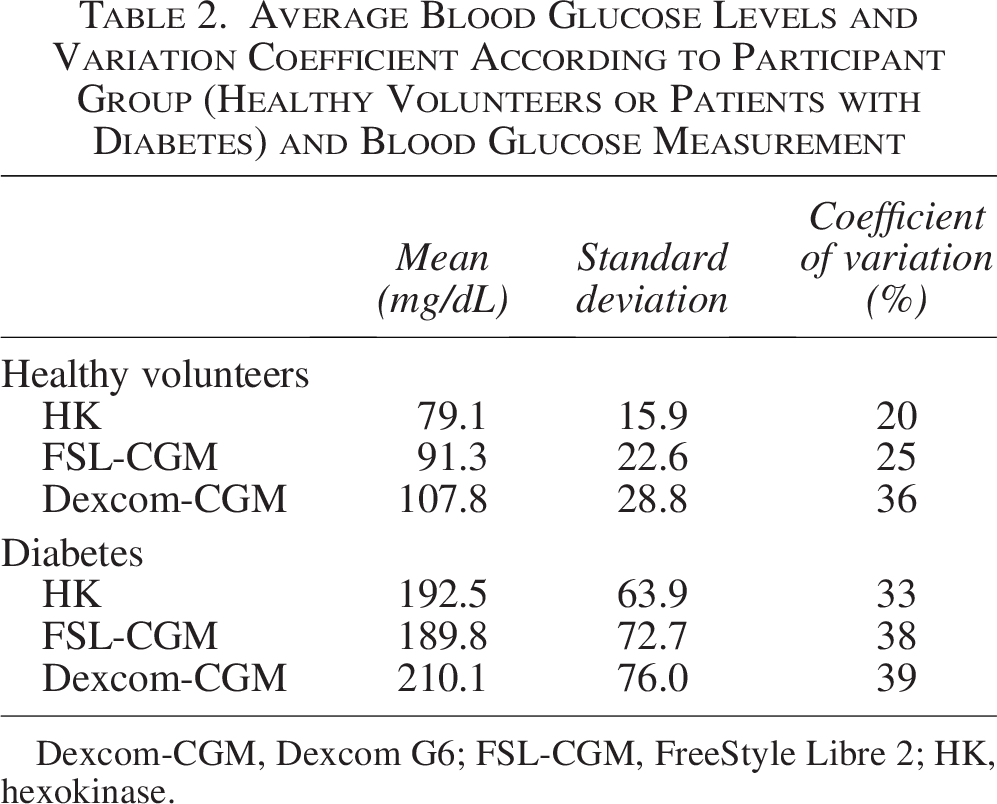
Dexcom-CGM, Dexcom G6; FSL-CGM, FreeStyle Libre 2; HK, hexokinase.
No statistical effect of sensor placement side was found, either on the difference between venous and FSL-CGM values (P = 0.52) or between venous and Dexcom-CGM values (P = 0.32). Therefore, a global analysis was performed.
FreeStyle Libre-continuous glucose monitoring
Glucose concentrations measured by FSL-CGM were statistically different from HK values in the healthy volunteer group at nine time points and only at one time point (150 min) in the diabetes group (P < 0.05) (Fig. 2A,B). The median individual MARD was 16.8 (IQR, 9.9–21.7)%, 11.8 (IQR, 6.5–17.6)%, and 21.2 (IQR, 16.6–37.9)% for all participants, participants with diabetes, and healthy volunteers, respectively. MARD between FSL-CGM and HK did not change over time (P = 0.11; Fig. 3). For FSL-CGM, the percentage of results in zone A of the CEGA was 76% and 97% for zones A and B (Fig. 4). When considering HK quintiles, FSL-CGM values were statistically higher than HK for the 2 lowest quintiles (glucose from <75 to 89 mg/dL) but not different for values ≥ 90 mg/dL (Table 3). There was no correlation between the FSL-CGM and HK difference and SpO2 (P = 0.02).
