
Abstract
This article presents the results of a systematic review of the consequences of elder abuse and neglect (EAN). A systematic search was conducted in seven electronic databases and three sources of gray literature up to January 8, 2016, supplemented by scanning of citation lists in relevant articles and contact with field experts. All observational studies investigating elder abuse as a risk factor for adverse health outcomes, mortality, and health-care utilization were included. Of 517 articles initially captured, 19 articles met our inclusion criteria and were analyzed. Two reviewers independently performed abstract screening, full-texts appraisal, and quality assessment using the Newcastle–Ottawa Scale. Across 19 studies, methodological heterogeneity was a prominent feature; seven definitions of EAN and nine measurement tools for abuse were employed. Summary of results reveals a wide range of EAN outcomes, from premature mortality to increased health-care consumption and various forms of physical and psychological symptoms. Higher risks of mortality emerged as the most credible outcome, while the majority of morbidity outcomes originated from cross-sectional studies. Our findings suggest that there is an underrepresentation of older adults from non-Western populations and developing countries, and there is a need for more population-based prospective studies in middle- and low-income regions. Evidence gathered from this review is crucial in upgrading current practices, formulating policies, and shaping the future direction of research.
Elder abuse and neglect (EAN) has been increasingly recognized as a global threat to public health. With the booming of older populations across the globe especially in middle- and low-income countries, EAN is expected to intensify. A systematic review by Cooper, Selwood, and Livingston (2008) found that the prevalence of EAN worldwide ranged from 3.2% to 27.5%, whereas the prevalence in developing nations was reported to be from 13.5% to 28.8% (Sooryanarayana, Choo, & Hairi, 2013). Published figures, however, are believed to be underestimates, with the actual magnitude of EAN being much higher than what is recorded (Lachs & Pillemer, 2015; Saveman, Åström, Bucht, & Norberg, 1999).
As EAN goes across cultures and geographical boundaries, reaching a consensus on a single definition has been an impasse. There are, however, a number of widely accepted definitions for EAN, one offered by the Action on Elder Abuse in the United Kingdom and World Health Organization (WHO, 2016) (https://www.cdc.gov/violenceprevention/elderabuse/definitions.html) reads: “a single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person” (Dixon et al., 2010, pp. 403–420). This definition is also adopted by the International Network for the Prevention of Elder Abuse (WHO, 2016) and is by far the most commonly used one. Similarly, the Centers for Disease Control and Prevention (CDC, 2016) defines elder abuse as “an intentional act, or failure to act, by a caregiver or another person in a relationship involving an expectation of trust that causes or creates a risk of harm to an older adult.” It is important to note that these constructs are heavily influenced by the work done in Canada, the United Kingdom, and the United States. Studies from countries such as Finland, Greece, India, Israel, Norway, and South Africa among others were said to have approached this subject differently (WHO, 2015).The Chinese society, for instance, regards the failure of family members to fulfill their kinship obligations toward older parents such as provision of housing and food as a form of abuse (WHO, 2015). EAN is categorized into five subgroups—physical, verbal or psychological, sexual, financial, and neglect (Laumann, Leitsch, & Waite, 2008)—with a newer type, social abuse, being highlighted recently (Yi, Honda, & Hohashi, 2015).
Various adverse health impacts of abuse in late life have been documented in the scientific literature. Abused older adults have been reported to be at higher risks of mortality (Dong et al., 2009; Lachs, Williams, O’Brien, Pillemer, & Charlson, 1998) and were more likely to experience disability (Schofield, Powers, & Loxton, 2013), depressive symptoms (Mouton, Rodabough, Rovi, Brzyski, & Katerndahl, 2010), hospitalization (Dong & Simon, 2013b), and nursing home placement (Lachs, Williams, O’Brien, & Pillemer, 2002) compared to those not abused. Similarly, associations between EAN and metabolic syndrome (Dong & Simon, 2015), sleeping problems (Olofsson, Lindqvist, & Danielsson, 2012), chronic pain (Fisher & Regan, 2006), gastrointestinal symptoms (Stöckl & Penhale, 2014), suicidal ideation (Wu et al., 2013), and stress and anxiety (Olofsson et al., 2012) have been reported in comparison to elder counterparts who never experienced EAN.
