
Abstract
Post-traumatic stress disorder (PTSD) widely occurs among victims or witness of disasters. With flashbacks, hyperarousal, and avoidance being the typical symptoms, PTSD became a focus of psychological research. The earthquake in Wenchuan, China, on May 12, 2008, was without precedent in magnitude and aftermath and caused huge damage, which drew scientists’ attention to mental health of the survivors. We conducted a systematic overview by collecting published articles from the PubMed database and classifying them into five points: epidemiology, neuropathology, biochemistry, genetics and epigenetics, and treatment. The large body of research during the past 6 years showed that adolescents and adults were among the most studied populations with high prevalence rates for PTSD. Genomic and transcriptomic studies focusing on gene × environment studies as well as epigenetics are still rare, although a few available data showed great potential to better understand the pathophysiology of PTSD as multifactorial disease. Phytotherapy with Chinese herbs and acupuncture are rarely reported as of yet, although the first published data indicated promising therapy effects. Future studies should focus on the following points: (1) The affected populations under observation should be better defined concerning individual risk factor, time of observation, spatial movement, and individual disease courses of patients. (2) The role of social support for prevalence rates of PTSD should be observed in more detail. (3) Efficacy and safety of Chinese medicine should be studied to find potential interventions and effective treatments of PTSD.
Introduction
On May 12, 2008, an earthquake with a magnitude of 8.0 on the Richter scale and a maximum intensity of 11, struck China’s southwestern Sichuan province. With Wenchuan in the center, it affected 237 counties in the provinces of Sichuan, Gansu, and Shaanxi, with a total stricken area of 252,000 km. According to a message from the national earthquake relief headquarters, by the deadline of September 25, 2008, a total of 69,227 people died, 17,923 people were missing, and 374,643 people were wounded. After the Wenchuan earthquake, the Chinese government activated the emergency medical rescue system and 10,630 medical workers were ordered to the affected areas. Until September 25, 2008, a total of 1,486,407 people were rescued by the rescue and disaster relief staff.
Natural disasters usually cause physical and psychological stresses to survivors, leading to the irreversible destruction and trauma. This was also true for the Wenchuan earthquake. The profound tragedy caused emotional and psychological traumata for tens of thousands of people who survived. Post-traumatic stress disorder (PTSD) is one of the most prevalent psychological diseases, affecting children, adolescents, adults, and health care workers exposed to disasters.
Up to now, a lot of studies on the Wenchuan earthquake and PTSD have been published, which have great scientific value for treatment and management of survivors. In the present review, we give an overview on the various aspects of PTSD in Wenchuan earthquake survivors, including epidemiology, neuropathology, biochemistry, genetics and epigenetics, as well as treatment approaches, aiming to draw conclusions and give perspectives for further research. We collected the articles related to the Wenchuan earthquake, which are listed in the Pubmed database, with the key words “Wenchuan earthquake” and “posttraumatic stress disorder” by October 1, 2014. In total, 69 articles were identified.
PTSD refers to a delayed and lasting psychological stress disorder caused by exposure to trauma. The traumata leading to PTSD include threat to death or threat to sexual or physiological integrity. PTSD was first recognized in the 1970s in veterans of the Vietnam War and described as post-Vietnam syndrome and later on termed PTSD (Berry, 1972; Van Putten & Emory, 1973). This disease also widely occurs in earthquake survivors and victims who experienced other traumatic events such as sexual abuse in childhood (McLean, Morris, Conklin, Jayawickreme, & Foa, 2014), rape (Armour, Elklit, Lauterbach, & Elhai, 2014; Weaver, Griffin, & Mitchell, 2014), accidents, or terroristic acts (Cavanagh, Fitzgerald, & Urry, 2014; Dekel, Ein-Dor, Gordon, Rosen, & Bonanno, 2013; Kucukoglu, Yildirim, & Dursun, 2014). Typical symptoms of PTSD are related to repeatedly experiencing trauma with disturbing recurring flashbacks, avoidance or numbing of memories of the event, and hyperarousal. As a result, PTSD brings great impairments in patients’ social life.
PTSD was first included into the third edition of the Diagnostic and Statistical Manual of Mental Disorders, third edition (DSM-III) by American Psychiatric Association in 1980 and continued to be listed in subsequent editions, that is, DSM-III, DSM-III-Revised (DSM-III-R), DSM, fourth edition (DSM-IV), and DSM-IV, text revision (DSM-IV-TR). As the Wenchuan earthquake occurred, DSM-IV-TR was used to diagnose PTSD. The latest edition is DSM, fifth edition (DSM-5), which was published in 2013, superseding the DSM-IV-TR, which was published in 2000. DSM-5 reveals some differences concerning PTSD compared to the former versions. PTSD is not enlisted anymore in the chapter “anxiety disorders” but as own chapter entitled “Trauma- and stressor-related diseases together with acute stress disorder and adaptation disorder.” In DSM-5, diagnosis criteria are further elaborated. For instance, Criterion A (stressor criterion) focusses more on the circumstances, how a person experiences a traumatizing event, while other criteria have been deleted. It should be born in mind that PTSD diagnoses of Wenchuan earthquake survivors in 2008 based on the former DSM version might differ to some extent based on the new criteria of DSM-5 from 2013. For instance, the duration of PTSD-like symptoms plays an important role. Symptoms that disappear within 6 months are indicative of the acute stress disorder, while symptoms persisting for longer times contribute to the diagnosis of PTSD. In practical terms, it might sometimes not be easy for practitioners to use this information and translate it for use in treatment. In addition to DSM-IV-TR and DSM-5, the Chinese Classification of Mental Disorders (CCMD-III) edited by the Chinese Psychiatric Association in the year 2000 is used for PTSD diagnosis in China. In May 2008, the description of the disease course was revised by the Chinese Ministry of Health. According to the descriptions of PTSD by CCMD-III, typical symptoms of PTSD are related to repeatedly experiencing trauma, nightmares, or involuntary memory in similar situations to the initial trauma, persisting hyperarousal, avoidance, selective memory loss related to traumatic experience, and feeling hopeless about the future. The symptom criteria include exposure to a traumatic event (Criterion A), repeatedly experiencing the initial trauma (Criterion B), hyperarousal reaction (Criterion C), and persisting avoidance to the trauma (Criterion D). Another serious criterion is related to impaired social function. The disease course is typically characterized by a delayed breakout after more than 1 month. Exclusion criteria are affective disorder, other stress disorders, neurological disorders, and somatoform disorders.