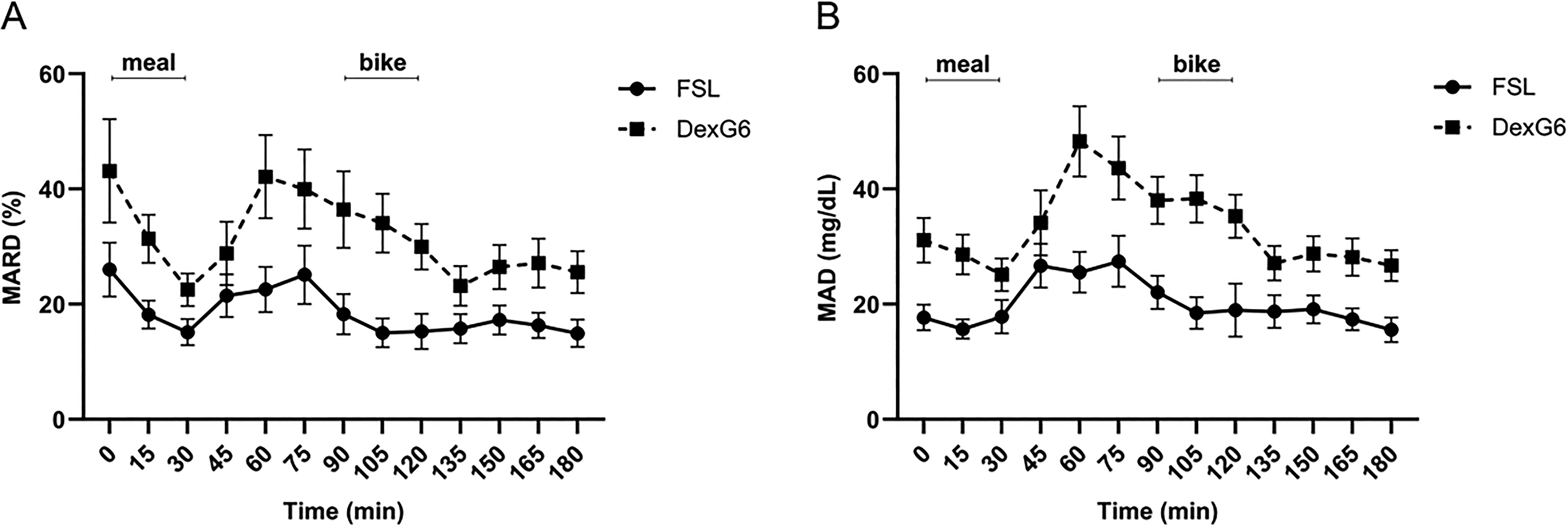
Mean absolute relative difference (MARD) and mean absolute difference (MAD) between FSL-CGM and HK and between Dexcom-CGM and HK. Bars indicate SEM.
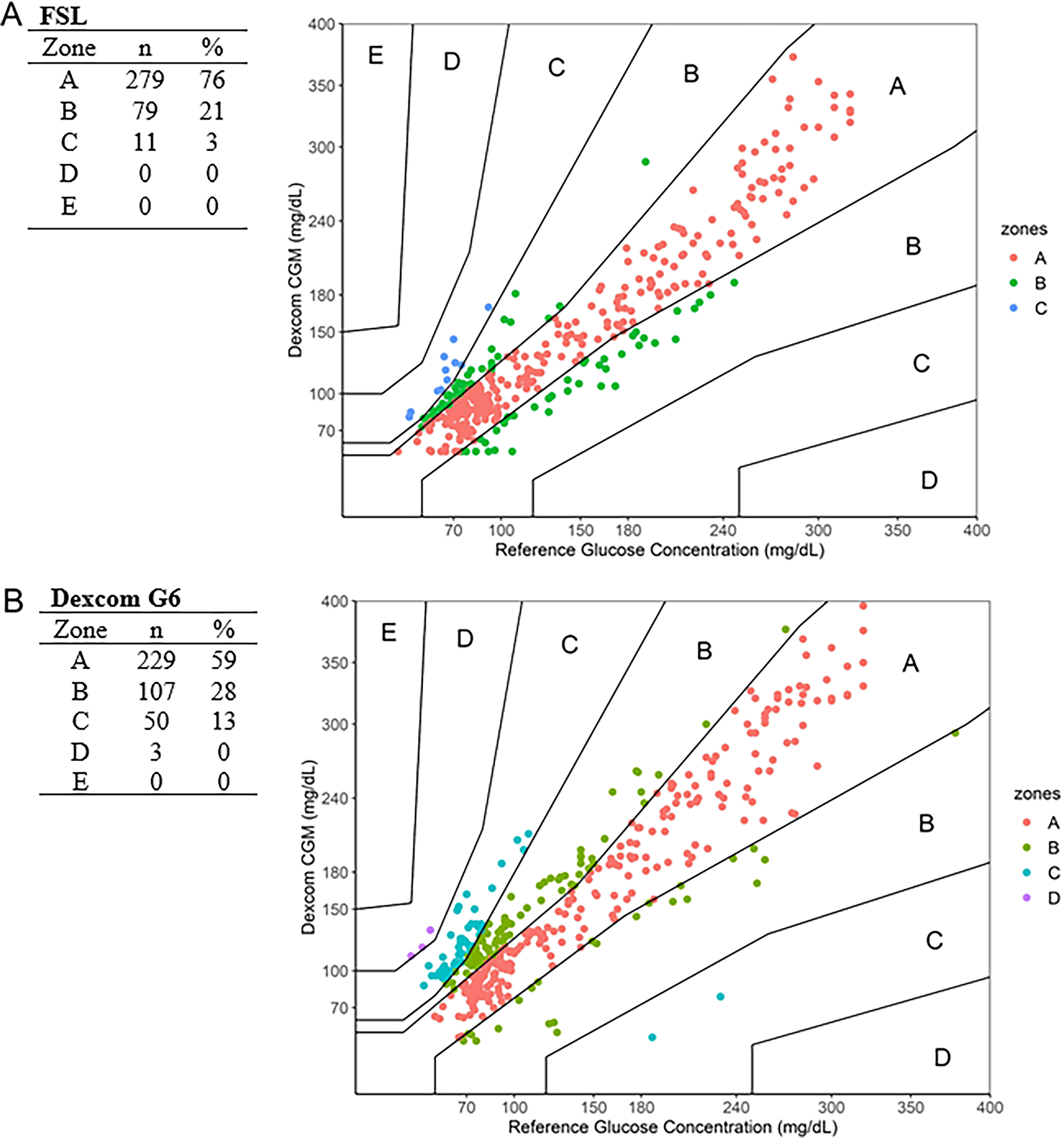
Consensus error grids analysis plot for CGM versus HK comparator glucose values. CGM: continuous glucose monitoring.
Glucose Measurement Data at Various Concentrations

SD, standard deviation; MAD, mean absolute difference; MARD, mean absolute relative difference.
Dexcom-CGM
For healthy volunteers, all glucose concentrations measured by Dexcom-CGM were statistically higher than HK (P < 0.05) (Fig. 2C). Among participants with diabetes, Dexcom-CGM glucose values were statistically different from HK at 8 out of 13 time points (Fig. 2D). The median individual MARD was 23.9 (IQR: 17.0–41.8)%, 17.5 (IQR: 14.3–23.5)%, and 41.8 (IQR: 26.9–69.7)% for all participants, participants with diabetes, and healthy volunteers, respectively. MARD between Dexcom-CGM and venous glucose did not change over time (P = 0.13; Fig. 3). For Dexcom-CGM, the percentage of results in zone A of the CEGA was 59% and 87% for zones A and B (Fig. 4). Dexcom-CGM values were consistently and statistically higher than HK over all HK quintiles (Table 3). There was no correlation between the Dexcom-CGM and HK difference and SpO2 (P = 0.1).
