
Abstract
Background:
Primary care providers have an important role in identifying survivors of intimate partner violence (IPV) and providing safety options. Routine screening rates by providers have been consistently low, indicating a need to better understand providers’ practices to ensure the translation of policy into clinical practice.
Aim:
This systematic review examines common themes regarding provider screening practices and influencing factors on these practices.
Method:
A literature search was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The search focused on research articles which met the following criteria: (1) health-care providers as participants, (2) provider reports on screening and counseling practices for IPV, and (3) were in English or Spanish.
Results:
A total of 35 studies were included in the review. Across studies, providers commonly acknowledged the importance of IPV screening yet often used only selective screening. Influencing factors on clinic, provider, and patient levels shaped the process and outcomes of provider screening practices. Overall, a great deal of variability exists in regard to provider screening practices. This variability may be due to a lack of clear system-level guidance for these practices and a lack of research regarding best practices.
Conclusions:
These findings suggest the necessity of more facilitative, clearly defined, and perhaps mandatory strategies to fulfill policy requirements. Future research directions are outlined to assist with these goals.
Intimate partner violence (IPV) is defined as behaviors such as physical aggression, sexual coercion, and psychological abuse that occur within an intimate relationship and results in physical, sexual, or psychological harm and remains a prevalent global health problem (García-Moreno et al., 2015). Globally, an estimated one in three women have experienced physical and/or sexual abuse by an intimate partner. In the United States, approximately one in four women have experienced some form of IPV, including rape and other forms of sexual, physical violence, and psychological abuse (Breiding et al., 2014). The worst outcome of IPV is death—in 2013, 62% of female homicides were attributed to their husbands or boyfriends (Violence Policy Center, 2015). There is now growing recognition of the adverse effects of IPV on women’s health and well-being and increasing attention to addressing the problem in health-care settings.
The adverse health impact and health-care costs from IPV are well documented. Women who experience IPV have greater risk for chronic pain, asthma, gastrointestinal, neurological, reproductive health problems (sexually transmitted infections, human immunodeficiency virus [HIV], unintended pregnancy), and poor mental health (notably post-traumatic stress disorder, depression, substance abuse) as well as increased injury and mortality from homicide and suicide (Centers for Disease Control & Prevention, 2008; Kouyoumdjian, Findlay, Schwandt, & Calzavara, 2013; Moyer, 2013). Among subpopulations in the United States, many of these and other health-care problems are exacerbated for African American, biracial, and American Indian/Alaska Native women, contributing to health inequities for those women (Stockman, Hayashi, & Campbell, 2015). These health problems consequently impact health-care utilization and costs. In the first year after assault, the costs for providing care to adult IPV survivors range from US$2.3 to US$7 billion (Bonomi, Anderson, Rivara, & Thompson, 2009; Futures Without Violence, 2010). Even after cessation of the violence and abuse, survivors have 20% more health-care utilization compared to nonabused women. Despite the high prevalence and serious associated health concerns from IPV, primary care providers continue to miss opportunities to identify and offer support to IPV survivors.
Primary care providers have been strongly encouraged and even mandated to perform screening for IPV and support services for survivors by professional organizations (American College of Obstetrics and Gynecology, American Nurses Association, and Emergency Nurses Association) since the 1990s (Campbell, 1998). Despite these policy recommendations, studies consistently show that routine screening rates in primary care are 10% or lower and only 79% when women present to their providers with an injury (Gerber, Leiter, Hermann, & Bor, 2005; Rodriguez, Bauer, McLoughlin, & Grumbach, 1999). In 2013, the U.S. Preventive Services Task Force (USPSTF) recommended routine screening—assessing for IPV as part of care rather than targeted screening—for IPV for all women 14–46 years old (Moyer, 2013) as did the Institute of Medicine (IOM) Women’s Health Care Committee (IOM, 2011). This was adopted by the Department of Health and Human Services (HHS, 2013), making provisions in the Affordable Care Act (ACA) for primary care providers to offer routine IPV screening and brief counseling as a component of preventative care. On the other hand, the World Health Organization does not recommend universal screening and instead recommends that providers should be knowledgeable and trained on how to respond to IPV and should screen when mental and physical indicators of abuse are present.
Screening by providers is considered essential by experts in the United States, as patients have low rates of initiating disclosure of IPV and provider unconscious bias may influence providers’ recognizing indicators of abuse (Ghandour, Campbell, & Lloyd, 2015). According to a national survey on intimate partner and sexual violence, only 21% of women disclosed their victimization to a doctor or nurse (Breiding et al., 2014). This low rate of reporting may be partially attributed to the lack of universal screening for IPV as women who are asked about abuse are more likely to disclose the problem (Nelson, Bougatsos, & Blazina, 2012). In addition, IPV survivors report lack of trust or confidence in the inquiring provider as a reason for not disclosing abuse (Battaglia, Finley, & Liebschutz, 2003; Chang et al., 2005). Facilitators to this trust include nonverbal cues such as the provider sitting down, listening, and showing interest in the patient’s situation (Battaglia et al., 2003). Some survivors also want to know the provider’s intention for asking about IPV, which suggests that survivors do not assume that providers plan to offer solutions for the abuse or fears that the provider may report the abuse to child protective services or the Immigration and Naturalization Service (Kelly, 2009). The provider’s response to a patient’s disclosure of IPV is a key factor, in that survivors qualitatively report seeking nonjudgmental, nondirective, and knowledgeable responses from their providers (Feder, Hutson, Ramsay, & Taket, 2006). Thus, how the provider communicates with survivors about their abuse may be the linchpin to not only identifying survivors of IPV but also developing the critical steps of referrals and safety planning to stop the violence and improve the health and safety of the survivor.