Earthquakes are traumatic events that threaten people’s safety. Since the past several decades, earthquakes drew the public attention for its frequent occurrence and huge destruction. Thousands of people have been affected by PTSD several months after earthquakes (Cenat & Derivois, 2014, 2015; Tanaka et al., 1999). The Wenchuan earthquake on May 12, 2008, was life changing for many individuals and families. After the earthquake, PTSD was widely found in different populations. One month after the earthquake, Lau and colleagues performed a cross-sectional survey among 3,324 secondary school students living in Chengdu (90 km away from the disaster’s epicenter). Of them, 22.3% reported PTSD symptoms (Lau et al., 2010). B. Wang, Ni, et al. (2011) investigated for PTSD among 430 survivors in Qiaozhuang town of Qingchuan county and observed that 62.8% subjects met the criteria for PTSD 1 month after the earthquake. Chen et al. made a cross design with 1,321 survivors who had endured both an earthquake and a mudslide. The prevalence rate of PTSD symptoms was 18.7% (H. Chen, Chen, et al., 2014). Six months after the earthquake, the prevalence rate of PTSD was 15.6% among adult survivors in the three severely affected areas (Dujiangyan, Beichuan, and Qingchuan) and was 15.8% among the adolescents in Dujiangyan (Fan, Zhang, Yang, Mo, & Liu, 2011; Zhou et al., 2013). One year after the earthquake, the prevalence rate of PTSD among survivors in Beichuan was 40.1% and 26.3% (Z. Zhang, Shi, Wang, & Liu, 2011). Three years after the earthquake, the rates of physical diseases and symptoms of PTSD were still relatively high. In Mao County, the worst-hit area (only 41 km away from the epicenter), PTSD prevalence rate among the students was 29.6% (Pan et al., 2013). In Beichuan, 22.7% of the earthquake survivors reported clinical symptoms of PTSD (G. Chen, Shen, & Chen, 2012). Taken together, it is quite obvious that a wide range of the population suffered from PTSD after the earthquake.
Epidemiology of PTSD Among Wenchuan Earthquake Survivors
There are numerous reports related to prevalence rates of PTSD during the Wenchuan earthquake in different periods. Two points should be emphasized in this context: (1) Incidence is “the number of instances of illness commencing or of persons becoming ill” (or dying or being hurt in injuries or whatever) “during a given period in a specified population” (Last & Association, 2001, p. 145). While prevalence gives a figure for a factor at a single point in time and tells us only what is happening at a certain point (Jekel, Katz, Elmore, & Wild, 2007, pp. 23–24), most of the reports on the Wenchuan earthquake used the term “prevalence,” not “incidence” for several months lasting aftershock period. Hence, we continue to speak about prevalence. (2) Most of the reports measured PTSD symptoms with checklists related to the DSM-IV-TR criteria. Nevertheless, it can be assumed that the reported prevalence rates are indeed related to PTSD.
Community Studies
Community studies on PTSD have been mainly carried out at different time periods after the Wenchuan earthquake and investigated collective of people broader than the specific population affected by the earthquake. Studies have been performed between 1 month and 3 years after this earthquake (Table 1). However, the prevalence rates of PTSD have not been studied in different periods.
PTSD Among Wenchuan Earthquake Survivors.
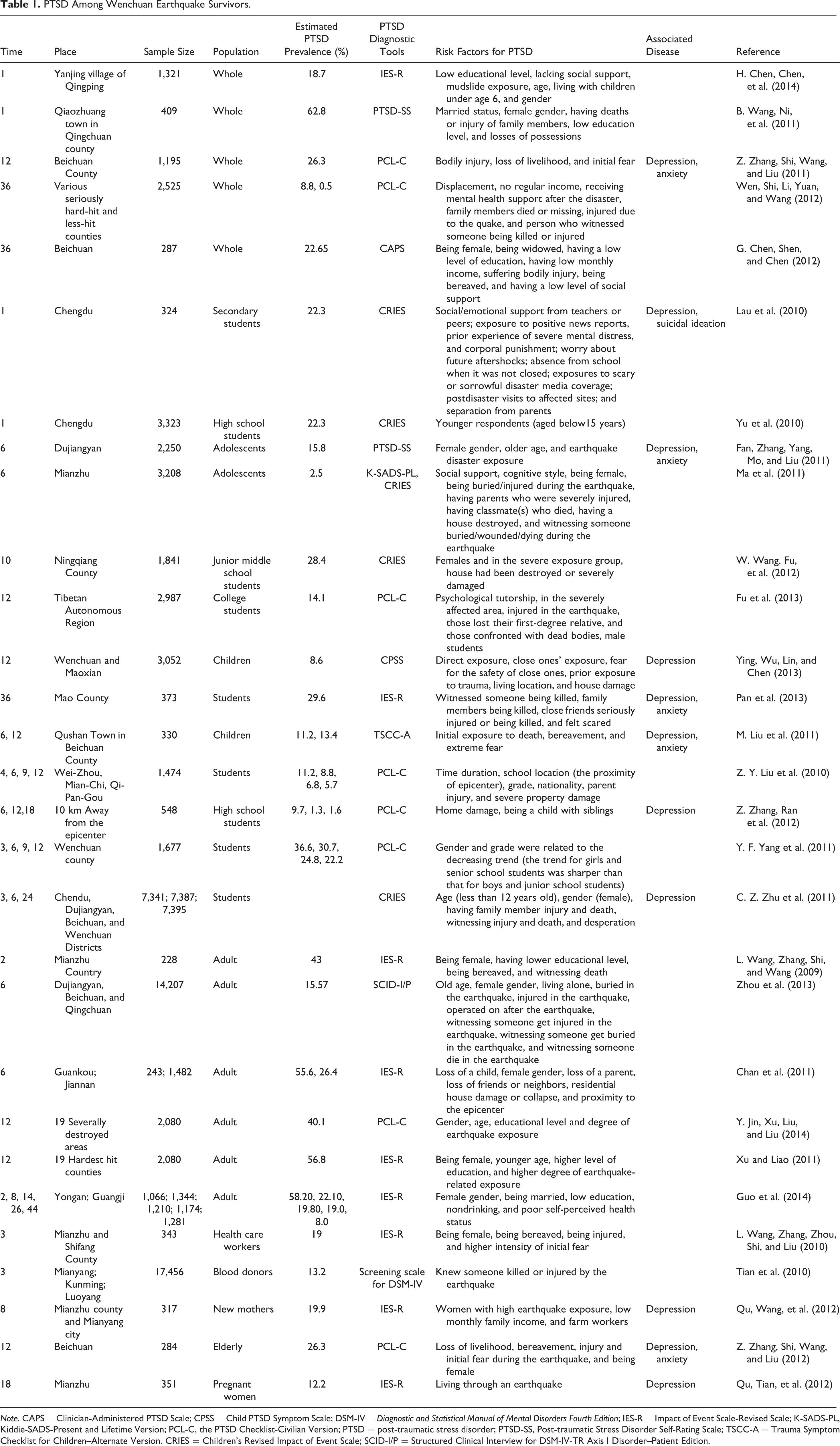
Note. CAPS = Clinician-Administered PTSD Scale; CPSS = Child PTSD Symptom Scale; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders Fourth Edition; IES-R = Impact of Event Scale-Revised Scale; K-SADS-PL, Kiddie-SADS-Present and Lifetime Version; PCL-C, the PTSD Checklist-Civilian Version; PTSD = post-traumatic stress disorder; PTSD-SS, Post-traumatic Stress Disorder Self-Rating Scale; TSCC-A = Trauma Symptom Checklist for Children–Alternate Version. CRIES = Children’s Revised Impact of Event Scale; SCID-I/P = Structured Clinical Interview for DSM-IV-TR Axis I Disorder–Patient Edition.