Safety
SpO2 in normoxia was 98.0 (IQR: 97.0–99.0)%, dropped to 91.0 (IQR: 88.0–92.0)% in hypoxia exposure, and returned to 98.0 (IQR: 97.0–99.0)% 1 h after hypoxia (Fig. 5). Hypoxia was well tolerated, and no participant experienced an episode of AMS (Lake Louise Score < 3 throughout).
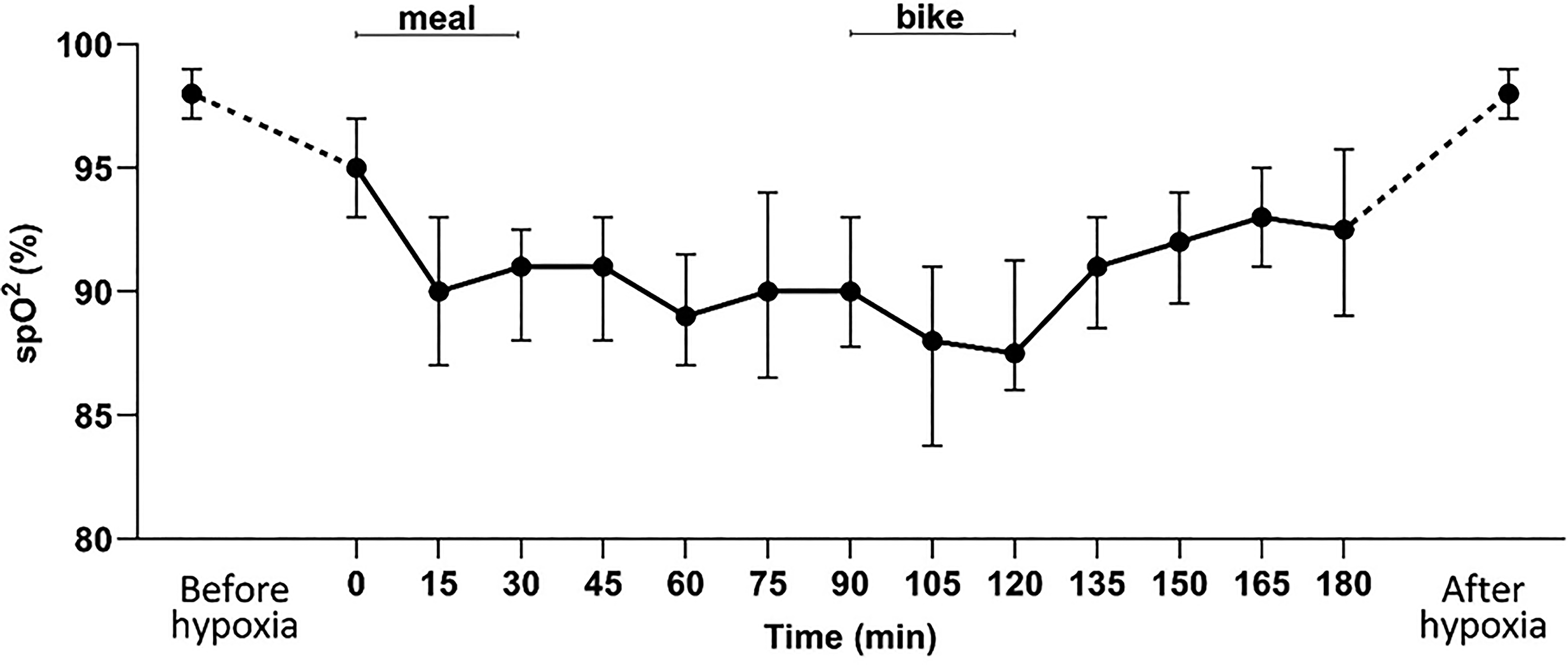
Arterial blood oxygen saturation over time. Values were presented as median and interquartile Q1 and Q3.
Two severe adverse events were recorded (one road traffic accident and one domestic accident). Both occurred before randomization, preventing one of the participants from being randomized.
Real-time glucose data were available for 94.9% (370/390) and 100% (390/390) for FSL-CGM and Dexcom-CGM, respectively (Supplementary Table S1). Twenty brief sensor disconnections occurred in six participants, resulting in 20 data points lost with the FSL-CGM and none for the Dexcom-CGM.