Also, providers may have a lack of understanding or the resources necessary to address IPV. Guidelines and suggestions for primary care providers in relation to screening and counseling IPV survivors have sought to provide some clarity and standardization to providers’ care but still remain both variable and unclear. The IOM’s (now National Academy of Medicine) Clinical Preventative Services for Women report recommends universal screening in conjunction with the universal provision of local resource information to patients (IOM, 2011), and the ACA recommends that this provision of resource information be part of a verbal discussion, not just written, and calls it “brief counseling.” Likewise, relationships between providers and local IPV service professionals are stressed as important for assisting in a coordinated referral system for patients who are IPV survivors. The USPSTF suggests that provider counseling “generally includes information on safety behaviors and community resources” and acknowledges that there is a lack of evidence-based practices for interventions after screening (Moyer, 2013). Reviews of the evidence around screening have shown that screening by itself does not increase safety for abused women (O’Doherty et al., 2014) in clinical trial comparisons, making it all the more important to develop best practices for providers in regard to screening and especially for developing and testing brief interventions to fulfill the mandate for counseling patients for IPV (Ghandour et al., 2015).
In acknowledgment of the challenges health-care workers face with IPV screening practices, organizations have offered guidelines on how to screen and counsel patients (Family Violence Prevention Fund, 2004; Warshaw, Ganley, & Salber, 1995). Further, multiple screening tools have demonstrated efficacy in identifying abuse (Basile, Hertz, & Back, 2007; Nelson et al., 2012; Rabin, Jennings, Campbell, & Bair-Merritt, 2009; Singh, Petersen, & Singh, 2014). These tools range in length and purpose, from single-item screening questions to danger assessment (DA) which assesses lethality potential, and have examined usage during primary care visits and other care such as in prenatal care settings (Campbell, Webster, & Glass, 2009).
This article is a review of research on providers’ screening and counseling practices for IPV. In particular, screening practices are examined, including rates of screening, who is screening, how screening is performed, responses to screening, influencing factors on screening, and results of studies of interventions for providers designed to improve screening practices. Learning more about the screening and counseling process from the provider perspective in settings both in the United States and abroad can help inform best practices to increase screening and improve the primary care sector response for IPV.
Method
Data Sources and Searches
We first built a search strategy with the help of a librarian who is trained as a clinical informationist. Our searches used Medical Subject Headings (MeSH) terms and key word searches for “providers,” “screening,” “counseling,” and “intimate partner violence” or “domestic violence.” No time parameters were imposed on the search. The database searches were conducted in January 2015 using PubMed, Embase, Cochrane, CINAHL, Scopus, and Web of Science, given these are considered the leading databases for health-care literature.
Study Selection
To be considered for review, articles had to be an original study concerned with screening and/or counseling for IPV among women. The articles were then reviewed for the following criteria: (1) included “frontline” health-care providers (e.g., nurses, physicians, nurse practitioners, nurse-midwives, and/or physician assistants) as participants, (2) addressed screening and counseling practices of IPV in women, (3) were in English or Spanish. Studies in which only screening rates were provided (i.e., provider screening for IPV was 15%) without further detail on frequency were excluded. Two authors independently reviewed titles and abstracts for relevance; differences in study selection were discussed and reconciled. Most articles were eliminated because they only included patients as participants and did not address the provider perspective.
Data Evaluation and Analysis
Two authors independently abstracted data on study aims, study design, sample characteristics, study setting, data collection procedures, and key findings pertaining to screening practices as well as how providers may respond and counsel patients upon disclosure of IPV. This information was systematically recorded via a data abstraction form and was compiled within an electronic database. These data were reviewed for accuracy by both the authors.
We evaluated study quality using the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist for observational/cross-sectional studies and criteria developed by Kitto, Chesters, and Grbich (2008) to assess the qualitative studies. The criteria for qualitative research included assessing for clarity of research aims/questions, justification for a qualitative approach, procedural rigor, sampling technique, linking findings to theory, evaluative rigor, and transferability of findings. Two authors independently rated the quality of the studies and then discussed the ratings and reconciled differences.
Results
The literature search yielded 4,441 articles, upon application of the inclusion criteria and review of titles and abstracts, 35 articles were included for review (Figure 1). The included qualitative (n = 13), quantitative (n = 22), and mixed-methods (n = 1) studies focused on provider IPV screening attitudes and screening practices, including frequency of screening. STROBE scores for the quantitative studies averaged 13.96, indicating that overall most studies did not provide a lot of detail to determine veracity of the findings; scores ranged from 10 to 18. Response rates for the quantitative studies ranged from 24% to 97%, however, almost half of the studies reported response rates of less than 50%; two studies had response rates greater than 90%. Most of the qualitative studies did not meet the 15 quality criteria from Kitto et al. (2008). Often missing from the studies were justification for qualitative methods, representativeness of the sample, linking results to theory, negative cases, and explanation of the researcher’s view and relationship with participants. Review of the qualitative articles included a thematic synthesis by the authors. Tables 1 and 2 provide summaries of the studies included.
