
Abstract
Objective:
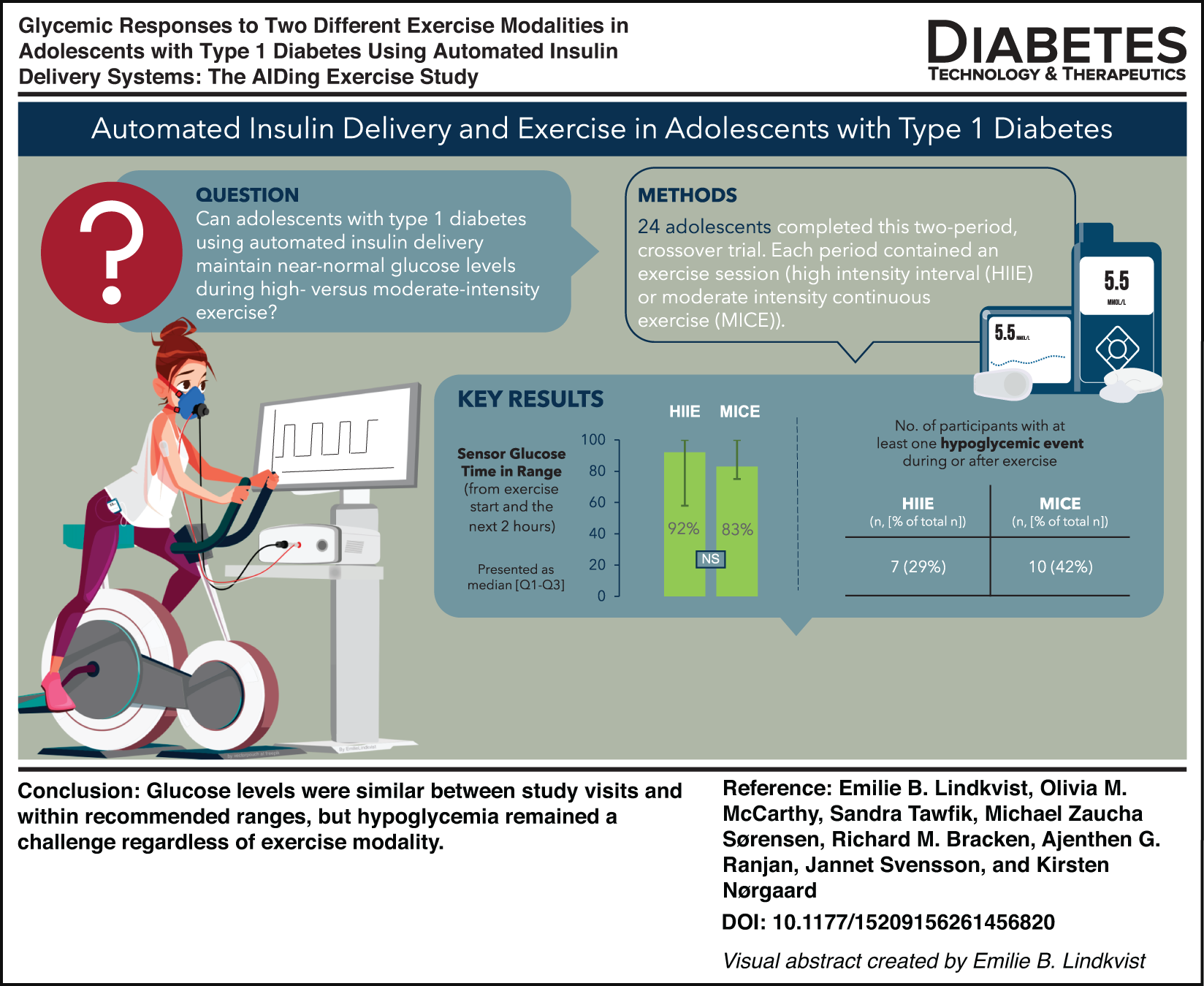
To examine the glycemic responses to two exercise modalities—high-intensity interval exercise (HIIE) and moderate-intensity continuous exercise (MICE)—when applying consensus guideline preexercise preparatory measures in adolescents with type 1 diabetes using automated insulin delivery (AID) systems.
Research Design and Methods:
In a two-period, crossover trial, 24 individuals (12 using MiniMed™ 780G and 12 using Tandem Control-IQ™) completed two experimental study days involving HIIE and MICE sessions. Participants were matched on age, sex, and total daily dose across AID systems. Continuous glucose monitoring (CGM) and insulin pump data were collected from participants’ AID systems. Plasma glucose (PG) was measured throughout the study days. Exercise was announced 60 min before MICE initiation, but not before HIIE.
Results:
No significant difference was observed for the primary outcome, CGM-derived time in range (TIRCGM: 3.9–10.0 mmol/L [70–180 mg/dL]), between study visits (HIIE: 91.7 [58.3–100.0] % vs. MICE: 83.3 [75.0–100.0] %, P = 0.261). Participants developed hypoglycemia during both visits (HIIE: 8 vs. MICE 11). When analyzed by the AID system, TIRPG (PG: 3.9–10.0 mmol/L [70–180 mg/dL]) was higher during MICE in the MiniMed™ 780G group, with no difference in the number of participants experiencing hypoglycemia at either visit.
Conclusions:
When applying consensus guideline preexercise recommendations, both exercise modalities achieved generally stable glycemic outcomes; however, hypoglycemia remained a challenge across study visits. These findings highlight that current AID systems still fall short of ensuring safe glycemic responses during exercise.