Nevertheless, these relationships are often not straightforward; they are to a great extent, influenced by various confounding, mediating, and moderating factors. For instance, the link between abuse and mortality was found higher among elders with greater levels of depression and poorer social network (Dong et al., 2010). Other studies (as mentioned above) acknowledged sociodemographic factors (e.g., age, gender, ethnicity, and income) as important confounders besides health-related variables (e.g., cognitive status, comorbidities), psychosocial variables (e.g., depression, social support), and substance use (e.g., smoking, alcohol). Likewise, gender was shown to moderate numerous impacts of abuse including musculoskeletal pain, digestive problems, headache, incontinence, allergy, anxiety, stress, suicidal ideation, and sleeping problem (Olofsson et al., 2012). This demonstrates a rather complex dynamic and interplay between abuse as a form of chronic stressor and its consequences.
Anetzberger (2012) in 1997 proposed a conceptual framework delineating the effects of elder abuse. The theory posits that outcomes of abuse are influenced by meaning; the manner in which an older individual perceives his or her experience of being mistreated. This perception in turn is a result of an interplay between cultural norms and beliefs, the nature of mistreatment, the relationship between the perpetrator and the victim, and the victim’s personal values and worldview. “Meaning” determines the response elicited, which subsequently influences the types and nature of outcomes. Health consequences of elder abuse were divided into four categories: physical, behavioral, psychological, and social (Anetzberger, 2012). Despite the limited number of available theoretical frameworks on health impacts of EAN, the connection can be postulated and understood from studies on other forms of family violence, like child abuse. In a study on long-term health impacts of child abuse, four pathways—behavioral, social, cognitive, and emotional—were identified through which mistreatment and abuse experiences influence health (Kendall-Tackett, 2002).
Preventive measures and intervention programs pertaining to EAN are expanding worldwide, albeit at different speeds across regions. A better understanding of EAN health-related impacts derived from scientific evidence is pertinent not only to justify the urgent need for a more concentrated effort in addressing this issue but to assist in quantifying the magnitude of health and economic burden that can be averted. Besides, the success of curative and rehabilitative measures for abuse victims is not possible without recognizing and comprehending the consequences of EAN in their entirety.
As impacts of abuse in late life are influenced by a variety of factors including cultural norms and individual values, excessive reliance on the results of a single study or a small group of studies without considering geographical distribution and racial representation may be misleading. It is crucial that an effort is made to systematically gather all the findings of current scientific investigations to address the abovementioned gaps and existing needs. To the best of our knowledge, there have been so far only two systematic reviews addressing the impacts of EAN: (1) one focusing only on psychological well-being (Dong, Chen, Chang, & Simon, 2012) and (2) the other exploring all types of outcomes (Dong, 2015). The latter, however, adopted a more general approach in presenting its results, with limited appraisal of included studies and minimal in-depth analysis of results which could be due to differences in priorities and objectives. We therefore conducted this systematic review not only to update the previous findings but also to focus on three domains (mortality, morbidity, and health-care utilization), thus enabling a more intense and detailed examination of EAN consequences.
The aim of this review is to gather, critically appraise, and summarize the best available evidence on the consequences of EAN in order to answer the following formulated questions: What are the health consequences of EAN in terms of mortality, morbidity, and health-care utilization? What is the strength of evidence of the outcomes?
Method
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Liberati et al., 2009) and was registered in the PROSPERO international database (registration no. CRD42016035532).
While formulating the research questions, the following criteria were adhered to (1) study population was community-dwelling and institutionalized older adults defined as those aged 60 and older in general. For older individuals in African countries, a cutoff value of 50 years was used instead (WHO, 2013); (2) exposure of interest was abuse or mistreatment in all forms. We included six types of abuse: physical, psychological/verbal, financial, sexual, social, and neglect (by a perpetrator). Self-neglect was excluded; (3) comparison group was older individuals within the same community setting who were not abused; (4) outcomes were categorized into mortality, morbidity (physical, mental, social, and behavioral), and health-care utilization (hospitalization, outpatient visit, emergency department visit, etc.); and (5) all observational studies—cross sectional, case control, and cohort—were incorporated into this review.