Prevalence
One month after the Wenchuan earthquake, the prevalence rate of PTSD in Qiaozhuang town in Qingchuan County was 62.8% (257 of 430; B. Wang, Ni, et al., 2011). One year after the earthquake, the prevalence rate in Beichuan was 26.3% (Z. Zhang, Shi, et al., 2011). Two years after the earthquake, the quality of survivors living in prefab houses was low, and there were still a number of people in temporary settlements affected PTSD 2 years after the earthquake (L. Zhang, Wang, et al., 2011). Three years later, symptoms of PTSD were reported by 8.8% of the respondents from the seriously affected areas and 0.5% from the less hit areas (Wen, Shi, Li, Yuan, & Wang, 2012). A cross-sectional study on PTSD 3 years after the earthquake reported a prevalence rate of 22.7% among elderly Qiang citizens in Beichuan County (G. Chen, Shen, et al., 2012).
Risk factors
A number of demographic factors significantly increased the risk for PTSD, such as high female gender (H. Chen, Chen, et al., 2014; B. Wang, Ni, et al., 2011), major property loss (H. Chen, Chen, et al., 2014; L. P. Zhang, Wang, Li, and Hu, 2012), bodily injury, death or missing of family members (H. Chen, Chen, et al., 2014; B. Wang, Ni, et al., 2011; Wen et al., 2012; Z. Zhang, Shi, et al., 2011), low or no regular income (H. Chen, Chen, et al., 2014; Wen et al., 2012), and lacking social support (B. Wang, Ni, et al., 2011). Besides, low education also was related to the likelihood of developing PTSD (H. Chen, Chen, et al., 2014; B. Wang, Ni, et al., 2011).
Specific Populations
Adolescents were most widely studied after the Wenchuan earthquake. The earthquake took thousands of students’ and teachers’ lives from elementary and middle schools. In these articles, adolescents include the school students and nonstudents. They are summarized as both adolescents and children in the present review. In addition, adult survivors were studied for their greater PTSD risk. Other populations include health care workers, blood donors, and so on (Table 1).
Adolescents and Children
Prevalence
Adolescents have been most frequently investigated. One month after the earthquake, 19.3% of all students bore suicide in their minds and 22.3% suffered from PTSD (Lau et al., 2010; Yu et al., 2010). In another study, 15.8% of adolescents showed clinical symptoms of PTSD 6 months after the earthquake (Fan et al., 2011). The prevalence rate of PTSD was 2.5% in 3,208 adolescents from the surrounding areas of the epicenter in Mianzhu City (Ma et al., 2011). Another study showed that the high-risk prevalence rate for PTSD was 28.4% among junior middle school students in Ningqiang County (W. Wang, Fu, et al., 2012). One year after the earthquake, a total of 420 (14.1%) college students in Tibetan autonomous region were diagnosed with PTSD, among whom mild, moderate, severe, and extreme symptoms were reported in 122, 185, 106, and 7 cases, respectively (Fu et al., 2013). Another study performed with 3,052 child survivor in 20 primary and secondary schools in the counties of Wenchuan and Maoxian indicated that 8.6% of them reported PTSD (Ying, Wu, Lin, & Chen, 2013). Prevalence of PTSD among junior high school students in worst-hit areas was 29.6%, 3 years after the Wenchuan earthquake (Pan et al., 2013).
Compared with discrete studies, longitudinal course studies might be more valuable. Y. F. Yang et al. (2011) performed a follow-up study with middle school students in the Wenchuan earthquake region and found that the average prevalence rates of PTSD after 3, 6, 9, and 12 months were 36.6% (613 of 1,677), 30.7% (515 of 1,677), 24.8% (416 of 1,677), and 22.2% (373 of 1,677), respectively. M. Liu et al. (2011) reported that the prevalence rates of PTSD in Beichuan County, which was completely destroyed by the earthquake, were 11.2% and 13.4%, respectively, after 6 months and 1 year. Liu et al. also did a follow-up study of PTSD among 1,474 adolescents students in Grades 7, 8, 10, and 11 from three Wenchuan secondary schools 4, 6, 9, and 12 months after the earthquake. The screened prevalence of PTSD was 11.2%, 8.8%, 6.8%, and 5.7% at 4, 6, 9, and 12 months after the earthquake, respectively (Z. Y. Liu et al., 2010). Z. Zhang, Ran, et al. (2012) reported rates of PTSD symptoms of 9.7%, 1.3%, and 1.6% among adolescents after 6-, 12-, and 18-month follow-ups, respectively. C. Z. Zhu, Situ, et al. (2011) also found that symptoms of young survivors from earthquake-struck areas had gradually alleviated 3, 6, and 24 months after the earthquake.
Risk factors
Multiple factors significantly increased the risk for PTSD in adolescents, for example, prior experience of severe mental distress and corporal punishment (Lau et al., 2010; Pan et al., 2013); worry about future aftershocks (Lau et al., 2010); exposure to scary, death, or sorrowful disaster media coverage (Fu et al., 2013; Lau et al., 2010; Ma et al., 2011; Pan et al., 2013; C. Z. Zhu, Situ, et al., 2011); postdisaster visits to affected sites (Lau et al., 2010); or separation from parents (Fu et al., 2013; Lau et al., 2010). Other factors such as gender and age also impacted the risk for PTSD (Fu et al., 2013; Xu & Liao, 2011; Y. F. Yang et al., 2011; Z. Zhang, Ran, et al., 2012; C. Z. Zhu, Situ, et al., 2011). Male students were more prone than female students to develop PTSD. Besides, students who lost their first-degree relative also were more likely to express PTSD (Fu et al., 2013). On the other hand, psychological tutorship and social support were protective factors for PTSD (Fu et al., 2013). Y. F. Yang et al. (2011) observed a trend for self-recovery among adolescents during the first year after the earthquake, but boys and junior school students recovered more slowly.