Graphical abstract
Keywords
Introduction
Regular physical activity (PA) is important for adolescents with type 1 diabetes (T1D) and considered an integral part of diabetes management.1,2 Despite this, adolescents with T1D have been reported to be less active than their healthy peers.3–6 Adolescence is a transitional phase of life characterized by physical changes, which lead to insulin resistance, elevated insulin requirements, and greater glycemic variability. 7 The fear of developing hypoglycemia has been cited as a major barrier to engaging in regular physical activity. 8 Conversely, greater knowledge about strategies to prevent hypoglycemia is associated with fewer perceived barriers.8–10 Therefore, equipping individuals with T1D with effective strategies for managing glucose around physical activities is important in supporting safe engagement. However, maintaining glycemic stability during acute physical exercise has proved challenging for those with T1D not least because glycemic responses vary depending on exercise characteristics such as modality and intensity.1,2,11 It is also highly dependent on different insulin treatment regimens, which require individualized approaches.2,11 Automated insulin delivery (AID) systems differ from other insulin delivery systems in that insulin administration is automated based on CGM-derived glucose readings, albeit manual entry of carbohydrates for meal bolus is still recommended. Two commonly used AID systems are the Medtronic MiniMed™ 780G (Medtronic Diabetes, Northridge, CA) and the Tandem t:slim X2 Control-IQ™ (Tandem Diabetes, San Diego, CA). Both systems have settings that can be adjusted during exercise: “Temporary Target” (TT) and “Exercise Mode” (EM), respectively. However, knowledge about the efficacy of using these settings during different exercise modalities is limited, particularly in adolescents. To date, most research using AIDs has been conducted in adults undertaking moderate-intensity continuous exercise (MICE).12–14 Whether these findings extend to adolescents, or to anaerobic interval-based activities—such as high-intensity interval exercise (HIIE)—remains underexplored.12,13,15 Recently, a new guideline on PA management for AID users was published, but many recommendations are based on low-certainty evidence. 2
Therefore, this study aimed to compare the CGM-derived time in range (TIR) during and after HIIE versus MICE in adolescents treated with either MiniMed 780G or Tandem Control-IQ, with the hypothesis that the current recommendations around PA can keep blood glucose levels within target 3.9–10 mmol/L during different modalities of PA.
Material and Methods
Study design and ethical approval
This was a single-center, two-period, crossover, clinical trial including 24 adolescents with T1D using AID systems (12 using MiniMed 780G and 12 using Tandem Control-IQ). Participants were matched across the two AID systems on age (±1 year), sex, and total daily insulin dose (TDD) (IU/[kg·d], ± 30%). The study was conducted at Steno Diabetes Center Copenhagen, Denmark, in accordance with the Declaration of Helsinki, and all procedures were approved by the National Research Ethics Committee of Denmark. It was approved by the Danish Regional Committee on Health Research (H-22025766), by the Danish Data Protection Agency (P-2022-311), and it was registered at clinicaltrials.gov (NCT 05619198).
Screening procedure
Inclusion criteria were age 13–17 years, T1D diagnosis for ≥1 year, use of 780 G or Control-IQ for ≥3 months, and HbA1c ≤ 75 mmol/mol (9.0%). Exclusion criteria were the use of other diabetes medications than insulin, pregnancy, or breastfeeding.
All participants and parents were provided with written and oral information before their involvement, and written consent and assent were subsequently obtained, after which individuals completed the screening visit. After inclusion, participants completed a cardiopulmonary exercise test (CPET) to volitional exhaustion.16,17 The data derived from the CPET were used to calculate the workload needed for the exercise sessions performed during the two experimental study visits. 16
Experimental study visits
All participants completed the experimental study visits in a fixed crossover sequence, undertaking the HIIE session first, followed by the MICE session, with a washout period of at least 3 days between study visits. In advance of each study visit, participants were asked to refrain from alcohol and strenuous physical exercise 24 h before their arrival. Additionally, participants were asked to consume their lunch at least 4 h before the exercise session, that is, no later than noon. They were instructed to announce this meal to the pump and take the suggested mealtime insulin dose. Participants were asked to replicate the lunch across the two study visits and to manage potential hypoglycemia and hyperglycemia as usual. Meal timing was confirmed upon arrival at the clinic, and information on meal carbohydrate content and meal bolus insulin was extracted from AID uploading platforms.
Participants arrived at the research facility at 3 pm for the 3 h in-clinic study visits (Fig. 1). Upon arrival, a canula was placed in the antecubital vein for venous blood sampling. Participants rested for 60 min before starting exercise. In order to adhere to consensus guidelines, 1 TT/EM was activated 60 min in advance of exercise on the AID systems during the MICE visit while no announcement was made during the HIIE visit.
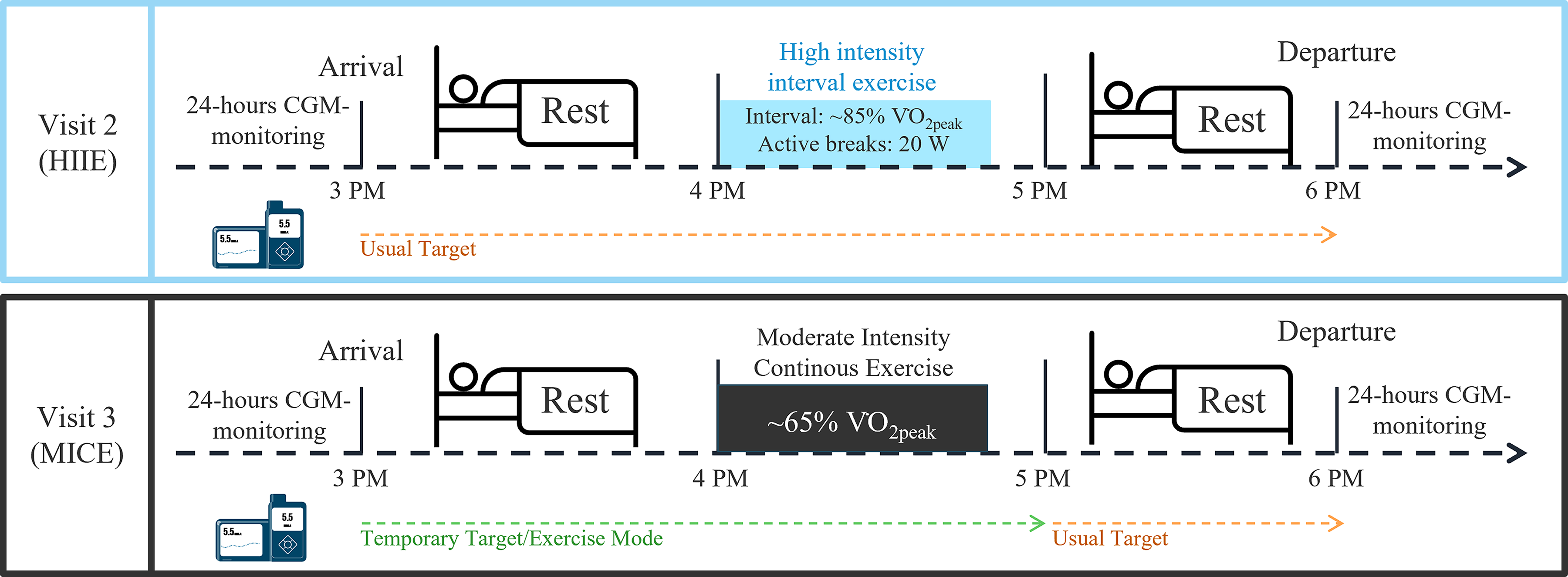
Study days outline. HIIE, high intensity interval exercise; MICE, moderate-intensity continuous exercise.