Inclusion criteria were (1) studies with primary data collection, (2) written in English, (3) outcomes must be quantitatively described and measured, with effect size(s), and (4) abuse occurs in late adulthood (60 years and onward). On the other hand, we excluded studies without comparator groups, narrative reviews, case reports or case series, publications without primary data, duplicate studies, qualitative studies, and studies whose exposure was lifetime abuse or abuse in adulthood without any age specification.
Only health-related outcomes were incorporated into this review; impacts of EAN on other spheres such as the social support services, legal field, or financial cost were considered out of scope. We did not restrict the review to a single, standard definition of EAN, given the lack of universal definition and the multidimensional nature of elder abuse. The categorization of countries into high-, middle- (upper and lower), and low-income groups in this review was based on the World Bank’s (2015) classification.
Data Sources
Our search strategy included electronic database searches, snowball searches of citation lists in relevant articles and reviews, and contacting authors/field experts to identify potentially eligible studies. Seven electronic databases were searched from their start date to January 8, 2016: Embase, PubMed, Cochrane Library, EBSCOhost (psychology and behavioral sciences collection), CINAHL, ScienceDirect, and Campbell Collaboration. Gray literature search was conducted in Gray Literature Report (The New York Academy of Medicine), OpenGrey, and Google Scholar.
A combination of text words and Medical Subject Headings will be used where suitable. Search terms were explored in title/abstracts/key words and they included: “elder abuse and neglect” or “elder abuse” or “elder mistreatment” or “elderly abuse” and “outcomes” or “consequences” or “impacts” or “effects”. The search was not restricted to any particular health outcome given the broader terms used. While searching in OpenGrey and Gray Literature Report, key words such as elder abuse or elderly abuse or elder mistreatment or elder abuse and neglect were employed without any addition. This was deliberately done to avoid missing out any potential papers at the initial stage.
Study Selection
Study selection occurred in few phases. First, titles were screened by one reviewer to identify relevant papers. Attention was given to a set of possible existing key words (same as those used in electronic database searching, in addition to “mortality,” “death,” “hospitalization,” and “health utilization”) while screening the titles. Whenever there was doubt concerning the relevance of a title, it would be included. At this stage, the reviewer tried to be as inclusive as possible.
Two reviewers then independently screened the abstracts of selected papers. In any case of doubt, the article would be included and its full-text retrieved in the next stage. Disagreements were solved first by discussion and consensus, followed by consulting an independent, third reviewer when necessary.
The full texts of all selected abstracts were then independently assessed and appraised by the two reviewers. Inability to retrieve the full text of a study was addressed by contacting the original author(s). After a maximum period of 8 weeks, the study was excluded if there was no response. Duplicate studies or those which were part of another study were treated as one, except when the outcomes investigated were different.
Data Extraction and Quality Appraisal
A specially designed and piloted form was used for data abstraction to gauge the following information from each study: author, year of publication, study design, sample/study subjects, setting, sample size, exposure (with operational definition), outcome, tool(s) of measurement, confounding factors, and effect sizes. This step was conducted by one reviewer and accuracy of information was cross checked by the second and third reviewer. Disagreements were solved by discussion and consensus. The complete data extraction form are available as Appendix A.
Quality assessment was performed by the two reviewers independently using the Newcastle–Ottawa Scale (NOS; Wells et al., 2014). For cross-sectional studies, an adapted version of NOS was used, with slight modifications (Appendix B). Discrepancies in scoring were solved by discussion and consensus first, followed by involvement of a third reviewer when necessary. Studies were ranked as high-, medium-, and low-quality groups according to the number of stars awarded. The categorization of the scoring system was as follows: 8–9 (high), 6–7 (medium), and less than 6 (low) for cohort studies; 8–10 (high), 6–7 (medium), and less than 6 (low) for cross-sectional studies; and 8–9 (high), 6–7 (medium), and less than 6 (low) for case-control studies.
Results
The initial search resulted in a total of 517 papers. Thirty-four duplicates were detected and removed. Screening of titles excluded 429 studies as they were found irrelevant to our review scope, questions, and objectives. Two reviewers then independently assessed the remaining 54 abstracts, from which 28 were ruled out. Those excluded were (1) eight studies measuring only self-neglect as exposure, (2) seven studies having elder abuse/mistreatment as the outcome, instead of exposure, (3) one case series, (4) four studies whose objectives did not fit with the review questions, (5) one qualitative study, (6) one literature review (not a primary study), (7) one study whose exposure was lifetime abuse, (8) one study in which the age of study subjects contradicts the definition of older adults, and (9) four studies which were not published yet, existing only as abstracts (based on correspondence with the original author).