Discussion
The FOX study is the first randomized clinical trial to assess the accuracy of CGM systems (i.e., FSL 2 and Dexcom G6) under controlled normobaric hypoxic conditions in both healthy volunteers and participants with diabetes. The MARD found in our study for FSL-CGM was 21.2% for volunteers and 11.8% for participants with diabetes. For Dexcom-CGM, the MARD was 41.8% and 17.5% for volunteers and for participants with diabetes, respectively. Furthermore, 97% of values were classified as zone A or B in the CEGA for FSL-CGM and 87% for Dexcom-CGM.
Compared with the accuracy data reported under normoxic conditions, a marked gap becomes evident. In a cohort of 144 adults with diabetes (91% of whom had T1D, 9% of T2D) who were equipped with a FSL 2, the MARD was 9.3% and 99.9% of data in zones A and B of the CEGA. 23 In an interventional study of 23 patients with T1D, the MARD under standardized conditions with breakfast provided at the research center was 10.9% for the FSL 1. 24 A study involving 218 hospitalized patients with diabetes found a MARD of 12.8% for the Dexcom G6. 25 In a study of 134 adults with diabetes, a MARD of 9.9% for the G6 was found. 26
The absence of significant correlation between level of SpO2 and HK-CGM difference in our study makes us consider that even small modification of saturation may have a real impact on device accuracy. These findings are consistent with previous observations reported by Gautier et al., who demonstrated reduced accuracy of blood glucose monitoring systems based on glucose-oxidase technology at simulated altitudes above 2000 m in a hypobaric chamber. 27
Despite the existence of environmental or medical conditions that can result in a decrease in tissue oxygen, existing literature on the accuracy of CGM in hypoxia is, to the best of our knowledge, limited. A study in rats sought to develop a CGM device without the use of oxygen-dependent enzymes to improve the accuracy of such devices in hypoxia exposure. 17 However, despite the improved accuracy of this experimental CGM in hypoxia in rats—never developed for human purpose—the only systems currently available for reimbursement remain enzyme-dependent CGMs.
Hypoxia is a prevalent clinical concern in the context of hospitalization in intensive care. In a scoping review, Nielsen et al. found a wide range of MARDs (6%–30.5%) and CEGA distribution in AB zones from 92.1% to 100% for the CGMs used in our study. 28 In another study of 86 patients hospitalized in cardiothoracic intensive care following cardiac surgery, the MARD of FreeStyle compared with venous blood glucose was 18.2% with 98.1% of values in zones A and B of the CEGA, even though there was no report of hypoxia measure in these patients at the time of blood glucose testing. 29
Despite the ISO 15197:2013 standard establishing accuracy criteria for capillary blood glucose meters, with 95% of values required to be within ± 15 mg/dL of the reference glucose for blood glucose levels < 100 mg/dL or within ± 15% for blood glucose levels ≥ 100 mg/dL, 30 recent studies primarily rely on MARD. In this context, Davila-Ruales et al. propose an acceptable MARD threshold of < 10%–12%. For a “clinical” analysis, the authors propose the CEGA as a suitable instrument, with a minimum of 99% in zones A + B. 31 In our study, although CGM performance met these criteria under normoxic conditions, accuracy validation thresholds were not reached during normobaric hypoxia.
Our hypothesis was based on a decrease in enzymatic activity of oxygen-dependent CGM sensors. Indeed enzymatic electrochemical CGM sensors rely on glucose oxidase, an oxygen-dependent catalyst, and hypoxia can limit local oxygen availability in the interstitial fluid, thereby constraining the enzymatic reaction and altering the dynamics of the sensor signal amplitude.17,32,33 Reduced peripheral perfusion, which commonly accompanies acute hypoxia, may further modify interstitial glucose dynamics, exacerbating discrepancies between capillary or arterial glucose and the values measured by the sensor. Changes in skin blood flow, tissue oxygenation, or interstitial fluid turnover have all been shown to influence CGM accuracy, although data specifically addressing these mechanisms during experimentally controlled hypoxia remain scarce.34,35 To the best of our knowledge, no study has directly quantified the relative contribution of each mechanism, but the combination of impaired tissue oxygenation and altered perfusion likely plays a central role in the decreased accuracy observed in our study.