Adult Survivors
Prevalence
In a study conducted 2 months after the Wenchuan earthquake, the prevalence rate of PTSD among adult survivors was 43.0% (L. Wang, Zhang, Shi, & Wang, 2009). Thereafter, Zhou et al. performed a study with 14,207 individuals 6 months after the earthquake. The prevalence of PTSD was 15.6% among adult survivors (Zhou et al., 2013). Chan et al. (2011) performed a study 6 months after the earthquake and reported that the prevalence rates of PTSD in Guankou and Jiannan were 55.6% and 26.4%, respectively. However, following studies estimated the prevalence of PTSD in 19 hardest areas, with 1 year after the earthquake to 40.1% and 56.8% (Y. Jin, Xu, Liu, & Liu, 2014; Xu & Liao, 2011). A follow-up study among adult survivors over a 4-year period after the earthquake indicated PTSD prevalence rates of 58.2% 2 months, 22.1% 8 months, 19.8% 14 months, 19.0% 26 months, and 8.0% 44 months after the earthquake (H. Chen, Chen, et al., 2014).
Risk factors
Adult survivor studies documented increased PTSD risk among women (Chan et al., 2011; G. Chen, Shen, et al., 2012; H. Chen, Chen, et al., 2014; L. Wang, Zang, et al., 2009; Xu & Liao, 2011; Zhou et al., 2013). Age was also claimed as a risk factor for PTSD among adult survivors, although with contradictory results. Xu and Liao (2011) agreed that being old may increase the risk, whereas Y. Jin, Xu, Liu, and Liu (2014) showed that younger age may be a negative factor. Other studies also provided contrary results concerning education level and marriage status among adult survivors (H. Chen, Chen, et al., 2014; L. Wang, Zang, et al., 2009; Xu & Liao, 2011). Other risk factors include loss of families, injury, exposure to great harm, low income, and low perceived level of social support. Furthermore, social support played a vital role in balancing and protecting mental health (He, Xu, & Wu, 2013).
Other Populations
Prevalence
Except adolescents and adults, other populations were also studied. The prevalence rate of PTSD was 19.9% among mothers with newborn babies 8 months after the Wenchuan earthquake (Qu, Wang, et al., 2012). Furthermore, the prevalence rate of PTSD among pregnant women was 12.2% between November 2009 and January 2010 (Qu, Tian et al., 2012). Among health care workers in earthquake-affected areas, 19.0% reported PTSD (L. Wang, Zhang, Zhou, Shi, & Liu, 2010). The overall prevalence of PTSD was 13.2% among blood donors (Tian et al., 2010). For elderly survivors in Beichuan, 26.3% were reported PTSD clinical symptoms 1 year after the earthquake (Z. Zhang, Shi, Wang, & Liu, 2012).
Risk factors
Mothers with newborn babies, high earthquake exposure, low monthly family income, and farm workers had a higher risk for PTSD (Qu, Wang, et al., 2012). Exposure to earthquake correlated with PTSD among pregnant women (Qu, Tian, et al., 2012). Being female, being bereaved, being injured, and higher intensity of initial fear all increased the PTSD risk among health care workers in earthquake-affected areas (Wang et al., 2010). Loss of livelihood, bereavement, injury and initial fear during the earthquake, and being female were negative factors of elderly survivors (Z. Zhang, Shi, et al., 2012).
Statistical Evaluation of Published Data
We were intrigued to find out, whether common trends were apparent regarding the temporal and spatial occurrence of PTSD among Wenchuan earthquake survivors. Based on the published literature in Table 1, we first addressed the question, as to whether PTSD systems many vanish over time. We took all studies into account, which measured PTSD prevalence rates at certain time points after the earthquake. If studies reported prevalence rates after the same time points, average values have been calculated. All values have been subjected to linear regression analysis and Pearson rank correlation test.
Figure 1A shows the correlation between PTSD prevalence (in percentage) and time after the earthquake (in months). The prevalence significantly decreased over time (R = .741, p = .028) in adult earthquake survivors. Comparable results have been observed for children and adolescents (Figure 1B). Again, PTSD prevalence significantly decreased over time (R = .880, p = .010). Two differences can be observed between adults and children/adolescents. Firstly, the PTSD prevalence rate among adult Wenchuan earthquake survivors was much higher (50.6%) shortly after the earthquake (1 month) than among children and adolescents (22.3%). Secondly, adults needed longer times (>40 months) than children and adolescents (˜20 months) to get rid of the PTSD symptoms (Figure 1A and B). Data were not available about the percentages of PTSD patients who did not regress at all and continued to suffer from PTSD for a long term. The reasons as to why adults mentally suffered more from the earthquake than children and adolescents are not known. It can be speculated that adults felt more challenged than children because of the worries as to how to manage everyday life after the earthquake, whereas children trusted their parents or (if they lost their parents) on relatives or governmental institutions to manage the aftermath. This speculation has to be validated by future investigations.

Prevalence of posttraumatic stress disorder (PTSD) among Wenchuan earthquake survivors. Correlations between PTSD prevalence (in percentage) and time after earthquake (in months) in (A) adults and (B) children and adolescents. Correlations between PTSD prevalence (in percentage) and distance (in kilometer) from the epicenter of the earthquake in (C) the whole population and (D) children and adults. Pearson’s rank correlation test has been used to calculate correlation coefficients (R values) and statistical significance (p values). Data have been taken from (A) Guo et al. (2014), Chan et al. (2011), L. Wang, Zhang, Shi, and Wang (2009), Y. Jin, Xu, Liu, and Liu (2014), Zhou et al. (2013), Xu and Liao (2011); (B) Lau et al. (2010), Fan, Zhang, Yang, Mo, and Liu (2011), Yu et al. (2010), Ma et al. (2011), Y. F. Yang et al. (2011), M. Liu et al. (2011), Z. Y. Liu et al. (2010), Z. Zhang, Ran, et al. (2012), Ying, Wu, Lin, and Chen (2013), W. Wang, Fu, et al. (2012); (C) G. Chen, Shen, and Chen (2012), H. Chen, Chen, et al. (2014), B. Wang, Ni, et al. (2011); (D) Lau et al. (2010), W. Wang, Fu, et al. (2012), Yu et al. (2010), Pan et al. (2013), Fan et al. (2011), M. Liu et al. (2011), Ma et al. (2011), Z. Y. Liu et al. (2010), Z. Zhang, Ran, et al. (2012).