The full texts of the remaining 25 studies were retrieved for final assessment and independently appraised by two reviewers, applying all the inclusion and exclusion criteria. One full text could not be obtained, and contacting the original author yielded no response for more than 8 weeks. Disagreements between the two reviewers were solved using a similar approach mentioned before. The following studies (n = 6) were further excluded: (1) one study which was part of another study (both treated as one), (2) one study whose exposure was family violence in adult life without age specification, (3) one study which merely described the outcomes without quantitative measurements, (4) one study whose exposure was lifetime abuse, (5) one study without a comparator group, and (6) one study whose outcome was out of the review scope.
Nineteen studies met all the inclusion criteria and thus were taken to the next stage. The steps of study identification and selection are shown in a flow diagram (Figure 1).

Flowchart of study selection.
Ten (52.6%) of the included studies employed prospective designs, whereas 9 (47.4%) were cross sectional. Altogether, an estimated number of 202,982 respondents were sampled and assessed. This calculation took into account the fact that some studies might have used similar subjects while investigating different health outcomes of abuse (published in separate papers), therefore the sample size(s) of papers belonging to the same study was considered once without repetition.
Seven studies (36.8%) took only women as participants while 12 (63.2%) included both sexes. In terms of geographical distribution, 17 studies (89.5%) were conducted in Western, high-income nations with 12 in the United States, 2 in Australia, 1 in Germany, 1 in Sweden, and 1 in the Netherlands. Two studies (10.5%) belonged to Hong Kong and China, respectively. Racial diversity in the sample characteristics was mentioned in 12 studies (63.2%); defined in this review as the inclusion of at least two different ethnicities; whereas in the remaining seven (36.8%), it was either not clearly stated or could not be conclusively determined.
Eight studies did not explicitly state the operational definition of abuse or mistreatment used or made reference to any source. Among the 11 studies which had clear working definitions, seven different definitions of abuse or mistreatment were employed. Similarly, tools of measurement (to determine abuse) varied. They included (1) reports made to social services agencies (may or may not be followed by verification), (2) Vulnerability to Abuse Screening Scale, (3) Revised Conflict Tactics Scale with or without additional items, (4) Measure of Wife Abuse, (5) Violence Against Man Scale, (6) Modified Activities of Daily Living (ADL) questionnaire (for neglect), (7) Modified version of the Hwaleke–Sengstock Elder Abuse Screening Test, (8) self-administered questionnaire or structured interview without specific reference to validated scales, and (9) combination of two or more.
Nine (47.4%) of the 19 studies achieved “high-quality” score by the NOS, 8 (42.1%) were categorized as “medium quality,” and 2 (10.5%) as “low quality.” The general characteristics of each study are presented in Table 1.
Summary of General Characteristics of Review Studies.

Note. HI = high-income country; UMI = upper-middle-income country; VASS = Vulnerability to Abuse Screening Scale; PCS = physical component summary; MCS = mental health component summary scores; BMI = body mass index; GHQ = General Health Questionnaire; CTS = Conflict Tactics Scale; CHAP = Chicago Health and Aging Project; PTE = prior traumatic events; SF-36 = Short Form Health Survey; CVD = cardiovascular; ADL = activities of daily living; RAND = RAND corporation (Research and Development) is an American global policy think thank formed by Douglas Aircraft company.
Health Consequences of EAN
Four studies (prospective cohort) investigated mortality as an outcome, all of which unanimously reported higher risks of death among abused older adults, albeit differences in effect sizes and subtypes of abuse investigated (Baker et al., 2009; Dong et al., 2009; Lachs et al., 1998; Schofield et al., 2013). With regard to health-care utilization, risk of hospitalization (Dong & Simon, 2013b), rate of annual visit to emergency departments (Dong & Simon, 2013a), and consumption of behavioral health services (Schonfeld, Larsen, & Stiles, 2006) were found to be higher among EAN victims than their nonabused counterparts. Morbidity outcomes in this review encompassed a wide range of health conditions and termed as follows: physical health, physical function, mental health, psychological health, disability, depressive symptomatology, depression, psychological distress, negative emotional symptoms, self-rated health, musculoskeletal pain, headache, incontinence, allergy, stomach problems, overweight, anxiety, sleeping problems, stress, suicidal ideation, suicidal attempt, digestive problems, metabolic syndrome, chronic pain, somatic complaints, and social dysfunction.