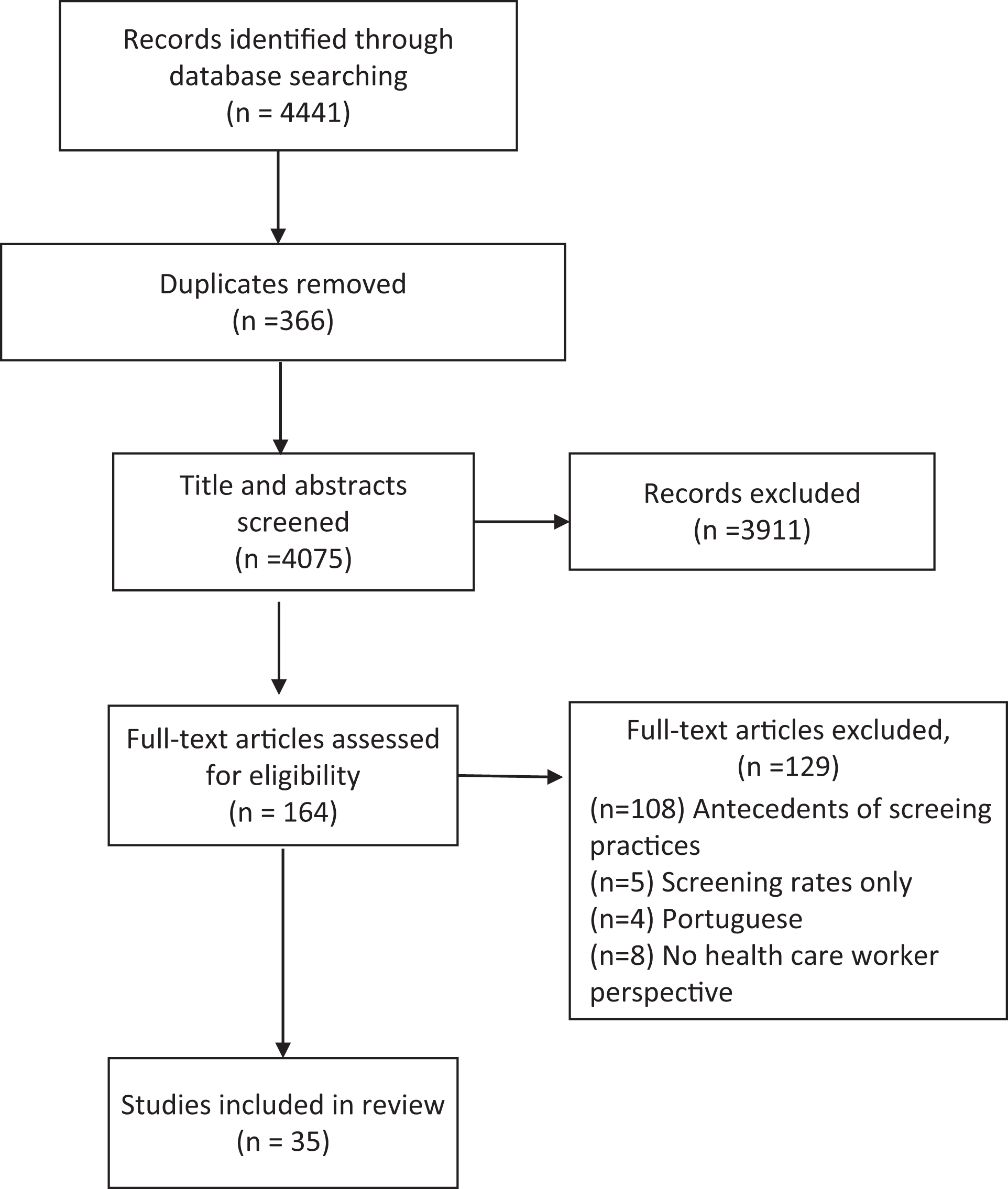
Flowchart for selection of eligible articles.
Overview of Quantitative Studies Included in Systematic Review.
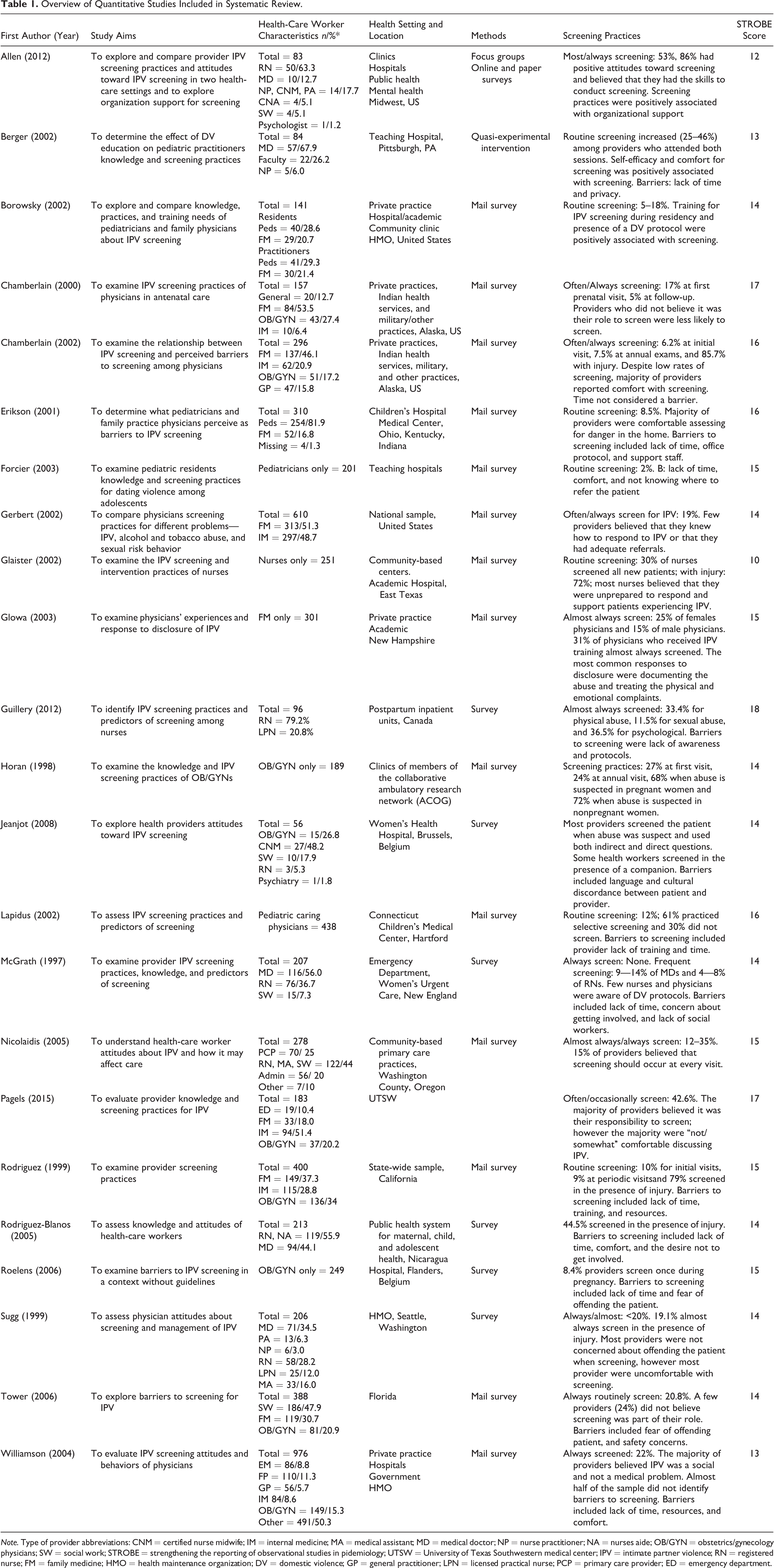
Note. Type of provider abbreviations: CNM = certified nurse midwife; IM = internal medicine; MA = medical assistant; MD = medical doctor; NP = nurse practitioner; NA = nurses aide; OB/GYN = obstetrics/gynecology physicians; SW = social work; STROBE = strengthening the reporting of observational studies in pidemiology; UTSW = University of Texas Southwestern medical center; IPV = intimate partner violence; RN = registered nurse; FM = family medicine; HMO = health maintenance organization; DV = domestic violence; GP = general practitioner; LPN = licensed practical nurse; PCP = primary care provider; ED = emergency department.