The next question we addressed was, whether the distance to the epicenter of the earthquake affected the prevalence rates of PTSD. Our initial expectations were that the prevalence rates increase with increasing closeness to the epicenter. As can be seen in Figure 1C and D, this was not the case. We observed a high correlation coefficient (R = .995) and statistical significance (p = .002) between increasing PTSD prevalence rates (in percentage) and increasing distance from the earthquake epicenter (in kilometer) among the whole population (Figure 1C). In children and adolescents (Figure 1D), the correlation did, however, show only a trend for statistical significance (p = .064, R = .546). Again the reasons are unknown for this observation and we can only speculate. It can be imagined that the governmental disaster management saved lives of buried alive victims, recovered dead bodies, and took care about survivors preferentially in the epicenter of the earthquake and less in the periphery. Therefore, PTSD might have developed more in the periphery, which has been termed “psychological typhoon eye” effect and which is closer to the danger and less frightened (Li, Rao, Bai, et al., 2010; Li, Rao, Ren, et al., 2009). In addition, the spatial movement of local people should be considered as a factor causing a mixture of affected and unaffected people. This circumstance might be reflected by the results we have obtained. The correlation coefficient in Figure 1D showing the relationship between distance and PTSD symptoms is weaker (r = .546) compared to the one obtained from the relationship between time and PTSD symptoms in Figure 1C (r = .880). These hypotheses deserve further attention and investigation in the future.
Other Psychological Symptoms Associated With PTSD
PTSD is remarkably often associated with depression, anxiety, suicide ideation, or other psychiatric disorders, especially depression, which was as high as 84.4% (Blanco et al., 2013; Galatzer-Levy, Nickerson, Litz, & Marmar, 2013; Pompili et al., 2013; Spinhoven, Penninx, van Hemert, de Rooij, & Elzinga, 2014). Among the numerous psychiatric disorders, depression, suicidal ideation, and anxiety were the three most common comorbidities of PTSD among Wenchuan earthquake survivors. Lau et al. reported that 1 month after the earthquake, Children’s Revised Impact of Event Scale scores were correlated with Children’s Depression Inventory scores and suicidal ideation. Among those with either PTSD or depression, 26.3% revealed comorbidity of the two problems (Lau et al., 2010). Similar outcomes of depression in association with PTSD have been reported by other authors (Fan et al., 2011; Lau et al., 2010; M. Liu et al., 2011; Pan et al., 2013; Ying et al., 2013; Z. Zhang, Ran, et al., 2012; Z. Zhang, Shi, et al., 2012; C. Z. Zhu, Situ, et al., 2011). Fang et al. reported that 6 months after the Wenchuan earthquake, PTSD, anxiety, and depression were significantly correlated with each other among adolescents. Longer term studies among different populations also proved the correlation between depression, anxiety, and PTSD (Z. Y. Liu et al., 2010; Pan et al., 2013; Z. Zhang, Shi, et al., 2011, 2012).
Neuropathology of PTSD Among Wenchuan Earthquake Survivors
The hippocampus, amygdala, and prefrontal cortex (PFC) belonging to the limbic system are three most important brain regions and play a fundamental role in emotional processing in both humans and animals (Heimer & Van Hoesen, 2006). Alterations in these regions are related to anxiety and affective disorders (Elzinga & Bremner, 2002; Shin & Liberzon, 2010). The hippocampus is involved in termination of stress response, and hippocampal lesions increase corticotropin-releasing factor (also known as corticotropin-releasing hormone, CRH) levels in the brain (Herman et al., 2003). The amygdala is responsible for threat detection and elaborating conditioned and unconditioned fear responses, by receiving projections from hippocampus and PFC. The medial PFC (mPFC) is the executive control center of the brain, providing top-down fashion to regulate the activity of amygdala and function in an inhibitory manner to extinguish conditioned fear response (Peters, Kalivas, & Quirk, 2009; Vidal-Gonzalez, Vidal-Gonzalez, Rauch, & Quirk, 2006). Subjects with PTSD show reduced activation of PFC and hippocampus, which might coincide with reduced top-down control of the amygdala, possibly resulting in hyperresponsive amygdala signals to fearful stimuli and leading to disordered fear regulation in PTSD (Etkin & Wager, 2007). Another anatomical observation in PTSD is a decrease in hippocampal volume and morphology, which might be caused by genetic variants of FK506 binding protein 5 (FKBP5; Fani et al., 2013; Levy-Gigi, Szabo, Kelemen, & Keri, 2013). Decreased gray matter volumes and altered white matter integrity were also observed in the pregenual anterior cingulate cortex in combat-exposed individuals with PTSD diagnosis versus healthy subjects in twin studies (Kasai et al., 2008).
After the Wenchuan earthquake, numerous studies have been performed related to neural changes in brain regions and electrophysiological mechanisms of missing memory. Wu et al. reported that PTSD patients exhibited shorter NoGo-N2 (an enhanced negativity at approximately 200 ms poststimulus onset in response to NoGo stimuli) latencies than the non-PTSD group. The authors concluded that the impairment of response inhibition in adolescent participants with PTSD is related to their impulsive cognitive functioning (J. Wu et al., 2010). Shang et al. (2014) found that PTSD patients of the Wenchuan earthquake had widespread deficits in both low-level perceptual and higher order cognitive networks. Chen et al. reported that PTSD patients had some attention deficits compared with non-PTSD individuals (X. Chen, Wei, et al., 2012; Yun et al., 2011). On the other hand, Yang et al. found that children and adolescents with PTSD from the Wenchuan earthquake had deficits only in the emotional control domain of executive function compared with controls exposed to the same disaster and that these deficits did not persist (R. Yang et al., 2014). Yin and colleagues investigated brain functions under a resting condition with PTSD patients from Wenchuan earthquake. They found that abnormal resting state functional connections linking the thalamus to cortical regions may be involved in the underlying pathophysiology of PTSD. Altered amplitude of low-frequency (0.01–0.08 Hz) fluctuation in predominantly right hemisphere cortical and subcortical regions and in cerebellum and alterations in the local functional connectivity of cortical regions and whole-brain functional connectivity potentially contributed to the neural mechanisms underlying traumatic memory and symptoms in PTSD (C. Jin et al., 2013; Yin, Jin, Eyler, et al., 2012; Yin, Jin, Hu, et al., 2011; Yin, Li, et al., 2011).
Biochemistry of PTSD Among Wenchuan Earthquake Survivors
The hypothalamic–pituitary–adrenal (HPA) axis coordinates neuroendocrine responses to stress by adaptation to stress and maintenance of homeostasis after challenge. Yet, it is also vital in supporting baseline functions (Kudielka & Kirschbaum, 2005). Exposure to a stressor can induce the release of CRH from the paraventricular nucleus of hypothalamus, which promotes the release of adrenocorticotropic hormone (ACTH) from the anterior pituitary. ACTH is released into the systemic circulation and stimulates the production and release of cortisol from the adrenal cortex (Charmandari, Tsigos, & Chrousos, 2005). Cortisol plays an important role during times of stress by binding to two different receptors: the mineralocorticoid and glucocorticoid receptors (MR and GR, respectively). GRs are ubiquitously present in the brain, promoting adaptation to and recovery from stress. MRs are observed most predominantly in limbic structures, which is mainly implicated in the appraisal process and the acute onset of stress response (de Kloet, Joels, & Holsboer, 2005; Reul & de Kloet, 1985). The binding of cortisol to GRs can mediate feedback inhibition of the HPA axis and limit stress-induced activation of it.