Two studies particularly explored gender differences in EAN outcomes. Women were more likely to experience poorer general health, more digestive symptoms and higher level of stress when psychologically abused, and greater anxiety when physically abused than their male counterparts. Conversely, men reported more headaches, allergic symptoms, anxiety and suicidal ideation when psychologically abused; incontinence and sleeping problems when physically and psychologically abused; and higher level of stress when physically abused. On the other hand, “exclusive male effects” were found between physical abuse and musculoskeletal pain, diabetes, weight problems, and headache; between financial abuse and suicidal ideation; and between psychological and physical abuse and suicidal attempt. “Exclusive female effects” were shown between physical and psychological abuse and health-care use index (Olofsson et al., 2012; Wu et al., 2013).
All studies corroborated the relationships between abuse and the various types of morbidity mentioned, with two exceptions: Cannell et al. (2015) in a 12-year prospective cohort study did not find any significant decline in physical function among abused, postmenopausal women, while Cisler et al. found no relationship between abuse and poor self-rated health after full adjustment for confounders (Amstadter et al., 2010).
Table 2 summarizes the consequences of EAN and their effect sizes according to the three categories: mortality, morbidity, and health-care utilization.
Summary of Consequences of Elder Abuse and Neglect.
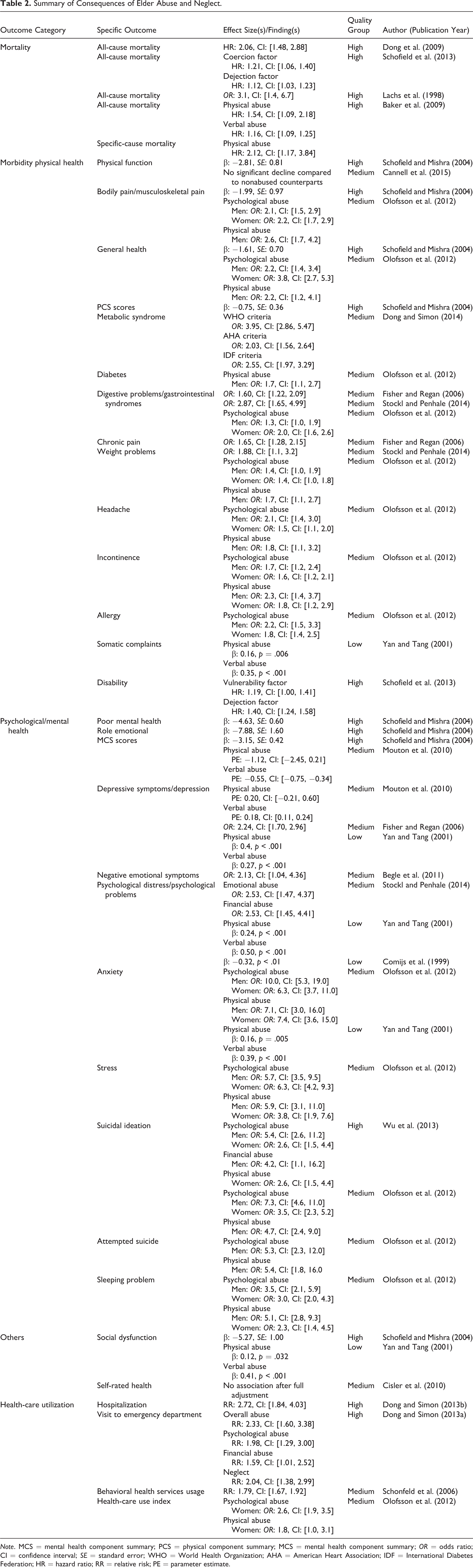
Note. MCS = mental health component summary; PCS = physical component summary; MCS = mental health component summary; OR = odds ratio; CI = confidence interval; SE = standard error; WHO = World Health Organization; AHA = American Heart Association; IDF = International Diabetes Federation; HR = hazard ratio; RR = relative risk; PE = parameter estimate.