More broadly, several alternative glucose-sensing technologies based on optical or spectroscopic properties of glucose and not relying on enzymatic reactions have been described, although most remain investigational or are not widely available for clinical use.36,37 Their evaluation under hypoxic conditions could represent an important direction for future studies, especially in normoglycemic individuals in whom relative error metrics such as MARD are particularly sensitive to small absolute deviations.
These mechanisms may also be relevant to other known sources of CGM inaccuracy, such as compression artifacts, where local reductions in tissue perfusion and oxygenation, alongside changes in pH and interstitial fluid turnover, have been proposed as contributing factors. 37
Sensor accuracy was not influenced by the insertion side (left vs. right). Importantly, all sensors were inserted exclusively on the upper arm. According to the manufacturer’s instructions, the FSL is approved for arm placement only, whereas the Dexcom is approved for both arm and abdominal use in adults. 38 We chose to position CGMs only on the arm for simplicity and practical reasons, especially since Dexcom’s accuracy was similar for the arm and the abdomen. 39
An important finding of the FOX study is the higher MARD values observed in healthy volunteers compared with participants with diabetes. Several hypotheses may account for these differences. In the diabetes group, glycemic excursions are typically larger than in healthy volunteers, which may reduce the relative error expressed as MARD.40,41 It is therefore hypothesized that this discrepancy may be attributable to the significantly lower glucose levels observed in healthy volunteers. Furthermore, CGM calibration algorithms are generally developed and validated in populations with diabetes, a design choice that could favor performance in this group relative to normoglycemic individuals subjected to experimental protocols.15,42,43
Our study has several strengths. First, it is the inaugural study to assess accuracy of CGMs under controlled hypoxic conditions using the hypoxic chamber at the Inserm Clinical Investigation Center. This equipment provides optimal conditions for studying human physiology with few material limitations. The chamber is more convenient than a hypobaric chamber or a hypoxic tent, and it is generally better tolerated by patients. This facilitates human exploration with fewer constraints. This study evaluated CGMs in people with diabetes as well as in healthy individuals, addressing the challenges of the increasing use of blood glucose monitoring in everyday life during physical activities or among athletes.
Our study also has some limitations. The study population is limited to 30 participants (15 healthy volunteers and 15 participants with diabetes). While the exposure to hypoxia was designed to be 14.5% FiO2 (corresponding to the oxygen availability observed at approximately an altitude of 3000 m), 44 which is a realistic condition that can be experienced during air travel or mountaineering, we did not measure direct tissue hypoxemia; choosing to assess this parameter using transcutaneous oxygen saturation. However, for the same hypoxia exposure, there may be different adaptability mechanisms in place to preserve tissue oxygenation, which we thus cannot assess, and this may introduce bias. We exposed participants to acute 3-h hypoxia. However, saturation measured by transcutaneous oxygen saturation evidenced that dropped oxygenation in tissue happened within the first 10 min. Finally, the relatively small sample size must be acknowledged, and despite increased MARD values under hypoxia, absolute glucose readings generally remained within ranges likely sufficient for most routine clinical decisions, particularly when interpreted alongside clinical context.
The potential reduction in CGM accuracy during hypoxia may have important real-world implications. People with diabetes who travel to high altitudes, engage in sports at elevation, or experience intermittent hypoxia during air travel may encounter conditions similar to those reproduced in this study. 45 Likewise, patients with chronic respiratory disorders such as sleep apnea, cardiovascular disease, or critical illness may also be exposed to varying degrees of hypoxia that could influence sensor performance. 46 In these contexts, CGM values may require additional verification using capillary or venous glucose measurements, particularly when therapeutic decisions depend on precise glucose estimation. 47
Of particular concern are automated insulin delivery systems operating in closed-loop configurations, in which insulin dosing decisions rely directly on CGM-derived glucose values. Even modest, transient inaccuracies in glucose sensing under hypoxic conditions could potentially lead to inappropriate insulin delivery if not adequately accounted for by the control algorithms.