A dysfunctional HPA axis is associated with numerous psychosomatic and psychiatric disorders (Glynn, Davis, & Sandman, 2013; Heim, Ehlert, & Hellhammer, 2000; Heim, Newport, et al., 2000; Holsboer, 1989; Maniam, Antoniadis, & Morris, 2014; Nicolaides, Charmandari, Chrousos, & Kino, 2014; Stratakis & Chrousos, 1995; Raison & Miller, 2003; Tsigos & Chrousos, 1994; Young, 1998). PTSD has been associated with a range of changes in HPA axis, including elevated levels of the CRH/CRH type 1 receptor (CRHR1) system (Amstadter et al., 2011; White et al., 2013; Wolf et al., 2013), low cortisol levels (T. Chen, Guo, et al., 2014; Horn, Pietrzak, Corsi-Travali, & Neumeister, 2014; Wahbeh & Oken, 2013; Yehuda, Engel, et al., 2005), and increased sensitivity of GR (Lehrner et al., 2014; Yehuda, Cai, et al., 2009). Except the HPA axis changes, other biochemical changes also were observed, such as high catecholamine secretion into urine (Pervanidou & Chrousos, 2010) and low serotonin and dopamine levels may also contribute to PTSD (Olszewski & Varrasse, 2005).
It has been widely acknowledged that cortisol can affect learning and memory processes. Cortisol generally impairs memory performance when administered before retrieval (de Quervain, Aerni, Schelling, & Roozendaal, 2009), but the opposite result was also observed, suggesting that beneficial effects of acute cortisol elevations on hippocampal mediated memory processes in PTSD. Cortisol levels were commonly reduced in PTSD patients in the saliva, urine, and blood, which had been used as biomarkers for PTSD (Bicanic et al., 2013; Masoudzadeh, Modanloo Kordi, Ajami, & Azizi, 2012; Yehuda et al., 2005; Yehuda, Bierer, et al., 2009; Wahbeh & Oken, 2013; Walsh et al., 2013). Recent studies showed, however, contradictory results. Cortisol levels were elevated in PTSD patients (Kotozaki & Kawashima, 2012; Stoppelbein, Greening, & Fite, 2012). Hair cortisol levels were widely observed in PTSD patients, measuring long-term cortisol exposure (Steudte et al., 2013). Wosu, Valdimarsdottir, Shields, Williams, and Williams (2013) performed a systematic review of correlates of cortisol in human hair to inform the design, analysis, and interpretation of future epidemiologic studies, suggesting that the study of hair cortisol presents a unique opportunity to assess chronic alterations in cortisol concentrations in epidemiologic studies. Studies also showed that lasting interindividual differences due to variation in early life experiences and/or dispositional (trait) emotional arousal moderate cortisol’s effects on neuroplasticity and learning (Abercrombie, Wirth, & Hoks, 2012; Bagot et al., 2009; Champagne et al., 2008). PTSD patients from the Wenchuan earthquake revealed changing hair cortisol levels over time, which were elevated directly after the earthquake. The non-PTSD subjects showed significantly higher cortisol levels than the PTSD group between 2 and 4 months and also between 5 and 7 months after the traumatic event (Luo et al., 2012). This phenomenon was also found in another study with 12 male adults and 8 females from the Wenchuan earthquake. Their hair cortisol contents were significantly higher than in the control group. But in another group, in 20 adolescents, hair cortisol levels increased 6 and 22 weeks after the earthquake and decreased 43 weeks after the outburst (Gao et al., 2014).
Genetics and Epigenetics of PTSD Among Wenchuan Earthquake Survivors
It has been a matter of long-lasting discussions, whether PTSD is associated with genetic predisposition. Initially, twin studies demonstrated that genetics may explain a significant proportion of vulnerability to PTSD following trauma exposure (Lyons et al., 1993; Stein, Jang, Taylor, Vernon, & Livesley, 2002). Ongoing research mainly focuses on the identification of biomarkers for PTSD. The vulnerability to PTSD development after trauma exposure has been conceptualized to involve a fear conditioning process, in which fear responses are exaggerated and/or resistant to extinction (Amstadter, Nugent, & Koenen, 2009; Jovanovic et al., 2010). In addition to research on etiology and conditions for maintenance of fear conditioning, the pathophysiology and molecular biology of PTSD were most widely studied, including the HPA axis, the locus coeruleus–noradrenergic systems and connections between the limbic system and frontal cortex as well as genetic and epigenetic factors of PTSD.
Gene × Environment (G × E)
There are numerous studies indicating that PTSD is an ideal candidate for G
FKBP5 is a co-chaperone protein that interacts with another molecular chaperone, Heat shock protein 90 (HSP90) and is part of the mature GR heterocomplex. It regulates GR sensitivity and nuclear translation of GRs. Reduced activity of FKBP5 leads to increased GR sensitivity. Studies have demonstrated an interaction between polymorphisms in FKBP5 and environment to predict PTSD severity. Four polymorphisms of the FKBP5 gene have been associated with PTSD risk among European and African Americans as well as Africans (Binder et al., 2008; Sarapas et al., 2011; Wilker et al., 2014; Xie et al., 2010). Despite the importance of these polymorphisms, data on the Wenchuan earthquake survivors are not available yet.
Serotonin is a catecholamine neurotransmitter, which plays an important role in regulating activity within the limbic–frontal system and inhibits the development of fear memories (Rainnie, 1999). Great attention has been focusing on polymorphisms in the promoter region of the serotonin transporter (5-HTTLPR), in which the short allele was less efficient than the long allele. It is also associated with decoupling of the circuit between PFC and amygdala responsible for extinction of fear conditioning (Lesch et al., 1996; Pezawas et al., 2005). Several studies worldwide indicated risk associated with the short allele of 5-HTTLPR in association with exposure to environments of high stress/trauma (Kilpatrick et al., 2007; Z. Wang, Baker, et al., 2011; Walsh, Uddin, Soliven, Wildman, & Bradley, 2014; Xie et al., 2009). Zhao et al. investigated this polymorphism of PTSD with Chinese Han adolescents after the Wenchuan earthquake. The frequency of 5-HTTVNTR allele 12 in the PTSD group was significantly higher than in the control group, indicating an increased PTSD risk in Chinese Han adolescents (Zhao, Wang, Yu, Li, & Ma, 2012).