Both exercise sessions were performed on a workload-controlled ergometer (Vyntus, IntraMedic) following a set protocol. The two exercise sessions were work-load-matched based on the CPET outcomes. 16 The HIIE sessions consisted of 5 min of rest, a 5-min warm-up at 20 W, and 40 min of interval work consisting of eight 1-min cycling bouts at ∼85% of V̇O2peak interspersed with 4-min recovery periods at 20 W followed by a 5-min period of stationary rest at 0 W. The work completed was calculated for each participant by adding the power output during the intervals (85% V̇O2peak for 60 s) and recovery periods (20W for 240 s) across all eight repetitions. This value was then used to determine the minutes of MICE required to match the same workload while cycling continuously at ∼65% V̇O2peak. The MICE sessions included 5 min of rest, 5 min warm-up at 20 W, the calculated duration at ∼65% of V̇O2peak (∼45 min), and 5 min rest at 0 W. During the exercise sessions, participants were wearing a calorimetry mask (Vyaire Vyntus® CPX, Intramedic A/S) to determine metabolic rate and fuel oxidation as well as a telemetry chest strap (Polar H10) for integrated heart rate (HR) measurements. In the MICE session, TT/EM was turned off 15 min after exercise cessation. After each exercise session, participants rested for another 75 min in-clinic before departing.
Home phase
The home phase was defined as the 12 h following the in-clinic study visit (6 pm to 6 am) under free-living conditions. CGM values were collected from the participant’s own CGM device. Participants uploaded data to their corresponding uploading platform (Carelink Professional, Glooko, or Stenopool).
Laboratory analysis
Blood sampling was conducted in 5- or 15-min intervals during the study visits. Plasma glucose (PG) and lactate samples were analyzed immediately using the YSI 2900 Biochemistry Analyzer (YSI Inc., Yellow Springs, OH, USA). The remaining samples were stored at −80°C after centrifugation and thereafter used to determine concentrations of adrenaline and noradrenaline (Bicat Elisa Kit, EA613/192, Eagle Biosciences, Amherst, NH, USA), insulin (Iso-Insulin Elisa, 10-1128-01, Mercodia, Uppsala, Sweden), and glucagon (MESO QuickPlex SQ 120, Z0047978, Rockville, MD 20850, USA) for 3–6 time points at baseline, during, and after exercise.
In the event of hypoglycemia (PG < 3.9 mmol/L [<70 mg/dL]), 15 g of dextrose tablets were administered. After 15 min, PG was reassessed, and the procedure was repeated until PG was above 3.9 mmol/L. If hypoglycemia occurred during exercise, the session was stopped immediately, and the treatment procedure was initiated. This marked the end of the exercise session, regardless of its duration. If hypoglycemia occurred within 30 min of exercise initiation, this was postponed until safe PG levels were reached. If PG was <6.7 mmol/L (120 mg/dL)10 min prior to the exercise session, participants received 15 g of oral dextrose and then started on time. In the event of level 2 hyperglycemia (PG > 13.9 mmol/L [250 mg/dL]), blood ketones were assessed. If ketones were ≤0.6 mmol/L, the study visit continued without any changes. If ketones were >0.6 mmol/L, an individualized insulin bolus dose was administered, and the study visit was rescheduled.
The primary outcome was the difference in CGM-derived time in range ([TIRCGM]: 3.9–10.0 mmol/L [70–180 mg/dL]) measured from exercise initiation to 120 min postexercise between the HIIE and MICE study visits.
Statistical analyses
Due to the absence of preliminary data to inform effect size estimates, an a priori power calculation was not performed. The sample size of 24 participants was therefore based on previously published studies employing similar designs. A post hoc sensitivity power analysis demonstrated that, with 24 paired observations, α = 0.05, and 80% power, the study was powered to detect a minimum within-subject effect size of Cohen’s d = 0.60. Baseline characteristics are displayed as mean ± standard deviation (SD) or n (%), depending on variable type. For the primary outcome and home-phase outcome measures, CGM-derived values are reported, but the remaining in-clinic measures reported are PG. Continuous outcomes are presented as medians with interquartile ranges. Comparisons between visits were performed using paired t-tests for normally distributed data or Wilcoxon signed-rank tests for non-normally distributed data. Secondary endpoints were assessed using the same methodology. Dichotomous outcomes were evaluated using McNemar’s or Fisher’s exact tests, depending on whether comparisons were made on paired or unpaired data. Repeated-measures data were analyzed using linear mixed-effects models with participant as a random effect and visit, time, and their interaction as fixed effects. Holm-adjusted post hoc tests were applied for multiple comparisons. In a post hoc, exploratory analysis, we fitted a logistic mixed-effects regression model to evaluate the predictors of hypoglycemic events during/after exercise. Fixed effects included exercise modality, AID system, total insulin delivery 3 h before exercise and preceding hypoglycemia, while participant was included as a random effect. All statistical analyses were performed using R (version 4.5.0 [2025-04-11]).
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Results
Baseline characteristics
A total of 24 participants were enrolled, and all completed the trial. The baseline characteristics are presented in Table 1. The carbohydrate content of the pre-visit lunch was 26 ± 25 g and 24 ± 28 g before HIIE and MICE, respectively. The corresponding mealtime insulin bolus was 3.8 ± 4.1 IU and 3.7 ± 4.4 IU. In the 24 h prior to each study visit, 14 and 8 participants experienced a level 1 hypoglycemic event before HIIE and MICE, respectively, while no participants experienced a level 2 hypoglycemic event.