Overview of Qualitative Studies Included in Systematic Review.
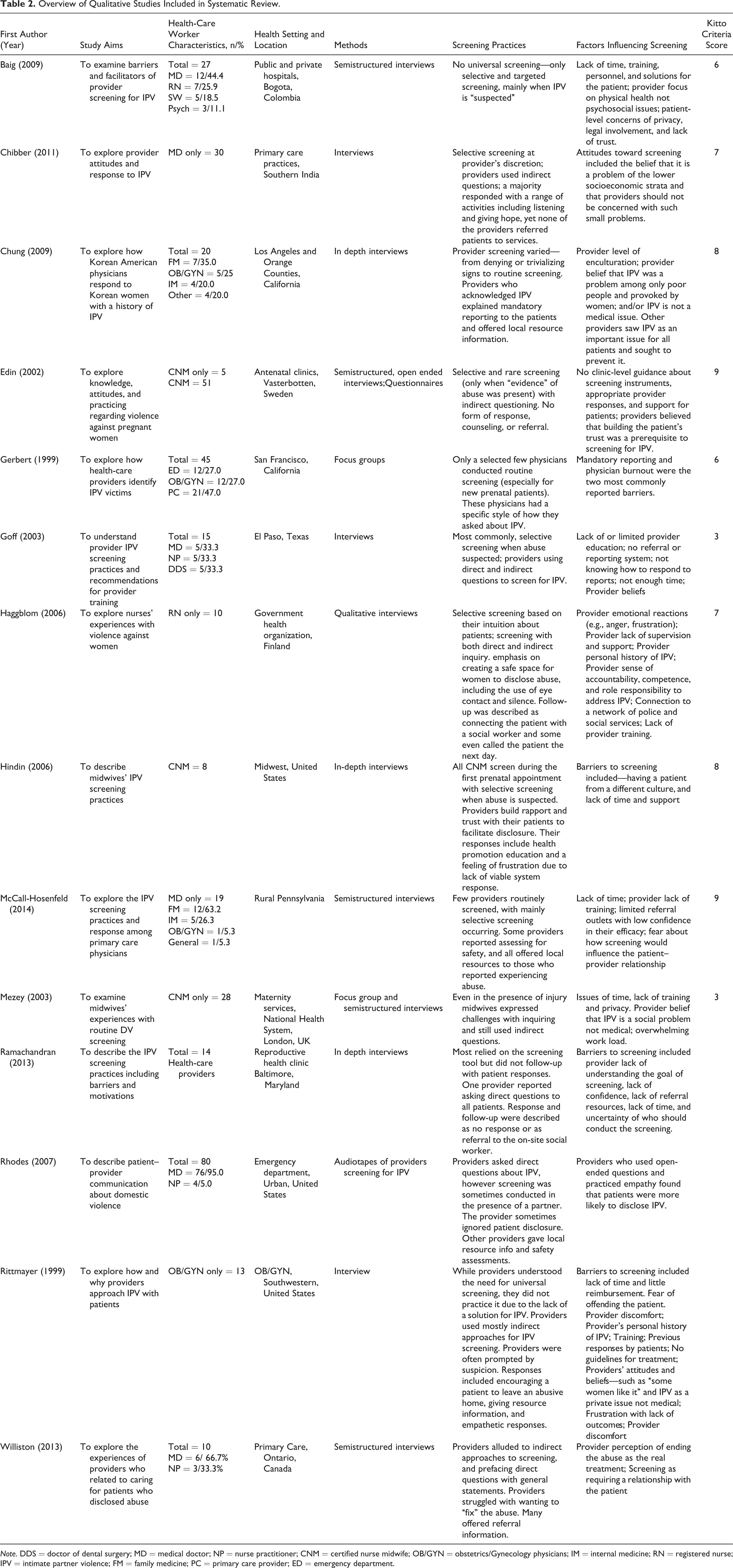
Note. DDS = doctor of dental surgery; MD = medical doctor; NP = nurse practitioner; CNM = certified nurse midwife; OB/GYN = obstetrics/Gynecology physicians; IM = internal medicine; RN = registered nurse; IPV = intimate partner violence; FM = family medicine; PC = primary care provider; ED = emergency department.
Eighteen studies included physicians only and twelve studies included a mix of health-care workers—nurses, dentists, social workers, and medical assistants. Six studies had nursing only study samples. Most studies also included providers from an array of specialties (n = 20); other provider samples were from family medicine (n = 5), obstetrics and gynecology (n = 7), and pediatrics (n = 4). Twenty-five studies were conducted in the United States; other countries included Belgium (n = 2), Canada (n = 2), Colombia, England, Finland, India, Nicaragua, and Sweden.
Almost all articles reported on descriptive studies based on surveys to providers; two articles were exceptional. We identified one intervention designed to increase screening for IPV among pediatric practitioners through training sessions (Berger, Bogen, Dulani, & Broussard, 2002). Another study used audio recordings of real patient–provider encounters and captured “live” provider screening practices for IPV (Rhodes et al., 2007). The providers being recorded were those who had recently received a 1-hr lecture and viewed a 30-min video on responding to IPV. Thus, these two studies looked at the effects of provider training for screening outcomes.