Except these two most widely studied genes, other genotypes include catechol-O-methyltransferase (COMT; Kolassa, Kolassa, Ertl, Papassotiropoulos, & De Quervain, 2010), D2 dopamine receptor (DRD2; Voisey et al., 2009), gamma-aminobutyric acid (GABA; Nelson et al., 2009), and G-protein signaling 2 (RGS2; Amstadter, Koenen, et al., 2009). After the Wenchuan earthquake, more attention was paid on polymorphisms in the tryptophan hydroxylase (TPH2) PAC1 receptor (ADCYAP1R1) and catalase (CAT) genes. Cao et al. conducted a study of a total of 326 Chinese adults who lost their children during the Wenchuan disaster. They found that TPH2 rs11178997 genotype, an SNP located in the transcriptional control region, may play an important functional role in PTSD development and contributed to PTSD symptoms (Cao, Wang, Wang, Qing, & Zhang, 2014). This was consistent with a previous study on the TPH2 rs11178997 genotype in 200 adults exposed to the 1988 Spitak earthquake from 12 families (Goenjian et al., 2012). Cao et al. (2013) also reported that the STMN1 rs182455 genotype was not associated with the severity of total PTSD symptoms either on females or on males. However, this polymorphism significantly predicted severity of PTSD reexperiencing symptoms in females. Another study indicated that the PAC1 receptor (ADCYAP1R1) rs2267735′CC′ genotype was not associated with total PTSD symptoms but significantly predicted the severity of emotional numbing symptoms in women (L. Wang, Cao, et al., 2013). This finding was confirmed by most, but not all reports (Almli et al., 2013; Duan et al., 2014; Ressler et al., 2011; Stevens et al., 2014; Uddin et al., 2013), indicating the existence of gender-specific relationships between polymorphic genotypes and development of PTSD.
Epigenetics
Recent evidence suggests that epigenetics plays an important role in mediating G × E interactions. Epigenetics critically influences long-term exposure to stressful life events (Meaney, 2010; Meaney & Ferguson-Smith, 2010; Mehta et al., 2013; Mill & Petronis, 2007). Negative experience in early life has been associated with DNA hypermethylation as well as demethylation of specific regulatory sites in key genes for stress processing including GR and neuropeptide arginine vasopressin (AVP; McGowan et al., 2009; Murgatroyd et al., 2009; Weaver et al., 2004). Lower SLC6A4 methylation correlated with increased PTSD risk (Koenen, Uddin, et al., 2011). Increased DNA methylation at the NGFI-A (nerve growth factor-induced protein A) binding site of the GR gene (NR3C1) promoter was associated with less intrusive memory of the traumatic event and reduced PTSD risk in male but not female survivors (Vukojevic et al., 2014). This indicates that epigenetic modifications may be linked to gender-specific differences in memory functions and PTSD risk. DNA methylation in the promoter regions of immune genes, COMT and brain-derived neurotrophic factor (BDNF) were also associated with PTSD (Norrholm et al., 2013; Roth, Zoladz, Sweatt, & Diamond, 2011; Rusiecki et al., 2013). Whether epigenetics might play a role in PTSD patients of the Wenchuan earthquake is still unknown.
Treatment of PTSD in Wenchuan Earthquake Survivors
Psychotherapy
Psychosocial interventions play a crucial role in the management of PTSD, which include trauma-focused cognitive–behavior therapy (TFCBT), exposure therapy, eye movement desensitization and reprocessing (EMDR), and so on. Among them, TFCBT and EMDR have the most empirical support (Ehlers et al., 2010). Goncalves, Pedrozo, Coutinho, Figueira, and Ventura (2012) performed a systematic review of published articles to evaluate the efficacy of virtual reality exposure therapy (VRET) in the treatment of PTSD, and the results showed that no differences were found between VRET and exposure treatment. After the Wenchuan earthquake, different psychological approaches have been applied to treat earthquake survivors with PTSD. Wu et al. conducted an RCT with 2,368 military rescuers 1 month according to the “512 Psychological Intervention Model” and then 1, 2, and 4 months later to follow-up changes in PTSD symptoms, anxiety, and depression based on the DSM-IV criteria. It showed that “512 PIM” was an effective psychological intervention for military rescuers in reducing symptoms of PTSD, anxiety, and depression after this crisis (S. Wu et al., 2012). Z. Wang, Wang, and Maercker (2013) developed the Chinese My Trauma Recovery approach, a web-based intervention strategy to provide mental health help for traumatized persons. Short-term cognitive–behavioral therapy (CBT) group intervention represents a robust intervention for natural disaster victims (Y. Chen, Shen, et al., 2014). A randomized waiting-list controlled pilot study was conducted at the site of the Sichuan earthquake in Beichuan County between December 2009 and March 2010 to evaluate the efficacy of narrative exposure therapy (NET) as a short-term treatment for PTSD. The results suggested that NET is effective in treating post-earthquake traumatic symptoms in adult Chinese earthquake survivors (Zang, Hunt, & Cox, 2013). In addition to the above psychotherapy, interpersonal psychotherapy (IPT) is a 12-week structured psychotherapy approach developed by Klerman and Weissman in the 1980s, aiming at examining and changing current relationships and social support in order to improve mood and anxiety symptoms. Jiang et al. performed a randomized clinical trial among Sichuan earthquake survivors with IPT. A significantly greater reduction of PTSD and major depressive disorder diagnoses was found in the IPT group versus the treatment as usual (TAU) group, indicating that IPT is a promising treatment for reducing PTSD and depression (Jiang et al., 2014).
Pharmacotherapy
Likewise psychotherapy, pharmacotherapeutic intervention can reduce PTSD symptoms to some extent (Ipser & Stein, 2012; Jeffreys, Capehart, & Friedman, 2012; Kerbage & Richa, 2013). Different pharmacological classes with different pathogenesis have been investigated to improve the symptoms, such as selective serotonin reuptake inhibitors, α-adrenergic antagonists, anticonvulsants, mood stabilizers, antipsychotics, β-blockers, benzodiazepines, glucocorticoids, tricyclic antidepressants, and monoamine-oxidase inhibitors. How effective pharmacotherapy was for PTSD patients form Wenchuan earthquake has not been documented in the literature.