Subsequent studies are required, using larger sample sizes and evaluating the accuracy of CGMs utilizing enzymatic methods and alternative systems.
In conclusion, normobaric hypoxia significantly reduces the accuracy of both Dexcom and FreeStyle CGM systems, particularly in normoglycemic individuals. These findings highlight the need for further studies specifically designed to evaluate the performance and safety of closed-loop systems under hypoxic conditions. Such investigations should assess both sensor accuracy and algorithm robustness to ensure reliable glycemic control in low-oxygen environments and to mitigate the risk of maladaptive insulin dosing.
Authors’ Contributions
N.B.L.: Investigation, writing—original draft, review and editing, and visualization; C.R.: Investigation and writing—review and editing; C.F.: Writing—review and editing; E.R.: Project administration and writing—review and editing; L.D.: Data curation, methodology, validation, formal analysis, visualization, and writing—review and editing; C.B.: Writing—review and editing; S.R.: Conceptualization and writing—review and editing; S.H.: Conceptualization and writing—review and editing; H.M.: writing—review and editing; X.P.: Investigation and writing—review and editing; B.A.: Investigation and writing—review and editing; R.T.: Investigation and writing—review and editing; and P.-J.S.: Conceptualization, investigation, supervision, writing—original draft, writing—review and editing, and visualization.
Footnotes
Acknowledgments
The authors are grateful to all participants for their time and commitment to the study. The authors thank Sabine Souchaud, MSc, for her valuable contribution to the organization of the study and for her help in drafting the study protocol. The authors also acknowledge Jimy Gotzamanis, PharmD, for his involvement in the conduct of the investigations and data acquisition. The authors further thank the staff of the Clinical Research and Innovation department of Poitiers University Hospital, and particularly Ms. Ferrand Rigallaud, for their support and assistance with regulatory and administrative aspects of the study. The authors would also like to extend their gratitude to the staff at the clinical investigation center, the nurses and nursing assistants, and the clinical research assistants for their involvement in this study. The authors also want to thank the CRB Poitiers—BB0033-0068 (Sonia Brishoual, Michelle Grosdenier-Bruneau). The authors acknowledge the use of the hypoxia chamber platform (University of Poitiers/CHU de Poitiers), supported by institutional funding and co-funded within the CPER-FEDER framework by the French Government, the Nouvelle-Aquitaine Regional Council, and the European Union (European Regional Development Fund, ERDF).
Author Disclosure Statement
P.-J.S. has served on advisory boards and received consulting fees from Novo Nordisk and has received travel support from SANOFI and speaking honoraria from AstraZeneca. X.P. has served on advisory boards and received consulting fees from Novo Nordisk and speaking honoraria from AstraZeneca, Sanofi, Lilly, and Abbott. S.H. has received grants from Asdia, AstraZeneca, LVL, Nestle Homeperf, ISIS Diabète, Pierre Fabre, and VitalAire; consulting fees from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Sanofi, Servier, and Valbiotis; payment or honoraria from Abbott, AstraZeneca, Boehringer Ingelheim, Bayer, Dino Santé, Eli Lilly, Novartis, Novo Nordisk, Pierre Fabre, Sanofi, Servier, and Valbiotis; and support to attend meetings from AstraZeneca, Abbott, Dino Santé, Eli Lilly, and Novo Nordisk. All other authors declare no potential conflicts of interest relevant to this article.
Funding Information
This study was sponsored by the Poitiers University Hospital (CHU de Poitiers). No financial support was provided by the manufacturers of the medical devices used in this study (Abbott and Dexcom). All devices were purchased commercially from the manufacturers using institutional funds from CHU de Poitiers. The manufacturers had no role in the study design, data collection, data analysis, data interpretation, or article preparation.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.