Baseline Characteristics
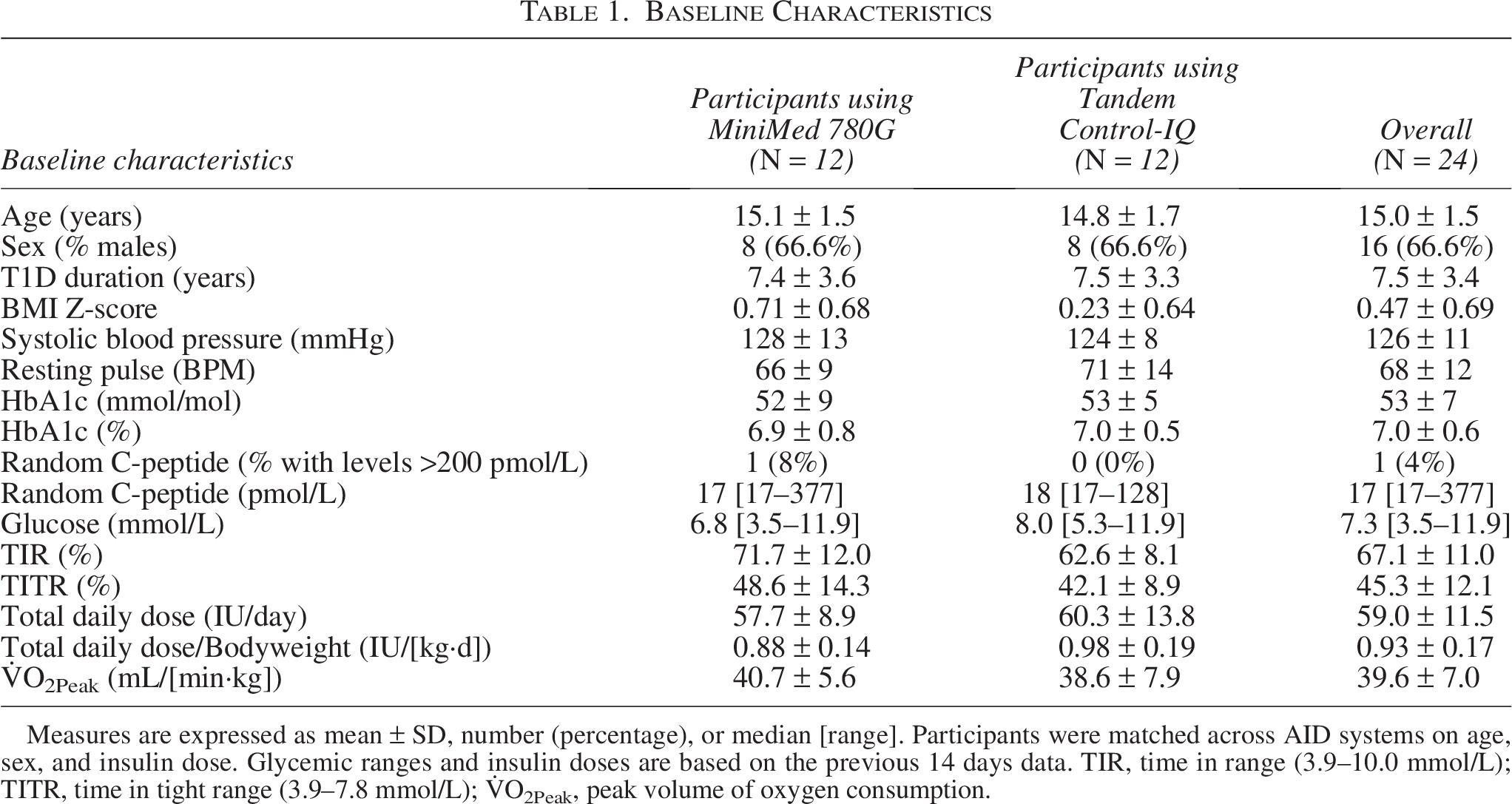
Measures are expressed as mean ± SD, number (percentage), or median [range]. Participants were matched across AID systems on age, sex, and insulin dose. Glycemic ranges and insulin doses are based on the previous 14 days data. TIR, time in range (3.9–10.0 mmol/L); TITR, time in tight range (3.9–7.8 mmol/L); V̇O2Peak, peak volume of oxygen consumption.
In-clinic glycemic and insulin outcomes
For the primary end point (TIRCGM from exercise initiation until end of in-clinic stay [2 h]), there was no statistical difference between the two study visits (HIIECGM: median [IQR] 91.7 [58.3–100.0] % vs. MICECGM: 83.3 [75.0–100.0] %, P = 0.261). The remaining glycemic outcomes for the entire in-clinic (PG values) and home-phase periods (CGM values) are reported in Table 2. During the entire in-clinic stay (3 h), there were no differences between the two visits regarding TIRPG, PG time in tight range ([TITRPG]: 3.9–7.8 mmol/L [70–140 mg/dL]), PG time above range ([TARPG]: >10.0 mmol/L [180 mg/dL]), and PG time below range ([TBRPG]: <3.9 mmol/L [70 mg/dL]). Additionally, there were no statistical differences between the insulin delivered in the 3 h before exercise initiation (HIIE: 3.6 [2.6–5.6] IU vs. MICE: 2.2 [1.4–5.4] IU, P = 0.118) and insulin delivery during the in-clinic period (HIIE: 4.4 [2.8–5.5] IU vs. MICE: 2.7 [1.8–4.7] IU, P = 0.147) (Table 2).