Strength of Evidence
Higher risks of or premature mortality as an outcome of abuse of older individuals emerged as the most robust finding, owing to the prospective design and the high-quality scores achieved by all the studies using the NOS. The longitudinal relationships between mistreatment and mortality were consistent across the four studies, after adjustment for confounding factors.
In the sphere of mental health, depression or depressive symptomatology was ranked first, followed by poor mental health, psychological distress, anxiety, and suicidal thoughts. There was limited evidence with reference to stress, suicidal attempt, sleeping problem, social dysfunction, and interference of daily activities due to emotional difficulties. Some of these findings came from cross-sectional designs therefore causality could not be determined, while some were supported by only one or two studies. More research with rigorous methods is needed to ascertain the consistency of these findings.
Impacts of EAN on physical health include bodily and musculoskeletal pain, poor general health, and digestive or gastrointestinal symptoms—all of which were categorized as inconsistent evidence and corroborated by a mixture of high- and medium-quality prospective and cross-sectional studies. Other findings such as metabolic syndrome, diabetes, chronic pain, weight problems, headache, incontinence, allergy, somatic complaints, and disability have been limited by the small number of studies conducted. Overall, findings suggest that EAN is likely to contribute to decline in both physical and mental health.
From the lens of health-care utilization, increased health-care consumption was reported in four studies, with one showing higher rates of hospitalization and another specifically documenting higher usage of behavioral health services. The summary of EAN outcomes according to strength of evidence is presented in Table 3.
Summary of Evidence Strength of Consequences of Elder Abuse and Neglect.

Unexplored Health-Related Domains
There is palpable scarcity of evidence with reference to delirium, fall, incontinence, frailty, pressure ulcers, dizziness, and syncope—all of which constitute the common health conditions of older adults known as the “geriatric syndromes.” Other unexplored, possible effects of EAN which have not been adequately studied and therefore necessitate future attention comprise (1) decline in quality of life (QoL), (2) deterioration of cognition and physical function such as gait speed and hand grip, (3) social and behavioral disorders, and (4) sexually transmitted diseases (STDs) and diseases of the reproductive system as outcomes of sexual abuse.
Discussion
This review summarizes and presents the consequences of EAN relating to mortality, morbidity, and health-care utilization. Nineteen studies were analyzed, all of which were peer reviewed and published. Despite using the best-evidence methods to search for relevant papers, less than 30 studies fulfilled our inclusion and exclusion criteria. This reflects a relatively rudimentary stage at which research into health consequences of elder abuse currently is, despite the burgeoning interest and evidence of proliferation of studies in this field.
Consequences of EAN
Mortality
Premature mortality emerged as a highly plausible outcome of EAN after rigorous processes of data abstraction and quality appraisal. Nevertheless, all the four studies investigating mortality originated from the United States and Australia, with two (50%) taking only women as their study subjects. Even with racially diverse samples, the representation of non-Whites or those of non-English origin was very small. Considering the geographical imbalance and inadequate representation of other ethnic groups in the existing studies on mortality among abused elderly, it is important that more research is carried out in middle- and low-income regions and among non-Western populations to determine the replicability of this finding.
A common approach adopted by most of the studies involved was to analyze EAN as a single entity rather than treating its subtypes separately. Studying how each category of abuse affects risks of death might give us a new dimension or deeper insight in understanding this relationship.
Morbidity
Studies assessing morbidity as an impact of abuse have given a slightly greater emphasis on the psychological or emotional domain than the physical health or function. The majority of findings came from cross-sectional studies, thus a temporal order and causality cannot be established. Depression and other interrelated terms such as poor mental health, negative emotional symptoms, and psychological distress recurrently and consistently emerged as significant outcomes. Consequences such as sleeping problem, suicidal ideation, incontinence, metabolic syndrome, and allergy were supported by only one or two studies, therefore more explorations are needed. Replication of existing research on morbidity outcomes with longitudinal, prospective design may be able to explain the mechanism of premature mortality.