Screening Practices
Rates of routine screening were typically low, with a range of 2–50% of providers reporting always or almost always routinely screening for IPV. Notably, the definitions of “routine screening” also varied in terms of the frequency across clinics and providers. For example, “routine” meant at every visit for some providers, and for others, only at every annual exam or as for obstetricians, at the first prenatal care visit. Selective screening was more commonly endorsed, specifically in the presence of injury, for which screening rates ranged from 45% to 85%. Similarly, findings from qualitative studies revealed that screening for IPV was at the providers’ discretion and influenced by whether the provider believed the patient to be at risk (Chibber, Krishnan, & Minkler, 2011). Reasons for suspecting IPV included the presence of injury or if the patient raised “problems in the home” (Baig, Ryan, & Rodriguez, 2009). Further, the providers’ narrative suggested that they believed they could “tell” when a patient is experiencing abuse and would screen in those moments of suspicion (Chibber et al., 2011; Goff, Shelton, Byrd, & Parcel, 2003; Hindin, 2006).
Most studies included samples of a wide array of medical providers (e.g., nurses, doctors, physician assistants, mental health professionals) from a variety of specialty areas (e.g., obstetrics, pediatrics, family medicine, emergency, and generalist). One study that had a sample of 50% nurses had the highest routine screening rate of 53% (Allen, Larsen, Javdani, & Lehrner, 2012) and samples of only nurses had rates of 30–36% (Glaister & Kesling, 2002; Guillery, Benzies, Mannion, & Evans, 2012). In contrast, studies with samples of all doctors had lower rates; for pediatricians screening mothers, a routine screening rate of 2–18% (Forcier, Patel, & Kahn, 2003; Garry et al., 2002) and physicians from 6% to 31% (Chamberlain & Perham-Hester, 2000, 2002; Erickson, Hill, & Siegel, 2001; Gerbert et al., 2002; Glowa, Frasier, Wang, Eaker, & Osterling, 2003; Horan, Chapin, Klein, Schmidt, & Schulkin, 1998; Rodriguez et al., 1999; Sugg, Thompson, Thompson, Maiuro, & Rivara, 1999; Williamson et al., 2004). One study in particular found that type of provider specialty was the strongest predictor of screening (Williamson et al., 2004). The range of providers involved in screening is a positive finding, as it is not just one provider’s role to screen but rather a clinic-wide responsibility that spans providers of different types and specialty areas. A clinic-wide responsibility would also include other members of a health-care team who may also be involved in the screening process, for example, medical assistants, clerks, or certified nursing assistants. While recommendations often do not suggest that these types of health-care workers implement screening, medical assistants and clerks are often involved in distributing and collecting screens or, even more broadly, are involved in seeing the patient, hearing patient concerns, and other key aspects of care. The perspectives of these other health-care workers, however, are lacking in the existing literature.
How are providers screening?
Provider screening for IPV was completed via an array of strategies and with a variety of screening styles. In terms of assessing for IPV, providers broached the topic of IPV with patients using general and nonthreatening questions such as—“How are you feeling?” “How are things going in your life?” and “Happy at home?” One study that audio recorded how providers were screened in an emergency department revealed some examples about how providers directly inquired about IPV (Rhodes et al., 2007). Examples included—“Are you a victim of domestic violence?” or “Any problems with domestic violence?” “Has anyone used you as a victim?” Some providers also initiated the screening with a general, nonjudgmental statement about domestic violence such as “I’m going to ask you a question that I ask all women.” None of the studies reported on how the phrasing of the question may have affected the patient’s response.
In regard to screening style, some providers specified strategies they use to facilitate screening and that dictate how they ask their screening questions. These providers shared strategies such as conducting the screening in a safe environment (e.g., when the patient is not with her intimate partner), waiting quietly and allowing time for the patient to respond, and maintaining eye contact with the woman (Gerbert et al., 2002; Haggblom & Moller, 2006). In addition, select providers described trying to create a comfortable, safe space and developing a rapport with the patient prior to inquiring about IPV. However, these style factors varied across providers, as contrary to asking about IPV in a safe space, some findings revealed that providers screen for IPV in the presence of the patient’s partner (Rhodes et al., 2007).
One study alluded to the use of screening tools (Ramachandran, Covarrubias, Watson, & Decker, 2013). However, there was no detail provided about the screening tool itself. Health-care workers of a health department gave the tool to incoming patients and were then supposed to review the responses with the patient. Results revealed that providers did not verify responses with patients. If responses were not reviewed, it is possible that affirmative responses were overlooked and no intervention was offered to the survivor.
How are providers responding?
For the most part, studies examined only provider practices around screening, not responses (e.g., Edin & Högberg, 2002). Only two studies revealed how providers respond to women disclosing IPV as part of their study’s research aims (McCall-Hosenfeld, Weisman, Perry, Hillemeier, & Chuang, 2014; Rhodes et al., 2007). Providers’ responses were mostly described within the qualitative studies in the context of exploring provider screening practices. Responses ranged from a lack of response (e.g., not acknowledging the disclosure of abuse) to just referral (e.g., to offering pamphlets with available resources) to two-component response (e.g., providers demonstrating empathy and discussing safety planning). Responses also included providers counseling women not to provoke or confront their spouses (Grace, Ramona, & Jennifer, 2009). Lastly, some providers also reported calling the patient to follow-up after screening and counseling, however, it was unclear what these discussions entailed or the result of such discussions (McCall-Hosenfeld et al., 2014).
Overall, not only was there variation across studies, but there was also a great deal of variation within studies (even within one clinic) about provider responses, from ignoring positive responses to referring to local resources (McCall-Hosenfeld et al., 2014; Ramachandran et al., 2013; Rhodes et al., 2007). For example, a study of providers’ responses in different states showed that in one state, providers only documented the abuse in the patient’s record and treated physical injuries versus in another state, providers responded by advising the patients to leave their partner (Glowa et al., 2003). Another study found that the provider’s enculturation level shaped their screening and response behaviors, resulting in providers who ignore or even blame the patient for IPV to providers who respond to patients by informing them of the state’s mandatory reporting policy, performing safety planning, and offering local resources (Grace et al., 2009).