Chinese Medicine
Chinese medicine is widely acknowledged by its long history and practices, not only in Asia but also worldwide. Acupuncture and phytotherapy are two major treatment methods of Chinese medicine. Acupuncture is widely used to treat trauma-related symptoms such as insomnia (L. F. Li & Lu, 2010), depression (Manber et al., 2010; T. M. Zhu, Jin, & Zhong, 2009), anxiety (Pilkington, Kirkwood, Rampes, Cummings, & Richardson, 2007; Spence et al., 2004), and other comorbidities (Hollifield, Sinclair-Lian, Warner, & Hammerschlag, 2007). Lee et al. (2012) conducted a systematic review of the effectiveness of acupuncture toward trauma spectrum response, and acupuncture appeared to be effective for treating headaches, anxiety, sleep disturbances, depression, and chronic pain. There are also some trials on acupuncture to treat PTSD of Wenchuan earthquake survivors. Zhang et al. compared the effectiveness with 24 cases treated by CBT and 67 cases treated by both CBT and acupoint stimulation in Wenchuan earthquake survivors suffering from PTSD. The total scores of Impact of Event Scale–Revised (IES-R), the scores of all factors, and the total scores of a questionnaire in the two groups after treatment were much lower than those before treatment. The comparison of reduction in the factor scores between the two groups showed that the curative effect in the treatment group was better than that of in the control group (L. Zhang, Wang, & He, 2011). Wang et al. also performed a clinical trial in 138 patients with earthquake-caused PTSD using RCTs to assess the efficacy and safety of electroacupuncture. The cases enrolled were randomly assigned to an electroacupuncture group and a paroxetine group. The electroacupuncture group was treated by scalp electroacupuncture on 4 points (Baihui, Sishencong, Shenting, and Fengchi), and the paroxetine group was treated with orally administered paroxetine. The results showed that the total scores of Clinician-Administered PTSD Scale (CAPS), Hamilton Depression Scale in the two groups after treatment showed significant efficacy compared to those before treatment, and the electroacupuncture group was more significant than the paroxetine group (Y. Wang, Hu, Wang, Pang, & Zhang, 2012).
Chinese herbs were also useful to improve the symptoms of PTSD (Head & Kelly, 2009; Mao, Ip, Xian, Hu, & Che, 2012; Qin et al., 2011; Y. Wang, Fan, & Huang, 2012). Free and Easy Wanderer (Xiao-Yao-Wan) is a famous herbal remedy in China, which consists of eight herbs. In rats challenged with enhanced single prolonged stress as experimental in vivo model, Free and Easy Wanderer reversed anxiety-like behavior and cognitive impairments to the behavioral values before stress exposure (H. N. Wang, Peng, et al., 2009). It is of interest that a Chinese herbal formula (Xiao-Tan-Jie-Yu-Fang), which consists of 14 components, has been proved to successfully treat PTSD in 245 survivors of the 2008 Sichuan earthquake in a randomized, double-blind, placebo-controlled clinical trial. PTSD-related symptoms in patients treated with this Chinese herbal formula were significantly improved compared with the placebo group. The herbs caused improvement in somatization, obsessive-compulsive behavior, depression, anxiety, hostility, and sleep quality without serious side effects, indicating that Xiao-Tan-Jie-Yu-Fang represents a safe and efficient option to improve the generally poor psychological status in PTSD patients (Meng et al., 2012).
Other approaches, such as Yoga and meditation, can be defined as mind–body practice, were also proved to be useful to treat PTSD (Bormann, Liu, Thorp, & Lang, 2012; Catani et al., 2009; Descilo et al., 2010; Kim, Schneider, Kravitz, Mermier, & Burge, 2013; Rosenthal, Grosswald, Ross, & Rosenthal, 2011). Taichi and qigong also belong to the repertoire of Chinese medicine and represent effective approaches to treat PTSD (Grodin, Piwowarczyk, Fulker, Bazazi, & Saper, 2008). But there is no study related to Wenchuan earthquake now. Remarkably, calligraphy therapy was also effective in reducing hyperarousal symptoms among child survivors in Wenchuan earthquake (Z. Zhu et al., 2014).
Discussion of Assessment Methods
Several methods have been developed to facilitate the diagnosis and assessment of PTSD, including screening tools to identify earthquake survivors suffering from PTSD, diagnostic methods to determine severity and duration as well as neurophsychological impairments. Examples are structured or semi-structured interviews, such as the CAPS (Friedman, 1981), the Schedule for Affective Disorders and Schizophrenia for School-Age Children (Kiddie-SADS-Present and Lifetime Version; K-SADS-PL, Version 1.0 of October 1996; M. Liu et al., 2011; Z. Zhang, Shi, et al., 2011), and the Structured Clinical Interview for DSM-IV (SCID; Y. Jin et al., 2014). Self-report screening tools are the IES-R (Berry, 1972; Tanaka et al., 1999) and the PTSD Checklist–Civilian Version (PCL-C; Ying et al., 2013; L. Zhang, Shi, et al., 2012). PTSD Self-Rating Scale (PTSD-SS) is a brief screening instrument for PTSD (X. C. Liu et al., 1998). Based on the definition and diagnostic criteria in the DSM-IV and Chinese Classification and Diagnostic Criteria of Mental Disorders, second edition, revised (CCMD-II-R), the PTSD-SS matched well with the specific conditions of Chinese culture and lifestyle and was proved to be a valid screening method to identify traumatized patients in China (Tanaka et al., 1999; L. Zhang, Wang, et al., 2011).
Despite the availability of numerous tools to assess PTSD among Wenchuan earthquake survivors, there was no consensus regarding their efficacy and reliability of PTSD prevalence rates (Table 1). SCID and CAPS are the gold standard of PTSD, but they are hardly practicable in the wake of large-scale traumas. There were only two reports among Wenchuan earthquake survivors using them (G. Chen, Shen, et al., 2012; Zhou et al., 2013). In many Wenchuan earthquake studies, screening methods for PTSD symptoms were used, such as the PCL-C, Chinese version and Children version of IES-R. Other screening tools used were the Child PTSD Symptom Scale, Trauma Symptom Checklist for Children–Alternate Version (TSCC-A), and PTSD-SS. With so many different methods and differing sample sizes in the studies, the estimated prevalence rates of PTSD could hardly reach sufficient accuracy. Further studies with standardized methods and higher sample numbers are therefore warranted to generate more accurate data on PTSD prevalence rates among Wenchuan earthquake survivors.
Conclusion and Perspective
Based on the above results of the past 6 years on PTSD in Wenchuan earthquake survivors, the following conclusions can be drawn: (1) The burden of PTSD among Wenchuan earthquake survivors with high trauma exposure was substantial. Adolescents and adults were among the most studied populations with high prevalence rates. (2) Genomic and transcriptomic studies focusing on the G × E and epigenetics were still rare, although the few available studies showed great potential to better understand the pathophysiology of PTSD as multifactorial disease. (3) Phytotherapy with Chinese herbs and acupuncture were rarely studied as of yet, although first published data indicated promising therapy effects.
However, as discussed above, the methods for assessing PTSD were not consistent, which represents a clear limitation of the current article. Methodological improvements are necessary in the future for standardized diagnostics reaching a better comparability of data. In addition, the current data ignored the spatial movement of local people, which restricts the full reliability of previously published data. Therefore, future studies should focus on the following points: (1) The affected populations under observation should be better defined concerning individual risk factor, time of observation, spatial movement, and disease courses of patients. (2) The role that social support plays in prevalence rates of PTSD should be observed in more detail. (3) Efficacy and safety of Chinese medicine should be studied to find potential interventions and effective treatments of PTSD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was funded by the DFG-graduate program 2015 “Life Science-Life Writing” at Johannes Gutenberg University, Mainz.