Making distinction between the subtypes of abuse while assessing morbidity outcomes might be vital, as treating elder abuse as a single entity may render results difficult to interpret. This is because different types of abuse have been reported to affect health differently (Katz & Arias, 1999; Leserman et al., 1996). In this review, some studies analyzed relationships between subtypes of abuse and health outcomes separately, while some others did not. Comparison therefore is to be made cautiously. Similarly, investigating dose–response relationships between severity of abuse and degrees of health impacts deserves emphasis in order to strengthen causality, as suggested by the Bradford Hill criteria (1965). This, however, was not commonly seen in the included studies.
Health services utilization
Four studies measured health-care consumption among abused and neglected older persons (Dong & Simon, 2013a, 2013b; Olofsson et al., 2012; Schonfeld et al., 2006). The first two were part of the Chicago Health and Aging Project and the third was conducted in Florida—all within the boundaries of the United States. One was conducted among Swedish older adults (Olofsson et al., 2012). Even though all studies reported greater health services utilization, alternative patterns of health-care consumption is still a possibility, especially in middle- and low-income regions or among non-Western populations. A wide range of factors which can be rather complex and intertwined—predisposing, enabling, and need characteristics—determine the utilization of formal health services as proposed by Andersen (1995). The organization of a health-care system in a country, for instance, affects the rate of health-care consumption and access to services. Middle- and low-income nations generally have less sophisticated health systems and lack adequate social support services to detect abuse cases and facilitate victims’ access to health-care personnel. Health services utilization among abused older adults therefore is likely to vary across settings. Cultural interpretations and understanding of abuse by victims is another factor which may render the amount and nature of health-care consumption different by influencing individuals’ choice of response and health-seeking behavior. The relationships between culture or sociocultural contexts and health-seeking behavior have been established by a number of studies (Ensor & Cooper, 2004; Oberländer & Elverdan, 2000; Shaikh & Hatcher, 2005). Current findings are thus insufficient, with more investigations needed to bridge the gap.
Methodological Inconsistencies
Seven operational definitions with varying degrees of overlap were employed across 11 studies, while the remaining eight did not give any explicit statement, indicating a lack of uniformity of EAN definition. As ascertainment of exposure (abuse) is strictly bound to operational definitions and given the varying definitions employed, it is difficult to fully gauge the extent to which abuse was conceptualized in a similar manner across the studies. On the other hand, nine different tools were used to measure EAN in 19 studies, another manifestation of methodological inconsistency. In addition, the measurement of an outcome was often established by multiple tools. For instance, depression or depressive symptomatology reported in three studies was ascertained by three different questionnaires: Center for Epidemiological Studies Depression Scale (6-item version), General Health Questionnaire, and the Women’s Health and Relationship Survey (WHRS) questionnaire (adapted from validated scales) through telephone interview. Such heterogeneity poses a challenge for comparison. One possible way to address this issue in the future is through the establishment of consensus at the national or international level among researchers and field experts on the research framework of EAN.
Cultural and Gender Differences
As stated before, the majority of studies included were conducted in high-income countries predominantly the United States and Australia. This reflects an underrepresentation of older populations from middle- and low-income regions whose sociocultural composition and contexts may have an influence on the dynamics between EAN and health consequences. Analysis of cultural differences in our review is limited not only by the small number of studies (two) among non-Western populations but also that these two studies have focused mainly on psychological outcomes of EAN, mental health (Yan & Tang, 2001), and suicidal ideation (Wu et al., 2013). However, an interesting finding is worth mentioning; while physical abuse was associated with suicidal ideation among Swedish men and not women, a similar relationship was found among Chinese women and not men. Even though gender might be a differentiating factor, culture is also likely to have a role. Cultural diversity has been said to exist in interpretations of suicide and suicidal behavior. For example, suicide is common among “White” American men, where it is regarded as a masculine behavior. Conversely, suicide is deemed an “act of the powerless” in Chinese society. Therefore, men who kill themselves are seen as weak. Consequently, it is more prevalent among women (Canetto, 2008). Other than that, culture was also said to affect expressions of bodily symptoms (Kirmayer & Sartorius, 2007; Kirmayer & Young, 1998), health-seeking behavior, and health utilization (Ensor & Cooper, 2004). Further explorations across geographical boundaries and ethnicities may reveal more variations in morbidity and health services utilization by EAN victims.