With examination of providers who did respond to patients’ disclosure of IPV, two main aspects of these responses were elicited: (1) providing referrals and local resource information and (2) utilizing empathy and specific interpersonal stylistic factors as a response (e.g., Rittmayer & Roux, 1999; Williston & Lafreniere, 2013). Some providers only provided referrals (Grace et al., 2009; Rittmayer & Roux, 1999; Williston & Lafreniere, 2013), some only responded with emphatic listening (Chibber et al., 2011), and some sought to do both responses (Haggblom & Moller, 2006). The variety of responses mirrors the ambiguous definition of counseling present in national policy recommendations. Also, these varied responses show inconsistencies for care provided to patients who are experiencing IPV. No study examined or compared the effectiveness of these responses.
Factors Influencing Screening Practices: Barriers and Facilitators
Across studies, several logistical factors influenced screening practices. One logistical factor was ensuring patient privacy (Berger et al., 2002; Haggblom & Moller, 2006; Mezey, Bacchus, Haworth, & Bewley, 2003), another was lack of reimbursement for this type of screening (Rittmayer & Roux, 1999). In particular, lack of time was a frequently cited barrier to screening. However, time alone is not enough to explain screening practices. For example, for Chamberlain and Perham-Hester (2002), only 6% of providers routinely screened and did not consider time a barrier. Other influencing factors across studies pertained to clinic-level, provider-level, and patient-level factors.
Clinic-level factors
At the clinic level, the presence or absence of a protocol for providers’ screening practices was a key influencing factor. Clinic-level protocols for how to screen and respond were cited as facilitating these practices (Allen et al., 2012; Borowsky & Ireland, 2002). Specifically, protocols were suggested to include detailed ways that providers can respond to patients experiencing IPV and resources for their patients (Forcier et al., 2003; Gerbert et al., 2002). Also, the inclusion of the clinic’s definitions of provider responsibilities and even details about which provider does the screening (Ramachandran et al., 2013) have been stressed as essential components. A lack of a protocol was cited as a barrier for providers (Erickson et al., 2001; Guillery et al., 2012), resulting in providers feeling unprepared for screening (Glaister & Kesling, 2002).
Clinic-level solutions and implications were often provided across studies, suggesting “top-down” (Goff et al., 2003, p. 144) assistance to improve practices. Suggestions included standardized screening and documentation such as adding screening questions to routine forms, provider training about local resources and legal responsibilities by the provider, and a coordinated system of response to reporting that is tailored to the clinic (Baig et al., 2009; Goff et al., 2003; Guillery et al., 2012; Haggblom & Moller, 2006; Edin & Högberg, 2002; Mezey et al., 2003; Rittmayer & Roux, 1999; Roelens, Verstraelen, Van Egmond, & Temmerman, 2006). These clinic-level resources were also often described as needed in addition to educational and training opportunities for providers and with a specific emphasis on the need for both resources and education/training (Borowsky & Ireland, 2002; Mezey et al., 2003). Overall, positive clinic-level factors could be described as organizational, formal support that facilitates consistent, best practices by all providers with support between and across providers and health administrators (Haggblom & Moller, 2006)—in other words, a “systems model to IPV screening programs” (Ramachandran et al., 2013, p. 856). Earlier studies have also shown the usefulness of system-level change (Campbell et al., 2001), as well as the recommendations recently made by Miller and colleagues (Miller, McCaw, Humphreys, & Mitchell, 2015), such as how to maximize electronic health records for better identification and management of IPV.
Provider-level factors
A majority of studies focused on provider attitudes, beliefs, and perceptions of screening for and responding to IPV. These studies elicited several key provider-level factors: provider level of knowledge of IPV, comfort, self-efficacy, level of enculturation, and sense of responsibility or role in screening for IPV. Low levels of these factors were connected with lower rates of screening and limited responses (e.g., Chamberlain & Perham-Hester, 2000; Grace et al., 2009; Meghan et al., 1997; Pagels et al., 2015; Rodriguez-Bolanos, Marquez-Serrano, & Kageyama-Escobar, 2005; Sugg et al., 1999; Tower, 2006; Williamson et al., 2004). Also, of importance, a few qualitative studies found that a provider’s personal history of experiencing IPV was a factor in how they screened and approached patients (Haggblom & Moller, 2006; Rittmayer & Roux, 1999). Thus, both providers’ skills and intrinsic feelings about the screening practices were found to be influencing factors.
Overall, the studies revealed that most providers have positive attitudes toward screening for IPV. Positive attitudes were found more often with providers who have a high rate of routine screening (Allen et al., 2012). The few exceptions included specific negative beliefs about IPV as a “personal issue” for patients (Rodriguez-Bolanos et al., 2005), a problem for only a certain group of patients (Chibber et al., 2011), a result of the patient’s poor decision-making or personal preference (Grace et al., 2009; Rittmayer & Roux, 1999), a behavioral issue that is not in the realm of physical health care (Baig et al., 2009; Grace et al., 2009), or as a social issue (Williamson et al., 2004). These negative beliefs were connected to providers’ decisions not to screen for IPV or to respond in limited ways.
Lastly, a major influencing factor was providers not having a clear referral system for IPV survivors (Forcier et al., 2003; Gerbert et al., 2002; Glaister & Kesling, 2002; Meghan et al., 1997) or not having a solution to be able to offer to patients (Baig et al., 2009). In conjunction, providers described not having a sense of making a difference in patients’ lives due to screening (Gerbert et al., 2002) and a sense of frustration in not having a viable response with proven positive outcomes (Haggblom & Moller, 2006; Hindin, 2006; McCall-Hosenfeld et al., 2014). A corresponding factor was the provider perception of the solution or treatment for a diagnosis of IPV. For example, providers who viewed IPV from a strictly medical perspective only treated injuries (Baig et al., 2009). Some providers endorsed the solution/treatment for IPV as getting a patient to leave an abusive home but also described having no tools or ability to accomplish this goal (Rittmayer & Roux, 1999; Williston & Lafreniere, 2013). Thus, not being able to stop the abuse was perceived as a reason to not screen (Rittmayer & Roux, 1999) and not to respond (Goff et al., 2003).