Glycemic Outcomes in-Clinic (3–6 pm) and Home-Phase (6 pm to 6 am)
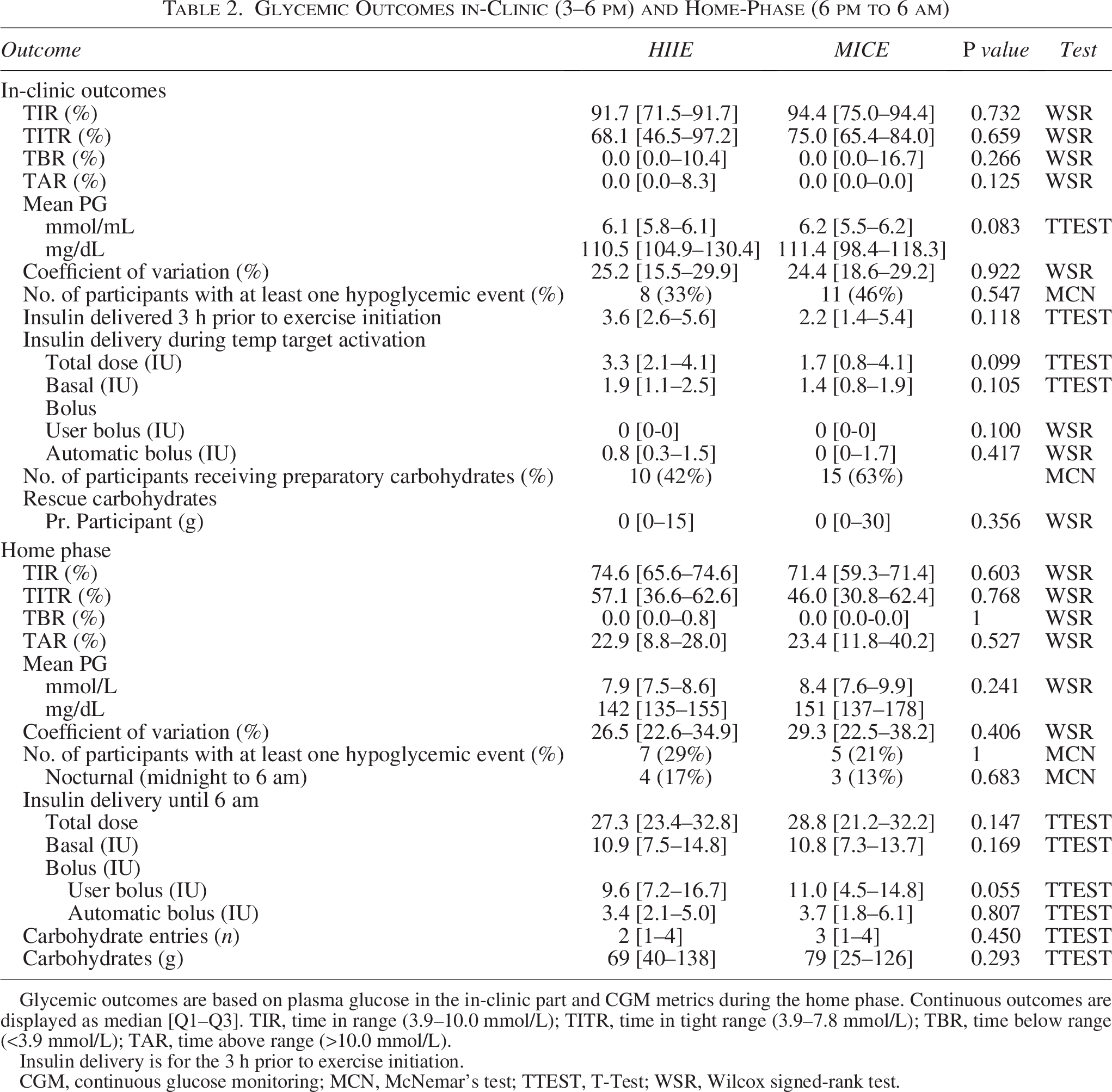
Glycemic outcomes are based on plasma glucose in the in-clinic part and CGM metrics during the home phase. Continuous outcomes are displayed as median [Q1–Q3]. TIR, time in range (3.9–10.0 mmol/L); TITR, time in tight range (3.9–7.8 mmol/L); TBR, time below range (<3.9 mmol/L); TAR, time above range (>10.0 mmol/L).
Insulin delivery is for the 3 h prior to exercise initiation.
CGM, continuous glucose monitoring; MCN, McNemar’s test; TTEST, T-Test; WSR, Wilcox signed-rank test.
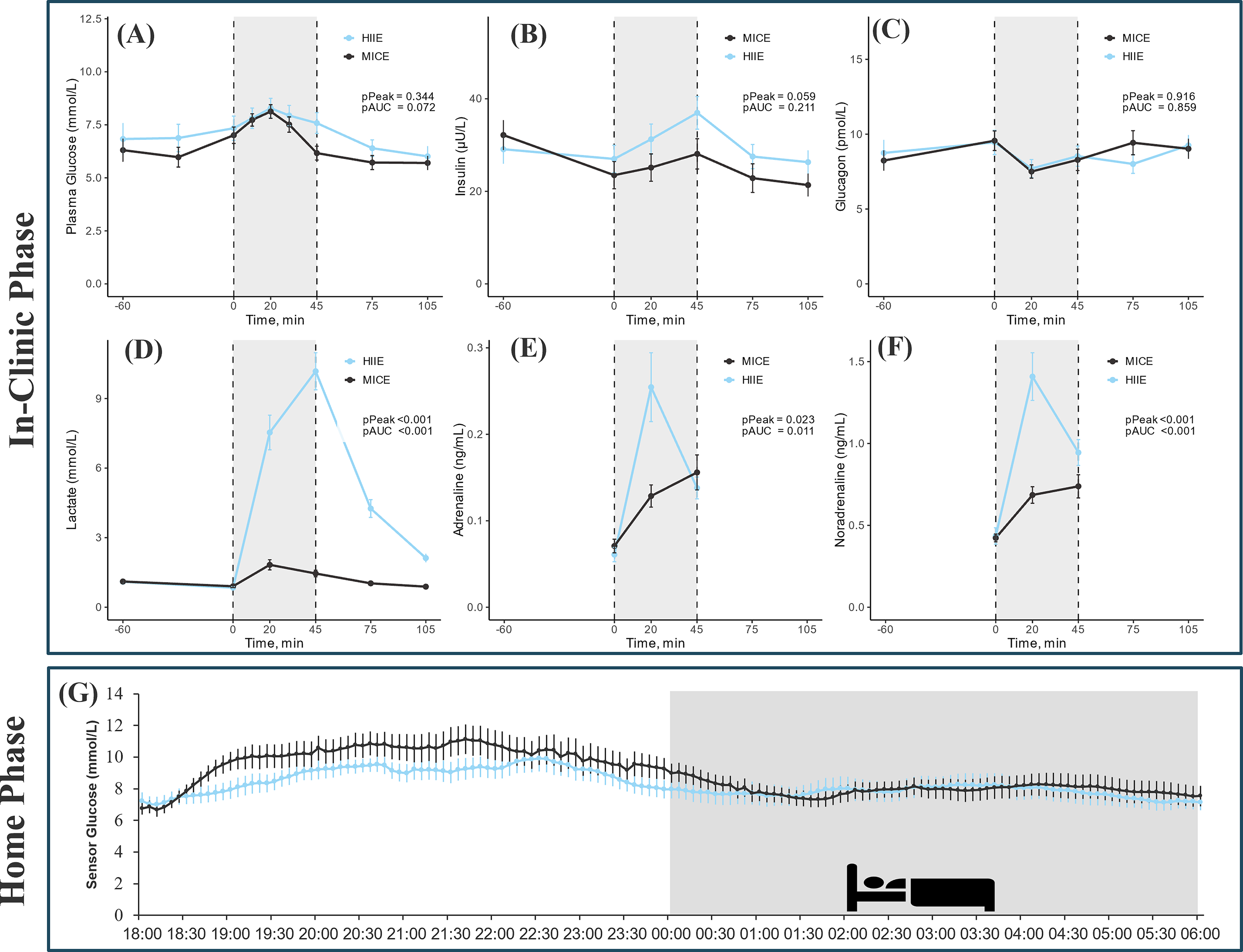
The time course of PG during the in-clinic period is illustrated in Figure 2A. At exercise initiation, PG levels were similar between the two study visits (HIIEPG: 7.3 ± 2.8 mmol/L vs. MICEPG: 7.0 ± 1.9 mmol/L, P = 0.568). However, the magnitude of change over the exercise sessions differed significantly (HIIEPG: +0.2 ± 2.3 mmol/L vs. MICEPG: −1.0 ± 2.3 mmol/L, P = 0.048). This resulted in significantly different PG at the end of exercise (HIIEPG: 7.8 ± 2.2 mmol/L vs. MICEPG: 6.0 ± 1.5 mmol/L, P = 0.009). PG leveled out over the subsequent resting period in both visits, resulting in similar end-of-study PG concentrations (HIIEPG: 6.1 ± 2.4 mmol/L vs. MICEPG: 5.7 ± 1.6 mmol/L, P = 0.499).
Hypoglycemia occurred in one participant during the HIIE session at 35 min, whereas four participants experienced hypoglycemia during the MICE session between 30 and 45 min, at which point exercise sessions were terminated. In the postexercise resting period, six individuals experienced hypoglycemia during both study visits. Among the participants who developed postexercise hypoglycemia, PG at the end of exercise was HIIE: 6.0 ± 1.2 mmol/L versus MICE: 4.7 ± 0.7 mmol/L, whereas CGM was for HIIE: 7.7 ± 2.6 mmol/L versus MICE: 5.6 ± 1.3 mmol/L. The post hoc analysis revealed that the strongest predictor of developing hypoglycemia during or after exercise was the occurrence of hypoglycemia during the preexercise resting period (estimated OR: 6.5 [95% CI: 1.4–30.2], P = 0.017). The other factors included in this analysis (visit number, AID system, and total insulin delivery 3 h before exercise at exercise initiation) did not reach statistical significance (Supplementary Table S1).