The role of gender in EAN and its health consequences, despite having not been adequately explored, was demonstrated in the findings of two studies (Olofsson et al., 2012; Wu et al., 2013). How abuse or mistreatment affects men and women differently with regard to suicidal thoughts and attempts, stress, anxiety, sleeping problem, and use of health care, for instance, indicates that gender is an important aspect to consider while investigating EAN consequences. The differences seen can be a result of (1) health disparities which already existed between older men and women at baseline level. For instance, a study among older adults in Great Britain showed that older women in general were materially and socially disadvantaged compared to older men. They also had higher levels of severe disability and poorer living arrangements, which negatively affected their health (Arber & Cooper, 1999). When accompanied by a chronic stressor such as abuse or mistreatment, such disparity may be aggravated, thus explaining the diverse effects seen among male and female abuse victims, (2) distinct ways in which older men and women respond to and cope with health problems and adverse experiences. For example, men and women were reported to show different patterns of health services utilization (Bertakis, Azari, Helms, Callahan, & Robbins, 2000) and express physical symptoms differently (van Wijk, Huisman, & Kolk, 1999). Similarly, when facing distressing situations, they employ distinct coping styles (Matud, 2004) and emotion regulation strategies (Nolen-Hoeksema, 2012). Future research on EAN should delve into how this variable shapes the impacts of abuse in late life.
Limitations
This review has a number of limitations. First, non-English publications were excluded. Accordingly, findings published by non-Western or non-English journals might have been systematically overlooked. Second, there is overlap between elder abuse and other forms of family violence such as intimate partner violence (IPV) and lifetime family violence, which can render interpretation of results rather difficult. For example, one of the studies included in this review investigated the consequences of IPV among older women (Stöckl & Penhale, 2014). But given that it fit into our eligibility criteria, the study was analyzed and its findings interpreted from the lens of elder abuse. Another example is that abuse episodes in our review should occur at the age of 60 and onward as a prerequisite for EAN. However, evidence suggested that “for many older adults, abuse and neglect may be part of a continuing pattern of mistreatment that begins very early in life” (Phelan, 2013, p. 55). As studies included in this review did not consider occurrences prior to age 60, the outcomes assessed could either be the true impacts of abuse in late life or the cumulative effects of long-term, on-going abuse. Third, publication bias has not been assessed in this review and we acknowledge the possibility of research with negative results not being published. Our review findings therefore have to be interpreted in the light of these limitations besides the methodological irregularities discussed before.
Implications on Practice, Research, and Policy
Several recommendations can be put forward based on the summarized findings of this review concerning clinical practice, research, and social or health policy: Understanding the wide range of morbidity outcomes of EAN points to the need for training of health-care providers and promotion of multidisciplinary engagements in managing EAN victims in the clinical setting. Future research work should consider analyzing the possible unique contribution of abuse subtypes to health outcomes rather than treating EAN as a single entity. The role of gender in mediating EAN consequences similarly deserves more attention, as findings might provide a new way of understanding and managing abuse victims. Research on how EAN impacts health-care utilization should be expanded and replicated in various settings, mainly regions with different sociocultural contexts and health systems composition. This can help identify the unmet needs of abuse victims for health care and estimate the health and economic burden of this social problem. Better planning and proper allocation of health-care and financial resources can therefore be implemented. More research is needed to explore how EAN can affect other health domains such as geriatric syndromes, STD’s and reproductive system diseases, cognition, QoL, and social and behavioral disorders. Population-based, prospective studies pertaining to consequences of EAN ought to be pursued especially in middle- and low-income countries. Standardization of tools to define and measure abuse and neglect is an issue to address, along with the need for modification to make them culturally sensitive and compatible. This can be achieved through establishing consensus among researchers and field experts. Given that health is a major issue in EAN, management of abuse victims should always include facilitation of access to health services and aim at improving their long-term health and QoL.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review is funded by the University of Malaya Grand Challenge Program: Preventing Elder Abuse and negleCtinitiativE (PEACE; GC 001A-14HTM). NNH’s work is partially sponsored by the University of Malaya Population Studies Unit (PSU). PROSPERO registration no. CRD42016035532.