Provider-perceived patient factors
Several studies found provider-perceived patient factors as key influences on screening practices. In particular, language and culture discordance between provider/patient was a barrier (Hindin, 2006). One study with midwives revealed that despite signs of physical abuse the provider did not screen citing fear and discomfort with another culture as a reason (Hindin, 2006). In another scenario, a Spanish-speaking patient disclosed being abused. The midwife was not fluent in Spanish and had challenges finding an interpreter; it remained unclear how the midwife responded to the patient and what type of support she was able to offer (Chamberlain & Perham-Hester, 2000).
In relation to communication, providers have expressed a fear of offending the patient or of disrupting the patient–provider relationship (McCall-Hosenfeld et al., 2014; Rittmayer & Roux, 1999; Roelens et al., 2006; Tower, 2006). Indeed, some providers have expressed needing to build a trusting relationship with patients before screening, given the nature of the inquiry which requires time and repeated visits (Edin & Högberg, 2002; Williston & Lafreniere, 2013). The style and quality of communication between providers and patients were cited as key aspects (Haggblom & Moller, 2006; Roelens et al., 2006).
Screening and Response Intervention Studies
Only two studies examined provider outcomes from interventions to improve screening practices. One intervention offered providers two training sessions, which demonstrated a modest effect on screening practices (Berger et al., 2002). There was a greater report of screening at 6 months postintervention. Although this increase was significant (25–46%), half of the providers still did not report routine screening. In addition, the intervention had no effect on attitudes and comfort with screening, and there was no report on screening 1 year after the intervention. Rhodes and colleagues (2007) also offered trainings on IPV to providers and presented audio recording of provider inquiry and response to IPV posttraining. Despite the training, some providers still demonstrated poor screening practices such as inquiring about IPV in front of their patients’ intimate partners and sometimes ignoring disclosures of abuse. These findings suggest that training sessions alone may not suffice for changing screening practices and further underscore the need for testing the efficacy in terms of actual behavior change of training modules for all of family violence first called for by the IOM Report in 2002—Confronting chronic neglect: The education and training of health professionals on family violence (Salmon, Stobo, & Cohn, 2002).
Discussion
Despite the ubiquity of IPV and its health implications, our findings demonstrate that overall, health-care workers remain challenged in screening and appropriately responding to IPV. This challenge exists regardless of provider type, specialty, and country. Considering the opportunity and importance of identifying and responding to IPV in the primary care setting, this review shows serious limitations in our evidence base so far. However, this review points to several key areas of future research and implications for practice.
One commonly proposed solution across the reviewed articles for improving screening practices is to train providers and health-care workers in IPV. However, the limited intervention literature consists of only two studies (Berger et al, 2002; Rhodes et al., 2007) and displays that training alone is not sufficient in producing consistent improvement across all providers or over time. A theme that emerged from this review is the need for personnel and systems support in order to improve IPV screening. In addition, efforts to improve screening need to address multilevel factors influencing these practices—on the clinical, provider, and patient levels, a model similar to the one developed and recommended by Hamberger, Rhodes, and Brown (2015). These kinds of models need to be rigorously tested in real-world clinical trials for cost benefit as well as effectiveness, so that sustained system change can be achieved (Ghandour et al., 2015).
Another dominant theme throughout the studies is that providers lack organizational support for appropriate screening and responding to IPV. In the midst of a busy clinical practice, one can understand how problems with no clear solution may overwhelm a provider and as a result be overlooked. None of the studies reported on an interdisciplinary approach to screening. Most provider reports of screening suggested that inquiring and responding to disclosures of abuse involved only the provider. None of the studies presented on how providers may work with other health-care workers to respond to abuse. In reviewing successful screening programs, researchers found that successful programs included on-site availability of staff who could support the needs of the survivor (O’Campo, Kirst, Tsamis, Chambers, & Ahmad, 2011) and also continuous training for all levels of staff (Plichta, 2007), which may assist with real-time challenges and addressing barriers to screening. The availability of such support staff may help providers overcome the barriers of not having a solution for the patient and thereby increase screening for IPV.
In order to help inform which health-care workers are best positioned to screen and respond to IPV, more studies are needed on how other members of the health-care team can contribute to IPV screening. Most of the studies represented in this sample focused on physicians. The few studies that did include a nursing majority, or nursing only sample (Allen et al., 2012; Glaister & Kesling, 2002; Guillery et al., 2012), suggest that nurses may be more likely to screen for IPV, despite facing similar barriers (Haggblom & Moller, 2006; Hindin, 2006; Edin & Högberg, 2002; Mezey et al., 2003) as physicians. However, we know less about whether nurses respond much differently than other providers. Likewise, medical assistants, clerks, and other forms of medical professionals may not be the main providers responding to formal forms of IPV screening but are still interacting with patients and may encounter patient disclosures of IPV. As members of health-care teams, such providers may offer insight into additional steps to consider for screening and responding to IPV.