Exercise outcomes
The exercise intensity was 88.9 ± 13.2% and 56.0 ± 10.0% (P < 0.001) of V̇O2Peak for the HIIE and MICE sessions, respectively. Mean exercise duration and respiratory exchange ratio did not differ significantly between sessions, whereas all other exercise outcomes were significantly different (Supplementary Table S2).
In-clinic AID-stratified outcomes
When looking specifically at each visit and comparing outcomes between the age, sex, and TDD-matched users of the two AID systems in-clinic, there were no differences in glycemic outcomes for the HIIE visits (Supplementary Table S3). However, at the MICE visits TIRPG differed (MiniMed 780 G: 100 [95.1–100.0] % vs. Tandem Control-IQ: 75.0 [58.3–75.0] %, P = 0.009). The number of participants who experienced hypoglycemia did not differ between the two AID systems at either study visit (Supplementary Table S3, Supplementary Material). Those using Tandem Control-IQ had higher insulin delivery in the 3 h before exercise initiation across both visits compared to those using Medtronic MiniMed 780G (Supplementary Table S3), and the total insulin delivery during the window of TT/EM activation was also higher for those using Tandem Control-IQ compared to those using Medtronic MiniMed 780 G during the MICE visit (MiniMed 780 G: 1.1 [0.8–1.5] IU vs. Tandem Control-IQ: 4.2 [2.3–5.3] IU, P < 0.002), which was mainly driven by higher delivery of autocorrection boluses for those using Tandem Control-IQ than those using Medtronic MiniMed 780G (Supplementary Table S3).
PG levels were similar between AID systems when starting the HIIE (780G 7.3 ± 2.7 mmol/L vs. Control-IQ: 7.0 ± 3.1 mmol/L, P = 0.804) and MICE sessions (780G: 6.7 ± 1.4 mmol/L, vs. Control-IQ: 7.0 ± 2.3 mmol/L, P = 0.750). There was also no difference between the magnitude of change in PG during the exercise sessions (HIIE; 780G: +0.8 ± 2.4 mmol/L/session vs. Control-IQ: −0.1 ± 1.9 mmol/L/session, P = 0.354 and MICE; 780G: −0.2 ± 1.9 mmol/L/session vs. Control-IQ: −0.5 ± 3.0 mmol/L/session, P = 0.786).