Interestingly, as lack of clear clinic-level support and protocol were detailed across studies and despite the many existing standardized screening tools for IPV (Basile et al., 2007; Rabin et al., 2009), there was little mention of their use in our sample of studies. Further, there was no mention of the use of the DA (Campbell et al., 2009), an evidence-based instrument for predicting the likelihood of the worst outcome of IPV—intimate partner homicide. Helping an IPV survivor objectively recognize her risk of being killed in a relationship could heighten the perceived urgency of the matter for both providers and survivors, thereby minimizing the tendency of some health-care providers to trivialize IPV. A benefit of these instruments is that they are self-administered, thereby eliminating the provider-reported barrier of fear and discomfort with inquiring about IPV. The increasing advances in technology may offer some solution to increasing screening for IPV. Research suggests that computerized screening is an effective mode of screening to deal with vulnerable women as it allows for easier disclosure of abuse and minimize the feelings of being judged (Chang et al., 2005; MacMillan & Feder, 2012; Rhodes, Lauderdale, He, Howes, & Levinson, 2002; Trautman, McCarthy, Miller, Campbell, & Kelen, 2007). More research is needed on how patients’ self-administered computerized screening can become part of the medical chart as well as require follow-up and intervention by the health-care team. There is also an online IPV intervention (decision aid) that is being tested in a randomized control trial (RCT) and already has shown to decrease women’s decisional conflict about what to do about the abusive relationship (Eden et al., 2015). This kind of decision aide could be made available to women in the primary care setting on portable tablets or computer stations to decrease problems of safe and affordable access to online technology. The online decision aid has also been programmed as an app (One Love MyPlan app—OneLove Foundation—www.joinonelove.org) that is also being tested in an RCT (Glass, 2014).
The studies included in this review were mostly quantitative with still a substantial number of qualitative studies. However, there was only one mixed-methods study meeting inclusion criteria. Future research may also benefit from a rigorous mixed-methods design in order to test variables, such as screening rates and other outcomes, as well as explore underdeveloped areas (e.g., the perspective of medical assistants and their participation in the screening and referral process.)
Limitations
The most glaring issue for this review was that a vast majority of the literature on screening practices focuses exclusively on screening—without attention to the screening forms and outcomes of providers’ responses to IPV survivors. A major concern is that while policy recommendations include counseling, there is no clear definition or model of response to guide providers’ practices. The range of responses from ignoring to (Rhodes et al., 2007)safety planning (McCall-Hosenfeld et al., 2014) which leaves little guarantee that survivors of IPV will receive uniform or even a base standard of care after disclosing IPV. In addition, none of the studies evaluated the outcomes from different forms of providers’ responses. It is unclear what happens in regard to provider follow-up with patients after disclosure and provider response. Without research about the multiple steps of the screening responses, it is difficult to define best practices in a thorough and comprehensive manner, contributing to cautionary perspectives about primary care providers screening practices (MacMillian et al, 2009; O’Doherty et al., 2014).
Another important limitation in the review was the lack of systematic attention to how screening practices may need to be tailored to specific marginalized and vulnerable populations such as immigrant women, non-English-speaking women, women of color, women who identify as lesbian, transgender or bisexual, adolescents, and pregnant women. These women may have particular concerns about confidentiality of their disclosure as well as further stigmatization and the cultural appropriateness of any referrals. Other particularly vulnerable women are those who are subject to multiple victimization (e.g., trafficked women who are also abused by an intimate partner; adolescent girls who are abused by a family member and a dating partner) and women who are suicidal as a result of IPV or highly at risk to be killed. Also important will be tailored referrals and protocols for survivors whose health-care conditions are the result of or complicated by current or prior IPV (e.g., abused women who are depressed, and/or substance abusers [including cigarettes] and/or HIV+ women or those highly at risk for HIV, and/or those who have neurological disorders or other disability as a result of head injuries or strangulation from IPV). There have been increased specific attention to these women with suggestions for research and programs for them (Ghandour et al., 2015; Weaver, Gilbert, El-Bassel, Resnick, & Noursi, 2015), and although much work remains to be done an increasing interdisciplinary group of health-care professionals is committed to improving the health-care system response to IPV.
There was a range in the quality of studies identified for this review. Overall, both the quantitative and the qualitative studies lacked the detail to demonstrate the veracity and credibility of the evidence. Only one study reported on live provider screening and response to IPV. Given our focus on how providers screen for and respond to IPV, our findings did not include the patient perspective on how IPV survivors respond to the different styles of IPV screening.
Recommendations for Improving Screening for IPV
Improving screening and response to IPV may require following protocols for other chronic care models. Researchers have shown that addressing other health problems, such as diabetes (Chin et al., 2007; Larsen, 2007) and colon cancer screenings (Taplin et al., 2008), improved not only with establishing system-level changes to encourage better management but also establishing and routinely measuring indicators to validate the quality of care provided by health clinics. Similar to how health clinics have to report on the control of their patients with diabetes and whether these patients have received the recommended foot and eye exams, requiring this level of detail for care of IPV survivors may also be needed.
Similarly, a model of trauma-informed care may help guide future research of best practices and guide the translation of policy into clinical practices. Indeed, trauma-informed primary care is suggested as an evidence-based strategy to address the myriad of patients’ needs efficiently and to effectively address health disparities (Browne et al., 2012). Likewise, trauma-informed interventions are being tested in primary care settings and indicating preliminary positive outcomes (e.g., Ford-Gilboe, Merritt-Gray, Varcoe, & Wuest, 2011; Substance Abuse and Mental Health Services Administration, 2014).
Conclusion
In summary, given the centrality of these clinic and provider-level factors, it is clear that training alone on IPV screening and brief counseling will not suffice. There needs to be system change in the overall health-care system and in individual health-care settings. The recommendations of the IOM, USPSTF in 2013 leading to the provisions of the ACA have given us a perfect opportunity to build on what is known from this review from the provider perspective to combine with other reviews of research on the effectiveness of IPV interventions and patient perspectives and concerns about screening to develop screening and brief counseling protocols that can be particularized to setting and patient population. These also can be used by a wide variety of health-care providers, integrated into electronic medical records and other computerized and smart phone applications and then tested in real-world multisite effectiveness trials as is being done for other health conditions.
Implications for Policy, Practice, and Research
Health-care settings should be incentivized to implement practices which support trauma-informed care Health-care settings should maximize the use of technology to optimize screening and planning care for survivors of IPV Health-care settings should routinely train, support, and hold health-care workers accountable on appropriately responding to disclosures of IPV Future interventions for screening and responding to IPV should consider and test applicability in health-care settings
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:Karen Trister Grace’s work on this publication was made possible by the Johns Hopkins Institute for Clinical and Translational Research (ICTR) which is funded in part by Grant Number TL1 TR001078 from the National Center for Advancing Translational Sciences (NCATS) a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, NCATS or NIH.