Metabolic and hormonal biomarkers
Hormonal and metabolic biomarkers are displayed in Figure 2B–F and Supplementary Table S4. Overall, insulin and glucagon levels were comparable between the two study visits at baseline, peak concentrations, and when expressed as an area under the curve (AUC) (all P > 0.05). When analyzed intravisit, insulin remained stable during HIIE but decreased in MICE following TT/EM activation, albeit with no significant differences between the study visits. Glucagon remained stable with no differences within study days or between. Concentrations of adrenaline and noradrenaline were comparable between visits at T = 0; however, the AUC and peak concentrations were significantly higher in HIIE than MICE. Lactate levels were similar at baseline; however, levels increased significantly from T = 0 during HIIE, peaking at T = 45. The AUC and peak concentrations of lactate were higher in HIIE compared to MICE.
Home-phase glycemic and insulin outcomes
The glycemic outcomes for the home-phase are shown in Figure 2C and Table 2. There were no differences in glycemic outcomes between the two study visits. In both instances, glycemic outcomes were within consensus guideline recommendations. 18 Following HIIE and MICE, seven and five participants developed hypoglycemia, respectively. Of these events, four and three occurred nocturnally (midnight to 6 am) for the two study visits, respectively (Table 2). Additionally, there were no differences in the amount of insulin delivered (total insulin dose; HIIE: 27.3 [23.4–32.8] IU vs. MICE: 28.8 [21.2–32.2] IU, P = 0.147) nor the amount of carbohydrates announced to the AID systems.
Discussion
In this in-clinic and home-based, crossover, controlled study, we found no difference in TIRCGM from exercise to 1 h postexercise between HIIE and MICE in adolescents with T1D using AID systems. However, hypoglycemia remained a challenge, with several events occurring in multiple participants during and after both exercise modalities. These events occurred despite following current guidelines for HIIE and MICE, that is, no exercise announcement for HIIE but with announcement 1–2 h before MICE alongside the ingestion of 10–20 g of glucose when preexercise glucose levels were below 7 mmol/L (126 mg/dL).
To our knowledge, these are the first data in adolescents to demonstrate that, even when using two advanced AID systems and adhering to consensus preexercise guidelines, exercise-related hypoglycemia remains a challenge. These data reinforce the ongoing need to consider prudent exercise management in this population to minimize the extent of clinically classified low glucose levels.
Our results align with two recent studies in adults with the MiniMed 780G 13 and adolescents with the older generation MiniMed 670G, 19 where different preventive measures ensured optimal glycemic outcomes. Even so, they too did not manage to prevent exercise-induced hypoglycemia. Like these studies, we observed that hypoglycemia occurred predominantly during and immediately after exercise during MICE, whereas delayed postexercise hypoglycemic episodes were more apparent in HIIE. These patterns imply that announcing exercise ahead of time for MICE is particularly important in preventing acute onset hypoglycemia that otherwise deters continued engagement. Though not currently recommended in consensus guidelines, our data suggest that applying exercise announcement for HIIE may be less time-sensitive but still beneficial, especially if activation occurs closer to the exercise bout to lessen the scope of latent-onset hypoglycemia. However, the results also emphasize, that additional strategies may be required to reduce hypoglycemia, for exmaple, spread-out feedings of carbohydrates during exercise, 20 use of alternative nutrition formulations, 21 or even low-dose glucagon administration.15,22 In an earlier guideline and consensus report, the need for carbohydrate intake during exercise was described in general terms, with recommendations suggesting that small amounts of carbohydrates may be required to prevent hypoglycemia.3,23 However, the most recent position statement have provided clearer, quantified thresholds, recommending the consumption of 3–20 g of carbohydrates when glucose levels fall below 7.0 mmol/L during exercise. 2 As this study was conducted prior to the publication of these updated guidelines, such strategies were not implemented.
Similarly, the newest position statement also introduces a quantified postexercise recommendation, advising the intake of 3–20 g of carbohydrates when exercise is completed with glucose levels below 5.0 mmol/L (90 mg/dL). 2 In our study, this strategy was not applied, and participants instead received carbohydrates only if hypoglycemia occurred. Those who developed hypoglycemia in the postexercise resting period generally had higher CGM levels (HIIECGM: 7.7 ± 2.6 mmol/L vs. MICECGM: 5.6 ± 1.3 mmol/L) at exercise termination, suggesting that the current 5 mmol/L (90 mg/dL) threshold may not be sufficient to prevent postexercise hypoglycemia for AID users. Future studies should focus on establishing an appropriate BG limit and amount and type for preparatory carbohydrate feedings and possible extension of postexercise TT/EM activation. Based on our findings, it seems reasonable to recommend a higher level, especially following HIIE, and if glucose is trending downwards.
An important challenge was the occurrence of hypoglycemia in some participants during the preexercise resting period, requiring treatment according to guidelines. 1 In our explorative, post hoc analysis, we showed that the main predictor of developing hypoglycemia during or after exercise was an event of hypoglycemia in the resting period beforehand (Supplementary Table S1, Supplementary Material). However, due to the small sample size and limited number of events, the study had reduced statistical power to detect significant effects; therefore, the findings should be interpreted with caution rather than as conclusive evidence. The mechanism is likely multifactorial: (1) antecedent hypoglycemia blunts counterregulatory responses, 24 (2) unstable preexercise glucose levels increase hypoglycemia risk, 25 and (3) rescue glucose given before exercise in users of AID systems may trigger automated insulin delivery, potentially increasing insulin on board (IOB), which would increase hypoglycemia risk.2,25–27 Hence, the most optimal strategy for avoiding hypoglycemia during or after exercise may be to ensure stable and safe glycemic levels before exercise initiation.3,24,25,28 Achieving this, however, can be particularly challenging in an adolescent population. 29 In our study, we attempted to reduce IOB at exercise initiation by having participants fast for 4 h before exercise. Although some residual insulin may remain 4 h after the last insulin bolus, the amount is expected to be minimal. Despite this measure, hypoglycemia still occurred, suggesting that fasting alone may be insufficient to mitigate exercise-related risk. Moreover, such a strategy may not be realistic or generalizable to a real-world setting.
Markedly higher lactate concentrations during HIIE compared with MICE confirm that the two exercise protocols elicited distinct physiological intensities. Adrenaline and noradrenaline increased substantially more during HIIE than MICE at T = 20 (the midpoint of cycling), reflecting greater sympathetic activation. This difference was no longer apparent at T = 45, likely because the final sample was drawn approximately 4 min after the final sprint, allowing partial clearance of catecholamines from circulation. 30 Insulin concentrations decreased during TT/EM activation in MICE but did not differ significantly from HIIE, while glucagon levels remained stable across both exercise modalities.
When examining the age, sex, and TDD-matched pairs across AID systems, glycemic outcomes differed between the two AID systems. During the MICE visit, TIRPG was higher in MiniMed 780G users compared with Tandem Control-IQ users. TITR and TBR were also numerically lower with MiniMed 780G; however, none of these differences reached statistical significance (Supplementary Table S3). The difference is most likely driven by a higher amount of insulin delivered in the hours preceding exercise, as well as by the increased delivery in Tandem Control-IQ users during TT/EM activation, where autocorrection insulin can be delivered. In contrast, the MiniMed 780G algorithm does not allow autocorrection during TT (4.2 [2.3–5.3] IU vs. 1.1 [0.8–1.5] IU, P < 0.001; Supplementary Table S3). This underlines the importance of considering intrapump differences in exercise management, as different AID-specific algorithms may require customized preparatory measures to ensure safe outcomes. An important caveat when considering our findings is the use of two commercial AID systems. Hence, future research would benefit from including a wider range of devices to facilitate generalizability on scale.
Following both exercise sessions, glycemic outcomes were generally maintained within recommended targets during the 12 h home phase, yet more than 20% of participants experienced hypoglycemia, including nocturnal episodes. A recent study reported higher TIR and lower TAR following HIIE than MICE, but this came at the cost of increased hypoglycemia. 19 One explanation may be the longer postexercise fasting period of 4 h in that study compared with our 1-h period, especially considering that participants had already fasted for 3–4 h before exercise. 19 Such extended fasting may not reflect real-world behavior and highlights the lack of consensus regarding the optimal time frame for reporting glycemic outcomes in relation to PA.
This study demonstrates that tailoring exercise announcement strategies to specific exercise modalities may help prevent hypoglycemia. For MICE, activating TT/EM is beneficial, and doing so at least 60 min before exercise initiation is important. When engaging in HIIE, it might be possible to do so spontaneously without activating TT/EM, when starting ∼45 min of high intensity interspersed with recovery periods. For either exercise modality, consuming 15 g of carbohydrates right before exercise when PG is <6.7 mmol/L is prudent. During MICE it is important to be aware of the glycemic level, and ingestion of small amounts of carbohydrates regularly may be a solution to avoid hypoglycemia.2,20 When engaging in HIIE, glucose intake or activating the TT/EM in the postexercise period may be needed, when the counterregulatory hormone levels decrease.
Adolescents often struggle to plan their daily activities,20,21 which reduces the likelihood of implementing preparatory measures that depend heavily on extensive preparation. Research has demonstrated that, in their everyday lives, only a small proportion adhere to existing guidelines when engaging in exercise.25,31 In this context, it is essential for health care professionals to be equipped with alternative strategies for ensuring safe glycemic outcomes while supporting and promoting regular PA. Moreover, the development of flexible strategies that enable adolescents to manage hypoglycemia through carbohydrate consumption should be actively explored.
The strengths of the study include that we measured relevant biomarkers and the in-clinic outcomes were reported as PG, minimizing the risk of wrongful outcome measures due to company-specific differences in sensor values. 32 Additionally, the exercise sessions were workload-matched but ended up being of similar durations as well, meaning the comparison across the two study visits can be attributed to the exercise intensity and the preparatory measures. A limitation of this study was the non-randomized design, which may have introduced order effects or residual confounding. However, the crossover design, in which participants completed both exercise modalities, reduced interindividual variability and allowed participants to serve as their own controls. Exercise sessions were conducted in the afternoon, when the included age group would typically engage in exercise as part of their after-school activities; however, the generalizability of the study is limited, as an in-clinic, controlled environment does not accurately reflect real-world life. However, to get more insight into the efficacy of the AID systems, controlled settings are needed before implementing them in everyday life. Another limitation is that participants were not randomized to the AID systems, and inherent differences between adolescents using the two systems may have influenced the findings. However, participants were matched on age, sex, and total daily insulin dose to minimize baseline differences between AID groups. Last and regrettably, the menstrual cycle phase was not recorded or controlled for in female participants, and potential effects of hormonal fluctuations on glycemic responses cannot be excluded.
In adolescents using AID systems, adherence to recommended preexercise guidelines ensured the maintenance of optimal glycemic outcomes during and after both high-intensity interval and MICE. However, hypoglycemia remains a significant challenge, particularly in the hours following exercise and when hypoglycemia occurs beforehand. Extending the use of TT/EM and/or consuming carbohydrates may help mitigate this risk, especially in situations where preexercise hypoglycemia is present.
Authors’ Contributions
E.B.L., O.M.M., R.M.B., A.G.R., K.N., and J.S. contributed to the conception and design of the study. E.B.L., O.M.M., S.T., and M.Z.S. contributed to the attribution of the data. E.B.L., O.M.M., and A.G.R. were responsible for data analyses. All authors were responsible for data interpretation. E.B.L. wrote the original draft of the article. All authors contributed to revising the article. All authors provided final approval of the version to be published.
Footnotes
Acknowledgments
The authors thank Jette Høgsmose and Nour Houssein Yaqub for their help in recruiting participants.
Author Disclosure Statement
R.M.B. has received grants from Novo Nordisk, Beneo, and speaker fees from Abbott, Novo Nordisk, Roche, and Sanofi Aventis. J.S. has served as an educator for Medtronic. She has received funding from Medtronic and Novo Nordisk. J.S. owns shares in Novo Nordisk. J.S. has received fees for speaking on behalf of Medtronic, Sanofi Aventis, Rubin Medical, and Novo Nordisk. K.N. serves as an adviser to Medtronic, Abbott, Convatec, Tandem, and Novo Nordisk; owns shares in Novo Nordisk; has received research grants to the institution from Novo Nordisk, Zealand Pharma, Dexcom, and Medtronic; and has received fees for speaking from Medtronic, Abbott, and Novo Nordisk. E.B.L., O.M.M., S.T., M.Z.S., and A.G.R. have nothing to disclose.
Funding Information
The study was funded by the Novo Nordic Foundation (grant number:
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.